
Abstract
The purpose of this study was to explore HIV/AIDS knowledge, perceived HIV susceptibility and severity, as well as barriers and facilitators to HIV prevention in primary care settings. Data were collected through both survey and semi-structured interviews. A total of 145 adults over the age of 50 participated in the study. We found that most older adults are willing to have discussions about HIV with their health care provider, however, they are waiting for their provider to broch the topic. The study findings also indicate that older adults need additional education regarding HIV/AIDS, particularly older adults need education about methods of transmission of HIV. Based on the results of this study, it is clear that changes to HIV-related policies and practices must take place to facilitate HIV prevention in primary care settings for older adults.
Human immunodeficiency virus (HIV) is the virus that leads to acquired immunodeficiency syndrome (AIDS). HIV has become an increasingly important health care concern for older adults and their families. The Centers for Disease Control and Prevention (CDC) defines older adults beginning at age 50 and over regarding HIV/AIDS. Until recently, individuals with HIV/AIDS did not live long lives, therefore the age 50 or older was used instead of the more commonly used 60 or 65 years of age. In 2016, nearly half of the people in the United States (U.S.) and dependent areas living with diagnosed HIV were aged 50 and older (CDC, 2019). “Among people aged 55 and older who received an HIV diagnosis in 2015, 50% had been living with HIV for 4.5 years before they were diagnosed—the longest delay for any age group” (CDC, 2019). Late stage diagnosis can be particularly detrimental for older adults, as it means a late start to treatment and possibly more damage to an already weakened immune system.
In 2013, the United States Preventive Task Force (USPSTF) released an HIV screening recommendation to increase early detection of HIV infection. The USPSTF recommends that clinicians screen for HIV infection in adolescents and adults aged 15 to 65 years (USPSTF, 2013). Furthermore, the USPSTF recommends that younger adolescents and older adults who are at increased risk should also be screened (USPSTF, 2013)—meaning that clinicians need to assess their patients risk factors. The USPSTF gives this recommendation a grade of an “A,” indicating that there is a high certainty that the net benefit is substantial and that clinicians should offer or provide HIV screening (USPSTF, 2013). The CDC has a similar recommendation. Despite the recommendations by both the USPSTF and the CDC, routine HIV screening and risk assessment among older adults has remained low.
Health care providers and older adults themselves, oftentimes do not consider older adults to be at risk of HIV and may mistake HIV symptoms for normal age-related changes (CDC, 2019). Several previous studies have reported that there is a general lack of knowledge and misconceptions about HIV transmission (Altschuler et al., 2004; Emlet, 2004; Henderson et al., 2004; Jackson et al., 2005). However, the studies that are available regarding HIV education interventions and older adults are more than 10 years old, more recent studies have been conducted in more rural areas, church-based populations, or in other countries. These studies cannot be generalized to urban areas, non-church-based populations, and U.S. citizens. Therefore, it is the purpose of this research to explore HIV/AIDS knowledge, perceived HIV susceptibility and HIV disease severity among a diverse urban population. Furthermore, this study explores older adults’ perceived barriers and facilitators regarding HIV prevention (i.e., education and screening) in primary care settings. It is important to address this topic among older adults so that they remain HIV negative, seek prompt treatment if positive, and reduce misconceptions about HIV/AIDS.
Conceptual Framework
The Health Belief Model (HBM) originated in the 1950s to understand the failure of people to adopt disease prevention strategies or screening tests for early detection of disease. The HBM is built on the foundation that there is a desire to avoid illness, or get well if already ill, and the belief that a specific health action will prevent or cure illness (Becker, 1974). The original model focused on four constructs: perceived susceptibility, perceived seriousness, perceived severity, and perceived barriers (Becker, 1974). Subsequently, Rosenstock and colleagues added two additional constructs as research regarding the HBM evolved: cues to action and self-efficacy (Becker, 1974). This study focuses on older adults’ knowledge of HIV/AIDS, perceived seriousness and susceptibility, and barriers and facilitators to HIV prevention, as depicted in Figure 1. Survey and interview questions for this study were designed based on the HBM and the utility of this model.

Specific Aims within the Context of the Health Belief Model (HBM).
Method
Sequential mixed methods were used for this study. Phase 1 included a quantitative survey used to assess participant’s HIV knowledge and perceived susceptibility and seriousness. Once all quantitative surveys were completed, semi-structured interviews were conducted later to explore barriers and facilitators of HIV prevention among older adults (Phase 2).
Procedures
Participants were recruited through four senior centers in New Jersey and Pennsylvania. The senior centers were selected through convenience sampling. Notifications were sent out to senior center directors informing them about the opportunity for seniors to participate in a survey and/or interview about HIV among older adults. Of the 10 senior centers that were contacted, four agreed to participate. To be included in the study participants had to be age 50 or older, believed to be HIV negative, and be able to read and write in English. In addition, for the qualitative interviews participants had to have a primary care provider (PCP). On the agreed upon date and time, the researchers visited the senior center and recruited interested participants. The researcher was given a quiet room to review the study procedures and to obtain consent from each participant. The first author reviewed the consent form with each participant and participants were asked to sign the Institutional Review Board (IRB)-approved consent form, if they were comfortable participating and met the inclusion criteria. Each participant was given a copy of the consent form for their records. Participants were given time and a quiet place to complete the survey and return it to the researchers immediately after completing it. Each senior center provided a quiet room for the semi-structured interviews, so that participants information would remain confidential and distractions were kept a minimum. All interviews took place in-person and were conducted by the first author. Interviews ranged from 5 to 35.53 min, with the average being 15 min.
Measures
Demographic information was collected in the first part of the both the survey and the interviews. Participants were asked to provide their date of birth, race, marital status, and highest level of education.
General knowledge of HIV transmission and prevention was measured using the HIV Knowledge Questionnaire (HIV-KQ-18) (Carey & Schroder, 2002). The HIV-KQ-18 has been found to be suitable for use among low-literacy populations (Carey & Schroder, 2002). The HIV-KQ-18 scale measured the extent of the participants’ knowledge of basic HIV information including information about routes of transmission and the disease itself. The HIV-KQ-18 is a shorter version of the HIV-KQ which is a 45-item scale (Carey et al., 1997). The HIV-KQ-18 is a reliable and valid instrument (Carey & Schroder, 2002). The scale response format is forced choice—true, false, or do not know—with scores ranging from 0 to 18. The number of correct items was summarized, with higher scores indicating higher levels of HIV-related knowledge.
An additional 38 questions were included in the survey to address participant’s perceived susceptibility to HIV, the perceived seriousness of HIV, and barriers and facilitators of HIV prevention in primary care settings—using the HBM. Furthermore, the supplemental questions inquired about the participant’s HIV status, last HIV test, and current sexual activity. The 38 supplemental questions were important to gain more insight regarding participant’s personal perceptions, experiences, thoughts, and knowledge about HIV not captured with the HIV-KQ-18 (see the appendix).
A semi-structured interview guide was developed based on the study research questions and the conceptual framework. The interview guide was developed by the authors and a researcher who has expertise in qualitative research and interview guide design. In addition, several older adults and one senior center director reviewed the interview guide to check for bias and errors. The interview questions were as follows: (a) Can you share your thoughts about HIV/AIDS over the last 10 years? (b) What are your thoughts on adults over the age of 50 having discussions about sexual health, including HIV, with their PCP? (c) What personal factors do you think influence HIV prevention among older adults? (d) Do you believe that it is important to increase HIV prevention efforts for older adults? (e) Is there anything that you would like to add on the topic of HIV/AIDS among older adults over the age of 50? Each question was asked of each participant, and follow-up questions were asked throughout the interview, as necessary for clarification. Follow-up questions both strengthened and deepened the understanding of the information not initially included in the interview guide. The Rutgers University Institutional Review Board (Protocol 20150001840) approved all study protocols and consent procedures.
Data Analysis
All quantitative data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 25. Descriptive statistics were used to describe the demographic characteristics of the sample and major study variables. Chi-square tests were used to analyze correct versus incorrect responses to HIV/AIDS knowledge questions. Multivariate general linear modeling procedures were used to identify predictors of HIV/AIDS knowledge (e.g., income).
Forty of the 41 interviews were recorded. One participant requested that her interview not be recorded. The first author transcribed all recorded interviews, verbatim, using Microsoft Word. Data analysis was conducted simultaneously with data collection by reviewing transcripts, making interpretations and notes, and revising questions, as appropriate. Once data collection was completed, the transcripts were reviewed repeatedly to ensure familiarity with the data and to make sure that there were no errors. Data from the semi-structured interviews were organized and analyzed using thematic analysis (Burnard, 1991), using NVivo 11. Thematic analysis is one of the most common forms of analysis within qualitative research. It emphasizes identifying, analyzing and interpreting patterns of meaning or themes within qualitative data. We methodically familiarized ourselves with the data and analyzed the data according to inductive thematic analysis procedures. Once familiar with the data the two authors independently analyzed the data by reading the data line by line and identifying codes from participant’s responses to each question. Categories were verified, if a code did not fit the data or if new data suggested several dimensions of the category, categories were adjusted. Toward the end of the analysis, core categories that revealed the meanings of the participants’ statements were grouped into themes to describe the viewpoints and experience of our participants. Throughout the process of data analysis, the authors’ codes, categories, and themes were compared. In cases of a difference of opinion, definitions were clarified, and discussions continued until consensus was reached.
Findings
Phase 1: Quantitative
Participant characteristics are shown in Table 1. A total of 104 individuals completed the current study. The average age of the sample was 73.7 years, with an average income of US$44,636. Much of the sample was female (81.7%), White (77.9%), married (35.6%), or widowed (30.8%). Most of the sample had less than a college degree (59.6%) and was retired (66.3%). On average, participants had visited their PCP within the last 3.7 months. A total of 73 participants indicated that they were HIV negative, whereas 15 indicated that they were unsure of their HIV status. Most of the sample indicated that they were not sexually active (71.2%).
Participant Characteristics (N = 104).
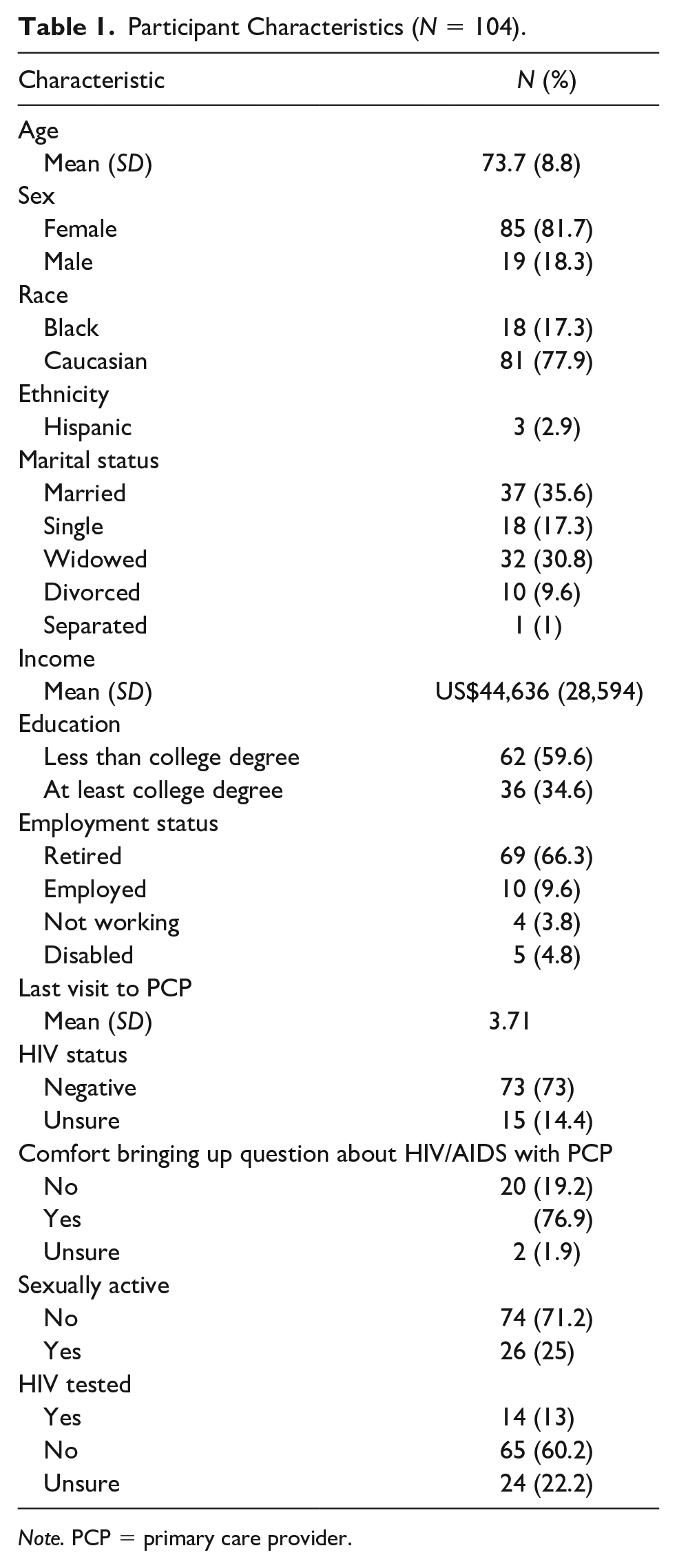
Note. PCP = primary care provider.
HIV knowledge
HIV knowledge was measured using the HIV-KQ-18 tool. Scores ranged from 0 to 17, with an average score of 10.8 (SD = 3.9). Higher scores indicated greater HIV knowledge. Table 2. summarizes responses to the HIV-KQ-18. A correlation matrix was used to examine the relationship between HIV knowledge and the variables listed in Table 1. Multiple regression was used to predict participants’ HIV knowledge score based on their income. The regression equation was significant, F (1, 53) = 6.470, p = .014. Those with a higher income tend to have slightly more HIV knowledge. Income was the only significant variable.
HIV Knowledge (Responses to HIV-KQ-18).

Note. KQ = Knowledge Questionnaire.
Responses to the 38 supplemental questions indicate that the participants are somewhat knowledgeable about basic facts regarding HIV, for instance, most of the sample responded correctly that there is no cure for HIV or AIDS (75.0% and 77.8%, respectively). Participants were also aware of the increased access and use of Sildenafil Citrate (Viagra®) and its contribution to increased sexual activity and increased HIV among older adults (80.6% and 61.1%, respectively). However, participant responses indicate that participants are less knowledgeable about HIV/AIDS information that is specific to older adults. For example, 47.2% of participants did not know that over 50% of deaths from AIDS occurred among older adults in 2012.
Perceived seriousness and severity of HIV
Most of the sample believed their chance of becoming infected with HIV was low (n = 18, 16.7%) to none (n = 83, 76.9%). However, most of the sample considered HIV to be a very serious condition (n = 94, 87.0%) and worth the effort to avoid the disease (n = 97, 89.8%).
Provider interactions
On average, participants had last seen their PCP (i.e., physician, nurse practitioner, or physician assistant) within the last 3.7 months. However, many participants indicated that their regular primary health care provider had not offered HIV prevention educational materials (n = 87, 80.6%), nor had they offered HIV testing (n = 84, 77.8%). Although not many participants reported having discussions about HIV with their PCP, 44 (40.7%) participants indicated that depending on the circumstances they would be willing to discuss their sexual health including HIV with their regular PCP. Forty participants (38.0%) indicated that they would be willing to discuss their sexual health with their PCP regardless of the situation. As aforementioned, many participants recognized that Sildenafil Citrate (Viagra) and similar medications have increased opportunities for sex and increased the prevalence of HIV among older adults. Forty-four participants (85.2%) agreed that when prescribing medications for erectile dysfunction, PCPs should give patients information about safe sexual practices. Finally, participants were asked if they had a question about HIV/AIDS would they be willing to ask their regular PCP, or would they wait for the provider to ask about sexual health—the majority indicated that they would wait for their PCP to bring it up (n = 80, 76.9%).
Prevention efforts
Many participants agreed that there is a need to increase HIV prevention in primary care settings for older adults (n = 86, 79.6%). In addition, over half (n = 59; 54.6%) of participants would like to learn more about HIV /AIDS. Approximately 78.7% of participants indicated that if a brochure about HIV/AIDS among older adults was available in their PCPs office that they would take one and read it.
Phase 2: Qualitative Findings
Participant characteristics
Participant characteristics are shown in table 3. A total of 41 community-dwelling adults over the age of 50 consented to participate. Saturation was reached. The participants ranged from 50 to 84 years of age with an average age of 70.6 years. The majority of the participants were female (n = 31), African American (n = 35), married (n = 16), and retired (n = 35). Many of the participants had either a GED or high school diploma (n = 15) or some college (n = 13) and had visited their PCP in the last 2.8 months on average.
Participant Characteristics (N = 41).

Note. PCP = primary care provider.
Themes
The findings are presented below by overarching themes: facilitators of HIV prevention, barriers to HIV prevention, older adult’s role in HIV prevention, provider’s role in increasing HIV prevention, patient comfort, provider comfort, and suggestions for HIV prevention.
Facilitators of HIV prevention
All participants were asked if there were any factors that helped to facilitate HIV prevention in primary care. Many participants mentioned that having a good rapport with their provider was essential in facilitating HIV prevention. For example, one participant said, “If you have a good rapport with your doctor and nurses, I don’t think there is a barrier.” Several participants felt that having a provider of the same race could help to facilitate HIV prevention, for instance one participant said, “I think you would figure a person of your own race would have more empathy for you,” whereas others shared a different view, as they indicated that they would be comfortable with a provider of any race.
Barriers to HIV prevention
Participants reported a number of barriers to HIV prevention. Fear on both the part of the PCP and patients was frequently mentioned as a barrier to HIV prevention. When talking about PCPs one participant said, “I think some doctors are afraid of HIV just as much as anybody else.” Furthermore, several participants indicated that providers might be unaware of older adults’ sexual health needs. For example, one participant said, “Because they think that because we are old, we don’t have to have sex.” Furthermore, there are many misconceptions and misinformation about HIV risk factors and testing. With regard to HIV risk, one participant when asked to share her thoughts, she said, “I don’t have any thoughts about it because I didn’t think people that old get AIDS. I thought AIDS really was for a younger generation.” Other participants were unaware of where they could go to be tested for HIV. While other participants thought HIV testing was a part of other tests. For instance, one participant stated, “I would, I would say I don’t need it because I get my PSA levels often even though they might not check for HIV.”
Older adults’ role in HIV prevention
Many participants agreed that they have a role in HIV prevention, even if they did not perceive any risk for HIV. Most participants agreed that they should be open to learning more about HIV and take responsibility for educating themselves about HIV. For example, one participant suggested that older adults should go to the library and check for new information about HIV. It was also suggested that older adults read available pamphlets in health care settings, for example, one participant said, “We should read pamphlets and understand that it [HIV] could happen to us.” Furthermore, some participants suggested that older adults should be asking more questions about their sexual health. And, that older adults should know their status and their partners’ status.
Provider’s role in HIV prevention
All participants were asked what they thought their health care providers should be doing to increase HIV prevention. One participant suggested that providers should be asking more questions, “Providers should discuss with you your sexual habits. What you’re doing, how you’re doing and whether or not you should, if you were involved sexually that you should know what’s going on with you by checking you.” Another participant shared the same sentiment when asked what participants should be doing regarding prevention and said, “They should ask you point blank.”
Patient and provider comfort
Participants were asked about their comfort and their providers’ comfort regarding discussions about HIV/AIDS. Several participants remarked that some providers were uncomfortable having discussions about HIV with their older patients. For example, one participant suggested the following, “Maybe the doctor feels uncomfortable about asking the patient.”
Regarding patient comfort, overall participants are comfortable being offered an HIV test. The interviewer asked one participant, “How would you feel if they offered you an HIV test?” The participant responded, “Go ahead, do it.” The majority of participants stated that they would feel comfortable having discussions with their provider about HIV, but they are waiting for their provider to initiate the discussions about sexual health including HIV.
Participants were asked if they had a preference for provider type in regard to HIV prevention. The majority of the participants indicated that they do not have a preference for provider type, meaning that they would be okay with a physician, nurse practitioner, or physician assistant.
HIV education and testing (prevention)
Participants were asked to provide suggestions for increasing HIV prevention among older adults. These results can be found in Table 4.
HIV Prevention Recommendations.

Discussion
The purpose of this study was to explore older adults’ HIV/AIDS knowledge, preferences for HIV prevention in primary care settings, perceived seriousness and severity of HIV, and barriers and facilitators to HIV prevention in primary care settings. The findings of the study suggest that older adults are in need of additional education about HIV/AIDS, as the scores on the HIV-KQ-18 varied quite a bit. Particularly older adults need education regarding HIV transmission, as evidenced by incorrect responses on the HIV-KQ-18. Predictors of participant’s HIV knowledge score were assessed, however, only one of the assessed hypothesized predictors was significant. Perhaps other variables that were not assessed predict HIV knowledge or perhaps HIV knowledge is generally low in the older population. Furthermore, the findings suggest that older adults need aging-specific HIV education. Several previous studies have reported that there is a general lack of knowledge and misconceptions about HIV transmission (Altschuler et al., 2004; Emlet, 2004; Henderson et al., 2004; Jackson et al., 2005). In addition, previous researchers have suggested that older adults are placing themselves at risk of HIV unknowingly, as a direct result of their lack of HIV knowledge (Karpiak & Lunievicz, 2017). Many older adults do not know what younger individuals know about safe sex, as they have not had the education and counseling about HIV prevention (Idso, 2009) and older adults are typically omitted from HIV-prevention programs (Altschuler & Katz, 2015). Lack of education in combination with other factors, such as assumptions that older adults are no longer sexually active has led older adults to have a low or non-existent perception of risk for HIV (Karpiak & Lunievicz, 2017). The current study found that many participants reported their risk of becoming infected with HIV as low (76.9%). With low or no perceived risk of becoming infected with HIV, seniors are unlikely to engage in activities to avoid HIV. PCPs are often cited as being able to increase HIV prevention for older adults, because of their frequent interactions with older adults, however, prevention rates have not increased significantly.
It is well documented in the literature that older adults frequently visit their health care provider for general health checkups and specific complaints (CDC, 2019). Older adults, those age 50 and older, represent the greatest consumers of health care, accounting for approximately 25% of all primary care visits (CDC, 2009). Recently, there has been an increase in the number of non-physician providers, including PAs and NPs to allow more time for preventive care in primary care settings (Kocher et al., 2010). Despite older adult’s regular visits to their health care provider, older adults are less likely to discuss their sexual habits or drug use with their health care provider (CDC, 2019). And, health care providers are less likely to ask their older patients about these issues. Similarly, this study found that older adults visit their PCP regularly—on average participants in this study saw their PCP within the last 3 months. Many participants indicated that their regular PCP had not offered any HIV prevention educational materials, nor had they been offered HIV testing. This study found that misperceptions/misinformation and fear are barriers to HIV prevention in primary care settings. We know from previous research that both patients and health care providers make assumptions that older adults do not, or rarely, engage in sexual activity or use illicit drugs, and they are therefore not at risk of HIV or other sexually transmitted infections (STIs; Karpiak & Lunievicz, 2017).
Given the increasing number of older adults being diagnosed and living with HIV, it is imperative to increase HIV prevention efforts for seniors. Despite the barriers identified as a part of this study, some participants recognized the need to increase HIV prevention efforts specifically for older adults and acknowledged that both the PCPs and patients have a role to play in increasing prevention efforts. Adekeye et al. (2012) suggested that practices and policies be developed to increase HIV awareness and screening.
This study focuses on older adults’ knowledge of HIV/AIDS, perceived seriousness and susceptibility, and barriers and facilitators to HIV prevention, as depicted in Figure 1, as they pertain to the HBM. The HBM can be used to develop HIV prevention strategies at each level of the model. For example, HIV education can be used to address perceived susceptibility. We learned through this study, that most older adults do not believe that they are susceptible to HIV and therefore are taking steps to prevent HIV infection. By providing HIV education (e.g., transmission, risk factors, symptoms, aging, and HIV), we can increase their perceived susceptibility, if they are indeed engaging in risky behaviors. In addition to developing educational interventions for older adults, continuing education courses can be developed for PCPs. As we have learned from previous research, PCPs need education and training about HIV among older adults. PCPs do not often think about older adults being at risk of HIV and therefore do not assess risk factors and provide screening (Davis et al., 2016). Education can be increased through the development of educational interventions (see Table 1). Findings from this study indicate that older adults are aware of how serious HIV is general, but perhaps focus on how HIV differentially affects older adults and delayed diagnosis, which is more common among older adults. In addition to education for both providers and patients, policies and practices for HIV screening need to be implemented to serve as a cue to action, which is aim three as depicted in Figure 1. For example, routine screening and prompts to screen when prescribing erectile dysfunction medications can serve as cues to action.
Future studies should test educational interventions in primary care settings, as well as other settings specifically targeting older adults. Additional studies should test the implementation of practices in primary care—such as, routine screening. It is important to educate patients so that they can be advocates and take responsibility for their own health, as well as to educate providers to provide more HIV education and screening to their patients.
This study is not without limitations. Study participants were recruited using snowball and convenience sampling methods. Snowball and convenience sampling methods can lead to a sampling bias (Henry, 2009), resulting in a sample that can be more homogeneous and less representative of the older adult population. Future studies should implement recruitment strategies to recruit a more diverse sample. In addition, future studies should incorporate seniors from a variety of settings—not just senior centers. Despite these limitations, the present study provides a better understanding of older adults’ perception of HIV/AIDS and barriers and facilitators of HIV prevention in primary care settings.
Conclusion
In conclusion, findings from the present study are exploratory and provide substantive data to the HIV/AIDS and aging literature. This study combined with previous research will allow for the development of age appropriate HIV prevention interventions. We know that the majority of older adults are willing to have open discussions about their sexual health with their PCPs; however, changes in policies and practice must occur to facilitate these discussions. Interventions should focus on education for both patients and providers. Given the increasing number of older adults being diagnosed and living with HIV, it is imperative to increase prevention efforts promptly.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.