
Abstract
Intelligent voice assistants (IVAs) such as Amazon Echo and Google Home present a promising opportunity to improve access to consumer health information and resources for older adults. However, researchers know little about older adults’ opinions of using IVAs for these potentially critical tasks, particularly those with already limited access. In this paper, we explore older adults’ views about IVAs for consumer health and wellness information with the goal of better understanding what they envision as benefits and barriers of using such technology in the future. We shared an IVA prototype with ten older adults (60 years of age or older). We interviewed them about how a similar system might impact their access to consumer health information. Participants saw the potential for IVAs to improve their search experiences and support them with other health tasks. However, participants were also concerned about adopting an IVA for health due to access barriers, confidentiality risks, and concerns about receiving trusted information. Based on our findings, we discuss considerations for designing IVAs for underserved, older adult populations.
Introduction
There has been growing interest in using intelligent voice assistants (IVAs), such as Amazon Echo and Google Home, to support older adults (Buinhas et al., 2019; Pradhan et al., 2019; Reis et al., 2018; Sanders & Martin-Hammond, 2019; Sayago et al., 2019; Trajkova & Martin-Hammond, 2020) at home for health-related and non-health-related tasks. IVAs (e.g., smart speakers) use “conversational-like” interactions to allow users to perform tasks using their voice or text and can be less expensive than other computing devices. Most IVAs provide functionality that allows users to search for information, including disease or medication information. IVAs, therefore, present an opportunity to support older adults with health information tasks by addressing some of the challenges they may face due to digital literacy (Fang et al., 2018). While some suggest that commercial IVAs may not be suitable for health information search (Bickmore et al., 2018), there is emerging interest in IVAs and other intelligent assistants to support older adults with health (Buinhas et al., 2019; Reis et al., 2018; Sanders & Martin-Hammond, 2019) and health information (Martin-Hammond et al., 2019). However, these studies are few, particularly among older adults who already have less access to existing online consumer health resources (Choi & DiNitto, 2013; Fang et al., 2018; Waterworth & Honey, 2018). Therefore, significant gaps exist regarding whether the introduction of IVAs as a tool might improve or hinder access to healthcare among underserved groups of older adults and their perceptions of potentially using IVAs to support their health information processes.
To better understand older adults’ views of a potential IVA for health, we interviewed 10 low-income older adults about their recent experiences finding health information to support them at home. We used an IVA prototype to elicit discussions among participants of how a future IVA device for health may assist them. We asked about their concerns for using IVAs for health and how a similar IVA technology might benefit or hinder their access to health information and resources. Our study addresses the following research questions:
RQ1: How do lower-income older adults perceive IVAs for health, and how might a future version of this technology assist them with access to healthcare information at home?
RQ2: What are the potential barriers to health-related IVA adoption among lower-income older adults?
Our findings suggest that low-income older adults see potential benefits of adopting IVAs for health. However, we must further examine inequalities in digital access and the ethical concerns surrounding that adoption.
Background and Related Work
Socio-demographic characteristics such as age, education, and income can significantly affect an individual’s access to health information and resources (Estacio et al., 2019). The internet and digital technologies broaden the availability of health information and resources for many individuals (Estacio et al., 2019; Fang et al., 2018; McAuley, 2014) and improve health outcomes and patient engagement (Pluye et al., 2013; Suziedelyte, 2012). However, some public health researchers note concerns about digital health interventions’ impact on increasing existing health inequities (Estacio et al., 2019; McAuley, 2014). Seeking health information online remains much lower for older adults and other underserved groups (Estacio et al., 2019; Fang et al., 2018; McAuley, 2014; McCloud et al., 2016). Some believe that while digital health interventions improve access to health information and services for both vulnerable populations of older adults and individuals with low socioeconomic resources, these technologies can widen the gap between those with and without access (Fang et al., 2018; McAuley, 2014).
Older age and lower-income levels are known factors that impact access to online health resources. For some older adults, one well-known barrier to accessing online health information or any other type of information is limited or zero technical skill (Choi & DiNitto, 2013; Fang et al., 2018). However, apart from technical skills, some older adults also tend to access online health information and other e-health resources less often than those with higher incomes (Choi & DiNitto, 2013; Fang et al., 2018; Waterworth & Honey, 2018). Choi and DiNitto (2013) found less internet use among those 60 years of age or older with lower incomes due to lack of exposure, financial resources, or medical condition/disability. Waterworth and Honey’s (2018) results suggest that while older adults use the internet more often to access health information, usage is more likely among those older adults with higher incomes. Therefore, barriers exist for lower-income older adults when accessing information online.
While the usefulness of voice for supporting older adults’ interactions with technology is not always apparent (Luria et al., 2017; Portet et al., 2013; Vacher et al., n.d.), older adults often appreciate the simplified interactions of voice-controlled devices, especially among those with limited technical experience (Wulf et al., 2014). Researchers are increasingly exploring IVAs as tools to support aging (Pradhan et al., 2018, 2019; Reis et al., 2018; Trajkova & Martin-Hammond, 2020), including supporting older adults’ healthcare needs (Buinhas et al., 2019; O’Brien et al., 2020; Sanders & Martin-Hammond, 2019). There are genuine concerns that commercial IVAs may not yet be ready to support consumers’ health information needs (Bickmore et al., 2018) or the complexities of the healthcare system (Sezgin et al., 2020). However, despite concerns, we see increased interest in voice technologies (Pew Research Center, n.d.) and their use in healthcare (Laranjo et al., 2018; Sezgin et al., 2020) with a recent focus on older adults. Buinhas et al. (2019), for example, examined prototypes to assist older adults in managing diabetes. Several other researchers have also begun to study the future of IVAs to support older adults’ health and wellness needs (Buinhas et al., 2019; O’Brien et al., 2020; Sanders & Martin-Hammond, 2019). Yet, we still know little about users’ perspectives on the future of IVAs for health, particularly among those that might benefit from alternative ways of access health information
Methods
We designed a prototype inspired by current off-the-shelf IVAs on the market, such as Amazon Echo and Google Home. We employed a prototype instead of a developed solution to (1) explore scenarios not yet supported by commercial IVAs and (2) not constrain our discussions to the current capabilities of retail IVAs. For example, commercial IVAs do not currently support conversational interactions (Ahire & Rohs, 2020), restrict access to personal health information without approval (Jiang, n.d.), and are not designed for supporting the healthcare tasks we explored in our study. Scenario-based design approaches (Rosson & Carroll, 2002) informed our method. We used scenarios and a Wizard of Oz (WOZ) approach to simulate interactions with a future IVA. The prototype included a physical enclosure made of cardboard and a Bluetooth speaker that was placed inside (Figure 1). We used Bot Society (https://botsociety.io/), a software tool for prototyping conversational agents, to simulate the IVA interactions.

Example of Wizard of Oz (WOZ) setup.
We collaborated with a local subsidized public apartment community that provides affordable housing options for older adults and individuals at least 58 years of age living with a disability. Participants were required to be 60 years of age or older and living independently. The study was reviewed and approved by the Institutional Review Board at Indiana University before recruitment and data collection began.
In three months, we recruited 14 participants from the community. However, four participants discontinued the study because although they thought the approach was useful, they felt it might be challenging to learn. Ten older adults completed the study (Figure 2). Participants’ ages ranged from 60 to 76 years (AVG = 67, SD ~ 5). All participants had household incomes of less than USD 20,000 a year. Five participants self-reported that they viewed themselves as relatively healthy. Of those five, three reported chronic illnesses such as diabetes or sleep disorders. Four participants were neutral about their health, and one participant rated herself as not so healthy.

Participants were mostly retired and had limited experiences using IVAs (Voice Assistant Use).
After completing a background survey, we asked participants questions about their current processes and challenges of finding health information and making health decisions at home. We asked participants to use the prototype (Gaver et al., 2004) and to guide interactions; we provided participants with two scenarios that included a fictional character’s medical background and goals for completing a health task (Figure 3). Participants also followed a script (Figure 4) to engage in a two-way dialog with the IVA to complete each of the two tasks. As participants followed the “user” portion, a researcher playing a wizard used a computer to provide the appropriate “system” response. The participants received only the “user” portion of the script (Figure 3). To be consistent across the study, we provided each participant with the same scenarios and script.
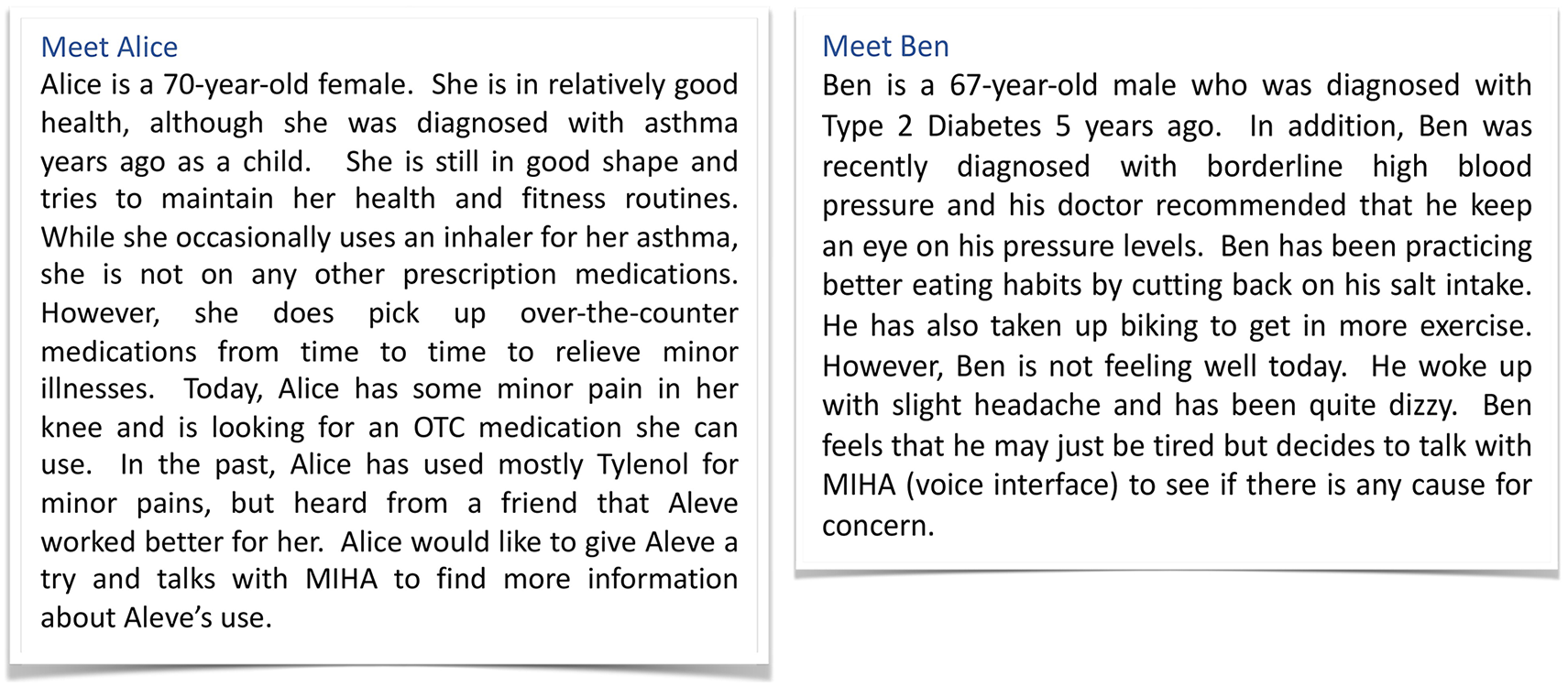
Two scenarios used to elicit discussion about the potential for IVAs for health.
We used prior work on the common reasons why older adults search for health information online to inform the scenarios and the types of assistance included (Medlock et al., 2015). We presented three types of assistance through the IVA prototype. Informational/Educational assistance represented fact-based responses typically found by searching a trusted online health-related website (Figure 4). Generic recommendations were similar to fact-based answers but also provided advice. Personalized recommendations attempted to reason and make recommendations based on the users’ health history.
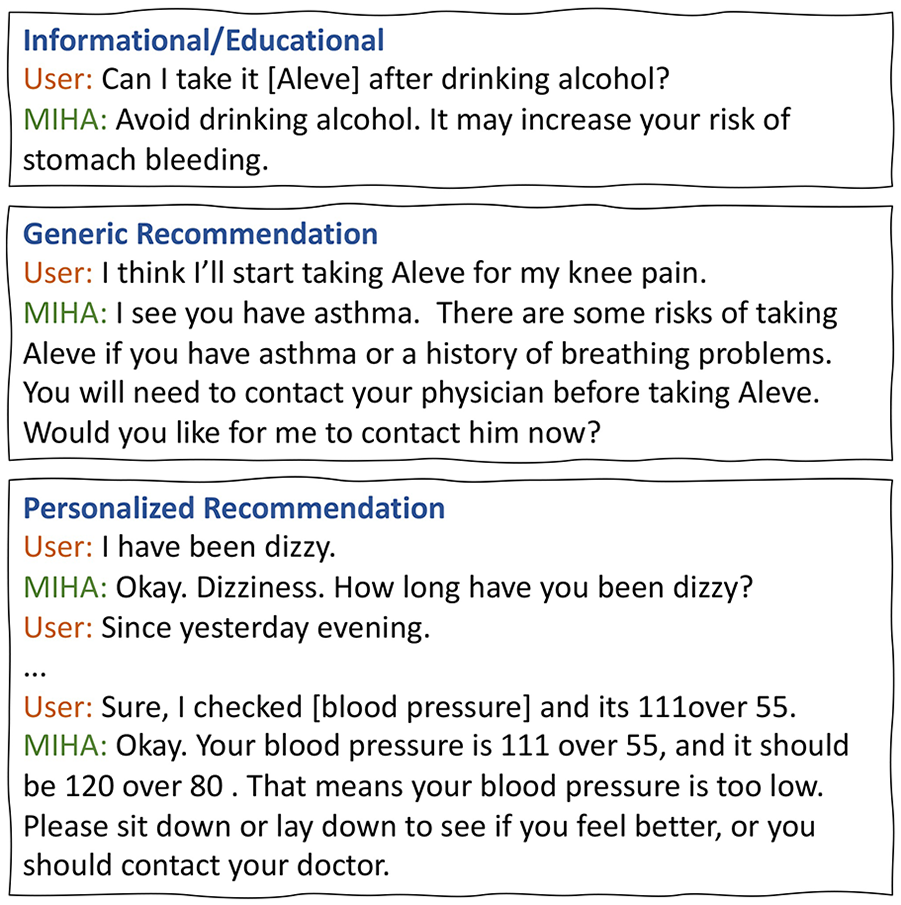
Types of assistance simulated in the prototype and example participant scripts.
After completing the scenarios, we asked participants their opinions about how they anticipate integrating an IVA for health in their homes might benefit them and their concerns about adopting such a device. Participants received a $20 gift card at the end of the study for their time.
We recorded and transcribed all interview sessions. Four researchers analyzed the data, two of which conducted interviews, by independently reviewing each transcript, and using an open coding approach to make marginal notes of emerging themes (Corbin et al., 2015). After reviewing all transcripts, we met several times to compare independent codes and used affinity diagramming (Blandford et al., 2016; Martin et al., 2012) to reconcile themes with similar descriptions into categories. From this process, we developed an initial set of themes and codes (i.e., codebook) and applied those codes to the transcripts. The analysis resulted in two high-level themes: (1) Perceived Benefits and (2) Perceived Barriers and six low-level codes corresponding to the specific benefits and barriers discussed in the results.
Results
Participants shared what they felt were the benefits and barriers of adopting an IVA for health in their home, emphasizing that they would still prefer advice from a trusted healthcare provider over any online information source. However, participants saw potential value in using IVAs to supplement that advice and improve access to resources if they could be designed to address their needs.
Perceived Benefits of an IVA for Health
All participants felt that an IVA could help them with general research on illnesses or medications and ease some of the challenges they faced in the current online search process. All but one participant currently used the Internet to supplement doctor’s advice (Figure 5), and of those that searched for information online, most searched for information about medications (Figure 6a). Most participants relied on their smartphone (n = 9) to search for information online due to portability or lack of Internet in their homes (Figure 6b).

Health information-seeking resources participants use.

(a) Topics participants search and (b) devices used to search.
Most commercial IVAs can provide some basic support for searching for health information, but recent studies have raised safety concerns about the information provided by these applications (Bickmore et al., 2018). Nevertheless, participants felt that this type of search would be beneficial to them. P2 shared that she was involved in medical billings and was comfortable searching for health information online. But she stated, “I’m blind in one eye. I’m visually impaired, so when you start doing these kinds of things [searches], you can get lost in reading, and my eyes get a little tired.”
Many commercial IVAs are currently not approved to provide medical recommendations or collect health data, although a small subset of applications has obtained necessary approvals (Jiang, n.d.). However, four participants discussed that they could see an IVA as useful to help with general decisions (e.g., recommending a medication) based on a verified fact. Six participants wanted additional personalization capabilities that could provide recommendations based on knowledge of their health. P9 gave an example of how the IVA might help them discern whether they should eat a particular food, “Ok, can you ask it questions about being overweight? Can it give you any type of information about that . . . like types of foods I should eat?”
Participants also discussed other situations in which they felt an IVA might be useful for them to manage their health apart from the ones presented in the scenarios. For example, participants shared their past hesitancy in contacting a doctor without good reason, considering the potential financial cost of what they believed would be an unnecessary trip to the doctor. P7 stated, “I think it’ll be able to help me [decide] whether I need to contact a doctor because I may be having symptoms of something that may be serious or that may be nothing at all. It may be side effects of medication, or something that all I need to do is relax or lay down or something. Although with my health, some things always come up with me. [But] like, you know [the IVA can help with] some simple aches and pains.” Therefore, participants discussed how an IVA for health might help decide whether to seek health services when ill.
Participants also felt that an IVA might assist them with obtaining emergency assistance. While some commercial IVA companies do not permit emergency assistance on their devices, participants viewed this as useful. P3 shared, “I do live alone, and because of the fact I do not have ready friends that can get to me. There’s the deacon at my church . . . And because I can’t utilize the outside network in terms of people to come to my aid, this would help me a lot . . . I’ve lived here for only three years, and I’ve fallen in my apartment five times – no four times. The last time I fell, I had to scoot. You’re not supposed to do that [get on your knees], and I had to knock the phone off the stand and grab it and call 911.” P3 shared that they had an alert device, but he would prefer a more integrated solution that was free, lower cost, or provided more functionality for the monthly fee.
Perceived Barriers to Adopting an IVA for Health
Participants were aware that they might need to share some part of their medical history for an IVA to provide any personalized information or recommendations. All participants, therefore, discussed potential concerns about keeping their data confidential. P3 stated, “If it [the medical data] was something very private and personal to the point where you don’t want that information leaking out, then I would say [share with] the doctor only. . . I have concerns in terms of what particular network will have all my health information because that can keep me from getting life insurance.” For these reasons, half of the participants suggested an IVA that served as a dedicated health device instead of a commercial tool such as Echo or Siri to provide greater flexibility for supporting their privacy and confidentiality needs regarding their health data. P6 stated, “This [the prototype] is pretty good. Siri answers everything but this answers medical ones. You need something for medical.” suggesting that commercial IVAs might not provide the confidentiality they desire.
Participants also expressed concerns about the trustworthiness of the information provided by an IVA for health. P1 voiced concern about whether the system would have up-to-date medical information when providing recommendations. He stated, “I suppose it could be potentially [risky] if it didn’t update constantly. Like the doctors and nurses everybody [would] have the update on it continually so the system would know what the drug interactions will be and side effects and all.” P2 raised similar concerns; she stated, “Well I think, one risk might be that they don’t [the user] give all symptoms. They’ll [the person managing the data] may give only partial symptoms and they [the system] got only half of the information. That could be the only problem I could see.” Therefore, while participants believed an IVA might provide improved access to health information at home, there were still genuine concerns about determining whether they could trust the data an IVA provided.
While participants had no general concerns about the affordability of retail IVAs, several participants raised concerns about what they perceived would be a constant need for an Internet connection. P2 stated, “Only thing is . . . what if the internet gets cut off? You know, you don’t have internet then that’s gonna be a problem. You gotta take this to a place that’s got a hotspot. Starbucks they would let you [use the Wi-Fi] but other than that, you know, you just gotta constantly keep your Wi-Fi up.” Several participants also did not use the internet often or have access to Broadband internet in their homes. Some shared that they would sometimes visit restaurants with free hotspots to limit the cost of maintaining Internet services in the home. P10 stated, “There must be some [assistance]. . . I think this should be [able to be used] alone without internet too. Because older adults [some], they can’t use internet and they [too] don’t know how to keep track of medicine. I think this is such an excellent idea for them for that reason. I think it’s excellent for someone not inclined to the internet and that stuff.” Both P10 and P2 had access to Wi-Fi in their homes at the time of the study; therefore, concerns were not limited to participants without internet access currently.
Discussion
Achieving equal access to digital resources represents one step for improving health outcomes. The National Academies of Sciences (2016) notes the following: “If the benefits of technology flow disproportionately to those who already enjoy better coverage, use, and outcomes than disadvantaged groups, health disparities could increase. But if technologies can be developed and implemented in such a way as to improve access and enhance quality for the members of all groups, the ongoing transformation of health care could reduce the gaps among groups while improving health care for all.” (p. 1).
Our findings suggest that while most participants saw the potential for a future IVA to improve their access to consumer health information and resources at home, concerns about access remain. Some tasks mentioned by participants, such as delivering personalized recommendations or decision support, are currently unavailable in commercial IVAs, while others are already available or known (Demiris et al., 2004, 2008; O’Brien et al., 2020; Reis et al., 2018). However, the question remains of how to ensure that we design IVAs for health equitably (Harrington et al., 2019; Harrington, 2020; Laura Ramí-rez Galleguillos & Coşkun, 2020) and in ways that are inclusive of those that might otherwise be further disadvantaged by lack of access to these technologies.
Like prior work, our findings suggest a need to explore approaches to design IVA interfaces in ways that support diverse users and contexts (Abdolrahmani et al., 2018; Demiris et al., 2004; Pradhan et al., 2018). Several participants, including those with internet access in their homes, expressed concerns about the need to sustain Internet services to maintain an IVA device in their home. It will be critical to look at ways to increase necessary access to digital resources, such as the Internet, to improve access to IVAs and other emerging health technologies. While some IVAs are portable (e.g., Siri), most are designed for in-home use, limiting access among users that rely on other ways of accessing the Internet (e.g., free hotspots in the community or the Library). Most participants in our study preferred mobile phones for searching for health for these reasons. We know that users are much less comfortable interacting with IVAs in public places (Lopatovska et al., 2019; Moorthy & Vu, 2015). Therefore, we must also explore designs that can support health information tasks using sporadic internet connections or through mobile connections in the future to address access gaps. For example, some are exploring IVA design approaches in resource-constrained environments (Pearson et al., 2019). We may also consider IVAs that allow for asynchronous voice interactions to allow users to manage internet access more easily.
Privacy and trust are known concerns in the study of IVA users (Bonilla & Martin-Hammond, 2020; Cowan et al., 2017; Ianzito, n.d.; Liao et al., 2019; Moorthy & Vu, 2015; Vacher et al., n.d.; Wulf et al., 2014), and our analysis suggests similar concerns of IVAs used for health. Therefore, this work extends prior work with physicians that raise concerns about using commercial IVAs for health (Bickmore et al., 2018), adding that older adult consumers share concerns about using IVAs to inform their health decisions. Our participants expressed hesitancy in trusting IVA health recommendations and discuss practical approaches for addressing concerns, such as using a dedicated device instead of an off-the-shelf device. However, it may also be beneficial to explore features to minimize errors, increase trustworthiness, and transparency to help users decide whether to follow the advice (Eiband et al., 2018). Similar to prior findings (Seifert et al., 2018), participants felt automatically transferring data from an electronic health record or adding healthcare providers in the process could address their concerns. Accessing personal health data presents future opportunities to provide personalization features. Companies such as Amazon are already exploring how to increase IVAs functionality in healthcare (Jiang, n.d.). Yet, this brings to question broader issues around privacy and data access. Therefore, it will be essential to examine the ethical implications of inequitable access to resources and those that may occur due to misinformation, miscommunication, and privacy violations.
Limitations
Most of our participants were considered young-old (60–75 years of age), self-identified as female, low income in the United States, and had little experience with commercial IVAs. While we provide a detailed description of our study to help contextualize our findings, the opinions and needs regarding IVAs for health may vary for other participant characteristics and contexts. We anticipate our findings will apply to different populations, but additional work is needed to understand similarities and differences.
Conclusion and Future Work
We conducted a semi-structured interview with 10 low-income older adults where we introduced an IVA prototype for health. We found that participants perceived IVAs that help them with health information search tasks and decisions as beneficial. However, participants had concerns about privacy, trusting the information provided by an IVA, and maintaining the s technical resources needed to support an IVA. Based on our findings, we discuss considerations for the future design IVAs for health among underserved populations of older adults.
Footnotes
Acknowledgements
We would like to thank our community partners and our participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.