
Abstract
Physical inactivity is a vital risk factor for the development and maintenance of chronic ill-health conditions among older adults. This study examined personal factors associated with physical activity (PA) behavior of urban-dwelling older adults in Sri Lanka, a middle-income country in South Asia. A total of 880 older adults (aged ≥60 years) participated in this cross-sectional study. They responded to anthropometrical, health, and socio-demographic data pertaining to their current physical and behavioral status. The mean age of the participants was 70.1 years (SD ±6.0), and the majority (75%) were women. Increasing age, male gender, middle income, having cardiovascular diseases or arthritis, deficiencies in muscle strength and balance, pain, and lower self-rated health were associated with insufficient PA behavior among the participants. Old-age physical activity promotion programs should target older adults in advanced ages and men in particularly, as they are highly vulnerable to sedentary lifestyles. Muscle strength and balance, a neglected area in PA promotion in older adults, seem to play an important role in older adults’ participation in physical activities. Incorporation of pain management, and muscle strength and balance techniques into older adults’ PA promotion programs would probably increase adherence rates of the participants in such programs.
Introduction
In older adults, sedentary behavior contributes to deterioration of health and well-being, and increases chronic disease morbidity and mortality rates (Kleinke et al., 2020; Notthoff et al., 2017). It is observed that 40% to 80% of older adults worldwide do not meet the World Health Organization (WHO) recommended levels of physical activity (World Health Organization, 2010). Thus, sedentary behavior has become a significant public health issue among older adults across the world. Socio-ecological models explain personal, social, environmental, policy, and organizational factors as vital determinants of adherence to physical activity by people (Manz et al., 2018; Schmidt et al., 2016).
Advanced age, female gender, and higher socioeconomic status were found to be major demographic risk factors associated with sedentary behavior among older adults across the world (Harvey et al., 2013; Manz et al., 2018), and impairments linked to body anthropometry, health status, strength, and balance were found to be the main biological underpinnings of physical activity levels among the said population group (Cruz et al., 2017; Ferreira et al., 2012). Motivation, self-efficacy, self-determination, and perceived barriers were the psychologically decisive factors of physical activity behavior among older adults (Gray et al., 2016; Schmidt et al., 2016). However, determinants of physical activity among older adults have been less frequently studied in low-and middle-income countries in Asia (Gaskin & Orellana, 2018; Guthold et al., 2018; Yap et al., 2020).
Sri Lanka, a middle-income country in Asia, has one of the fastest-aging populations in Asia (Asian Development Bank, 2019; Department of Census and Statistics, 2017). It is estimated that the percentage of adults older than 60 years in the country will increase from 16.7% in 2021 to 29% in 2050 (Asian Development Bank, 2019). As Sri Lanka is an agricultural country, Sri Lankan older adults are a physically active cohort (Katulanda et al., 2013). However, urbanization and westernization of the Sri Lankan society have led many Sri Lankan older adults to be less active and consequently vulnerable to developing chronic ill-health conditions. A study conducted in urban Sri Lanka found that 63.4% of older adults were suffering from chronic diseases (Ranaweera et al., 2013). Further, only a small proportion of older adults have social security benefits, and it was observed that Sri Lanka’s higher non-communicable disease mortality burden is driven by under-treatment (Asian Development Bank, 2019; Ministry of Health Sri Lanka, 2016) probably due to poverty.
It is argued that urbanization and increases in sedentary living will increase non-communicable disease burden in older adults in many low and middle income countries (Asian Development Bank, 2019; Gaskin & Orellana, 2018). Non-communicable disease burden would make devastating effects on healthcare systems and economies in such countries and Sri Lanka is no exception. Reduction in the prevalence of insufficient physical activity in older adults would therefore be one of the promising and feasible healthcare strategies that could reverse non-communicable disease burden and associated financial crisis in Sri Lanka. However, public health and economic strategies designed to address the problem of sedentary behavior in older adults must be based on country and culture specific scientific evidences of that behavior. Such scientific evidences are scarce in the Sri Lankan context and therefore studies focusing on physical activity and health seeking behavior of older adults in Sri Lanka are urgently needed. This study has aimed to identify the personal determinants of physical activity behavior among urban-dwelling older adults in Sri Lanka. In this study, age, gender, income, self-reported health problems, muscle strength and balance, pain and self-rated health were considered as vital personal determinants of PA, and mean metabolic equivalence task per week (MET/week) was used to measure physical activity behavior of the participants (World Health Organization, 2012).
Materials and Methods
Population, Sample, and Settings
A cross-sectional community survey was conducted involving a random sample of older people (60 years of age and over) in Colombo district in Western Sri Lanka. This district is one of the highly urbanized districts in the country, and urban dwelling older adults in the district fairly represent urban dwelling older adult population in the country. Multi-stage cluster-sampling technique was used to select the participants. The sample size was determined using an estimated older adults’ physical inactivity prevalence of 20% (Bishwajit, O’Leary, et al., 2017; Hosseinpoor et al., 2012), margin of error of 0.05, and design effect of 2.5. The number of age-sex estimates and the anticipated response rate were taken as 1.5 and 0.9, respectively (World Health Organization, 2015). Thus, the required sample size was 1,100 (Lwanga et al., 1991). However, only 898 of the selected participants completed the survey. This cross-sectional survey was conducted following the STROBE reporting guidelines.
Procedures
Those older adults who were willing to participate were screened for cognitive impairment using the Mini Mental State Examination (MMSE). Older adults with cognitive impairments (a score of <17 in MMSE) who had an illness or difficulties speaking or hearing were excluded from the study (De Silva & Gunatilake, 2002). Eligible participants were interviewed in their home settings, and available medical records were checked by the principal investigator (a nurse practitioner) after obtaining the informed consent. Data collection was conducted by the principal investigator with support from a trained research assistant.
Variables Measured
Physical activity and five categories of personal determinants: demographic, anthropometric, strength, balance, and health status were the variables measured under this study. These variables were found to be the most important response and predictor variables in studies on physical activity behavior in older adults (Aro et al., 2018; Bishwajit, Tang, et al., 2017; Cruz et al., 2017).
Dependent Variable
Physical activity was the outcome variable and the Global Physical Activity Questionnaire version 2 (GPAQv2) was used to collect the physical activity data of the participants. GPAQv2 is a 16-item tool that collects domain-specific physical activity data under three domains: activity at work that included six items such as “How much time do you spend doing moderate-intensity activities at work on a typical day?” active transport that included three items such as “in a typical week, on how many days do you walk or bicycle for at least 10 minutes continuously to get to and from places?” and leisure time-related activities that included six items such as “in a typical week, on how many days do you do moderate-intensity sports, fitness, or recreational (leisure) activities?” This tool measured physical activity using the mean metabolic equivalence task per week (MET/week) (Armstrong & Bull, 2006; World Health Organization, 2012). The tool has been validated and extensively used in low and middle-income country settings including Sri Lanka (Bull et al., 2009; Wickramarachchi at al., 2020). Participants’ physical activity status was categorized as either sufficiently active or inactive. Sufficiently active individuals are defined as those who do a minimum of 1,500 MET/Week of physical activity, and those who do less than 1,500 MET/Week of physical activity were classified as inactive individuals.
Independent Variables
Demographic variables
Socio-demographic variables collected included age, gender, marital status, family income, level of education and living arrangements.
Anthropometric measurements
Body mass index (BMI), waist circumference, and fat percentage were measured. BMI was calculated using the formula body weight measured in kilograms divided by height in meters squared (kg/m2). Waist circumference was measured using a non-elastic tape to the last 0.1 mm, and fat percentage was tested based on the skinfold thickness in the biceps, triceps, supra-iliac, and subscapula. Fat percentage was calculated using the Durnin and Womersley method (Durnin & Womersley, 1974).
Strength
Leg strength and hand grip strength (HGS) were tested. A 30-second chair stand test was performed to assess lower-extremity muscle power (leg strength). HGS was measured using a dynamometer (TANITA, no 6103, Japan) to the nearest kilogram according to the Southampton protocol. A higher value is an indicator of good performance.
Balance
Dynamic and static balances were measured. To test the static balance, a four-stage balance test was performed, including standing balance, semi-tandem position, tandem stance position, and one-leg stance position. Each task was tested for 10 seconds, and the number of seconds required for each activity was recorded. Dynamic balance was tested using a 360° turning test and Timed-Up and Go (TUG) tests. In the 360° turning test, the time taken by the participant to do a 360° turn was recorded. In the TUG test, the person was asked to stand up and walk 3 m and turn back to the chair and sit down. The average time taken to perform two rounds was recorded. A lower value is an indicator of good performance.
Health status
Presence of listed medical conditions, presence of aches or pain, self-rated health (SRH), and frequency of doctor visits (FDV) were assessed. The presence of medical conditions was assessed according to the self-reported medical conditions disclosed in participants’ medical records and interviews. The presence of aches or pain was evaluated by asking the participants whether they suffered from any kind of pain or body ache. A dichotomous variable was constructed with categories “no” and “yes.” Self-rated health was assessed using a single-item asking, “How do you rate your health status from ‘very good’ to ‘very poor’.” Responses were further categorized into three categories as “poor/very poor,” “fair,” and “good/very good.” The FDV in the previous 12 months was recorded using self-reported data and medical records. The FDV was grouped into four categories: none, 1 to 5 times, 6 to 11 times, and more than or equal 12 times per year.
Ethical Consideration
Ethical approval was obtained from the Ethics Committees of the Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka (12.07.2018:3.1) and the Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak, Malaysia (UNIMAS/NC-21.02/03-02 Jil.2(94)). Written consent was obtained from each participant before the questionnaire was administered.
Analysis
Data analysis was performed using SPSS (version 25). The prevalence of sufficiently active and inactive individuals was calculated. The Shapiro–Wilk test showed that the physical activity data were not normally distributed (p = .00). Therefore, non-parametric statistics were used where necessary. The association between physical activity with socio-demographic variables and other dependent variables were determined using Pearson’s chi-square test and independent t-test. Multivariable binary logistic regression determined the individual factors associated with physical activity. Mean and Standard deviations were used to summarize continuous variables. An odds ratio (OR) of more than one indicated the likelihood of inactivity. Spearman correlation coefficient was used to determine whether income and FDV are related. The significance level was set at 5% level.
Results
A total of 898 participants were surveyed. Thus the response rate was 81.6%. Sixteen uncompleted questionnaires and two outliers (as defined in the GPAQv2 analysis guide) were removed from the final analysis. Thus, data from 880 respondents were analyzed.
Socio-Demographic Characteristics
The mean age of the participants was 70.2 years (SD ±6.0). The majority were female (75%), and about half of the participants were in the 60- to 69-year age group. Approximately two-thirds of the participants were in the low-income category (63.2%). Almost all (98.2%) were married, and among the married persons, 36.4% were either widows or widowers. Only 13.2% of the participants had obtained or completed no more than a primary education, and the others had a secondary or tertiary education level. Of the participants, 10.7% reported living alone, while 3.2% reported living with relatives or with non-family members. The rest were living with spouse, children, or spouse and children.
Prevalence of Physical Activity
Overall, 78.5% of the participants were sufficiently physically active (Table 1). Physical activity declined with increasing age (p = .00). Older women were more likely to be physically active than older men (p = .08). One-fifth of married persons were physically inactive. Older adults from the lower-income brackets were more likely to be physically active than others (p = .01).
Activity Status of the Older People According to the Socio-Demographic Characteristics (n = 880).

Note. p is form Pearson’s chi-square test that tested associations between activity status and socio-demographic variables.
The M (SD) of leg strength, static balance, and dynamic balance reflected significant differences between inactive and sufficiently active categories (p < .001) (Table 2). Significantly higher proportions of older adults with cardiac or arthritis/joint pain were inactive. A higher proportion of those who have rated their health as “very good/good” compared to others were sufficiently active. A higher proportion of those who had made zero doctor visits over the previous year compared to that of others were physically inactive. A higher proportion of those older adults who reported having pain/aches were physically inactive compared to that of others.
Distribution of Physical Activity of the Significantly Associated Covariates from the Binary Logistic Regression Models (n = 880).
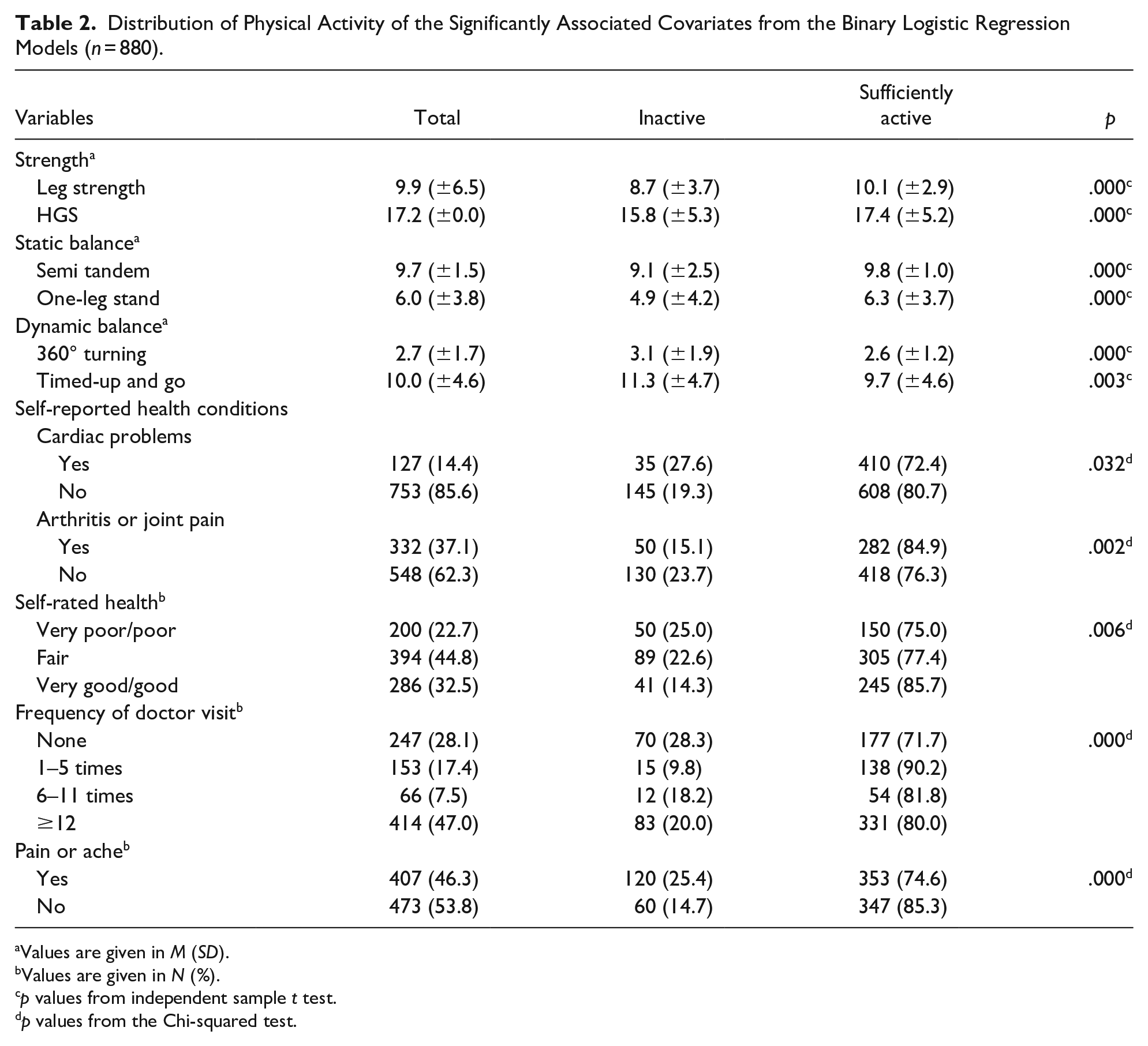
Values are given in M (SD).
Values are given in N (%).
p values from independent sample t test.
p values from the Chi-squared test.
Personal Determinants of Physical Activity
Significantly associated factors of physical activity found in the bivariate binary logistic regression model were loaded into three multivariable binary logistic models. Age, family income, HGS, leg strength, semi-tandem position, one-leg stand, 360° turning test, TUG test, cardiac problems, arthritis or joint pain, SRH, FDV, and presence of pain or aches were significantly associated with physical activity of the participants.
In multivariable models, model one included all socio-demographic factors. In model two, strength and balance were added to the model one. In model three, health statuses SRH, FDV, and presence of pain or aches were added to the model two. These models met all the assumptions for the analysis. The Hosmer–Lemeshow goodness-of-fit test showed a non-significant p-value (p = .532) and a higher −2 log likelihood (780.0), indicating a good model fit (χ2 = 7.0). The multivariable-adjusted model for the older urban population provided determinants of physical inactivity. The model summary and odds of physical inactivity among the participants are presented in Table 3.
Multivariable Binary Logistic Regression Analysis for Determinants of Physical Activity of the Participants (n = 880).
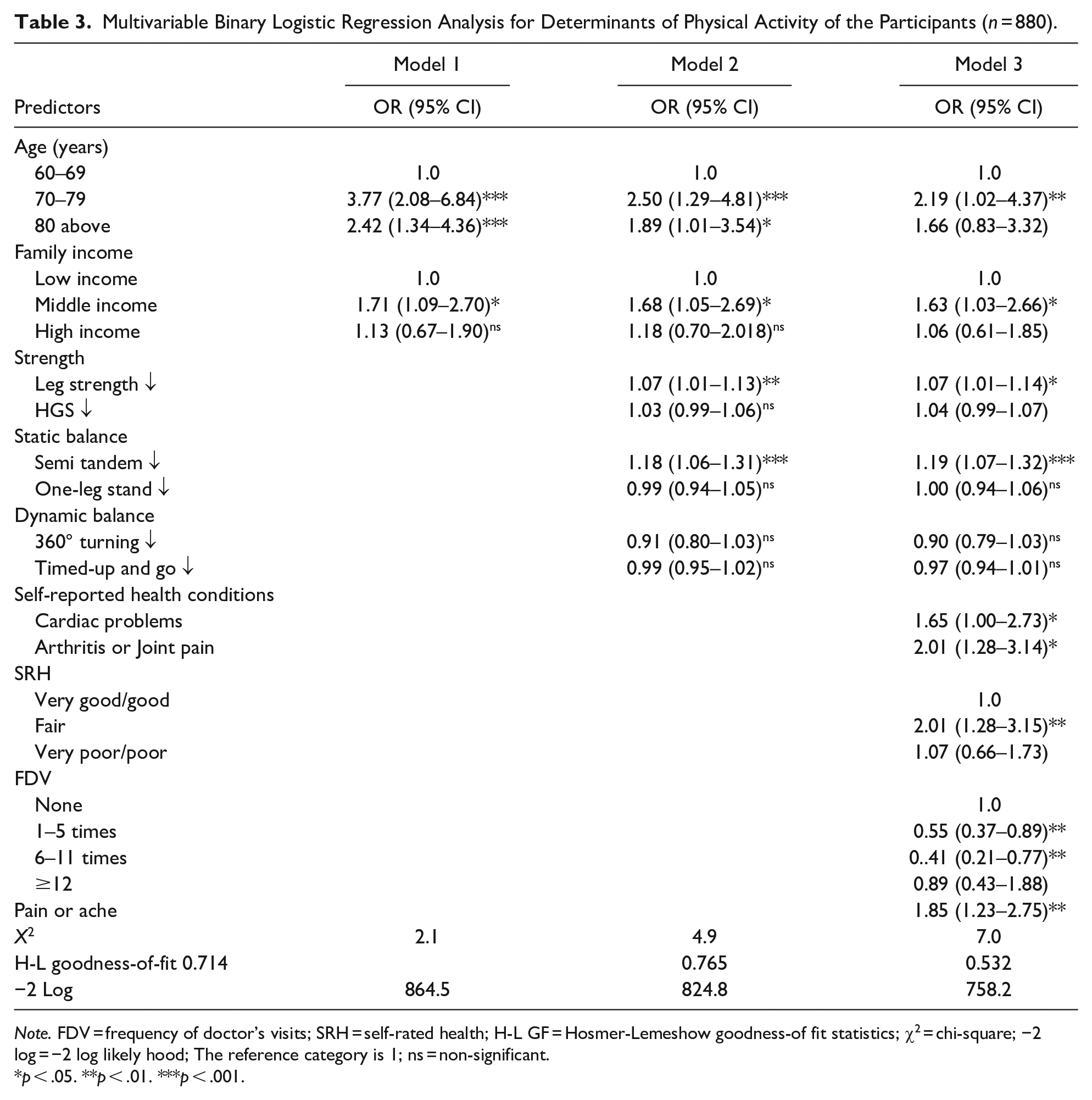
Note. FDV = frequency of doctor’s visits; SRH = self-rated health; H-L GF = Hosmer-Lemeshow goodness-of fit statistics; χ2 = chi-square; −2 log = −2 log likely hood; The reference category is 1; ns = non-significant.
p < .05. **p < .01. ***p < .001.
The final model (model 3) indicated that those aged 70 to 79 years and those aged 80 and older were more likely to be physically inactive compared to those aged 60 to 69 years, but a significant result was found only for the age group 70 to 79 years (OR = 2.19, p < .01, and OR = 1.66, p > .05 respectively). Further, older adults in the middle income category seem to be the most vulnerable group to experience physical inactivity (OR = 1.63, p < .05 compared to older adults from poor income category). Those participants with lower scores in leg strength (OR = 1.07, p < .01) and higher scores in semi-tandem position (OR = 1.19, p < .001) were more likely to be inactive. Cardiac problems (OR = 1.65, p < .01) and arthritis or joint pain (OR = 2.01, p < .01) correlated with higher odds of inactivity. Older people who reported their SRH as “fair” or “very poor/ poor” were more likely to be inactive than those who rated their health as “very good/good” although a significant result was found only for the “fair” category (OR = 2.01, p < .01, and OR = 1.07, p > .05, respectively). Those who had made doctor visits in the preceding year were more likely to be active compared to the participants who had made no doctor visits in the previous year. Participants who suffered pain or aches were 1.8 times more likely to be inactive (OR = 1.85, p < .001) than those who reported no pain or aches (Table 3). Monthly income and FDV were not related (r = 0.037, p = 0.27).
Discussion
This study assessed the personal determinants of physical activity of urban-dwelling older people in Sri Lanka. Age, strength, balance, cardiac problems, pain or aches, arthritic and joint pain, SRH, and FDV significantly determined the activity status of the participants. In this study, 75% of the participants were women. In the year 2019, the estimated sex ratio in the country was 0.93 (Department of Census and Statistics, 2017). Labor force participation rate for females in Sri Lanka was 33.5 in 2019 and therefore the vast majority of women in Sri Lanka tend to stay at home during the day time. Sri Lankan culture is such that men are busy and somewhat reluctant to participate in these types of surveys. On the other hand adult females are more concern about their health than that of adult males. These were the probable reasons why there was a higher participation rate of older women in the current study. However, it should be noted that 220 older men participated in the study, an adequate number for analytical purposes.
Age is a vital determinant of inactivity among urban older adults, an observation that applies to many older populations worldwide (Larsson et al., 2016; Murtagh et al., 2015; Rai et al., 2020). Older adults living in urban areas are confined to closed environments with limited social interactions in Sri Lanka. These environmental restrictions, coupled with chronic ill health that grows gradually with aging, would have caused urban-dwelling old-older adults (those of aged 70+ years) to be vulnerable to reduced physical activity (Ding et al., 2020; Rai et al., 2020). Older women seem to be more physically active than older men. Primary care physicians in the country should be educated and motivated to screen older adult patients in advanced ages to detect possible physical fitness and pain management issues that bar them from engaged in physical activities. Health promotion policies and strategies aimed at old adults should be adjusted to address these age- and sex-specific physical activity behaviors. Since female life expectancy in Sri Lanka is continuously growing the extension of the retirement age would facilitate female activity in old age. This is especially true for urban-dwelling women and needs attention from health policy makers.
Older adults who came from lower-income brackets were more likely to have higher physical activity levels. A study conducted in an urban area in Sri Lanka had indicated the same result (Karunanayake et al., 2020). In the developed world, however, the reverse has been observed (McPhee, 2016; Rawal et al., 2020). Not only young older adults but older adults in advanced age categories in low- and middle-income countries also have to work in advanced ages for survival, as the majority of them do not enjoy any social security benefits.
According to the current study, those who exhibited reduced lower leg strength were more likely to be physically inactive. Several studies supported this assertion (McKee et al., 2015; Trombetti et al., 2016). Declining muscle mass, strength, and power finally reduce the physical performance of older people. The loss of muscle mass and alterations in the properties of individual muscle fibers influence the loss of muscle strength among older adults (Tieland et al., 2018). Aging affects all lower extremities, and femoral muscle mass has been associated with physical function among older adults (Ferreira et al., 2012). According to Milanovic et al. (2013), after age 75, muscle strength decreases by an average of 3.4% annually, and muscle strength loss is greater in the lower limbs than in the upper limbs (Landers et al., 2001). Declining strength is found to be an independent contributing factor to increased fear of falling, which may prevent older adults from engaging in exercise.
The results of the binary logistic regression supported the already established relationship between physical activity and balance performance among older adults (Bootsman et al., 2018; Cruz et al., 2017). However, in the multivariable model only the semi tandem position had a significant result. The significant decline in balance performance with aging discourages activity among older people (Bootsman et al., 2018). In particular, Blewitt and Chockalingam (2017) who investigated the balance performance of older adults, revealed that adults with less balance (semi-tandem position) were much less likely to be physically active. This finding provides a rationale for developing interventions to improve muscle strength and balance to enhance physical activity participation among older adults. Furthermore, the use of a strength test (HGS and leg strength) as a screening activity to predict the potential risk of a sedentary lifestyle among older adults should be considered in primary health care and primary care services in the country.
Pain, including arthritis and joint pain, emerged as another strong determinant of avoiding activity in the target population. Pain is the main cause of work-related disability among middle-aged and older adults worldwide (Vadal et al., 2020). In this study, older people with arthritis or joint pain were more likely to be inactive than participants with no pain. This is in line with similar studies across the world (Baert et al., 2015; Larsson et al., 2016), in which chronic pain has been identified as a major barrier to physical activity among older adults. A cross-sectional multi-country study on older people conducted in South Asia, however, reported somewhat contradictory findings (Bishwajit, Tang, et al., 2017). In this study, back pain was not significantly associated with walking behavior among Sri Lankan older adults, and the association between back pain and vigorous physical activity was significant among women but not among men. Definitions of back pain and subjective measures of back pain and physical activity in this study may explain these incongruent findings. The practice of fear-avoidance technique is found to be an effective strategy for remaining active among older adults suffering from pain (Larsson et al., 2016). The probable etiologies of all kinds of pain among older adults in Sri Lanka should be investigated, and pain prevention in old age should be incorporated in youth and adult health promotion programs nationwide.
Consistent with other studies (Hong, 2016; Macniven et al., 2014), this study found the presence of cardiac and arthritis conditions to be risk factors for physical inactivity among participants. Health education and promotion programs for cardiac and other chronic diseases aimed at older patients should stress the need for physical activity to regain at least some portion of the living potential older adults had enjoyed in the past. Improving physical activity among older adults with chronic diseases improves their overall health, independence, and quality of life (Reiner et al., 2013; Roman et al., 2016; Taylor, 2014). Individual guidance and appropriate medical advice are needed to make them confident about the tremendous benefits of having a physical active life-style in old age.
In the current study, participants with higher levels of SRH were more likely to engage in higher levels of physical activity participation. Similar to the current study, studies reported older people who rated their health as “very good or good” as being highly active (Showa et al., 2016; Song et al., 2019). The association between SRH and physical activity found in this study is probably attributable to acceptance, tolerance, and lack of seriousness about the health and good family support extended to older adults in Asian communities. Qualitative studies are needed to explore the socio-cultural factors contributing to SRH among older adults. Promotion of physical activity would ultimately further urban-dwelling older adults’ contentment with their physical and psycho-social status and circumstances and reduce unnecessary psychological burdens.
In this study, an association was found between physical activity and healthcare utilization of the participants; older adults who had made more visits to the doctor in the previous year were more likely to be sufficiently physically active. However, some studies have demonstrated the opposite (Jacobs et al., 2013; Rocca, 2015). Physical activity, health status, and FDV are interrelated (Jacobs et al., 2013; Sari, 2011) but older adults’ decisions to seek medical consultation highly depend on many personal, environmental, and economic factors. Thus, further studies are needed to identify personal, structural and environmental factors, such as transportation, access to free medical care, and physical activity among older adults, and possible interactions among these factors. Such information is imperative in strategic planning for national public health initiatives in geriatric medicine. Implementation of pain management strategies in old-age physical activity promotion programs would also provide space for the geriatric population to enhance physical activity participation.
Several policy implications can be drawn from the results of the study. Older adults of advanced ages seem to be more sedentary than other older adults. Social influences such as physical activity advices from physicians, developing and harnessing natural social networks in urban areas, effective use of mass media to promote culturally relevant physical activity programs that could be adapted to urban living using role models are some of the strategies that could be seriously considered by health policy makers to enhance physical activity and quality of life of urban dwelling older adults in Sri Lanka. Development of health screening programs for older adults to check strength, balance and pain related issues and physical activity surveillance programs would also greatly assist older adult’s physical activity promotion programs to create culture sensitive and cost-effective physical activities of older adults and to enhance behavioral decision making processes of them.
Lack of participation of minor ethnic groups would not allow us to generalize the findings to all urban-dwelling older adults in all ethnic groups in Sri Lanka. Self-reporting measures were used in addition to objective measures; hence, the data may be susceptible to biases such as social desirability. The study was a cross-sectional study, so cause-and-effect relationships cannot be elucidated.
Conclusions
Advanced age, male gender, being in a middle income category, having a lower strength and balance, being an individual suffering from heart diseases or arthritis/joint pain, and having pain or aches were found to be the vital determinants of physical inactivity among older adults in this target population. Improved physical fitness and balance would assist older adults to maintain active lifestyles by enhancing their confidence when engaging in exercise. Chronic diseases, specifically cardiovascular diseases, arthritis, and pain would demotivate older adults to be physically active and physicians should develop practical strategies and good communication methods to promote physical activity in their clients in advanced ages because contentment with their current health status, irrespective of the number of ailments they have, would be a tonic allowing them to lead active and successful lives.
Footnotes
Acknowledgements
We acknowledge all the participants who volunteered in this survey.
Author Contributions
BW: conceptualization, methodology, data collection, analysis, and writing the original draft. SJS: review and editing, supervision. BP: data analyzing, review, and editing the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.