
Abstract
Few studies have investigated the relationship between neuropsychiatric symptoms (NPS) and cognitive status among older Mexican-American adults. Our objective was to describe the NPS of Mexican-Americans 85 years and older according to cognitive status. Data came from Wave 9 (conducted in 2016) of the Hispanic Established Populations for the Epidemiological Study of the Elderly. The final sample consisted of 381 care recipients ≥85 years. The 12-item Neuropsychiatric Inventory was administered to measure NPS among care recipients. Cognitive impairment was defined as a score of ≤18 on the Mini Mental State Exam or by clinical diagnosis of dementia as reported by the caregiver. Logistic regression models were used to estimate the average marginal effect (range = –1 to 1) of cognitive impairment on NPS, controlling for care-recipient characteristics. Overall, 259 (68.0%) participants had one or more NPS. Approximately 87% of care recipients with cognitive impairment had at least one NPS compared to 55.8% of those without cognitive impairment (p < .01). The predicted probability of having one or more NPS was 0.25% points (95% CI = 0.14–0.35) higher for participants with cognitive impairment than those without. NPS are present in the majority of very old Mexican American adults, particularly in those with cognitive impairment.
Keywords
Key Points
Neuropsychiatric symptoms often manifest in dementia and other neurodegenerative disorders. These symptoms can be measured using the Neuropsychiatric Inventory (NPI).
We found that neuropsychiatric symptoms are present in the majority of very old Mexican-American adults, particularly those with cognitive impairment. The prevalence of NPS among cognitively unimpaired participants could imply that they have not been appropriately diagnosed with cognitive impairment or are at risk to be diagnosed at more advanced stages of dementia.
Higher NPI scores have been linked to higher caregiver distress. Recognition and quantification of neuropsychiatric symptoms may lead to effective management of symptoms and reducing caregiver distress in the progression of cognitive decline.
Introduction
Population aging will cause the number of older adults living with Alzheimer’s disease and related dementias to increase (Matthews et al., 2019; Vonk et al., 2019). Dementia is a disease of progressive cognitive impairment and functional decline (McKhann et al., 2011), in which behavioral and psychological changes are often observed (Serra et al., 2010).
The Neuropsychiatric Inventory (NPI) is a widely used tool to measure neuropsychiatric symptoms (Cummings, 2020). The NPI assesses the frequency and severity of symptoms experienced by the care recipient as reported by the caregiver or other informant, along with caregiver burden associated with those symptoms. The NPI has been shown to be valid and reliable in Spanish-speaking countries (Boada et al., 2002). Older adults living with dementia have been shown to have higher NPI scores than those who are cognitively intact or who are cognitively impaired but do not have dementia (Hinton et al., 2003). Although the total prevalence of neuropsychiatric symptoms is similar between Alzheimer’s disease and vascular dementia, the two dementia subtypes differ by presentation of specific symptoms (Fernández-Martínez et al., 2008; Manso-Calderón et al., 2020). Studies have also shown that being female, lower education, and a medical history of psychiatric disorder place individuals at risk for higher frequency and prevalence of neuropsychiatric symptoms (Nagata et al., 2017; Poulin et al., 2017; Steinberg et al., 2006). Higher NPI scores are also associated with increased caregiver burden and an increased risk of being institutionalized (Dufournet et al., 2019; Rote et al., 2015).
Hispanics, particularly Mexican-Americans, are the fastest growing minority group and represent nearly 10% of the US population aged 65 and older (Bureau USC, 2019). Hispanic older adults have a high risk for dementia and have been shown to be diagnosed at more severe stages of dementia than non-Hispanic Whites (Fernandez & Johnson, 2020). Some family members may be reluctant to seek a diagnosis because dementia has a strong, negative stigma in Hispanic culture (Blay & Peluso, 2010; Gray et al., 2009). This is especially true for the behavioral manifestations of dementia (Chavez-Duenas et al., 2020).
However, few studies on the prevalence of neuropsychiatric symptoms among older adults have been conducted in Hispanic populations. An exception is Salazar et al. who used data from Wave 7 (conducted from 2010 to 2011) of the Hispanic Established Populations for the Epidemiologic Study of the Elderly (HEPESE) to show that a majority (62.7%) of community-dwelling older Mexican-American adults age 80 and older experienced one or more neuropsychiatric symptoms (Salazar et al., 2015). Agitation/aggression was the most commonly reported symptom (32%) whereas elation/euphoria was the least frequent (5%) (Salazar et al., 2015).
In our study, we used data from Wave 9 (conducted in 2016) of the HEPESE, in which the participants were 85 years and older, to describe the prevalence of NPS in community-dwelling Mexican-Americans. We build on the study by Salazar et al. by describing the frequency of neuropsychiatric symptoms according to the cognitive status of the care recipient. We hypothesize that the majority of older Mexican-American adults will have one or more neuropsychiatric symptoms and that those classified as cognitively impaired will experience more neuropsychiatric symptoms than their counterparts who are not classified as cognitively impaired.
Methods
Data and Sample Population
Data came from Wave 9 (2016) of the HEPESE. The HEPESE is an ongoing, longitudinal study of Mexican-Americans living in the southwestern United States (Markides et al., 1997). The HEPESE began in 1993/94 and included a cohort of 3,050 participants who were representative of the Mexican-American population aged 65 and older living in Texas, Colorado, New Mexico, Arizona, and California. Participants have been interviewed approximately every 2 to 4 years. The most recent wave of data collection (Wave 9) was completed in 2016.
At Wave 7 (2010/11), 925 of the surviving 1,078 participants gave the name and contact information for the person they were closest to or depended on the most for help (Rote et al., 2015). These 925 informants were interviewed on the health, daily function, living situation, and mental status of the respondent as well as their own health characteristics. Participants were asked again at Wave 9 to provide the name of the person they were closest to or depended on the most for help. Participants could give the name and contact information for the same or different person than who they named at Wave 7.
Figure 1 presents the selection of the final analytical sample. A total of 480 participants were interviewed at Wave 9 of which 460 provided the name and contact information for an informant. We excluded 55 participants who did not attempt or complete the Mini Mental State Exam (MMSE) and did not have information for having ever been diagnosed with Alzheimer’s disease as reported by the informant. We then removed 24 participants who were missing information for demographic and health characteristics (see Covariates). The final sample included 381 participant-informant dyads.

Selection of the final analytic sample.
Measures
Cognitive status
Cognitive functioning was measured using the MMSE (Folstein et al., 1975). The MMSE includes items for orientation to time and place, attention, registration, recall, and language and praxis. The total score for the MMSE ranges from 0 to 30 with higher scores indicating better cognitive functioning. Participants can attempt the MMSE in English or Spanish in accordance with their preference for the language of interview. Because of the old age of the HEPESE participants interviewed at Wave 9 and generally low educational attainment of the cohort, participants who scored lower than 18 points on the MMSE were classified as cognitively impaired (Downer et al., 2016b).
Thirty-five participants in the final sample did not attempt or complete the MMSE. The cognitive status of these participants was determined by the informant’s response when asked if the target participant had ever been diagnosed with Alzheimer’s disease. Participants were classified as cognitively impaired if the informant reported that the participant had ever been diagnosed with Alzheimer’s disease.
Neuropsychiatric symptoms
The Neuropsychiatric Inventory (NPI) was used to determine the presence and absence of neuropsychiatric symptoms as reported by the informant (Cummings et al., 1994). The NPI includes 12 symptoms: delusions, hallucinations, agitation, dysphoria, anxiety, elation, apathy, disinhibition, irritability, motor disturbances (e.g., repetitive behaviors), nighttime behaviors (e.g., waking early in the morning, excessive naps), and changes in appetite. The informant can respond as yes or no according to if the symptom occurred in the past month.
We used the NPI items to create three outcomes. First, we created a dichotomous variable that identified participants who were reported to have experienced 1 or more NPI symptoms in the past month. Second, we examined each NPI symptom as a separate, dichotomous outcome. Third, we calculated the total number of NPI symptoms that the participant was reported to have experienced in the past month. This variable was a continuous measure with a total score that could range from 0 to 12 points.
Covariates
Selected covariates included care recipients’ demographic, health, and functional characteristics as reported by the informant. Demographic characteristics included age, sex, years of education, and marital status. We also created a variable describing the care recipient’s relationship to the informant. This variable was categorized as son or daughter, friend or paid employee, and other family member (e.g., spouse, sibling, nephew/niece, grandchild, great grandchild). Health conditions included having ever been diagnosed by a physician with arthritis, cancer, heart attack, stroke, hypertension, diabetes, hip fracture, and if the participant reported having pain while walking. Informants were also asked if the care recipient needed help with activities of daily living (ADLs) and instrumental ADLs (IADLs). ADLs included walking across a room, bathing, personal grooming, dressing, eating, moving from a bed to a chair, and toileting. IADLs included using a telephone, driving or using transportation, cooking a hot meal, shopping, doing light cleaning, and taking medications. The number of ADL limitations was categorized as 0 limitations, 1 to 3 limitations, and 4 or more limitations. The number if IADL limitations was categorized as 0 to 1 limitations, 2 to 4 limitations, and 5 to 6 limitations.
Statistical Analysis
Independent sample t-tests and chi-square tests were used to describe the 381 care recipients included in the final sample by cognitive status. Logistic regression was used to model the association between cognitive status and one or more NPI symptoms. For easier interpretation, we present the results as the average marginal effect. The average marginal effect is interpreted as the difference in the predicted probability for one or more neuropsychiatric symptoms for care recipients with cognitive impairment compared to care recipients without cognitive impairment. Logistic regression models were also used to estimate the average marginal effect of cognitive impairment on individual neuropsychiatric symptoms. Finally, negative binomial regression was used to model the association between cognitive status and number of NPI symptoms. We used this model to estimate the predicted number of neuropsychiatric symptoms for care recipients with and without cognitive impairment. All analyses controlled for care recipients’ demographic, health, and functional characteristics.
Results
Sample Characteristics
Table 1 shows the demographic and health characteristics of the 381 care recipients. The mean age of the total sample was 90.2 years and 65.4% were female. The majority were widowed (66.7%) and most of their caregivers were their sons/daughters (61.9%). Their average number of years of educational attainment was 5.2 years. Most caregivers reported that the care recipients had health problems, such as arthritis, hypertension, and pain upon walking. Approximately, 41.5% had no limitations in ADLs whereas 43.8% reported five or more limitations in IADLs. Of the 381 care recipients, 148 were classified as cognitively impaired. Approximately 60.0% of care recipients with cognitive impairment had limitations in four or more ADLs and 81.1% had limitations in five or more IADLs as reported by the caregiver. Fifteen percent of care recipients who were cognitively intact had limitations in four or more ADLs and 20.2% had limitations in five or more IADLs.
Descriptive Characteristics of Older Mexican-American Care Recipients by Cognitive Status.

Note. Differences in care recipient characteristics were determined using independent t-tests and chi-square tests. SD = standard deviation; ADL = activities of daily living; IADL = instrumental activities of daily living.
Bold p < .05.
Figure 2 shows the percentage of care recipients experiencing any neuropsychiatric symptoms and each neuropsychiatric symptom by cognitive status. Overall, 68.0% of care recipients had one or more neuropsychiatric symptoms. Agitation, apathy, and irritability were the most common symptoms. Approximately 87% of care recipients with cognitive impairment had one or more symptoms compared to 55.8% of care recipients without cognitive impairment (p < .01). Every neuropsychiatric symptom was more common among care recipients with cognitive impairment than those without cognitive impairment.

Frequency of neuropsychiatric symptoms among older Mexican-Americans with and without cognitive impairment.
Cognitive Impairment in Association with One or More NPI Symptoms
Table 2 shows the average marginal effect (AME) of cognitive impairment on the presence of one or more NPI symptoms, adjusting for care recipient characteristics. The predicted probability for participants with cognitive impairment to have one or more neuropsychiatric symptoms was 0.25 (95% CI = 0.14–0.35) percentage points higher than participants who were not cognitively impaired. Participants with four or more ADL limitations had a predicted probability of 0.17% points (95% CI = 0.02–0.32) higher to have one or more neuropsychiatric symptoms than those with less than four limitations.
Average Marginal Effects (AME) of Care Recipient Characteristics on the Presence of One or More Neuropsychiatric Symptoms as Reported by the Caregiver.
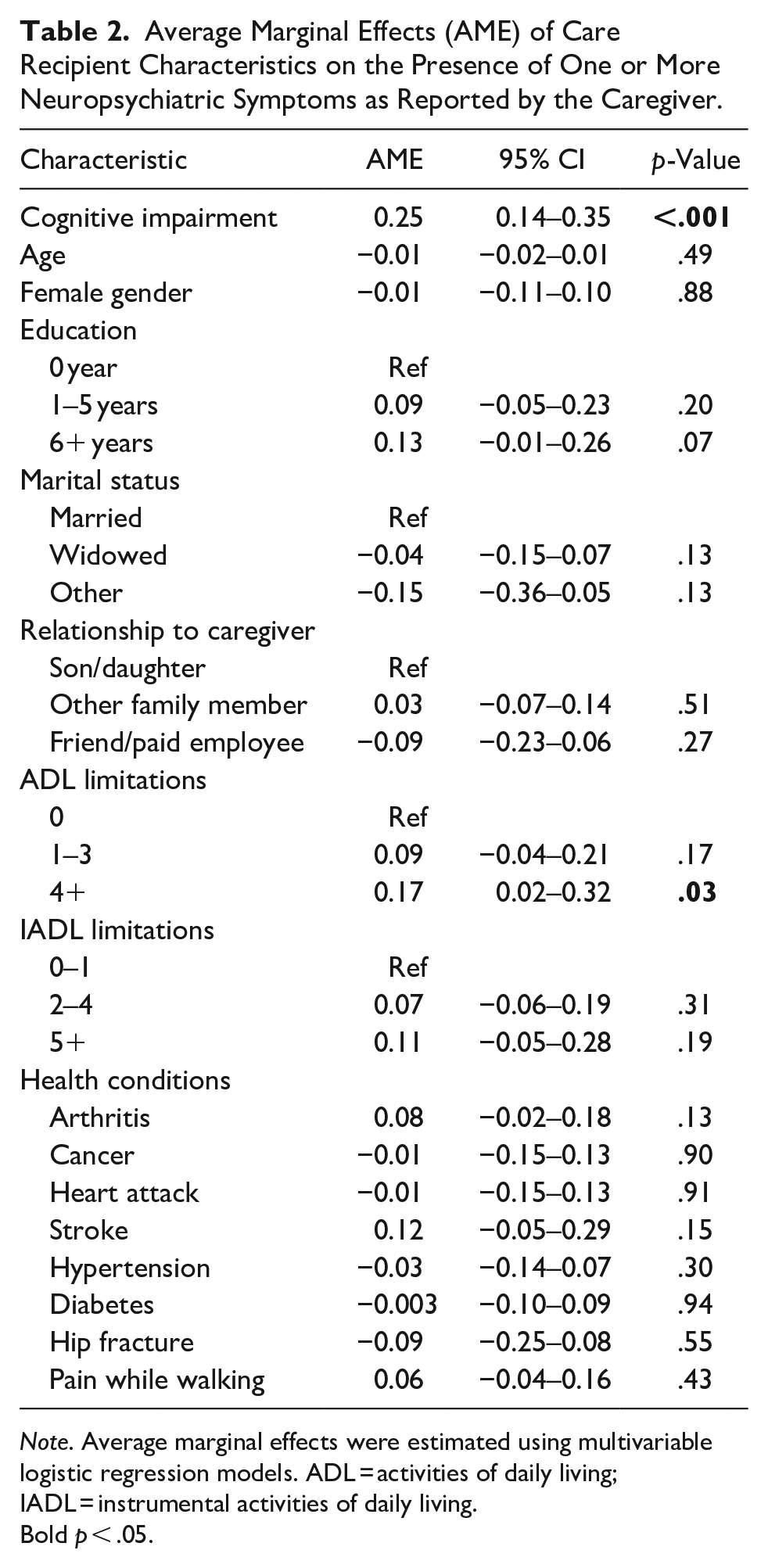
Note. Average marginal effects were estimated using multivariable logistic regression models. ADL = activities of daily living; IADL = instrumental activities of daily living.
Bold p < .05.
Cognitive Impairment in Association with Individual Neuropsychological Symptoms
Figure 3 presents the AME of cognitive impairment on each neuropsychiatric symptom. With the exception of dysphoria, impulsiveness, and elation, care recipients with cognitive impairment have a significantly higher predicted probability of experiencing each of the remaining nine neuropsychiatric symptoms. The AME ranged from 0.09 (95% CI = 0.01–0.16) for hallucinations to 0.22 (95% CI = 0.09–0.34) for irritability.

Association between cognitive status and neuropsychiatric symptoms.
Predicted Number of NPI Symptoms by Cognitive Status
Table 3 shows the average predicted number of neuropsychiatric symptoms according to care recipient characteristics. The average number of neuropsychiatric symptoms for participants who were cognitively impaired was 3.84 compared to 1.64 for those who were cognitively intact. This difference was not statistically significant.
Association between Care Recipient Characteristics and the Average Predicted Number of Neuropsychiatric Symptoms.
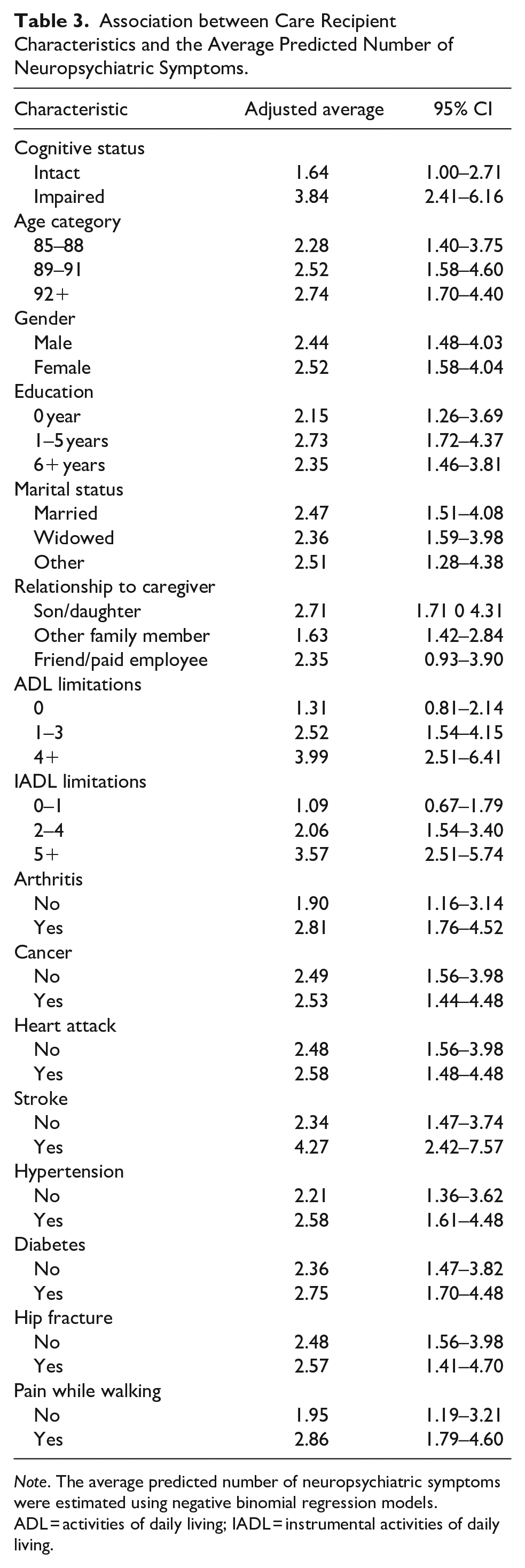
Note. The average predicted number of neuropsychiatric symptoms were estimated using negative binomial regression models. ADL = activities of daily living; IADL = instrumental activities of daily living.
Discussion
Few studies have investigated the presence of neuropsychiatric symptoms among older Mexican-American adults with and without cognitive impairment. Using data from wave 9 of the HEPESE, we found that neuropsychiatric symptoms were present in the majority of Mexican-American adults aged 85 and older. Studies that have used data from predominately non-Hispanic White cohorts of older adults have reported that 75% to 90% of older adults with dementia experience one or more neuropsychiatric symptoms (Aarsland et al., 2007; Lyketsos et al., 2002; Zuidema et al., 2007).
The prevalence of one or more neuropsychiatric symptoms as well as the individual symptoms in our analysis are consistent with the analysis by Salazar and colleagues, which used data from wave 7 of the HEPESE and included participants aged 80 years and older. Salazar et al. reported that nearly 63% of participants had one or more neuropsychiatric symptoms, with aggression/agitation being the most frequently reported (32%) and euphoria/elation being the least frequent (5%). Sixty-eight percent of all care recipients in our analysis had one or more neuropsychiatric symptoms and agitation/aggression and euphoria/elation were also the most (34.4%) and least (7.1%) common symptoms, respectively. The slight differences in the prevalence of neuropsychiatric symptoms detected in our analysis and Salazar et al. are likely due to the older average age and lower cognitive functioning of care recipients in our sample.
Nearly 39% of participants in our sample were cognitively impaired of which 87.2% had one or more neuropsychiatric symptoms. In another longitudinal Hispanic cohort, higher NPI scores were also associated with cognitive and functional decline (Hinton et al., 2008). Prior studies of ethnically diverse oldest-old populations have shown that rates of depression and the prevalence of neuropsychiatric symptoms increased with age, with apathy and agitation/aggression being the most common symptoms and disinhibition the least (Melikyan et al., 2019; Sampson et al., 2018). Neuropsychiatric symptoms have been traditionally viewed as outcomes of dementia, but more recent studies suggest that NPI scores may predict the severity of cognitive impairment and be a symptom for older adults who progress from mild cognitive impairment to dementia (Acosta et al., 2018; Mallo et al., 2020).
Particular neuropsychiatric symptoms may be more prevalent in different types of dementias (D’Onofrio et al., 2012; Fernández-Martínez et al., 2008; Fitten et al., 2001; Manso-Calderón et al., 2020; Savulich et al., 2020). Older adults with Alzheimer’s disease typically have higher NPI total scores and a higher prevalence of appetite changes, aberrant motor behaviors, delusions, and hallucinations than older adults with vascular dementia (Manso-Calderón et al., 2020). Older adults with Alzheimer’s disease and vascular dementia both experience high rates of anxiety and sleep disturbances, but those with vascular dementia are more likely to experience apathy, euphoria, and irritability (Fernández-Martínez et al., 2008). We observed that care recipients with cognitive impairment were more likely to experience nine of the neuropsychiatric symptoms. Among these nine symptoms, irritability had the strongest association and may give some evidence that vascular dementia is more common among H-EPESE participants with cognitive impairment. Interestingly, there has been a higher increase in the prevalence of vascular dementia than Alzheimer’s disease in Hispanic populations (Fitten et al., 2001). This may be due in part to the high prevalence of hypertension and type II diabetes among older Hispanics of which are both associated with an increased risk for vascular dementia (Bangen et al., 2015; Downer et al., 2016a; Stickel et al., 2019).
Previous studies have noted that higher severity in each symptom was correlated to more advanced stages of dementia. Rather than total number of neuropsychiatric symptoms, caregiver distress has been correlated to the prevalence of certain symptom clusters; namely, depressive symptoms, agitation, and aberrant motor behaviors have been associated with higher levels of caregiver burden (Okura & Langa, 2011; Tsai et al., 2020). Studies focusing on caregiver burden have found increasing distress from neuropsychiatric symptoms in the mood cluster, which include depression, apathy, and irritability (Hinton et al., 2003; Rote et al., 2015). Studies have also shown that concurrent functional disabilities in older adults with dementia increase caregiver distress (Lima-Silva et al., 2015). To improve or lessen their stress as the dementia progresses, caregivers, who are usually among the care recipient’s relatives, should be informed and educated on the presence of neuropsychiatric symptoms and how to approach them in the care plan.
Neuropsychiatric symptoms have also been associated with pre-clinical dementia. The high prevalence of neuropsychiatric symptoms among care recipients who were cognitively unimpaired could imply that either a large portion of the older adults have not been appropriately diagnosed with dementia or are at a higher risk to soon develop dementia. Our current study does not include adequate data to comment further on that possibility, but previous studies have shown that Hispanics may have a delayed diagnosis or are diagnosed with dementia at more advanced stages than their non-Hispanic counterparts (Fitten et al., 2014; Ramirez Gomez et al., 2017).
Our study has limitations. First, most care recipients were classified as cognitively impaired or cognitively unimpaired according to the MMSE. The MMSE is a widely used cognitive testing tool and it has been validated in clinical settings and in Hispanic populations (Norris et al., 2016). However, studies have shown that the MMSE can misclassify cognitive status of older with low levels of education and those of more advanced ages (Tsoi et al., 2015). Second, the HEPESE consists of only Mexican-Americans and our findings may not be generalized to other Hispanic populations. Finally, our sample size was relatively small, which may have reduced our statistical power to identify other care recipient characteristics associated with NPI symptoms. Despite these limitations, consideration needs to be given to the prevalent health conditions and neuropsychiatric symptoms of this age group since they differ from younger geriatric age groups, such as increased depression and decreased ADLs.
In summary, neuropsychiatric symptoms are present in the majority of both cognitively impaired and cognitively intact Mexican-Americans at very advanced ages, but are more prevalent in the former. The most common neuropsychiatric symptoms are consistent with mood changes, which have been associated with higher levels of caregiver distress. Future studies should investigate the progression of cognitive decline in association with changes in neuropsychiatric symptoms among those care recipients who are cognitively unimpaired to assess the cause of neuropsychiatric symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was was supported by the National Institute on Aging at the National Institutes of Health (grant numbers P30AG024832, P30AG059301, R01AG010939, K01AG058789).