
Abstract
The rapid increase in immigration to the United States in the past decades has resulted in an influx of individuals who have to familiarize themselves with a completely new health care system and practices, often in a new language. The purpose of this study was to assess health literacy and investigate its correlates among older U.S. Polish immigrants living in the Greater Chicago area. We conducted a cross-sectional study on 60 older adults (24 men, 36 women; mean age = 71.1 years) who completed the Short Test of Functional Health Literacy (S-TOFHLA) and a demographic survey. Scores on S-TOFHLA were lower among older and less-educated immigrants. Undocumented immigrants reported using health care services less frequently than those with legal status. These results confirm the findings of previous studies that older age and fewer years of education are associated with inadequate health literacy. Being familiar with at least the basic information about one’s condition will help patients to better understand a diagnosis, manage their symptoms, and improve any preventive treatment. The findings emphasize the importance of health education among older Polish immigrants. More research employing diverse groups of immigrants is needed to better understand the factors associated with health literacy.
Introduction
Currently there are 43.3 million immigrants constituting 13.5% of the nation’s population, and this number is projected to increase to 18% during the next 40 years (López & Radford, 2017). This demographic shift and increase in the number of immigrants pose challenges to the health care system. Taking into account the increasing number of immigrants, there is a growing interest among researchers and health care professionals in preparing themselves to adequately address and treat immigrants’ health concerns. This includes reducing factors that lead to health disparities and barriers to health equality. One important issue where immigration and health care intersect pertains to health literacy, a concept introduced in the early 1970s (Nutbeam, 2000). Although it has been conceptualized in various ways, health literacy is often defined as a patient’s ability to obtain, process, and understand basic health information and services needed to make appropriate health decisions (e.g., Nielsen-Bohlman et al., 2004; Ratzan & Parker, 2004). In other words, patients with adequate health literacy possess a set of skills, including writing (i.e., filling in forms), reading, and comprehending health-related materials such as appointment cards, prescriptions, medicine labels, and directions for home health care (Parker et al., 1995).
The numerous negative consequences of having inadequate health literacy have been identified in various studies as low health literacy has been associated with increased mortality, longer periods of hospitalization, inadequate disease management, and poor adherence to a treatment regimen (D. W. Baker et al., 2002; Ngoh, 2009; Pignone & DeWalt, 2006). Studies have also demonstrated that individuals with low health literacy are less likely to engage in preventive measures such as vaccinations, mammograms, Pap smears, and other routine screenings (Scott et al., 2002; Sun et al., 2013). A poor understanding of preventive care information and an underutilization of preventive resources among patients with inadequate health literacy often result in a higher use of emergency services, which in turn lead to higher health care costs (D. W. Baker et al., 2002; Bennett et al., 2009).
Most of the research focusing on demographic factors indicates that age, education, language, and culture can significantly affect a person’s health literacy skills (e.g., Christy et al., 2017; Protheroe et al., 2017). In fact, older adults, racial and ethnic minorities, and individuals with low income and low educational attainment (less than a high school degree or General Educational Development [GED] certificate) are more likely to have inadequate health literacy (National Center for Education Statistics, 2006). The 2003 National Assessment of Adult Literacy (NAAL) revealed that those aged 65 and older have the smallest proportion of individuals with proficient health literacy skills (Kutner et al., 2007). This group also includes the highest proportion of individuals with health literacy defined as “below basic” (Manafo & Wong, 2012). Being an immigrant is also a risk factor that contributes to poorer health literacy, especially among older adults with low educational attainment (Bennett et al., 2009).
Inadequate health literacy in developed countries, which ranges from 7% to 47% (Nutbeam, 2008), has become a high priority public policy issue tackled by governmental agencies. The U.S. Department of Health and Human Services (HHS) in its report “The Healthy People 2020,” which describes national goals and objectives for improving the health of all Americans, placed emphasis on health literacy as a key issue in the Health and Health Care domain. The HHS’s agenda recognized that adequate health literacy may positively affect individuals’ capacity to take responsibility for their and their family’s health needs and, therefore, a National Action Plan to Improve Health Literacy was developed. The plan is based on two principles: (a) every individual has the right to health information that helps them make informed decisions and (b) health services should be delivered in ways that are easy to understand and that improve health, longevity, and quality of life. The HHS also recognizes the importance of improving health literacy across different cultures because one of the strategies for implementing the plan highlights actions including supporting and expanding local efforts to provide adult education, English language instruction, and culturally and linguistically appropriate health information services in the community (U.S. Department of Health and Human Services, 2010). Achieving this goal is especially important for immigrants.
Addressing the issue of health literacy among immigrants living in the United States (especially older adults) is of critical importance. Similar to the general population, limited health literacy among immigrants has been linked to increased health disparities and a poor understanding of one’s condition and disease management (Grubbs et al., 2009; Safeer & Keenan, 2005) which, in turn, can lead to an exacerbation of health issues and high medical expenses (Howard et al., 2005; Noureldin et al., 2012). The prevalence of chronic health conditions increases with age (Vogeli et al., 2007); therefore, it can be anticipated that as the population ages, the proportion of older immigrants who need professional health care will rise.
What is known about health literacy among immigrants is largely based on the country’s Spanish-speaking population. According to recent estimates, Mexicans are the largest group of immigrants and account for approximately 26% of the total share of immigrants in the United States (López & Radford, 2017). Research has shown that health literacy may differ depending on race or ethnicity (Chaudhry et al., 2011), but one of the limitations of existing research on health literacy is that immigrants are still often aggregated into one homogeneous group. This approach undervalues the role of culture. Immigrants are not a homogeneous population because each group has a unique culture, different systems of health and illness beliefs, and health habits (Nielsen-Bohlman et al., 2004). For instance, when treating medical conditions, some cultures rely on various complementary and alternative medicine methods more often than others (Suzuki, 2004).
Given the ethnic and linguistic diversity of individuals living in the United States, studies should include data from diverse groups of immigrants to gain a better understanding of factors influencing health literacy. Conducting research on health literacy among immigrants from different groups is also important for designing interventions. Without a more comprehensive understanding of health literacy, interventions designed to improve patients’ abilities to understand medical information may not be effective for particular groups as the interventions may fail to consider different cultures.
In addition, one of the major drawbacks of the existing research is that it fails to assess whether immigration status influences health literacy. There are reasons to include immigration status as an important variable. Although the majority of foreign-born individuals are naturalized citizens or lawful permanent residents (77%), according to the Department of Homeland Security’s estimates, there are 12.1 million unauthorized immigrants (foreign-born noncitizens who are not legal residents) living in the United States (B. Baker, 2017; Passel & Cohn, 2019). This population of undocumented immigrants is especially vulnerable because they are often uninsured or underinsured, they tend to have higher rates of illiteracy, and they underutilize the health care system when compared with native-born individuals (Hacker et al., 2015; Preibisch & Hennebry, 2011 ).
The purpose of this study was to assess health literacy and examine its correlates among first-generation Polish immigrants living in the Chicago area. The population of Polish immigrants in the United States is understudied. To the best of our knowledge, there are no studies that focused specifically on the health literacy of Polish immigrants living in the United States. Studying this particular population seems to be important because, according to a survey conducted in European countries, only 46% of Polish people trust their physicians, which is one of the lowest levels of trust in Europe (the European average is 76%; Łosiewicz & Ryłko-Kurpiewska, 2015 ). Therefore, Poles tend to delay seeking medical advice and instead rely on information provided by their friends and family members. Avoiding seeking medical advice in combination with limited health literacy may lead to an underuse of preventive medicine and poor disease management. The overarching aim of this study was to add to the state of knowledge in the field of health literacy by studying its correlates among Polish immigrants.
Method
Data and Sample
The data for this study were gathered from a convenience sample of 60 older adults living in the Chicago area. This area was chosen because it has the largest share of Polish immigrants living in the United States. Participants were recruited through flyers distributed in a Polish community and nearby communities and snowball sampling (older adults referred peers to researchers). Eligible participants were 60 years of age or older, suffering from at least one chronic health condition, having been born in Poland, and immigrants to the United States. The study was conducted between November 2017 and February 2018. We examined self-reported health status, the utilization of health care services, health literacy, and demographic variables using a questionnaire. Participants received verbal information about the purpose of the study and the conditions of participation (including confidentiality and the right to withdraw from the study). All participants provided informed consent prior to participation. There were no incentives for participation.
Measures
The key independent variable in our study was health literacy, which was assessed using the Short Test of Functional Health Literacy in Adults (S-TOFHLA), a shortened version of the Test of Functional Health Literacy (D. W. Baker et al., 1999). Upon receiving the test authors’ permission, the test was translated into Polish by two independent translators with a psychology background who applied a forward–backward method. The forward–backward translation method ensures comparability of the translated measure by translating it from the source language into the target language (forward translation), and then translating the target language back into the source language (back translation), (Tsang et al., 2017). The backward translation was compared with the original measure. Any discrepancies were discussed among the research team and the translator until consensus was reached. To evaluate the wording and understanding of the translated test, the authors conducted a pilot study with a monolingual sample of 10 individuals.
The S-TOFHLA is a practical measure of functional health literacy with good reliability and validity (Cronbach’s α = .68 for numeracy items and .97 for prose passages). It uses practical tasks related to health care settings. The S-TOFHLA consists of two passages that use a 36-item test to measure a patient’s reading comprehension skills. In each passage, every fifth or sixth word is missing and the respondent has to insert the word that best completes the sentence using a word from a set of four possibilities. The total score on the test is 36 points (with each item worth one point). Individuals scoring between 0 and 16 points are considered to present inadequate health literacy, between 17 and 22 points demonstrates marginal health literacy, and those who scored between 23 and 36 points present adequate health literacy (D. W. Baker et al., 1999). The test was chosen because it is one of the most frequently used measures of health literacy (Housten et al., 2018).
Respondents were also asked to rate their general health status (“Would you say that in general your health is excellent, very good, good, fair, or poor?”). The scale ranged from 0 to 4 points. Higher scores indicate better self-reported health.
A presence of medical conditions was self-reported by respondents indicating one or more conditions from a series of noncommunicable diseases (high blood pressure, angina, arteriosclerosis, congestive heart failure, ischemia, stroke-related conditions, pulmonary diseases, chronic obstructive pulmonary disease and asthma, chronic kidney disease, cancer, diabetes, and stroke). Although dementia belongs to one of the most common noncommunicable diseases, we excluded patients suffering from dementia because previous research has shown that the S-TOFHLA is not a suitable tool for measuring literacy in patients with cognitive impairment (de Oliveira et al., 2014). We also asked about the frequency of health care services utilization (measured by the number of doctor visits per year).
Sociodemographic variables included age, gender, education, length of living in the United States, and immigration status.
Analyses
First, descriptive statistics were calculated to describe the characteristics of study participants. Scores on the S-TOFHLA were categorized as inadequate (0–16 points), marginal (17–22 points), or adequate (23–36 points). Educational attainment was categorized into three groups: less than a high school diploma, high school diploma or GED equivalent, post high school education (some college, associate degree, bachelor’s degree, master’s, or doctorate). We calculated the Spearman correlation coefficients to examine the relationships among all variables. The preliminary results revealed that the data were not normally distributed. The S-TOFHLA scores indicated a negatively skewed distribution, with the majority of participants obtaining fewer than 22 points. Therefore, to determine whether or not documented and undocumented immigrants differed significantly on the key study variables, Mann–Whitney tests were calculated. A p value of .05 was used to indicate statistical significance. All statistical analyses were performed using SPSS Statistics v25 software package (IBM Corp., 2017, Armonk, NY).
Results
Table 1 presents means and standard deviations calculated for each study variable. We also divided the sample into two subsamples based on their legal status (see Table 1). Participants’ ages ranged from 65 to 80 years, with a mean of 71.1 years (SD = 4.4). Men comprised 40% of the sample. Nearly 70% of participants self-described themselves as monolingual (did not speak English well) and 53% completed high school. The majority of the respondents had been living in the United States for seven or more years (M = 11.7, SD = 5.8). Twenty-one participants (35%) were undocumented immigrants. Having more than one chronic health condition was reported by 56% of participants. Twenty-eight participants reported poor or fair health status. The mean S-TOFHLA score out of 36 was 20.4 (SD = 5.4). Seventeen respondents (27%) had scores in the inadequate health literacy range. Twenty-six respondents (43%) had marginal and 18 (30%) had adequate health literacy. The Mann–Whitney tests did not indicate differences between the S-TOFHLA scores based on legal status, but the test revealed that legal immigrants utilized health care services more often than undocumented immigrants (p = .23).
Sample Demographic, Health Status, Health Literacy, and Health Care Service Utilization by Legal Status.
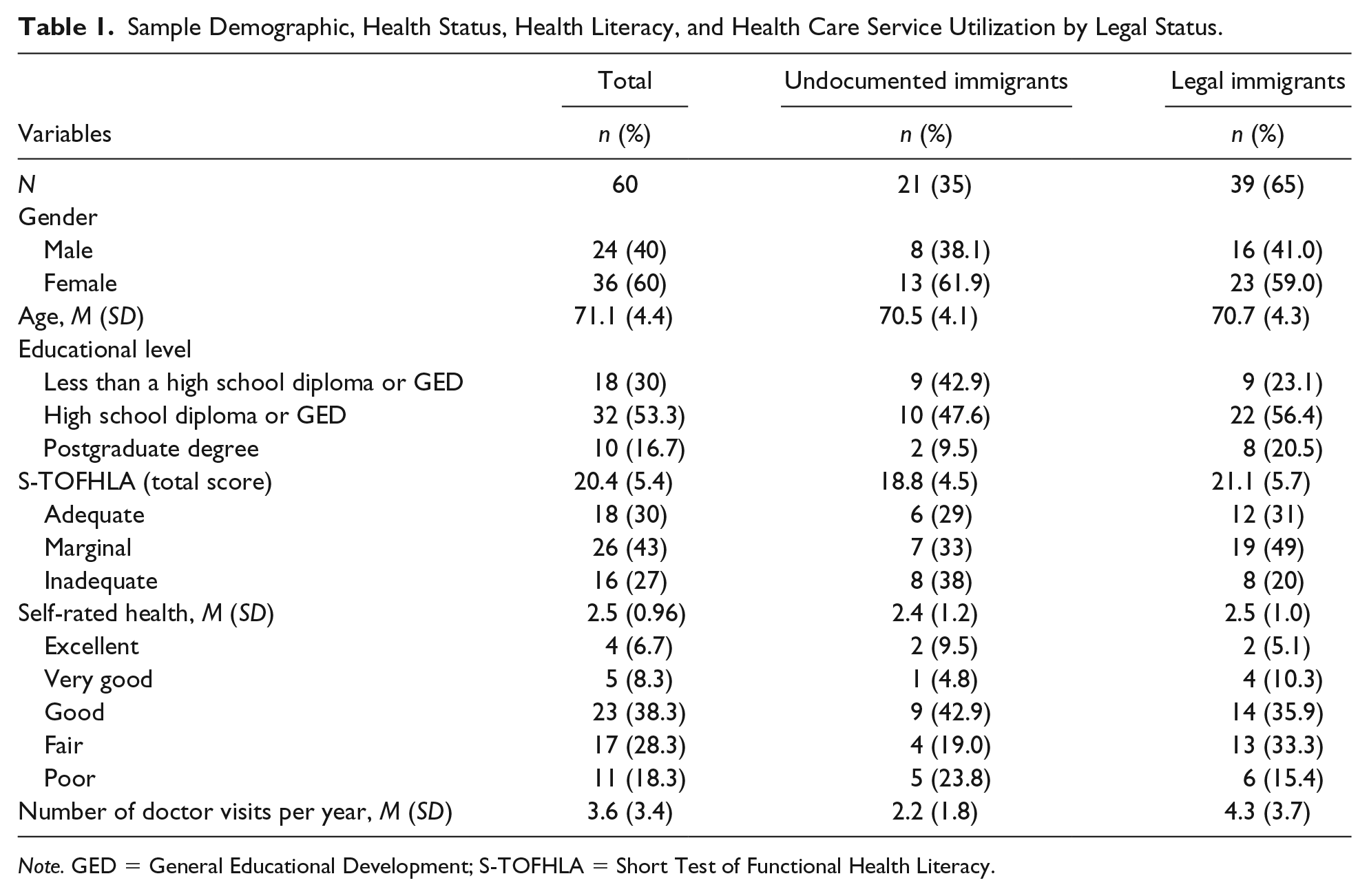
Note. GED = General Educational Development; S-TOFHLA = Short Test of Functional Health Literacy.
Bivariate correlations indicated that health literacy was significantly positively correlated with education, r = .70, p < .00 (Table 2). Health literacy was negatively correlated with age. The older the immigrants were, the fewer points on the S-TOFHLA they received (r = .39, p < .00). Health literacy was also associated with self-rated health (r = .45, p < .00). Utilization of health care services was positively associated with education, r = .28, p = .33. Health literacy was not associated with the length of residence in the United States nor with the number of chronic health conditions. The observed correlations stratified by legal status were similar. However, they should be treated with caution due to the limited sample size (only 21 were undocumented immigrants).
Correlations Among Variables for the Total Sample.

p < .05 level (two-tailed); **p < .01 level (two-tailed).
Discussion
The primary purpose of the study was to assess the health literacy levels of older Polish immigrants who live in the Chicago area, the largest Polish community outside of Poland. Our findings support previous studies which demonstrated the relationship between inadequate health literacy, lower educational attainment, and older age (D. W. Baker et al., 2002; Schillinger et al., 2002). We found a significant association between education and age. Older and less-educated immigrants obtained lower scores on the S-TOFHLA, whereas immigrants with a higher educational attainment utilized health care services more often. Health literacy was also associated with self-rated health and immigrants with higher levels of health literacy reported better overall health. Health literacy was not associated with the length of residence in the United States or with the number of chronic health conditions. Although we found an association between health and education, some researchers argue that years of education do not fully explain the differences in health literacy (Morrow et al., 2005). Therefore, more research is needed to investigate the demographic correlates of health literacy and mechanisms to explain these associations.
Although we did not observe any statistically significant differences in regard to health literacy based on the participants’ legal status in the United States, the results demonstrated that legal immigrants utilized health care services more often that undocumented immigrants. This finding should not be surprising because undocumented immigrants have a limited access to coverage options due to their status and, therefore, the majority of them remain uninsured (Kaiser Family Foundation, 2019). As a result of a limited access to coverage options, undocumented immigrants tend to delay seeking medical help. Data have also shown that undocumented immigrants use health care less frequently because of the fear of deportation (Gusmano, 2012; Kaiser Family Foundation, 2019).
In our sample, we observed that 27% of participants had inadequate health literacy. These results are similar to findings obtained by Paasche-Orlow and colleagues (2005), who in their pooled analysis of data from 85 studies conducted in the United States revealed that the weighted prevalence of low health literacy was 26%. Studies conducted in the general population have demonstrated that patients do not always understand prescription instructions and often forget a significant amount of information they received from their health care professionals (Jimmy & Jose, 2011). Given that inadequate health literacy can negatively impact an individual’s mental and physical health, it is important to design interventions that could facilitate communication between patients and health care providers and help immigrants to increase their level of understanding of medical instructions. In addition, strategies applied to the population of immigrants can possibly benefit other populations.
To reduce the adverse consequences of inadequate health literacy, such as increased hospitalizations or higher mortality rates, it is crucial to provide sufficient information about patients’ specific health conditions and to make sure that they understand medical instructions. Research has shown that physicians tend to overestimate patients’ literacy abilities (Bass et al., 2002). Understanding instructions may be difficult for immigrants with both low health literacy and limited English proficiency. An effective strategy to improve patients’ understanding of their health conditions is to provide clear written information, including how long and when exactly the medication should be taken and list the possible side effects (Jimmy & Jose, 2011). Previous research has demonstrated that information leaflets including pictograms and text increased the medicine-related knowledge in patients compared with longer and text-only leaflets (Mansoor & Dowse, 2007). It has been also advised to use simple, everyday language and avoid medical jargon as well as idioms (Jimmy & Jose, 2011; Katz, 1997).
Previous studies also suggest the need to increase cultural awareness among health care professionals (Kimbrough, 2007). Some patients feel embarrassed and do not want to admit that they struggle with understanding health information. To maintain their dignity, these patients hide their limited ability to read or speak English (Parikh et al., 1996). Cultural barriers and economic challenges can present additional obstacles to access, obtain, and understand health care information (Kreps & Sparks, 2008). Health care providers play an important role in improving patients’ health literacy; therefore, they should be more aware of the culture and social influences that also play a role. It is especially important among Polish immigrants because it is common in their culture to rely on a patient’s own experience or ask friends for medical advice (IPSOS, 2009). According to a national survey, only one third of Polish patients adhere to their physician’s recommendations (Centre for Public Opinion Research, 2018).
This study contributes to the literature of health literacy by demonstrating that age and educational attainment play an important role in understanding health literacy and utilizing health care services among Polish immigrants. However, it has several limitations. The first limitation of this study is that it examines older Polish adults living in the Greater Chicago area. Therefore, findings cannot be generalized to other populations of Polish immigrants living in other geographic areas of the United States nor can they be generalized to other immigrants. Second, a relatively small sample size, which included 60 immigrants and lacked a comparative group (e.g., younger adults), also limits the generalizability of the findings. Another limitation was that data were gathered using self-reporting. The main disadvantage of self-reporting is that there are a number of potential validity problems associated with this method because self-reporting measures allow respondents to strategically modify their responses to suit their particular self-presentation motives (Johnson & Richter, 2004). Fourth, we employed convenience sampling which is a commonly used, nonprobability sampling technique. Although this technique is widely used and efficient, it has several limitations including a higher level of sampling error (Battaglia, 2008). Taking into account the limitations, our findings should be considered preliminary. Future research should incorporate larger samples of immigrants and combine qualitative and quantitative methods to gain a better understanding of the barriers that immigrants may face while managing their health conditions. Future research could also explore the correlates of health literacy by comparing the results of individuals from different age groups.
Despite these limitations, this is one of the first studies to investigate health literacy among Polish immigrants. The results of the study emphasize the importance of health education among individuals with limited English skills and provide insights into older immigrants’ perceptions of how their legal status may influence their decisions on whether or not to see a health care professional.
Conclusion
Health literacy has gained more attention and is being recognized as a major public health concern (Centers for Disease Control and Prevention, 2018). There is substantial variation among immigrants not only with respect to their country of origin but also with respect to age, education level, or legal status within groups of the same foreign descent. It is important to investigate health literacy across different groups as it may help health care providers to facilitate communication and informed decisions and adequately respond to the needs of diverse groups of immigrants. Knowledge about the most common chronic health conditions is crucial because awareness of a disease’s symptoms may prompt the individuals to seek help at an earlier stage of the disease, which could improve the efficacy of treatment. Our preliminary findings point to the need for improving the health literacy of older Polish immigrants. Further research is needed to investigate the correlates of health literacy among diverse groups of immigrants.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.