
Abstract
The aim of the current study was to examine the acceptability and feasibility of a multicomponent care management program in older adults with advanced dementia in a long-term memory care unit. Eighteen older adults with moderate to severe dementia were asked to wear an activity monitor (Fitbit Charge 2 HR) and participate in a once monthly telehealth intervention via iPads over a 6-month period. Activity monitor data were used to assess compliance. Acceptability was assessed through qualitative interviews conducted with the caregiving staff on the memory unit. The care management program was acceptable to residents and their caregivers. Results indicated that the care management program is feasible in older adults with advanced dementia although activity monitor adherence was better during the day than at night. Telehealth session compliance was excellent throughout the study. A long-term multicomponent dementia care program is acceptable and feasible in individuals with advanced dementia. Future studies should aim to evaluate whether data received from activity monitors can be used in a dementia care intervention program.
Introduction
Alzheimer’s disease and related dementias (ADRDs) result in progressively declining cognitive (e.g., memory, language, judgment) and functional status (e.g., managing medications and handling self-care independently). Globally, rates of ADRDs are increasing with no known cure or disease modifying therapy on the horizon. The World Health Organization (WHO, 2017) estimated that 47 million cases of dementia existed worldwide in 2015, a number that is projected to triple by 2050 given the high rate of older adults over the age of 65 and increased life expectancies. Managing the myriad cognitive, behavioral (Kales et al., 2015), and physical health (Groot et al., 2016; Wennberg et al., 2017) declines associated with ADRDs creates significant care management challenges for family and health care providers as people with dementia (PWD) progress through the disease (Bossen et al., 2015). An increasingly efficient and effective method for managing and monitoring care in dementia populations involves technology-based care management strategies (e.g., telehealth/digital-medicine, wearable technologies).
Technology-based care management programs in dementia populations are inherently appealing for two reasons. First, in-office or emergent medical visits may be disruptive to patients and their caregivers. Therefore, telehealth visits have the potential to reduce that disruption. Second, there is significant difficulty in obtaining timely and accurate subjective data from individuals with ADRDs to better monitor their health status (Farina et al., 2019). Current approaches to technology-based care management of PWDs typically utilize one or more assistive technologies (AT) that fall into three main categories: formal assistive AT (e.g., tele-health care), “off the shelf” AT (e.g., wearable technologies, dementia-friendly clocks/phones), and everyday household AT (e.g., music to enhance reminiscence, written notes; Gibson et al. (2015).
Several studies have demonstrated that individuals with dementia and their caregivers find technology-based monitoring (e.g., Farina et al., 2019; Kikhia et al., 2018; Mahoney & Mahoney, 2010) and care management (e.g., Dang et al., 2018; Gately et al., 2020) acceptable. Furthermore, several studies have found that these interventions are feasible and can aid in providing patient-centered care that results in improved quality of life (QoL) and reduced caregiver burden (Bossen et al., 2015; Cavallo et al., 2015; Holthe et al., 2018). However, most studies have been conducted in community-dwelling samples and in individuals with mild dementia (e.g., Farina et al., 2019), with few studies examining the acceptability and feasibility of using these technologies in individuals in memory care residential facilities with more advanced/progressed dementia (e.g., Merilahti et al., 2016). Studies that have examined the acceptability of technologically based care in individuals with more advanced dementia have found them to be acceptable (Lazar et al., 2016; Subramaniam & Woods, 2010). For example, in a study by Lazar and colleagues (2016), the authors found that a commercially available computer-based recreational and leisure program was acceptable to and provided benefits for PWD and their caregivers. In addition, many of these studies have examined acceptability and feasibility over short periods (e.g., 7 days), whereas the current study examines these parameters over a 6-month period. Examining the acceptability and feasibility of a technology-based care management in this population (moderate to advanced dementia) and over longer periods (months rather than days) is a critical next step prior to exploring their efficacy. If technology-based care management strategies (telehealth patient visits, wearable monitoring) are acceptable and feasible, then individuals in long-term care facilities with moderate to advanced dementia may experience benefit either in terms of QoL, reduced physical or neuropsychiatric problems (Lawrence et al., 2012), and/or health care utilization (e.g., hospitalizations, unnecessary outpatient visits).
The current study aims to address a gap within the literature by examining the acceptability and feasibility of a multicomponent telehealth intervention in individuals with moderate to severe dementia who live in a long-term memory care facility. The present study aimed to incorporate different aspects of AT including telehealth and wearable technology. Specifically, wearable devices provide an abundance of objective information that can be easily used for tracking and monitoring of different outcomes such as physical activity and sleep (Merilahti et al., 2016), fall risk (Schwenk et al., 2014), and behavioral disturbance (Marcén et al., 2016) by caregivers and health professionals. A multimodal approach (i.e., objective and qualitative) was used to examine the acceptability and feasibility of the intervention.
Method
Participants
Participants (n = 18) were residents of a long-term memory care facility in the southeast United States who were previously diagnosed with various types of dementia. The mean age of the participants was 84.56 (SD = 7.12), and participants were generally well-educated (M = 16.53, SD = 2.70). The sample was 50% female, and all were White/Caucasian. Caregivers who were employed at the long-term care facility (n = 6) also participated to provide accounts of acceptability and feasibility of the current intervention given concerns regarding difficulty obtaining accurate subjective data from the present sample.
Procedure
The current study was approved by Ochsner Medical Center’s institutional review board. Informed consent was obtained from caregivers/legal guardians and assent was obtained from participants with dementia. Dementia diagnosis was confirmed through the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005; M = 8.50, SD = 6.72) and the Clinical Dementia Rating Scale (CDR) at baseline (Hughes et al., 1982; M = 2.24, SD = 0.75). The CDR was also completed at the 6-month visit to track progression (M = 2.67, SD = 0.71). Caregivers completed the following questionnaires at baseline and monthly thereafter: Bristol Activities of Daily Living Scale (ADL; Bucks et al., 1996), Neuropsychiatric Inventory−Questionnaire (NPI-Q; Kaufer et al., 2000). Quality of Life−Alzheimer’s Disease (QoL-AD; Logsdon et al., 2002), and Quality of Life in Dementia (QUALIDEM; Dichter et al., 2014). All participants were provided with an activity monitor (FitBit Charge HR) and were instructed to wear it daily. Average daily physical activity (i.e., steps) and sleep (i.e., minutes asleep) were tracked monthly. Participants received a once-monthly telehealth visit with a neuropsychologist (R.J.S.) to assess for and manage neuropsychiatric symptoms. Wellness plans that included cognitive, behavioral, and medical goals for each month were created during telehealth visits, and completion of the goal (i.e., met/not met) was assessed by staff (Bradley et al., 1999; Sachs, 1998). Outcome data (i.e., falls, hospitalizations, medication changes, behavioral episodes, mortality) were also tracked monthly throughout the study. Staff caregivers (n = 6) were invited to participate in interviews to explore their opinions regarding the acceptability of the devices at the 6-month visit.
Acceptability
The current study examined retrospective acceptability of the care management program. As suggested by Sekhon et al. (2017), it is important to assess multiple facets of acceptability (e.g., affective attitude, burden, effectiveness). The present study attempted to address several aspects of acceptability (e.g., affective attitude, adherence) through both quantitative (i.e., step count) and qualitative (e.g., caregiver interviews) methods.
Measures
Activity monitors
Fitbit Charge HRs (Fitbit, San Francisco, CA) were provided to all participants and placed on the nondominant hand throughout the study. The Fitbit Charge HR is a wrist-worn activity monitor worn on the nondominant hand that tracks physical activity (e.g., step-count, HR, steps climbed, and sleep data) that has shown to have acceptable validity and reliability in older adults (Farina & Lowry, 2017; Straiton et al., 2018). Fitbit data were downloaded directly from the Web server using an application issued by Fitbit.
Questionnaires
The MoCA is a brief 30-question cognitive screening measure and was completed only with the individual with dementia. A score of 24 or less is typically indicative of cognitive impairment (Nasreddine et al., 2005).
The CDR is a structured clinical interview that assesses stages of decline throughout the dementia process. A score of 0.5 or higher is indicative of dementia (Hughes et al., 1982). The CDR was completed with the resident’s caregiver.
The Bristol ADL Scale is a 20-item assessment of an individual’s daily functioning abilities (e.g., eating, drinking, toileting) that was completed by the resident’s caregiver.
The NPI-Q is a brief 12-item informant-based questionnaire that assesses the frequency and severity of various forms of psychopathology that commonly occur in progressive cognitive decline (Kaufer et al., 2000).
The QoL-AD is 13-item measure designed to obtain a rating of the patient’s QoL from both the patient and a caregiver. Higher scores are indicative of better QoL (Logsdon et al., 2002).
The QUALIDEM is a 37-item informant-report of QoL for use with individuals aged 65 years and older with mild to severe dementia. The QUALIDEM assesses various domains of QoL (e.g., care relationship, positive affect, feeling at home, etc.).
Telehealth Care Management
Once-monthly telehealth sessions were completed with the participant and their caregiver via iPads (6th generation; Apple Inc., Cupertino, CA) to assess for neurobehavioral issues (e.g., behavioral outbursts, resistance to bathing, cognitive or activity disengagement, anxiety) and provide recommendations/strategies to staff (e.g., behavioral strategies, refer for medication consultation, activity recommendations) to improve concerns. For example, neuropsychologists would set monthly personalized cognitive goals for each resident such as reminiscing about positive aspects of their lives (e.g., family, work), listening to music, or reading books.
Caregiver/Staff Interviews
Caregivers were invited to complete interviews that were used to explore acceptability of the intervention among individuals with dementia and feasibility of integrating the intervention into routine care. Semi-structured interviews were created based on common themes found in the acceptability research on integrating technology in dementia care (e.g., Farina & Lowry, 2017). Themes were organized into the following categories: caregiver attitudes, resident attitudes, device design, adherence, and impact on care (see Table 4). Interviews were completed with all caregivers and lasted approximately 5 to 10 min. All interviews were audio-recorded to allow for separate thematic analysis by two independent coders.
Analysis
Descriptive data on participant demographics (see Table 1) and questionnaire responses (see Table 2) were analyzed using IBM SPSS Version 25. Adherence to the intervention was assessed using the percentage of days within a month that the participant wore the Fitbit as well as monthly completion for the telehealth intervention. Step count and sleep totals were averaged using only days with valid data (e.g., sum of steps on valid days/number of valid days). Regarding analysis of the qualitative data, two researchers (Alyssa De Vito and Jasmin Pizer) independently coded caregiver responses using deductive methods. A Microsoft Excel base calculator used to calculate Cohen’s kappa coefficient (Cohen, 1960) was used to assess interrater reliability (Mackinnon, 2000).
Participant Demographics.

Assessment Descriptive Statistics.

Note. MoCA = Montreal Cognitive Assessment; CDR = Clinical Dementia Rating Scale; ADL = activities of daily living; NPI-Q = Neuropsychiatric Inventory−Questionnaire; QoL-AD = Quality of Life−Alzheimer’s Disease; QDEM = QUALIDEM; Care = Care Relationship; Pos = Positive Affect; Neg = Negative Affect; Rest = Restless Tense Behavior; Social = Social Relations; Isolation = Social Isolation.
Results
Participants
Of the 18 participants initially enrolled in the study, 11 remain enrolled in the study. Death (n = 1) and discontinued residence at the long-term care facility (n = 6; largely due to hospice placement) were reasons for attrition. Please see Table 1 for participant demographics and Table 2 for assessment descriptive statistics.
Adherence to the Intervention
Activity monitors
Adherence to the activity monitors better during the day than at night. Daytime average adherence across 6 months was 88.0% or good. Nighttime adherence was poor (range = 58.5%−70.9%) for all months except Month 3 (i.e., 70.9%; acceptable). See Table 3 for activity monitor adherence.
Intervention Adherence.
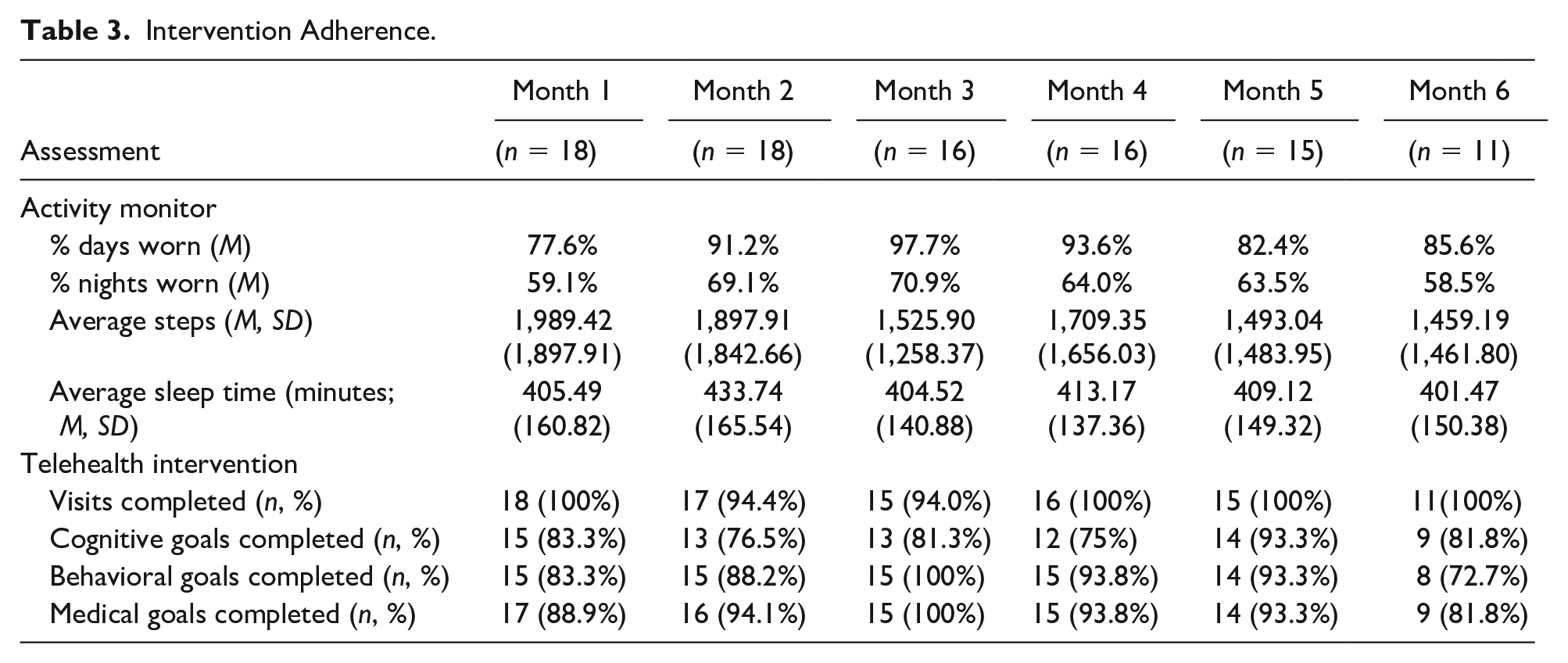
Telehealth intervention
Adherence to the telehealth-intervention was excellent across all months (i.e., above 90%), but was impacted by patient hospitalization (n = 2). Wellness plan goal completion varied by wellness category. Average goal completion across all months was highest for medical goals (i.e., 92.0%) followed by behavioral goals (88.6%) and cognitive goals (81.7%). Please see Table 3 for intervention adherence.
Caregiver interviews
Five themes were considered when constructing the interview: (a) caregiver attitudes toward the device, (b) resident attitudes toward the device, (c) device design, (d) adherence, and (e) impact on care. Summaries of the themes and examples can be found in Table 4. Agreement between raters was near perfect (k = .87; Cohen, 1960; Landis & Koch, 1977).
Summary of qualitative themes.

Caregiver attitudes toward the device
Caregiver attitudes were generally positive regarding residents wearing the device. Caregivers reported that having residents wear the device made care easier (e.g., could easily check the resident’s heart rate) and made them more aware of the residents’ behavioral patterns (e.g., agitation, sleep).
One caregiver did note that including the device in care did mildly increase burden on caregiver routines due to the maintenance (e.g., cleaning, charging) of the devices. However, most other caregivers noted that the upkeep of the device was easy and took less than 5 minutes per resident during their shift.
Resident attitudes toward the device
Many caregivers reported that residents liked the device because it also served as a watch. Caregivers also reported that some patients liked to see the number of steps they completed each day and that residents liked to compare the number of steps they took. Other caregivers reported that residents appeared to be neutral or having no seeming opinion or awareness of the device.
Design
Caregivers reported that they would not change the device design because it was easy for residents to operate (e.g., check time, step count) and did not appear to cause the residents discomfort. One caregiver reported that one way to improve the device would be to have an indicator that would appear on the screen to make the wearer/care staff aware that the device battery was low.
Adherence
Many caregivers reported that adherence was better during the day than at night, although they believe adherence improved over time. This was partially due to standard routines associated with wearing jewelry/watches such as removing accessories when showering or before going to bed. Another reason commonly cited for residents removing the device was agitation associated with sundowning which typically occurred during the late afternoon/early evening. Caregivers reported that when residents became agitated, they frequently try to remove the device.
Impact on care
Several caregivers indicated that having access to data regarding residents’ physical and behavioral patterns positively impacted care. For example, a few caregivers reported that if they noticed that residents had a low step count, that they would encourage residents to participate in exercise-related activities. Similarly, several caregivers noted that they were more understanding of and compassionate toward residents’ behavior if they had slept poorly the previous night.
Discussion
The present study aimed to examine the acceptability and feasibility of a longitudinal technology-driven care management program employing wearable technology and monthly telehealth visits with a neuropsychologist in a sample of individuals with advanced dementia. Consistent with previous studies, we found high acceptability by both the residents and their caregivers (Dang et al., 2018; Farina & Lowry, 2017).
A unique aspect of the present study is that participants (with the aid of their caregivers) were outfitted with the device and participated in telehealth visits over a 6-month period. Previous studies are limited in that they examine acceptability and feasibility at shorter intervals (e.g., days, weeks) which make justification for including these types of interventions in routine health care difficult. Examining acceptability and feasibility over longer intervals is crucial in this population given that individuals with advanced dementia require continuous monitoring and intensive care management (e.g., Zylstra et al., 2018) for many years.
Qualitative interviews with caregivers provided significant insight into beneficial aspects and areas of future improvement for the care management program. Similar to other studies that have assessed the feasibility/adherence of using wearable technology in dementia populations, the current study found that adverse events (e.g., hospitalizations), agitation (Merilahti et al., 2016), and night-time routines (e.g., removing accessories before showering and at bed time; Farina et al., 2019) were the primary reasons for reduced adherence. Regarding beneficial aspects of the program, several caregivers reported using the data on the device (e.g., step count, sleep data) in their daily treatment plan as well as interaction and communication with residents despite not being instructed to do so. This may indicate the feasibility of future intervention programs that incorporate the aforementioned data to inform and improve personalized care, reduce caregiver burden, and improve QoL for PWDs. Several studies have demonstrated benefits of exercise on health and well-being in PWDs, especially those in long-term care placements (Brett et al., 2016; Heyn et al., 2004). Therefore, if wearable technology can be used to track exercise and encourage PWDs to increase physical activity, there is the potential to improve QoL and health. Furthermore, telehealth programs as the one in the current study can be used to improve patient mental and cognitive health through monthly wellness visits during which cognitive and behavioral goals are created and reviewed with caregivers to keep PWDs cognitively and socially stimulated which has been linked with improved QoL in PWDs (Penninkilampi et al., 2018). This also has the potential to minimize caregiver burden and reducing negative outcomes (e.g., behavior-associated hospitalization) by allowing caregivers access to health care professionals that specialize in managing behaviors associated with dementia to develop more effective behavior-treatment plans.
Limitations
An important limitation of the current study is that this small sample of residents consists of primarily White, well-educated individuals. Therefore, acceptability and feasibility of the program may differ in those with diverse backgrounds (e.g., Scott Kruse et al., 2018) and should be explored in future research. It is also important to recognize that residents required aid in the use of the devices (i.e., Fitbit Charge 2 and iPad 6th generation) given their advanced stage of dementia. Therefore, the care management program does require additional efforts from care staff which may increase caregiver burden. Caregivers in the current study reported that ATs were largely beneficial rather than burdensome as AT aided them in performing typical daily tasks such as quickly checking residents’ heart rate through the FitBit. ATs have been shown to decrease caregiver burden in other samples although these studies were done in informal caregivers of PWD such as family members or friends (Marasinghe, 2016). However, given differing pressures between informal and professional caregivers such as time constraints and the number of individuals being cared for, the level of burden imposed by AT utilization on professional caregivers needs to be formally assessed in future research.
Finally, qualitative interviews were solely conducted with caregivers given concerns regarding accuracy of resident report. Future studies may wish to conduct interviews with both residents and their caregivers to more fully assess resident acceptability of the care management program.
Footnotes
Acknowledgements
We would like to thank the staff at Mercer’s Way Memory Unit at Lambeth House for their help in making this study successful. We would also like to thank Jasmin Pizer for her help in coding qualitative interview responses.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to thank Broadway Services, Inc., for their financial support.