
Abstract
Introduction
Societies worldwide are aging rapidly, presenting a range of challenges (Aaltonen et al., 2019). In the United States, people aged 65 and over represented 15.2% of the population in 2016, and expected to grow rapidly. In addition, the number of elderly patients with dementia in Japan is currently estimated as 4.62 million and is expected to increase to 7 million by 2025 (Ninomiya et al., 2015; United Nations, Department of Economic and Social Affairs, Population Division, 2017). Compared with a younger population, the elderly patients with dementia are at increased risk of infection, malignancy, or heart failure (Izawa et al., 2016). In addition, because of decreased overall condition that may include lower immunity or dysphagia, the elderly typically require prolonged treatment for acute illnesses, which often involves long periods of intravenous administration. In addition, attitudes regarding life and death are changing with the times; therefore, several treatment options are required (Penders et al., 2017).
Peripherally inserted central catheters (PICCs) are now used as standard practice in various patient populations, as recommended in the Centers for Disease Control and Prevention guidelines (O’Grady et al., 2011; Xiong et al., 2019). Compared with conventional central venous catheters (CVCs), PICCs are less invasive at insertion and less likely to lead to infection (Chrisman et al., 1999; Safdar & Maki, 2005). PICCs are versatile and can be used short- to long-term, from acute to palliative care, and in patients with a variety of underlying conditions, including malignancy, inflammatory bowel disease, amyotrophic lateral sclerosis, and hematologic diseases (Hashimoto et al., 2017; Juntas-Morales et al., 2017; Park et al., 2016). As used in the treatment of various diseases, PICCs also could be a useful option during the treatment of elderly patients with dementia, although to our knowledge, no currently available reports have addressed. Therefore, we conducted a retrospective study to report the experience of using PICCs in elderly patients with dementia.
Methods
Study Setting and Participants
This retrospective observational study was conducted at a single dementia treatment center. We extracted data on all hospitalized patients aged over 65 years in whom the PICCs were inserted from April 2016 through August 2018. The PICCs were inserted for the following reasons: (a) acute treatment in patients who needed, in addition to supplemental nutritional support and dysphagia rehabilitation, intravenous therapy during the acute phase of an illness; (b) end-of-life administration of minimal maintenance doses of intravenous fluids during the terminal stage of a disease; (c) total parenteral nutrition (TPN); and (d) difficulty in obtaining peripheral vascular (PV) access, where PICC was used as an alternative (Figure 1). This study was approved by the human research ethics committee of Toin Hospital (No. TH001).

Flowchart capturing patient inclusion process.
PICCs
The PICCs (Groshong Catheter, NXT single-lumen [4Fr] or dual-lumen [5Fr]; C.R. Bard, Murray Hill, NJ, USA) were inserted into the left or right upper arm in all patients except four, in whose case they were inserted into the femoral regions. The basilic vein was the preferred choice to insert. The PICCs were inserted under maximal barrier protection to prevent infection, and using real-time ultrasonographic guidance (Hitachi Aloka F37, Tokyo, Japan). Thoracic radiography was performed during and after procedure to check the position whether the PICC tip was in superior vena cava. The transparent dressing of the PICC was changed every 48 hr. The same physician, who had sufficient training and experience at inserting the catheters, inserted all PICCs.
Definitions and Data Collection
The catheter-related bloodstream infection (CRBSI) was diagnosed according to the Clinical Practice Guidelines for the Diagnosis and Treatment of Intravascular Catheter-related Infection (Mermel et al., 2009). Briefly, the CRBSI was confirmed either when the same microorganism was isolated from at least one peripheral vein blood culture and from the catheter tip, or from two blood culture samples where one was collected from a catheter hub and the other from a peripheral vein. We recorded instances when the criteria for the CRBSI were not met, despite the existence of positive peripheral blood cultures. Deep venous thrombosis (DVT) was suspected when the limb into which the PICC had been placed was swollen and painful; it was confirmed by ultrasonography. We collected severe bleeding cases both during insertion and postinsertion. Accidental removal was defined as a removal of PICC because of malposition of the catheter tip, including complete accidental withdrawal.
Statistical Analysis
Categorical variables were presented as numbers and percentages (%). Continuous variables were presented as mean ± standard deviations or medians (interquartile range). The incidence of complications was reported as a rate and per 1,000 PICC-days. The PICC lifespan was defined as the number of days from insertion to removal and is presented as Kaplan–Meier estimates. Statistical analyses were conducted using SPSS statistical software (SPSS version 24.0 for Windows; SPSS, Chicago, IL, USA). A p value of <.05 was considered to be statistically significant.
Results
In total, 59 elderly patients with dementia underwent PICC insertion from April 2016 through August 2018 at our institution, and the observation period lasted through September 2018 (Table 1). Reflecting the focus of our institute as a dementia treatment center, the mean age of patients was 83.5 ± 6.9 years. In the acute treatment group (n = 36), pneumonia was the most common indication for PICC insertion (Table 1). In addition, evaluating the patient’s consciousness just before the PICC insertion by alert/verbal/painful/unresponsive (AVPU) responsiveness scale, 78% were alert, 17% were verbal, 5% were painful, and none was unresponsive. The end-of-life care group comprised 10 patients in whom the PICCs were inserted to deliver minimal intravenous fluid support. In addition, the PICCs were inserted in five patients who required TPN. The remaining eight patients did not have any acute illness, however, they required continuous intravenous fluid; because of the difficulty obtaining a peripheral venous catheter (PVC), PICC were inserted instead.
Clinical and Demographic Characteristics of Participating Patients.

Note. BMI = body mass index; HDS-R = revised Hasegawa dementia scale; PICC = peripherally inserted central catheter; eGFR = estimated glomerular filtration rate.
Remaining two groups (13 patients) are not shown in this table; five patients had PICC inserted for total parenteral nutrition and another eight patients for difficulty in obtaining peripheral vascular access.
PICCs were replaced once in six patients and twice in another. Therefore, in total, 67 PICC insertions were made, and no complications occurred at any PICC insertion. In most cases, PICCs were inserted into an upper arm (Table 2). The median PICC lifespan was 42 days (range: 23–87.5; Figure 2). The incidence of the CRBSI was 0.22 per 1,000 PICC-days. Four cases did not meet the criteria of CRBSI despite positive blood cultures. The PICCs were removed promptly upon diagnosis of confirmed or suspected CRBSI.
PICC Insertions and Complications.

Note. PICC = peripherally inserted central catheter; CRBSI = catheter-related bloodstream infection.

Kaplan–Meier curve of PICC lifespan.
The incidence of DVT was 0.66 per 1,000 PICC-days and occurred twice in the same patient. In addition, in our patients who developed DVT, the catheter tip was not dislocated at the time of the diagnosis of DVT. Overall, the most common reason for PICC removal was death of the patient. In the end-of-life care group, nine of the 10 patients received continuous venous infusion by initially inserted PICC without complication for a median of 15 days, until death (Table 3). In the acute treatment group, 19% of the patients resumed oral intake of either blended or more solid food to achieve sufficient nutrition by oral intake only.
Reasons for PICC Removal and Resuming Oral Intake.
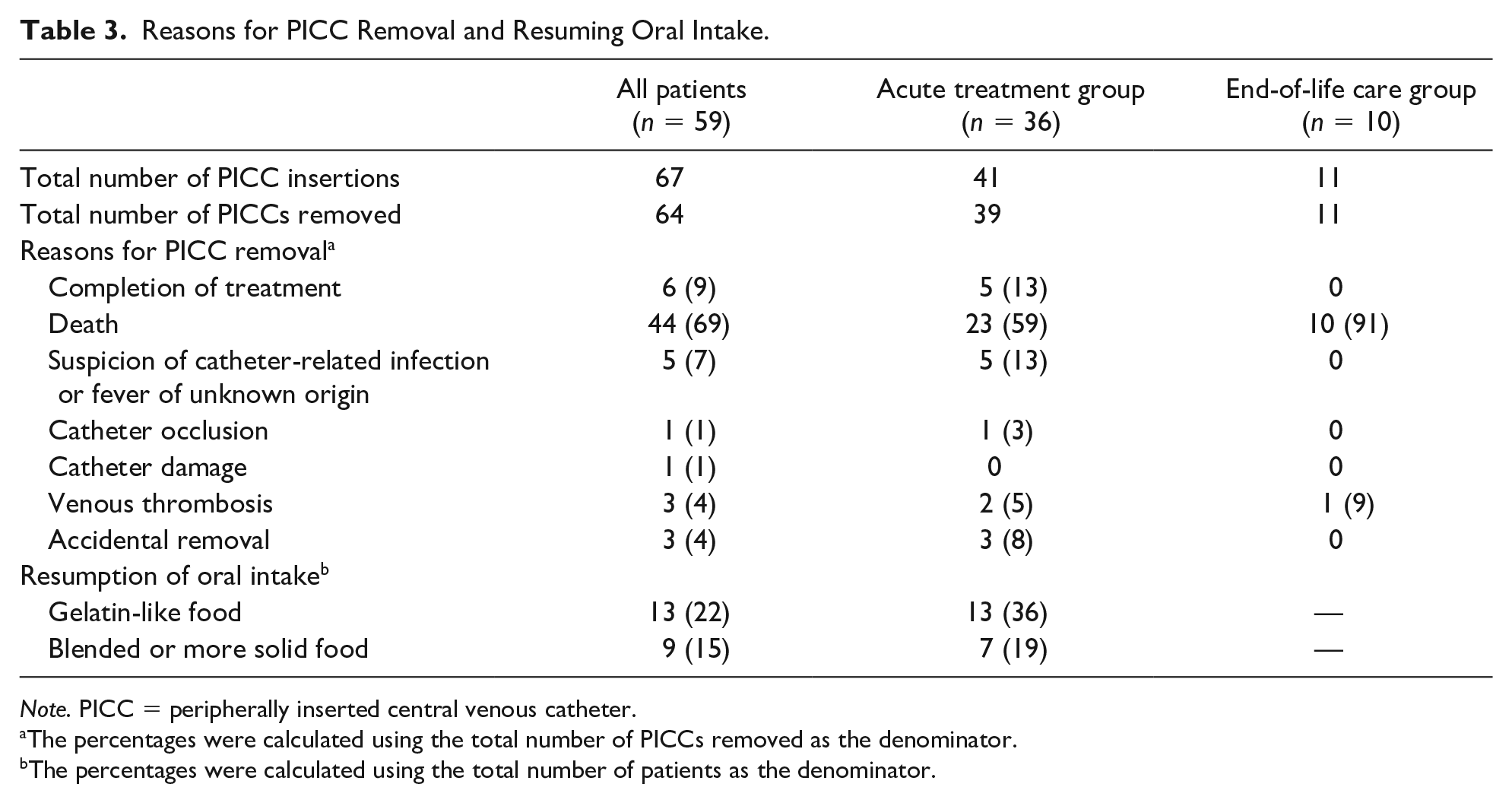
Note. PICC = peripherally inserted central venous catheter.
The percentages were calculated using the total number of PICCs removed as the denominator.
The percentages were calculated using the total number of patients as the denominator.
Discussion
In this study, we have reported the clinical course and rate of complications associated with the use of PICCs in elderly patients with dementia. No severe technical complications occurred at the time of insertion, and PICCs were used for a median of 42 days despite the fact that acute illness was complicated by delirium in most patients in the acute treatment group, or patients were in poor general conditions in end-of-life care group.
Several reports have addressed the usefulness of PICCs in the context of malignancy, neuromuscular disease, or hematologic disease (Hashimoto et al., 2017; Juntas-Morales et al., 2017; Park et al., 2016). In addition, previous research has shown that PICC insertion is a relatively low-risk procedure compared with CVC insertion (Brass et al., 2015; Saugel et al., 2017). For example, Howard et al. reported that the rate of complications at initial PICC insertion was only 0.75% to 1.08%; these complications comprised hematoma or arterial puncture, considered as non-major complications. Furthermore, the risk of inadvertent puncture of nearby vessels or nerves is mitigated when a highly experienced physician inserts the PICC while using real-time ultrasound guidance (Chrisman et al., 1999). Indeed, inserted by well-experienced physician using real-time ultrasound guidance, no technical severe complications at PICC insertion occurred in our study.
Regarding the incidence of the CRBSI, PICCs are considered to be superior or at least noninferior to CVCs. The reported incidence of CRBSI is 2.3 per 1,000 catheter-days for CVC compared with 0.4 per 1,000 catheter-days for PICCs among outpatients, or 2.1 per 1,000 catheter
The major disadvantage of PICCs is their association with the risk of DVT (Chopra et al., 2013; Kang et al., 2016; Nolan et al., 2016; Zochios et al., 2014). In one review, the risk of upper extremity DVT was 8.1 per 1,000 admissions in those using PICCs, compared with 4.8 per 1,000 admissions in patients using CVCs (Winters et al., 2015). In this study, the incidence of DVT was 0.66 per 1,000 catheter-days, comparable to previous studies. Despite the fact that our patients were frail, tended to be lean and small in stature, malnourished, and had severe illness, the incidence of PICC-related DVT was similar to that reported in previous studies of other populations (Chopra et al., 2013; Nolan et al., 2016; Winters et al., 2015). Moreover, no patient in our study population had developed symptomatic pulmonary embolism.
In elderly patients with dementia—especially those with acute illness complicated by delirium—it is often difficult to maintain treatment using peripheral intravenous lines. Peripheral catheters carry a risk of phlebitis, repeat insertion can be difficult, and, most importantly, the risk of self-removal is high in patients with dementia (Sato et al., 2017). In this study, we inserted almost all of the PICCs into the patient’s arm, and self-removal occurred in three cases (median 14 days from insertion) at the beginning of the study and none after the dressing method was devised, covering not only the insertion site but also the proximal site of PICC with transparent dressing, hiding the infusion line under patient’s sleeve, and so on. Consequently, PICCs safely delivered the necessary therapies for a median of 59 days in the acute treatment group.
In elderly patients with dementia, during the acute phase of any illness wherein nutritional therapy is very important, providing enteral nutrition through a nasogastric tube is often difficult to be understood and accepted, and is associated with adverse effects such as aspiration pneumonia. As an alternative to the nasogastric tube, we inserted PICCs to deliver parenteral nutrition only during the treatment period to avert or ameliorate malnutrition. Furthermore, all of our patients in the acute treatment group had disrupted oral intake at the time of acute illness because of dysphagia; therefore, they received dysphagia rehabilitation. Following treatment for their acute illness, total parental nutrition using PICC, and 1 to 2 months of dysphagia rehabilitation, 19% of the patients in acute treatment group were able to consume sufficient oral intake of blended or more solid food. Thus, PICC played an important role for preventing the deterioration of the nutrition state.
In this study, we have demonstrated the importance of PICC use during end-of-life care. In our hospital, we have multiple, thorough, interdisciplinary discussions, involving the patient and patient family, regarding the patient’s end-of-life care, particularly at the time of hospitalization, during acute illness, and at diagnosis of poor oral intake. If the choice of end-of-life care involves the administration of minimal intravenous maintenance fluids, the PICC insertion is discussed. Once PICC is inserted, the patient is relieved from frequent punctures, phlebitis, ecchymoma, and local edema, thus improving patient comfort and family satisfaction. In one noteworthy case, PICC insertion enabled our patient to shift to home medical care and to spend the last 3 weeks toward the end of life with family. In addition, in 23 patients of the acute treatment group, their swallowing function was cautiously assessed through 2 to 3 months of dysphagia rehabilitation and, ultimately, diagnosed as irreversible dysphagia. Afterward, the treatment plan was shifted to end-of-life care, involving administration of minimal maintenance doses of intravenous fluids through a PICC. We noted that 43% of these patients were able to consume a small quantity of gelatin-like food for a certain period immediately before death.
This study has several limitations. First, the current retrospective observational study was conducted only at a single institution. Second, because of the limited number of participants, we could not compare incidence between the acute treatment and end-of-life care groups. Third, the same physician inserted all PICCs in this study; therefore, the incidence of technical complications during insertion might not have been comparable to those of larger trials where varied levels of personnel experience might contribute to the risk of complications. Fourth, PICCs of only one brand—most of which were single-lumen devices—were used. However, these third and fourth limitations mentioned above enabled us to interpret the results without a bias of interpractitioner or interdevise. Finally, we did not collect data from patients who decided not to receive intravenous therapy or undergo PICC insertion.
Conclusion
In conclusion, we have reported the use of PICCs in elderly patients with dementia. In particular, although the indications for PICC insertion should be interdisciplinary discussed and carefully considered for each patient, these devices facilitated therapy in elderly patients with dementia during acute illness, even when complicated by delirium, as well as during end-of-life care.
Footnotes
Acknowledgements
We would like to express our greatest appreciation to Kouhei Miyauchi, the Vice President of Toin hospital for his general support.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Y.N. and T.K. belong to the endowed department by Actelion Pharmaceuticals Japan Ltd. Other authors declare they have no conflict of interest to disclose.
Ethical Statement
Study was carried out in accordance with the Declaration of Helsinki and approved by the Institutional Ethical committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.