
Abstract
Objectives:
This study examined the mediation role of fear of COVID-19 in the association between perceived health status of older adults and their insomnia, mental health, and COVID-19 preventive behaviors so as to have better understanding of the factors associated with COVID-19 and its preventive measures.
Methods:
A total of 413 older adults with a mean age of 57.72 (SD = 7.31) were recruited for this study. They responded to the measures on fear of COVID-19, insomnia, mental health, and COVID-19 preventive behaviors.
Results:
There were small-large significant interrelationships between insomnia, mental health, fear of COVID-19, and preventive behaviors. Fear of COVID-19 significantly mediated the associations between perceived health status and insomnia, mental health, and COVID-19 preventive behaviors. It was also observed that perceived health status directly influenced insomnia and mental health of older adults but not their COVID-19 preventive behaviors.
Conclusion:
Fear of COVID-19 has an important role to play in the management of the health and preventive behaviors of older adults. Health experts and communicators may capitalize on these findings to educate people on COVID-19. Future studies are needed to perfectly ascertain the extent of fear needed to stimulate or initiate better preventive behaviors and healthcare practices.
Introduction
The debilitating effect of COVID-19 on the economy of various countries (Gössling et al., 2020; Nicola et al., 2020), health (Ahorsu, Imani, et al., 2020; Lin, 2020) and social life (Chen et al., 2020) is particularly troubling. Ever since the COVID-19 situation attained a pandemic status (Cucinotta & Vanelli, 2020), there have been strenuous efforts by health experts and authorities worldwide to mitigate the spread of the virus (Lin & Cheng, 2020). This includes putting in place health protocols such as washing of hands regularly, wearing of face mask, and keeping at least a meter of physical distancing from each other during a social gathering (Islam et al., 2020; Rieger, 2020). The need for these changes in socio-economic lifestyle has its unique challenges especially among older adults combined with their compromised state of health presents a real challenge among health experts, health communicators, authorities, and family members.
As people age, they develop health challenges such as high blood pressure (hypertension), diabetes, and/or stroke due to their lifestyle which includes but not limited to smoking and drinking alcohol (Li et al., 2019; Nawagi et al., 2018). These health conditions may coexist and/or further result in insomnia, depression or other mental health condition (Burns et al., 2017; Ohrnberger et al., 2017). The prevalence rates of depression among older adults in United States of American is about 8% (Byers et al., 2010; Cheruvu & Chiyaka, 2019) and 7% worldwide among older adults (World Health Organization [WHO], 2017). Prevalence of insomnia symptoms/disorder among older adults are between 6% and 62.1% depending on the country (Gulia & Kumar, 2018; Patel et al., 2018). Taking into consideration these health challenges among older adults as well as their compromised health state, it would be reasonable to assume that older adults are more at risk of COVID-19 compared with their younger counterparts (Morley & Vellas, 2020; Nagarkar, 2020). They are more likely to have a severe or critically severe COVID-19 condition (Guo et al., 2020; Nagarkar, 2020). Further, previous studies have found strong associations between COVID-19 and health (Ahorsu, Imani, et al., 2020; Cao et al., 2020; Wu et al., 2020). Hence, it would be prudent for all to do well and protect older adults from contracting COVID-19.
Toward prevention of COVID-19, health experts and the World Health Organization (WHO) have outlined several safety protocols such as hand washing, wearing of face mask, physical distancing, and quarantining (Chang, Hou, et al., 2020; Chang, Strong, et al., 2020; Chu et al., 2020; Islam et al., 2020; Lin, Imani, et al., 2020). However, these preventive measures conflict our usual way of life thereby making it difficult to abide by them. Among older adults, following these preventive measures can be particularly challenging due to their long years of living a particular lifestyle and their inflexibility in changing these lifestyles as they age (Hong & Rebec, 2012). Hence, they may need considerable support from friends and family members in adapting to this new lifestyle to get through the tough period of COVID-19 pandemic (Cudjoe & Abdullah, 2020; Gyasi, 2020; Morrow-Howell et al., 2020).
In order to better understand the performance of the preventive behaviors, measures assessing or evaluating the COVID-19 preventive behaviors among various populations have been developed (Ahorsu, Imani, et al., 2020; Chang, Hou, et al., 2020; Pakpour & Griffiths, 2020; Taghrir et al., 2020). It has been found that having adequate knowledge of COVID-19 do not directly relate to its preventive behaviors nor its risk perception (Taghrir et al., 2020). However, fear of COVID-19 or its risk perceptions is strongly associated with COVID-19 preventive behaviors (Ahorsu, Imani, et al., 2020; Taghrir et al., 2020). This suggests that another variable may serve as a mediator in the association between adequate knowledge of COVID-19 and/or any other predictor variable and COVID-19 preventive behaviors. Hence, an exploration and subsequent understanding of the links between the variables associated with COVID-19 would help health professionals and researchers to outline strategies of tackling this pandemic effectively.
A study that examined the path model of COVID-19 and psychological distress revealed that “believing COVID-19 information” was associated with “fear of COVID-19” which in turn was associated with “preventive behavior” and “psychological distress” (Chang, Hou, et al., 2020; Lin, Broström, et al., 2020). This suggests that fear of COVID-19 has a special mediation role in its preventive behaviors. Furthermore, other studies have reported on the role of fear as a mediator in changing behaviors (Fang et al., 2020; Pia et al., 2020). Hence, due to the current COVID-19 pandemic situation, this study aimed to examine the mediation role of fear of COVID-19 in the association between perceived health status of older adults and their insomnia, mental health, and COVID-19 preventive behaviors. The findings of this study will further inform researchers and clinicians on the path to chart in their quest to communicating preventive behaviors of COVID-19 and improving ways that older adults can deal with COVID-19 as well as managing COVID-19 situation in general.
Methods
Participants and Procedure
This cross-sectional study was conducted between 1 April to 30 April 2020. The study included older adults who were living in Qazvin. In order to select participants, the IHS (Integrated Health System: SIB in Persian: http://10.124.253.30/home/login) was used. All health information and vital events about households, type of health services required in community health centers and health houses are recorded in this system, electronically. Of 15,235 registered older adults in the IHS, 1,000 older adults were randomly selected based on the following criteria: 50 years old or older, able to speak and understand Persian, and access to smartphone and SMS. Three hundred and twelve older adults were not eligible and 275 older adults did not respond to participate in the study. This, together with calculated effect size of 0.12 to 0.61, p-value of .05, and total sample size of 413 for correlational analysis, yielded a power ranging from 0.69 to 1.00 for this study. An SMS containing study information and the link of questionnaire (Google Form) was sent to the participants. The online consent form was completed by participants before study enrollment.
Measures
Insomnia Severity Index
The Insomnia Severity Index (ISI) was used to assess older adults’ level of insomnia severity over 2 weeks. This seven-item self-report scale is rated on a five-point Likert-type scale response format which ranges from 0 (no problem) to 4 (very severe problem). Its aggregate score is generated by adding all seven items hence, the score may range from 0 to 28 with five sub-scores: 0 to 7 (absence of insomnia), 8 to 14 (sub-threshold insomnia), 15 to 21 (moderate insomnia), and 22 to 28 (severe insomnia) (Bastien et al., 2001). This study used the Persian version (Yazdi et al., 2012).
Patient Health Questionnaire
The Patient Health Questionnaire (PHQ-9) was used to assess the level of depression severity and suicidal ideation over the past 2 weeks (Kroenke et al., 2001) but in this study, it was used for generally assessing older adults’ mental health. This nine-item self-report questionnaire is rated on a 4-point Likert-type scale response format which ranges from 0 (not at all) to 3 (nearly every day). Its full score is generated by adding all the response items. Hence, the score may range from 0 to 27 with higher scores indicating higher levels of mental health challenges. This study used the Persian version (Dadfar et al., 2018).
Fear of COVID-19
The Fear of COVID-19 (FCV-19S) was used to assess older adults’ fear of COVID-19. This seven-item scale is rated on a five-point Likert-type scale response format (strongly disagree = 1 to strongly agree = 5). Its full score, generated by adding all the response items, ranges from 7 to 35 with higher scores indicating greater fear of COVID-19 (Ahorsu, Lin, et al., 2020). This study used the Persian version (Ahorsu, Lin, et al., 2020).
Preventive COVID-19 behavior
The Preventive COVID-19 behavior (PCV-19BS) was used to assess older adults’ COVID-19 preventive behaviors for the past 1 week. Based on the safety protocols for preventing COVID-19 infection by the WHO, this scale assesses frequency with which people practice COVID-19 preventive behaviors such as washing hands frequently, staying home if feeling unwell, practicing respiratory hygiene, and maintaining spatial distancing (WHO, 2020). The PCV-19BS has a Likert-type scale response format (strongly disagree = 1 to strongly agree = 5) which are added to generate its full score. Hence, higher scores indicate greater adherence to COVID-19 preventive behaviors as recommended by the WHO. This scale has been used among Persians (Ahorsu, Imani, et al., 2020; Lin, Imani, et al., 2020).
Perceived health status
Self-perceived health status was measured a single item with a 5-point scale 1 = very poor, 2 = poor, 3 = fair, 4 = good or 5 = very good. Specifically, the older adults responded to the items “How would you characterize your health overall?”.
Background information
The older adults were asked to further furnish us with information relating to their age, gender, educational status, marital status, employment status/details, residency, medical history (e.g., hypertension and diabetes), lifestyle (e.g., smoking and drinking), and their source of COVID-19 information (e.g., social media, newspaper, and television).
Data Analyses
Pearson’s correlations were used to examine the relationships between the variables of this study (perceived health status, fear of COVID-19, mental health, preventive behavior). For the mediation model, perceived health status was the independent variable, fear of COVID-19 was the mediator, and insomnia, mental health and preventive behavior were taken as the dependent variables. Also, age and gender were controlled for in these mediation models. The PROCESS macro for SPSS was used for the mediation analyses using model 4 and a 10,000 bootstrapping resamples (Model 4, Process Macro) (Hayes, 2018).
Results
Among the 413 older adults with mean age of 57.72 (SD = 7.31), more than half were males (n = 256; 62%), majority have attended university (n = 171; 41.4%), employed (n = 208; 50.36%), live in the city (n = 237; 57.4%), and/or married (n = 363; 87.9%). Minority were found to smoke (n = 73; 17.7%), drink alcohol (n = 10; 2.4%), have diabetes (n = 150; 36.3%), hypertension (n = 152; 36.8%), asthma (n = 86; 20.8%), and/or other health condition (n = 70; 16.9%). Additional demographic information is shown in Table 1.
Characteristics of the Study Participants (N = 413).

Table 2 shows the interrelationships between insomnia, mental health, fear of COVID-19, and preventive behaviors. All the correlations were significant (p < .05, range = 0.12–0.61).
Pearson Correlation Matrix of the Variables of Interest.

Assessed using Insomnia Severity Index (ISI).
Assessed using Fear of COVID-19 Scale.
Assessed using Patient Health Questionnaire (PHQ)−9 Item 9.
Assessed using Preventive COVID-19 Behaviors Scale.
p-value <.05; **p-value <.01.
Three mediation analyses were conducted to examine whether fear of COVID-19 was a significant mediator in the association between perceived health status and insomnia, perceived health status and mental health, and perceived health status and COVID-19 preventive behaviors. Table 3 shows that fear of COVID-19 was a significant mediator (unstandardized coefficient = 0.360; LLCI = 0.112; ULCI = 0.664) in the association between perceived health status and insomnia. Also, there were significant direct effects of perceived health status on fear of COVID-19 (unstandardized coefficient of 1.199; SE = 0.395; p = .003) and insomnia (unstandardized coefficient of 1.621; SE = 0.378; p < .001) as well as a significant total effect on insomnia (unstandardized coefficient of 1.981; SE = 0.392; p < .001).
Models of the Effect of Perceived Health on Insomnia With Fear of COVID-19 as a Mediator.
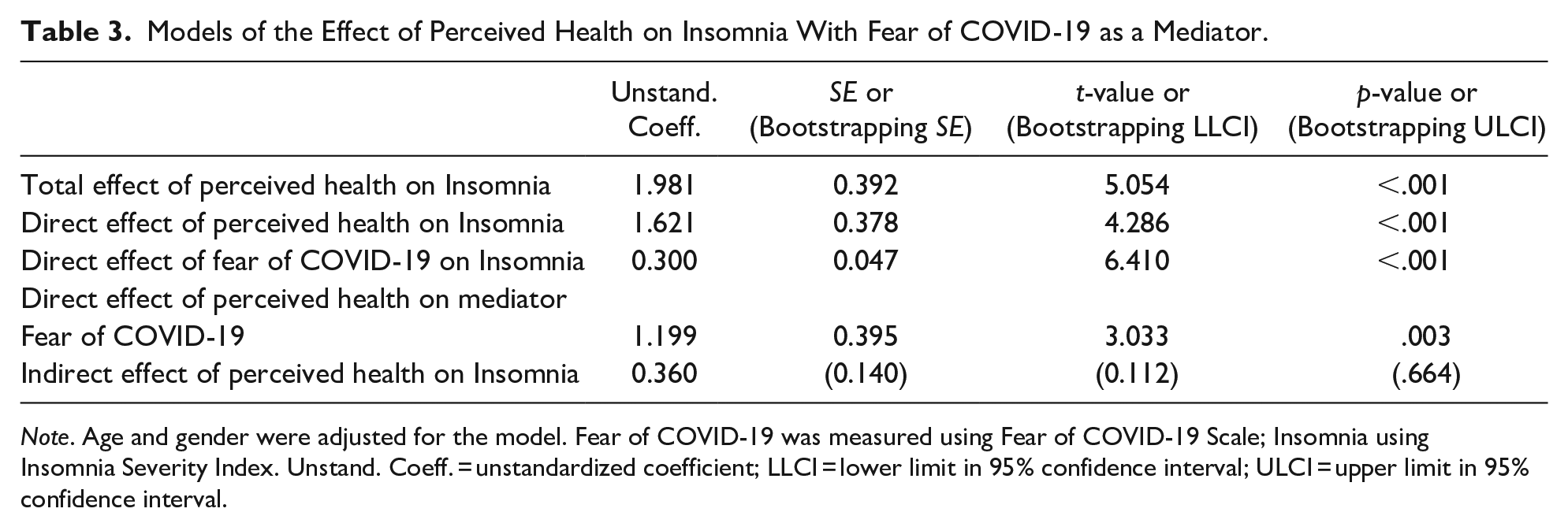
Note. Age and gender were adjusted for the model. Fear of COVID-19 was measured using Fear of COVID-19 Scale; Insomnia using Insomnia Severity Index. Unstand. Coeff. = unstandardized coefficient; LLCI = lower limit in 95% confidence interval; ULCI = upper limit in 95% confidence interval.
Similarly, Table 4 shows that fear of COVID-19 was a significant mediator (unstandardized coefficient = 0.302; LLCI = 0.088; ULCI = 0.559) in the association between perceived health status and mental health. Also, there were significant direct effects of perceived health status on fear of COVID-19 (unstandardized coefficient of 1.199; SE = 0.395; p = .003) and mental health (unstandardized coefficient of 1.304; SE = 0.279; p < .001) as well as a significant total effect on mental health (unstandardized coefficient of 1.606; SE = 0.293; p < .001).
Models of the Effect of Perceived Health on Mental Health With Fear of COVID-19 as a Mediator.

Note. Age and gender were adjusted for the model. Fear of COVID-19 was measured using Fear of COVID-19 Scale; Mental health using Patient Health Questionnaire (PHQ−9). Unstand. Coeff. = unstandardized coefficient; LLCI = lower limit in 95% confidence interval; ULCI = upper limit in 95% confidence interval.
Table 5 shows that fear of COVID-19 was a significant mediator (unstandardized coefficient = 0.054; LLCI = 0.017; ULCI = 0.097) in the association between perceived health status and COVID-19 preventive behaviors. Also, there were significant direct effects of perceived health status on fear of COVID-19 (unstandardized coefficient of 1.199; SE = 0.395; p = .003) but neither on preventive behaviors (unstandardized coefficient of 0.019; SE = 0.050; p = .707) nor total effect on COVID-19 preventive behaviors (unstandardized coefficient of 0.072; SE = 0.052; p = .163).
Models of the Effect of Perceived Health on Preventive Behavior With Fear of COVID-19 as a Mediator.

Note. Age and gender were adjusted for the model. Fear of COVID-19 was measured using Fear of COVID-19 Scale; Preventive behaviors using Preventive COVID-19 Behaviors. Unstand. Coeff. = unstandardized coefficient; LLCI = lower limit in 95% confidence interval; ULCI = upper limit in 95% confidence interval.
Discussion
This current study examined the mediating effect of fear of COVID-19 on the associations between perceived health status and insomnia, mental health, and COVID-19 preventive behaviors. The correlation results revealed that there were significantly positive relationships between the variables with small to large effects, which indicates that when one variable increases the other also increases and vice versa. These support the findings of previous studies that there exists an association between fear of COVID-19, mental health, and COVID-19 preventive behaviors (Ahorsu, Imani, et al., 2020; Fernandez-Mendoza & Vgontzas, 2013; Lin et al., 2018; Wang et al., 2020).
The mediation results revealed that there was a significantly direct association between perceived health status of older adults and their insomnia severity. This suggests that their health status does directly relate with their insomnia severity. This finding is consistent with the categorization of health status (see Table 1) of our participants as a fair majority had poor health status with most of them having diabetes, hypertension and/or other health conditions. This finding is also supported by previous studies that reported pains (e.g., abdominal pain, generalized body pain, and persistent headaches) and cardiometabolic outcomes (e.g., hypertension and diabetes) are significantly associated with insomnia (Fernandez-Mendoza & Vgontzas, 2013; Ogunbode et al., 2014). Hence, it can be assumed that older adults with poor health status may likely have severe symptoms of insomnia and vice versa. The strong mediating effect also suggests an indirect effect of health status on insomnia through fear of COVID-19. That is, apart from their health status directly relating to their insomnia levels, it can also do so via fear of COVID-19. It is reported that fear increases anxiety and worries which are not good for sleeping (Killgore et al., 2020; Mertens et al., 2020). In this COVID-19 period, it is possible that older adults with poor health status have heightened fear of COVID-19 which could, either separately or compositely, be associated with their severe insomnia symptoms. It may, therefore, be appropriate for older adults to be supported in all possible ways such provision of adequate information, face masks, sanitizers so as to calm their fears and protect as well as helping them to manage their health in this COVID-19 period (Apisarnthanarak et al., 2020).
Also, there was a significant direct association between perceived health status of older adults and their mental health which indicates that health status does directly relate with their mental health. That is, it can be anticipated that older adults who have poor health status may have worse mental health and vice versa. This is likely so as older adults with poor physical health have challenges with physical activity and in addition to poor lifestyle choices (e.g., smoking and alcohol consumption) (Burns et al., 2017; Durstine et al., 2013; Ohrnberger et al., 2017), may have negative effects on mental health (Hegberg & Tone, 2015; Ohrnberger et al., 2017). Furthermore, people who do not practice physical activity are reportedly two times more likely to exhibit symptoms of depression and anxiety compared to those who perform physical activity regularly (De Mello et al., 2013). Additionally, the mediation analysis indicated a strong mediated effect for fear of COVID-19 which also suggests an indirect health status on mental health via fear of COVID-19. Therefore, altogether, it can be assumed that there are both direct and indirect effects of perceived health status on mental health of older adults. This implies that poor health status can solely or in combination with fear of COVID-19 may likely worsen older adults’ mental health (Killgore et al., 2020). A good social or family support systems may be needed as a vital tool toward re-assuring and improving older adults’ health in general (Cudjoe & Abdullah, 2020; Satre et al., 2020).
There was no direct association between perceived health status of older adults and COVID-19 preventive behaviors though there was a significant positive relationship between them. This suggests that health status does not directly relate with COVID-19 preventive behaviors hence it is most likely that older adults who have poor health status may not initiate preventive behaviors for COVID-19. This further suggests that there may be other variables that may be significantly associated with COVID-19 preventive behaviors. It is reported that just information of one’s medical condition especially in a chronic condition is not very effective in changing behavior and even less effective is prevention by way of behavior change (Kelly & Barker, 2016; Taghrir et al., 2020). The mediation analysis indicated that there was a significant mediated effect for fear of COVID-19. This further suggests that health status is indirectly associated with preventive behaviors via fear of COVID-19. This implies that fear, although may have its downside, is very important to likely aid in initiating preventive behaviors for COVID-19 among older adults (Apisarnthanarak et al., 2020). Hence, clinicians and health communicators may apply this finding appropriately to aid in preventing COVID-19 among older adults.
The findings in entirety suggest that fear of COVID-19 may play an integral role in the health and preventive behaviors of older adults in this COVID-19 period. By extension fear, when applied appropriately, may be beneficial during health crises by helping to initiate preventive behaviors toward protecting or preventing the crises and preserving life. That is, clinicians, health communicators, and researchers may use these findings to improve the COVID-19 situations especially among older adults as well as to help abide with COVID-19 safety protocols. However, further studies are needed to empirically confirm this assertion especially concerning the severity level of fear needed to harness its benefits. Furthermore, future studies may examine other supportive variables that may aid preventive behaviors and improve insomnia and mental health among older adults.
Limitations
This study has some limitations. First, the study included participants who can be re-categorized as younger older adults hence the findings cannot be generalized to all older adults. Future studies may replicate this study among all older adult groups to ascertain a holistic idea of the pandemic situation. Second, self-report measures were used to gather the data for this study. Hence, the data may be susceptible to biases such as social desirability. Nonetheless, the robustness of the psychometric properties for these self-report measures does suggest that the data are valid and trustworthy to an appreciable degree. Third, this study used a cross-sectional design which limits the cause and effect relationships of our variables and so the findings should be applied with caution. Fourth, our study did not control some other important variables (e.g., family support) in the models hence, readers should interpret or use the findings with caution.
Conclusion
This study demonstrated the mediating effect of fear of COVID-19 on the associations between perceived health status and insomnia, mental health, and COVID-19 preventive behaviors. It was also observed that perceived health status directly influenced insomnia and mental health of older adults but not their COVID-19 preventive behaviors despite that there were small-large significant positive relationships between all these variables. This, therefore, suggests that fear of COVID-19 has a significant role to play in the management of the health and preventive behaviors of older adults. Health experts and communicators may capitalize on these findings to educate people on COVID-19. Future studies are needed to perfectly ascertain the extent of fear needed to stimulate or initiate better preventive behaviors and healthcare practices.
Footnotes
Authors’ Note
The study procedure was approved by the local Ethical Committee (Qazvin University of Medical Sciences; ref. IR.QUMS.REC.1398.375).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.