
Abstract
As the proportion of older people in Greece grows and the need for promoting healthy aging is apparent, it becomes increasingly important to investigate the relationship between social support and health-related quality of life (HRQoL) of older people in the community. A cross-sectional study was conducted in 451 older people living in the community in greater Athens, Greece, with an anonymous questionnaire, including demographics, and the EQ5D including EuroQol–visual analogue scale (EQ-VAS) and the Multidimensional Scale of Perceived Social Support. Multivariate linear regression analysis was applied to identify independent factors related to perceived social support and HRQoL. The majority of older people were women, married or widowed, living with their family or alone. Perceived social support was medium and higher from significant others and family. A statistically significant positive relationship was found between social support from significant others/friends and HRQoL, as well as between social support from friends/family/significant others and EQ-VAS. In conclusion, HRQoL of older people is influenced by the received social support.
Introduction
Prolongation of life expectancy is one of the most complex challenges of developed societies (Jin et al., 2015). Population projections predict a small change in the total number of inhabitants in Europe between 2010 and 2060. These changes also apply to Greece, which already has one of the most aged populations (European Commission Economic and Financial Affairs, 2017). In Greece, there are still close family ties and respect for older people. For this reason, older people receive assistance and care from their children, whether living together in the same house or by assisting them whenever they need it, if they live independently (Triantafyllou et al., 2006).
Open-Care Centers for Older People (KAPI) is an exception and services provided through them or complementary to that offered by the health service, such as Help at Home and day care (Daniilidou et al., 2003).
Social relationships affect mental health, behavior, physical health, and mortality (Umberson & Montez, 2010). Sociologists have played a central role in defining the relationship between social networks and health outcomes (Umberson & Montez, 2010). The impact of social networks on health, demand, or use of health services and the health-related quality of life (HRQoL) of the population has attracted the interest of the international research community (Hawe & Shiell, 2000). Both loneliness and social networks have been linked to emotional mood, well-being, and self-esteem that reduce the impact of stressful situations (Zimet et al., 1988). Social networking of individuals usually differs according to their social and economic position, with certain demographic factors (marital status, size of the household, presence of children), with contacts with children, and working conditions of individuals (Fakiolas, 2012). Increased life expectancy is of no value if HRQoL of older people is not present. Most health and social care services are aimed at the entire population, not only at older people and this applies to Greece also. Particularly in modern societies, where the population is constantly aging, social support is a key factor in maintaining a good standard of health and HRQoL for older people (Berkman & Krishna, 2014). At the same time, despite the deterioration of health, older people have a positive perception of their health status and are satisfied with their lives (Greve & Staudinger, 2006). This may be possible due to psychosocial resources promoting well-being during the aging process (Bueno & Navarro, 2003; Diener et al., 2003).
Social support protects older people from the negative impact of age-related challenges such as family members’ death, interpersonal conflicts, even extraordinary events like natural disasters, and also prevents experiences or emotional disturbances as anxiety and depression (Hatfield et al., 2013; Hsu & Tung, 2010; Taylor & Lynch, 2004). Therefore, social support could be considered as a treatment strategy that allows older people to interpret stressful conditions and to reduce pathological consequences that arise from normal deterioration during aging (Chou et al., 2001; Gow et al., 2007).
Social Support is measured in different ways; most commonly by questionnaires with open or closed questions. One of the most frequently used questionnaires is the Multidimensional Scale of Perceived Social Support (MSPSS) (Zimet et al., 1988).
There has been a keen interest in the quality of life, over the last two decades. HRQoL is a specific field of research, including aspects of lives of people affected by both personal health and activities which aim at maintaining or improving health. HRQoL is a subjective perception of health level which focuses on the effect of a particular health condition on a person’s ability to live a satisfying life. In other words, it is a multidimensional concept with a dual character, which refers to the positive and negative aspects of well-being and life and includes physical, mental and social health. Also, HRQoL is a dynamic concept, the assessment of which, changes as the level of health, relationships, experiences and roles change (Yfantopoulos, 2007). The assessment of HRQoL is done by questionnaires that meet strict criteria of validity, reliability, specificity, and responsiveness. One of these questionnaires is EQ5D questionnaire that has been translated into Greek, and it is tested for its credibility and validity by Yfantopoulos (2001), and it is the most appropriate tool for older people (Brazier et al., 2004; Holland et al., 2004).
Purpose
The purpose of this study was to investigate the factors that affect the relationship between social support and HRQoL of older people living in the community. More specifically, the objectives of the study were to investigate the impact of demographic variables on HRQoL of older people and the relationship between social support and HRQoL of older people living in the community. The hypothesis was that HRQoL for older people is improved in those that receive social support by their social network.
Method
A cross-sectional study was conducted. A convenience sample of older people living in the community in greater Athens was included. Older people were approached at the Open-Care Centers for Older People (KAPI) of the municipalities selected for the study; municipalities were selected to differ in term of socioeconomic status. The sample inclusion criteria were older people of both sexes in similar proportion with that in the general population and only older people without cognitive limitations or functional disability.
The protocol and questionnaire of the study along with the informed consent form were approved by the Ethics Committee of the Nursing Faculty of the National and Kapodistrian University of Athens. Subsequently, a written permission was sought and granted by each Municipality before stratification of KAPIs. Older people were informed about the purpose of the study and gave their consent before they were asked to answer the questionnaire. Participation at all stages was voluntary and they had the opportunity to leave at any stage of the study. The privacy of personal data was maintained and only the research team had access to the data.
Data collection was made using an anonymous questionnaire that was filled by interview carried out by the principal researcher. The questionnaire included demographic questions, questions about the social network of older people, and a question of self-reported health. Also, participants answered the EQ5D questionnaire and the MSPSS.
The EQ5D essentially consists of two parts, the EQ5D descriptive system and the EQ–visual analogue scale (EQ-VAS). The EQ5D descriptive system comprises the following five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has three levels: no problems, some problems, and extreme problems. The respondent is asked to indicate his or her health state by ticking (or placing a cross) in the box against the most appropriate statement in each of the five dimensions. The EQ-VAS records the respondent’s self-rated health on a vertical, visual analogue scale where the end points are labeled “best imaginable health state” and “worst imaginable health state.” This information can be used as a quantitative measure of health outcome as judged by the individual respondents (The EuroQol Group, 1990). This questionnaire has been translated into Greek, and it is tested for its reliability and validity by Yfantopoulos (2001).
MSPSS is a multidimensional tool, with 12 queries, measuring perceived social support from three perspectives. The support received by the individual from Friends, and Family and Significant Others (who are other important people like a partner). The answers are given on a 7-point Likert-type scale, ranking from 1 = completely disagree to 7 = fully agree (Zimet et al., 1988). The scale has been translated and validated in a Greek Cypriot sample of people with heart failure. Construct validity was examined with a confirmatory factor analysis (CFA) and an exploratory factor analysis (EFA). CFA of the Gr-MSPSS failed to extract the original construct of MSPSS. EFA identified a model with two factors: one factor is “Friends” and the other factor is “Family and Significant Others.” The internal consistency reliability was examined by Cronbach’s alpha, which was found to be .87 and for the factors “Friends” and “Family and Significant Others,” .92 and .97, respectively. Test–retest showed high correlation between the total score of the scale (r = .907, p < .01). The results of the reliability and validity tests showed satisfactory results of the psychometric properties of the Gr-MSPSS, providing a useful tool for the assessment of perceived social support of Greek speaking patients (Chamboulidou et al., 2016). This version with two factors was also used in the analysis of this study.
Mean values and standard deviations are used to describe the continuous variables. Absolute numbers and percentages are used to describe the categorical variables. Parametric statistical methods were used for the bivariate analysis, whereas Pearson correlation coefficient was used for studying the relationships between continuous variables. Linear regression analysis was used to find independent factors that are related to the different scales from which dependency factor (b) and standard error (SE) have occurred. A variance inflation factor (VIF) was detected to examine multicollinearity in regression analysis. For all correlations or comparisons, the statistical significance level was set to less than or equal to .05. For the statistical analysis, the SPSS 22.0 was used.
Results
Five hundred older people were approached from the five municipalities in which the study was conducted. Forty-nine older people refused to participate in the study, resulting in a total sample of 451 older people and a response rate of 90.2%. The majority of older people (61.4%) were women, with an average age of 75.2 years. The largest percentage was either married (46.3%) or widowed (43.9). The largest proportion of older people (40.6%) had completed primary school. Almost all of the older people reported having financial autonomy (94.5%). Nearly half of older people (43%) lived with their family, while many of them were living alone (37.5%). The majority lived permanently in Athens (69.2%) and 17.5% of them were living with their children. Nearly half of them (41.2%) visit KAPI every day, 32.4% meet their children every day. More than half of them had a visit recently and 56.8% declared that had good relations with their neighbors but not friendly (Table 1).
Demographic Characteristics of the Sample of Older People in the Study (N = 451).

When older people were asked to compare their health with their peers, almost half of them (48.1%) said they had a better level of health (Table 1). In the EQ5D scale, most of older people (86.9%) had no problems with mobility or in self-care the majority, as well as establishing daily activities (76.9%). In the field of pain and discomfort, half of the participants reported having some problems, and in the field of anxiety and depression, 43% reported they had some problems and 40% of them reported they had many (Table 2). Results of the VAS scale showed that older people rated their health as moderate (M = 67.8, SD = 19.7). The mean value of the data collected with MSPSS was 61.4, while higher was for support from important others and family and lower from friends (Table 3).
Frequency Distribution (%) of the Six 3-Point EQ5D Questions (N = 451).

Descriptive Statistics of the Data Collected Using the Multidimensional Scale of Perceived Social Support Scale (N = 451).

All scales showed a statistically significant positive correlation between them. There was a significant correlation between MSPSS scale and its two subscales. There is moderate correlation between social support from family and significant others and social support from friends. There is also moderate correlation between social support from family and significant others and EQ5D index or between social support from family and significant others and health status (EQ-VAS). Similar results were found between social support from friends and scales and HRQoL. Finally, there is mediocre correlation was found between EQ5D index and health status EQ-VAS (Table 4).
Pearson’s Correlations (r) Between the Subscales of MSPSS and EuroQol (N = 451).

Note. MSPSS = Multidimensional Scale of Perceived Social Support; EQ-VAS = EuroQol–visual analogue scale.
p < .001.
The questionnaires had a satisfactory internal consistency; the MSPSS showed high internal consistency with α = .91 and from .86 to .95 in its subscales. As for EQ5D, .70 was obtained in this study.
Linear regression analysis showed that some of the demographic were statistically significant in their dependence on EQ5D. All variables with p < .2 were included as independent ones in a multifactorial linear regression analysis with a dependent variable on each of the above-mentioned ranges. Multifactorial linear regression analysis with dependent variable EQ5D was conducted twice, once with the original version of MSPSS (three subscales) and second with two subscales as it was assessed in its Greek language form (Chamboulidou et al., 2016). The multifactorial analysis was performed using the backward method where the final model of SPSS finally shows the variables that influence the dependent variable each time with those with p < .1, and Tables 5 and 6 include those that had a statistically significant relationship (p < .05) with the dependent variables. A VIF was detected to examine multicollinearity in regression analysis. All variables with a VIF > 4 were excluded from the regression analysis. As for EQ5D, there were no problems with the multicollinearity results, contrary to EQ-VAS. After the regression analysis with dependent variable the health status scale (EQ-VAS), two variables (very good relations with neighbors & consumption of more than three medicines) were excluded from the model because of a VIF > 4 in both cases (MSPSS with three and two subscales). The regression was conducted again and independent variables that finally affect EQ-VAS scale examined for multicollinearity are shown in Table 6.
Multifactorial Linear Regression Analysis for the EQ5D With Independent Variables.
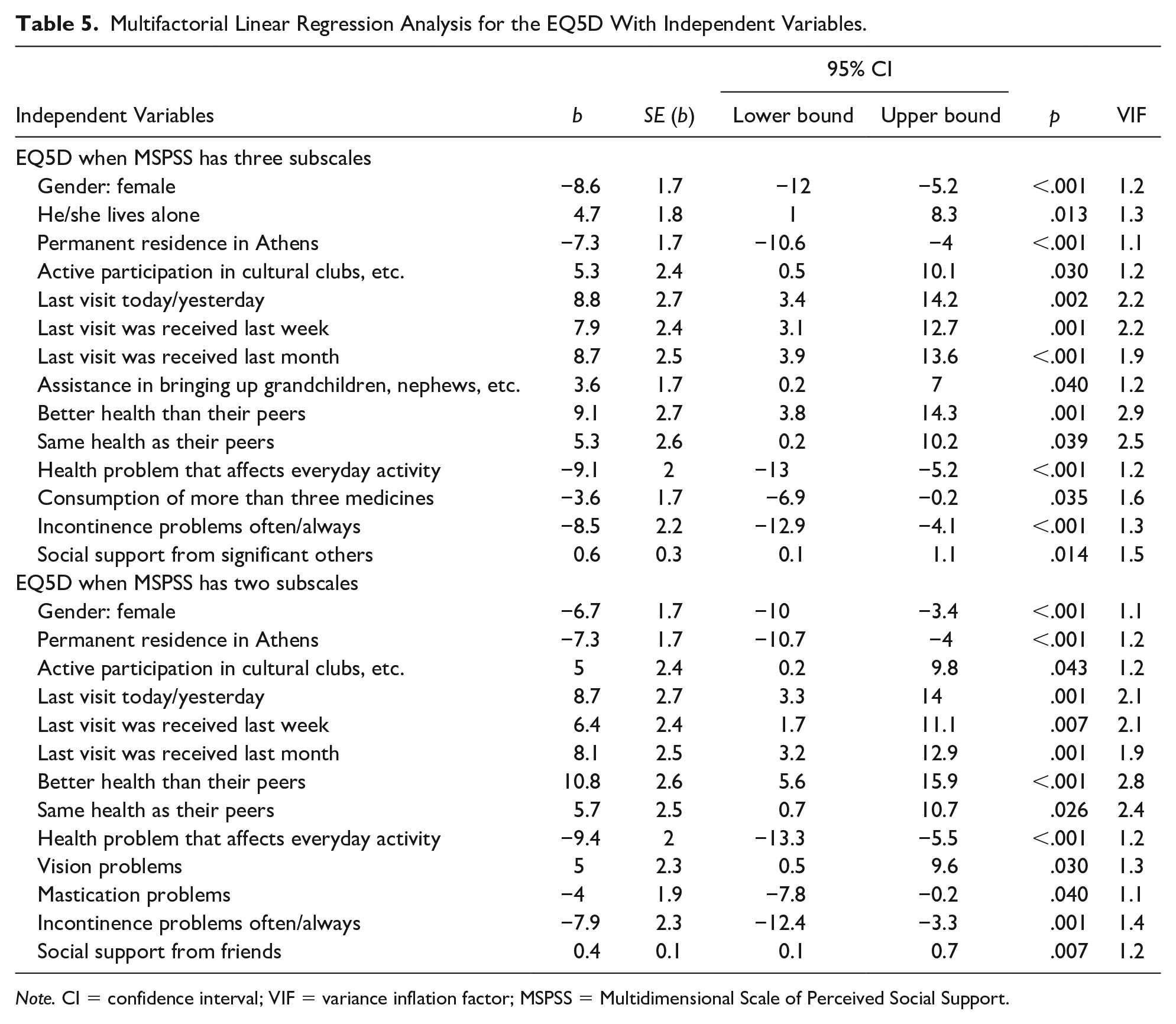
Note. CI = confidence interval; VIF = variance inflation factor; MSPSS = Multidimensional Scale of Perceived Social Support.
Multifactorial Linear Regression Analysis for the EQ-VAS With Independent Variables.
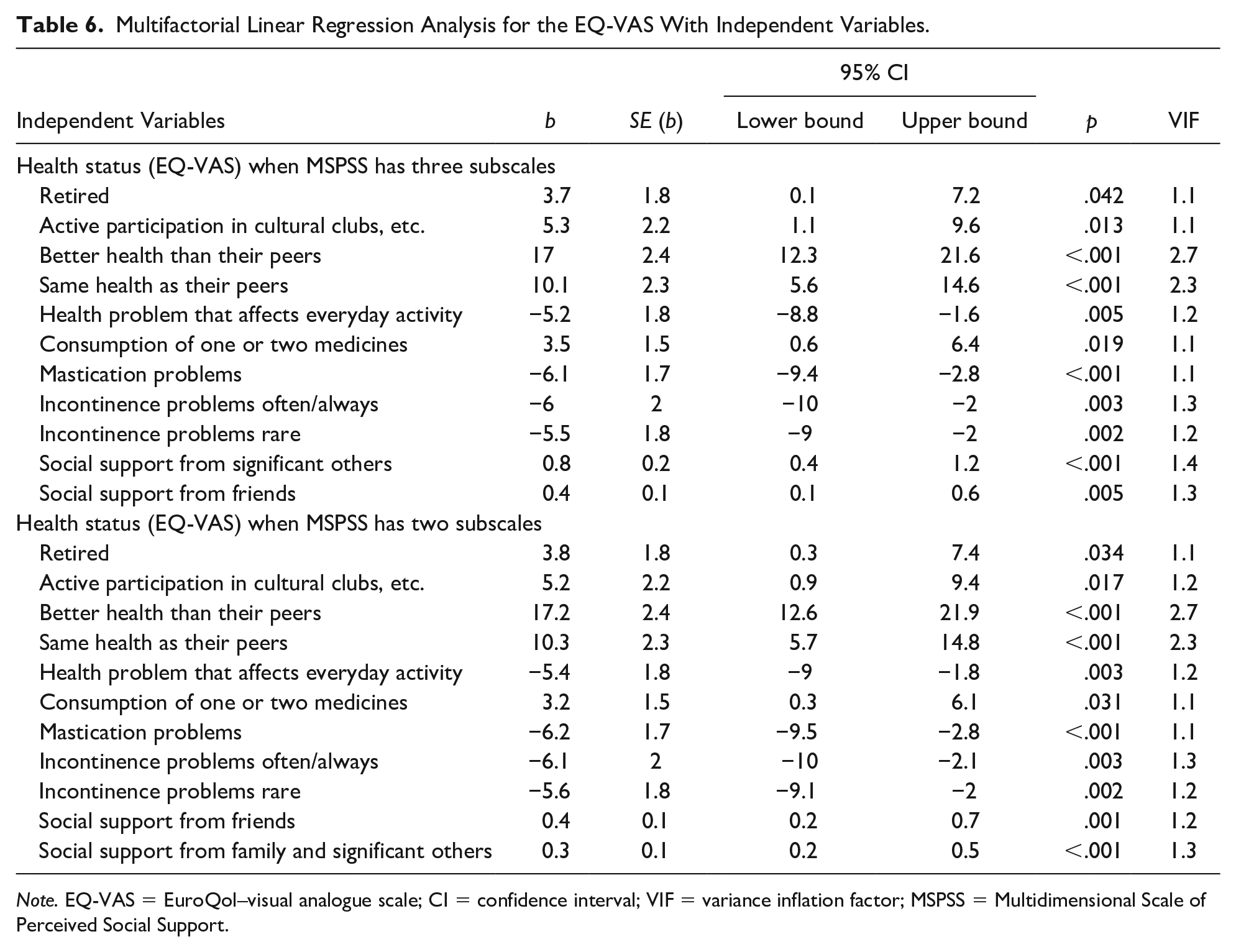
Note. EQ-VAS = EuroQol–visual analogue scale; CI = confidence interval; VIF = variance inflation factor; MSPSS = Multidimensional Scale of Perceived Social Support.
Discussion
The purpose of this study was to investigate the factors that influence the relationship between the supportive environment and HRQoL in older people living in the community. The majority of participants were women, a finding similar to that of other studies (Y. Chen et al., 2014; Unsar et al., 2016). Although there was an effort to have an equal number of men and women, this was not achieved because in most KAPIs women were more and were also more willing to participate in the study. The average age of the sample was 75.2 years, married or widowed and of low educational level, a finding expected for this sample.
In this study, the percentage of older people who maintain their economic self-reliance is slightly higher than those who said they did not. This is particularly important for Greece with the rapid changes that have occurred in the lives of citizens due to the financial crisis that the country went through. The finding, however, that all participants insured and entitled to a pension, is not common with other studies, and this could be explained by the fact that this group lived in a more prosperous economic period. Similar studies indicate that older people lacked economic autonomy (Y. Chen et al., 2014; Unsar et al., 2016). It is also important to underline that permanent residence in Athens is negatively correlated with HRQoL. This finding could be interpreted by the urban lifestyle in Athens. Older people who live permanently in the capital, although they could visit KAPIs and their children may live near them, they still feel loneliness and have difficulties to adapt to everyday challenges due to the aging process, especially when they are widowed or live by themselves; the latter is supported by the study of Nikas et al. (2009) about how older people experience their everyday lives.
HRQoL was reported moderate to high, with the main problems being traced to pain and anxiety/sadness. In Hellström and Hallberg’s (2001) study, older people had a lower quality of life reporting depressed mood, loneliness, fatigue, sleeping problems, and a number of reported diseases that were significantly associated with poor quality of life. Jakobsson et al. (2004) also showed that aging, pain, functional limitations, fatigue, sleeping problems, and depressed moods were associated with poor quality of life.
Social support, as measured by the MSPSS scale, was found to be high by the family and significant others and lower by friends. The finding is explained by the way this generation of older people live, which mainly involves living with the spouse and the wider family. In contrast, in the study of Liao and Brunner (2016), the friendly network as well as the family is positively related to HRQoL, but when both are present, friends seem to offer more benefit to the family. Shin and Sok (2012) showed that older people living with their family rated their health levels higher than those who lived alone, as shown in this study where lower VAS levels had those who reported living alone of those who reported not living alone (p = .004).
Older people who feel good about their health tend to be more satisfied with their lives in general (Efklides et al., 2003). A good perception of health means improved functionality, and it is positively associated with life satisfaction (Cole & Dendukuri, 2004). As life satisfaction increases, depression and poor health decrease (Depp & Jeste, 2006). In this study, health issues such as health problems that affect everyday activity, consumption of more than three medicines, incontinence, and a bad perception about their health leads to lower HRQoL.
Sok and Yun (2011) report that older people who lived with their family had better health than those who lived alone because they had higher social support from the family. Older people live alone because they are able to do so or they have no other choice in life. It is important to note that the percentage of the older people who lived alone in the study of Gallegos-Carrillo et al. (2009)—and in this study—was lower than in other studies (Chalise et al., 2007). Unmarried and those who lived alone according to Gallegos-Carillo et al. (2009) did not show a reduction in HRQoL, and the same finding was reported by Litwin (2010). Similarly, in this study, those who lived alone had a better EQ5D profile. The VAS scale was affected by retirement, participation in community activities, perception of their health compared with their peers, health problems that affect their daily activities, consumption of medicines, mastication problems, incontinence, and social support from significant others and friends.
Verropoulou (2012) analyzed the data from Phases 1 and 2 of the Health, Age and Retirement Survey in Europe and stated that chronic health problems determine reduced self-perceived health. Whenever there is a health problem that concerns them, activities of daily living are affected and health perception is modified (Ocampo, 2010). For this study, it is important to note that older people who successfully treat their health problem report improved VAS. Older people are more likely to feel safer by being treated extensively for their health issues. However, with regard to EQ5D, taking multiple medications is significantly and negatively related to quality of life.
In this study, EQ5D appeared to have a negative relationship with gender (women), which means that women had worse quality of life. This generally is in agreement with similar studies that have investigated the effects of social support on women’s subjective health (Chemaitelly et al., 2013; Cheng & Chan, 2006; Prus & Gee, 2003). Gender effect in this study remained significant and indicated the independent effect of gender on HRQoL scores. Nevertheless, findings of this study are corresponded with other studies (Campos et al., 2014; P. L. Chen et al., 2017; Hajian-Tilaki et al., 2017). The differences which are reported in HRQoL in elderly women may be mainly due to the higher rate of chronic conditions and disability. Although women are generally more sociable, they also have more restrictions in daily activities, something that could explain the HRQoL. The poorer HRQoL in women may be attributable to higher rate of nonfatal disable disorders and the difference in the perceived health between sexes. Women may exaggerate their worse health conditions in their health self-report.
Thus, HRQoL is influenced by older people who live alone, in a way that leads us to the hypothesis that perhaps because they are not restricted by other people, they broaden their social relationships, they are more active—by increasing their social network from which they receive influences continually—and consequently, their quality of life is also increasing. In addition, they live alone and refer to a better quality of life so they are able to self-handle and therefore live alone and have a better quality of life. This is in contradiction with the study of Sok and Yun (2011), who found that living with the family leads to better health and health promotion behaviors, a finding that is also supported by Okkonen and Vanhanen (2006), where they claim that when an older person stays with the family, the positive view he has for himself facilitates health promotion behaviors, but runs counter to Tomaka et al. (2006) where one control group living alone had a lower risk of developing cardiac diseases.
The latter again agrees with the findings of Gallegos-Carillo et al. (2009) where it is shown that the social network plays an important role in HRQoL and the fact that they live alone or not. By comparing two groups, those living alone without a network of close relatives had lower levels of HRQoL compared with those who maintained the network, while the number of friends and relatives increased, the HRQoL was higher.
In societies where family interdependence is important, cohabitation with adult children in a wider family is a common phenomenon. The older people who received more social support from the family reported good self-reported health and low anxiety (Kotkamp-Mothes et al., 2005; Leung et al., 2007). A previous study has shown that support from the “home” of the elderly encourages well-being, autonomy, and participation in activities (Kim, 2007). Golden et al. (2009) showed that social networks independently affect the well-being of older people. Garcia et al. (2006) found that older people with a poorer social network had a worse quality of life. Kahn et al. (2003) showed that the relationship between perceived social support and well-being was quite strong. In the study by Unsar et al. (2016) and that of Y. Chen et al. (2014) found a positive correlation between social support and quality of life of older people. Family is the main source of emotional and social support in Turkey. The latter is also confirmed in other studies (Deng et al., 2010; Huang et al., 2005). In this study, living alone, the assistance in children upbringing, visits from friends with better health than their peers, and participation in clubs and groups with social role as well as social support from significant others or friends have a positive relationship with EQ5D.
In this study, it is shown that despite the double multifactorial analysis with the original version of MSPSS (three subscales), and with two subscales as it was assessed in its Greek language form (Chamboulidou et al., 2016), the factors that affect HRQoL are quite the same with some differences in social support groups.
Limitations
The study presents some design-related limitations, the selection of which was chosen as the most feasible in terms of time and cost. Its cross-sectional type was chosen due to the limited time and the objective difficulty of visiting KAPIs for personal interviews, as long as it was a time-consuming process that was difficult to repeat at different times. Because of its cross-sectional nature, the results present the situation at the given momentum and cannot be used to draw conclusions for the general population of older people is could be used to plan both appropriate interventions to achieve healthy aging and future research.
The sample of the study, although large enough, was a convenience one, which affects representativeness and therefore the generalization of results. In spite of the effort made to get gender and age representation as much as possible from the KAPI members, this was not achieved. In addition, if the same study could include participants from other parts of the country either urban or rural, the findings might have been more representative.
Finally, the way of completing the questionnaire by an interview, although selected to facilitate the process, is a weakness because there was no possibility of confirmation of the results by a second researcher.
Conclusion
HRQoL of older people is affected by their health status as well as by the social support that they receive. Their contact with family, social groups they belong to, and other contacts can increase their level of self-care, HRQoL, and social support despite health problems. This study has shown the relationship between HRQoL and social support of older people living in the community. Results can be used to develop health and social care services for the elderly.
The study of the impact of social support on health, quality of life, and the self-care of older people do not in any way lead to the depletion of relevant research as the achievement of a comprehensive picture of this issue requires further investigation. First, an in-depth study should be carried out to investigate the obstacles to achieve a better quality of life. An appropriate methodological approach would be a prospective study through which the changes in both health and social support could be explored, including a larger sample of older people living permanently away from urban centers. This would make it possible to compare the way of life that may vary depending on whether someone lives in a city or province.
Footnotes
Acknowledgements
The authors thank older people who participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The protocol and questionnaire of the study along with the informed consent form were approved by the Ethics Committee of the Nursing Faculty of the National and Kapodistrian University of Athens. Subsequently, a written permission was sought and granted by each Municipality before stratification of KAPIs.