
Abstract
Objectives:
Older adults with impaired physical function are at risk for further functional decline in part due to limited ability to engage in regular exercise. Effective approaches to exercise in this vulnerable population are needed to improve functional capacity and optimize independence.
Methods:
Thirty-two residential care apartment complex (RCAC) residents, age ≥70, with low short physical performance battery (SPPB) scores were recruited and randomly assigned to a crossover-design study exploring feasibility and safety of semi-recumbent vibration exercise in older adults living in one RCAC. The primary outcomes were retention and adherence rates and adverse events.
Results:
The retention rate was 78%. Adherence rate was 79.7% and 78.6% during the vibration and control training sessions, respectively. Thirty-eight adverse events (AEs) occurred. Mild muscle soreness and knee pain were the only AEs related to vibration exercise. No serious adverse events (SAEs) were study-related. Participants were able to increase training intensity and load and rated the training enjoyable.
Conclusion:
Semi-recumbent vibration exercise was feasible, well tolerated, and safe in RCAC residents with reduced physical function. Future studies need to examine the effect of this type of exercise on physical function, mobility, falls, and quality of life.
Introduction
Sarcopenia, the age-related decline in muscle mass, strength, and function, becomes common with advancing age and is associated with dependency, falls, fractures, morbidity, and mortality (Cruz-Jentoft et al., 2019). These negative consequences reduce quality of life and lead to increases in hospitalization, long-term care use, and health care costs (Bruyère, Beaudart, Ethgen, Reginster, & Locquet, 2018; Hirani et al., 2015). It is apparent that clinical recognition of sarcopenia and interventions for prevention and management may have major benefits including reduction of falls and fractures, maintained independence, and reduction of health care costs.
Sarcopenia is particularly prevalent in institutionalized older adults (Shen et al., 2018; Taani et al., 2018). This is not surprising because sarcopenia is a major contributor to increased dependency and frailty and a major reason precipitating movement to assisted living or nursing home environments (Hirani et al., 2015). Interventions to improve or maintain functional status may optimize independence for older adults thereby enhancing quality life and decreasing use of expensive health care services (Beaudart et al., 2017).
Exercise is an attractive intervention to mitigate sarcopenia and thereby maintain function among older adults (Dent et al., 2018). However, adherence to exercise recommendations is very low in this population. Failure to exercise among older adults may reflect cognitive decline and/or other comorbidities including cardiac, respiratory, and vascular disease (Keadle, McKinnon, Graubard, & Troiano, 2016). As such, novel approaches allowing older adults with comorbidities to experience the benefits of exercise are urgently needed. In this regard, vibration exercise is a promising modality as it may not cause substantial cardiovascular stress.
Whole-body vibration (WBV) exercise has been reported to be effective and safe in older adults and is feasible in individuals with comorbidities (Rogan et al., 2017; Sitjà-Rabert et al., 2012). However, most current WBV exercise devices require standing on a platform, necessitating concentration, musculoskeletal coordination, and some degree of stamina. These requirements may preclude older adults with cognitive and physical impairment from standing WBV exercise. Indeed, most prior WBV studies were conducted among community-dwelling older adults with high levels of independent functional ability (Rogan et al., 2017; Sitjà-Rabert et al., 2012). To overcome the limitations of standing WBV, a novel vibration system (VibeTech One®) has been developed allowing for seated exercise in frail older adults.
There is a gap in understanding the use of WBV for older adults living in residential care apartment complexes (RCACs) that are a part of a continuing care system. Residents living in these settings with decline in function are particularly at risk for moving to assisted living or skilled care. Hence, the purpose of this article was to evaluate the safety and feasibility of semi-recumbent vibration exercise in older adults living in an RCAC. The effect of semi-recumbent vibration exercise on muscle mass, strength, and function will be analyzed by other team members.
Materials and Methods
Sample, Setting, and Design
Of the 63 invited, 32 residents with decreased physical function were recruited from one RCAC in the Midwestern United States to participate in a randomized crossover-design study examining the feasibility and effectiveness of semi-recumbent vibration exercise. RCAC is defined as a place where five or more adults reside, consisting of independent apartments, and providing not more than 28 hr per week of supportive, personal, and nursing services. Study inclusion criteria included English-speaking, age ≥70 years, ability to stand independently, free of major acute illness, a short physical performance battery (SPPB) score ≤9 or ≤2 in any of the three sections (balance, gait speed, or chair rise), ability and willingness to sign informed consent and to train for 10 min, 3 times per week for two 8-week periods. Excluded were those with injury or surgery in the past 6 months that limited ambulation or ability to perform muscle and physical function tests and those who were not able to stand without assistance. Use of assisted devices such as a cane or walker was allowed. The study was approved by the University of Wisconsin–Madison Health Sciences Institutional Review Board (IRB) (Study ID number 2015-0480). All 32 participants provided written, informed consent prior to conduct of any study procedure.
A baseline visit consisted of questionnaire administration, muscle and physical function, and body composition assessments, all specified and described below. Participants were then randomly assigned to initiate study participation with the vibration treatment or sham treatment. The treatment was conducted 3 times per week for 8 weeks. At the end of this training cycle, muscle and physical function and body composition assessments were repeated by assessors blinded to training assignment, then participants were given a 4-week washout period, and the same assessments were repeated at 12 weeks. Participants then crossed-over to the opposite training group for another period of three weekly training sessions for 8 weeks. After this period, at 20 weeks, blinded assessors conducted a final visit repeating the same assessments (Figure 1).

Study flowchart.
Semi-Recumbent Vibration Exercise Overview
The VibeTech One® (VibeTech, Inc., Sheboygan, WI, USA) chair allows vibration exercise in a semi-recumbent position (Figure 2). This system allows vibration exercise for older adults with comorbidities that prevent them from performing standing vibration exercise or traditional exercise (Merriman & Jackson, 2009). The device is configured to allow users to receive vibration training to their legs while seated and performing leg presses against the system’s vibrating footplate. The applied load simulates the weight of standing (or partial bodyweight) by applying force on a footplate, while restraining movement of the knees and back. The footplate is force-driven with a robotic loading mechanism that supplies between 5 (2.3 kg) and 100 lbs (45 kg) of force to the user’s legs depending on the participant’s ability level. This force is increased over time as tolerated by the user. The footplate moves slowly, taking between 20 and 30 s to complete a leg press, depending on the range of motion of the participant. This encourages the participant to apply slow and controlled pressure while vibrations are transmitted through the major muscle groups of the legs (quadriceps and hamstrings) and while the muscles traverse throughout their physiological range of motion (0-90 degree knee flexion).
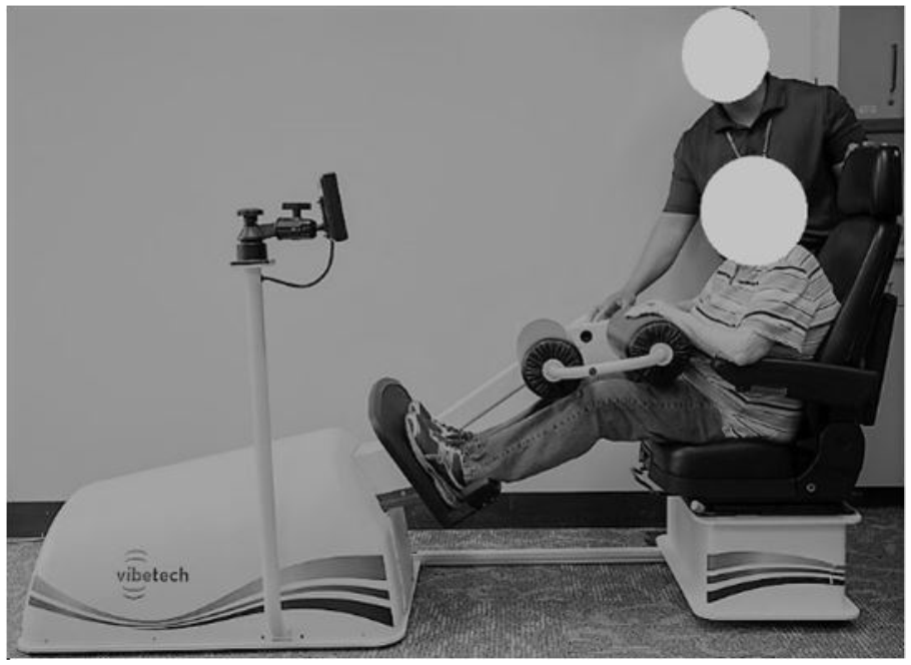
Participant receiving control treatment on the VibeTech® One device.
The footplate supplies low-amplitude vibrations at 30 Hz, a frequency associated with musculoskeletal benefits (Rittweger, 2010). The vibration supplied through the footplate is considered safe according to ISO2631 (ISO2631-1:1997). Vibration amplitude can be increased as tolerated over an adjustable range from 0.05 to 0.5 mm. The higher the vibration amplitude, the higher the alternating force supplied. While it is not known how much vibration reaches muscle, tendon, bone, and other tissue, it is hypothesized that larger amplitude vibrations result in greater force being absorbed by the muscles (Cardinale & Wakeling, 2005).
Training Protocol
Participants were blinded to the initial group assignment. Each participant was told they would receive two different types of exercises for 8 weeks: one followed by the other. To ensure correct exercise execution, all training sessions were supervised by a research assistant. In the control group, participants were seated in the vibration device and experienced leg loading via the device for 10 min 3 times a week, with no vibration administered. Conversely, the vibration treatment group participants trained with leg loading and vibration for 10 min 3 times a week. The training interval length was chosen based on positive results of other vibration studies (Buehring et al., 2011; Cardinale & Rittweger, 2006). The vibration frequency setting for all participants was 30 Hz.
The load applied on the legs was set by putting a regular weight scale on the footplate of the vibration device and having the participant push as hard as they could on the scale. One hundred percent of the pounds measured or a maximum of 100 lbs was used as the load for the training session. Participants completed this procedure to determine applied load before every training session, that is, the applied load was individualized based on the participant’s ability on the particular day. If the chosen load was not tolerable as indicated by the participant, the load was reduced back to that of a prior training session. The device has four levels of vibration intensity. The vibration intensity was regularly assessed every 2 weeks and adjusted. The vibration intensity was initially set to 0.2 g (Level 1) and was increased by 0.2 g every 2 weeks, as tolerated by the participant, with a maximum of 0.8 g (Level 4) (0.4 g = Level 2; 0.6 g = Level 3). If the increase in vibration intensity caused any discomfort, that increase was reduced back to the same vibration intensity as in the prior 2 weeks.
Tolerability and Safety
Participants were assessed for discomfort verbally and through a questionnaire during every training session. If a participant undergoing the vibration treatment could temporarily not complete the leg press motion, they were allowed to hold their legs in a fixed position while the load and vibration were maintained until they were able to perform the leg press again. During training sessions, participants were able to stop exercising whenever they chose to. They were encouraged to continue their training session after a short break to finish 10 min of exercise, but if they declined, the session was ended. The participants were asked why they stopped and these comments were recorded. If the research assistant felt that a participant became too exhausted to continue training, the training was stopped and the length of the session recorded.
Measures
Demographic characteristics, that is, age, sex, body mass index (BMI), history of falls in the last 12 months, and history of adult fractures, were obtained from an interviewer-administered questionnaire at baseline.
Retention and adherence
Retention rate was calculated as the percentage of participants who completed the study. To evaluate adherence, attendance to the vibration and control training sessions was recorded. Adherence rate for the vibration treatment and control groups was assessed separately by calculating the total number of completed training sessions divided by the total number of possible sessions.
Adverse events
All participants were questioned regarding adverse events (AEs) at all training sessions and testing visits. Participants were asked to report any AEs regardless of the cause. Serious adverse events (SAEs) were defined as an AE if it was life-threatening, resulted in hospitalization, or led to a substantial disruption of normal life functions. All AEs and SAEs were reviewed by members of the IRB that included physicians and nurses with relevant expertise. In addition, reviews were completed by the study team which included two physicians and two nurses with geriatric expertise.
Evaluation of pain
Self-reported pain before and after each training session was measured by a numerical pain scale, where 0 is “no pain” and 10 “pain as bad as it could be.”
Training intensity and load
Progression of training intensity and load was measured during the vibration treatment sessions only. The level of vibration intensity was recorded after each vibration treatment session. The increase in the level of intensity every 2 weeks was also recorded. The training load (lbs) was recorded at each vibration treatment session. The change in the load from baseline to the last training session was used to calculate the percentage change for each participant.
Training effect on health
Data on the participants’ perception about whether the training altered their health was collected after each 8-week training period by responding to the following statement: “I feel that this treatment improved my health.” The perception was rated on a 5-point Likert-type scale with response categories: strongly agree, agree, neutral, disagree, and strongly disagree.
Exercise enjoyment
Data on the participants’ perception of exercise enjoyment were collected after each training session by responding to the following statement: “I enjoyed my training.” The perception was rated on a 5-point Likert-type scale with response categories: strongly agree, agree, neutral, disagree, and strongly disagree.
Statistical Analysis
SPSS® version 24 (IBM Corp, Armonk, NY) was used for analysis. Descriptive statistics were calculated for all variables. Participants who dropped out (N = 7) were excluded from the analyses. Using independent sample t-test and a level of significance of .05, there were no differences in results between men and women and they were, therefore, analyzed as one group.
Average pain during vibration and sham treatments (24 visits each) for each participant was calculated. The Wilcoxon signed rank test was used to examine the perception of training effect on health between the vibration and control exercise at p level of .05. Self-reported training enjoyment was calculated as the mean for each participant.
Results
Participant Characteristics
Baseline characteristics are presented in Table 1. Thirty-one (49%) of the 63 sequential RCAC residents who were invited during recruitment were excluded for two main reasons: not meeting inclusion criteria (n = 4) and declined participation after learning more about the study (n = 27) due to busy schedule, not interested, having deteriorating health status with frequent doctors’ appointments, and providing care for an ill spouse.
Baseline Characteristics.

Note. BMI = body mass index; Fall = falls in the past year; Fracture = fractures after age 50; SPPB = short physical performance battery (Guralnik et al., 1994).
Retention and Adherence Rates
Of 32 enrolled residents, seven dropped out, resulting in an overall retention rate of 78%. Reasons for not finishing the study are described in Table 2. The overall mean adherence rate was 79.7% during the 24 vibration treatment sessions and 78.6% during the 24 control treatment sessions. All participants were able to perform the training at all sessions (vibration and control) they attended and complete the specified exercise duration. Sessions were missed due to conflicting health care appointments and illness. Increased pain or other conditions such as muscle soreness or knee pain related to the training occurred, but did not lead to training discontinuation with the exception of one participant drop out related to worsening knee pain.
Description of Participant Drop-Outs.

AEs
Of the 25 study completers, 20 reported at least one AE and four participants reported at least one SAE during the study. In study completers, there were 38 AEs and seven SAEs (Table 3). Mild muscle soreness and pain in the lower extremity (particularly knee pain) were the only AEs that deemed to be related to the vibration treatment. All SAEs were not study related.
Adverse Events Among Study Completers (n = 25).

Other includes during vibration exercise, three upper respiratory infection, one upper respiratory infection, one cellulitis, two stomach pain, two abdominal pain, and one headache. During sham exercise, one eye infection, one lower respiratory infection, one upper respiratory infection, one toe pain, one developing squamous cell carcinoma, and one worsening of Parkinson’s symptoms.
Pain Before and After Each Training Session
During the vibration treatment, pre-training pain for 21 (84%) participants ranged from 0 to 3 while four (16%) had pre-training pain of 4 to 6. Post-training pain for 22 (88%) ranged from 0 to 3 while three (12%) had post-training pain of 4 to 6 (Figure 3a). During the control treatment, pre-training and post-training were similar; pain for 24 (96%) participants ranged from 0 to 3 while one (4%) had a pain level of 6 (Figure 3b).
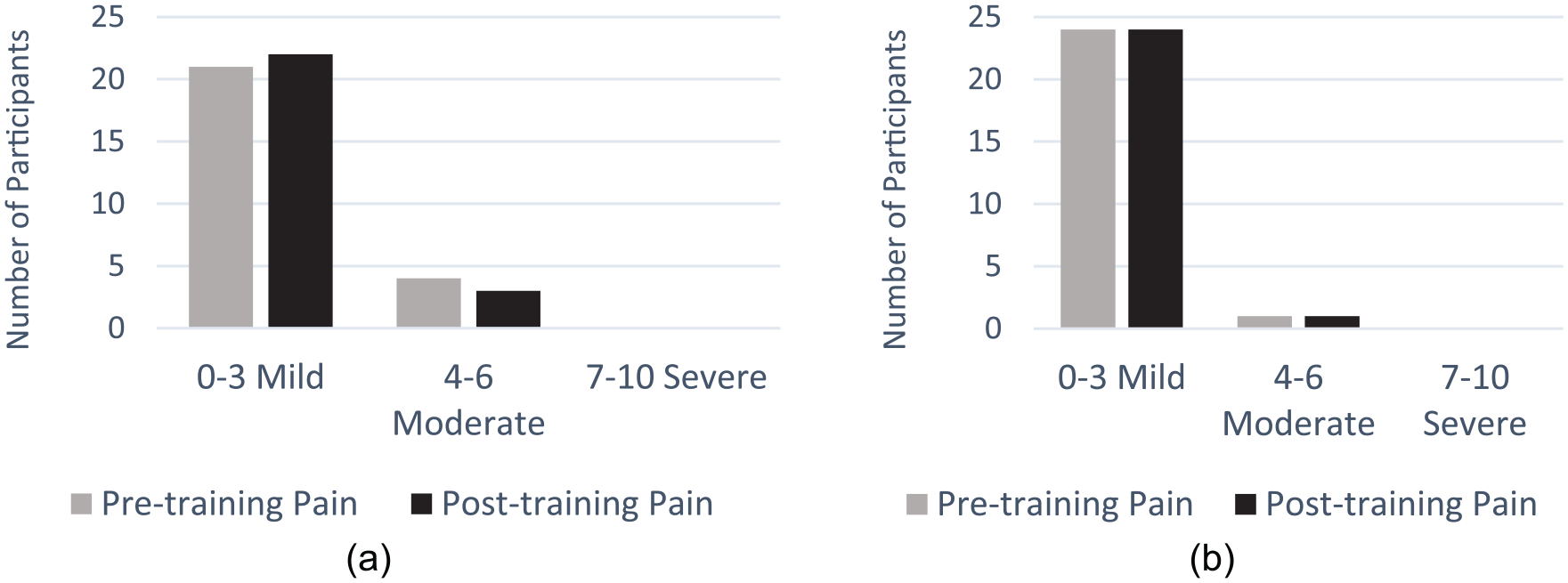
Pre- and post-training pain during the intervention and control training (N = 25): (a) vibration and (b) control.
Progression of Training Intensity and Load
All study completers (n = 25) were able to increase their vibration intensity to the maximum level. Specifically, each participant trained on Level 1 in Weeks 1 and 2, on Level 2 in Weeks 3 and 4, on Level 3 in Weeks 5 and 6, and on Level 4 in Weeks 7 and 8. The load at the baseline ranged from 10 to 80 lbs and ranged from 30 to 100 lbs at the last training session. The change in load ranged from 0 to 80 lbs with a median of 18.3 lbs, and average percent increase was 28.6%.
Perception of Training Effect on Health
Following vibration treatment, nine (36%) participants indicated the training subjectively improved their health, 10 (40%) responded neutral, and six (24%) did not feel vibration training made their health better. At the conclusion of the control sessions, four (16%) participants indicated that the training improved their health, 12 (48%) responded neutral, and eight (32%) did not feel the training made their health better. There was no significant difference in the perception of training effect on health between the vibration and control exercise (p = .400).
Exercise Enjoyment
Thirteen (52%) participants reported that the exercise was enjoyable during the vibration intervention and nine (33%) reported it was enjoyable during the control sessions. None of the participants in either group felt the exercise was not enjoyable (Figure 4).

Exercise enjoyment during the vibration and control sessions. None of the participants responded “disagree” or “strongly disagree.”
Discussion
This is the first study to investigate the feasibility and safety of semi-recumbent vibration exercise in RCAC residents with reduced physical function. We found that this exercise was feasible, well tolerated, and safe in terms of adherence, AEs, progression of training intensity, and load. There were a few dropouts, often for health reasons, an indicator of how frail these participants were and how many comorbidities they had. Only one participant discontinued the study due to knee pain, a possible training-related AE. Other reasons for discontinuing the study were personal reasons that commonly included time commitment. This highlights the need for a training that is short and yet effective for frail older adults with functional limitations. The three 10-min training sessions per week are shorter than many other exercise protocols for older adults and were felt acceptable by most participants in this study, which is reflected by the adherence rate of almost 80%.
The dropout and adherence rates of this study were similar to that reported in other studies of WBV exercise among community-dwelling and institutionalized older adults (Lam et al., 2018; Ma, Liu, Sun, Zhu, & Wu, 2016; Smith et al., 2016). These rates are not unexpected, but must be considered when studies are conducted among frail older adults. It also reflects the multiple morbidities and pre-existing physical disability, which was more pronounced in this study cohort than others (Ko et al., 2017; Lam et al., 2018; Ma et al., 2016; Sitjà-Rabert et al., 2012; Smith et al., 2016; Yang, King, Dillon, & Su, 2015). However, we observed good adherence unless the participants developed an acute illness. It is to be expected that any exercise intervention among such frail individuals will be confounded by the multiple morbidities and illnesses of study participants.
A key component of our intervention was the one-to-one supervision and support and conducting the program in the same facility where the participants live. We were very flexible in training session scheduling based on participant availability. The research team collaborated with facility social workers, physical therapists, and registered nurses to recruit the greatest possible number of participants and to facilitate successful study completion. These considerations are relevant for planning future studies examining exercise intervention in this population as larger numbers of volunteers will need to be included to allow for substantial study dropout.
Our results demonstrate that the training was generally safe. Although several SAEs occurred during the study, none were deemed related to the exercise. Knee pain occurred in a few participants but, with one exception, was brief and not severe enough to skip a training session or drop out of the study. Interestingly, there were no increases in pain level post-training compared with pre-training. Furthermore, the vibration intensity could be increased according to protocol with no injuries or additional pain sustained as a result of the vibration exercise. Nonetheless, as knee osteoarthritis is common in older adults, participants with pre-existing knee pain/problems should be assessed in future studies to determine if there is a cohort more likely to develop knee pain with vibration exercise. Other studies are examining whether vibration exercise affects knee function and pain in individuals with knee pain (Lai, Wang, Lee, Hou, & Wang, 2017; Yoon, Kanamori, Fujii, Isoda, & Okura, 2018).
Encouraging older adults to engage in exercise over time can be challenging. Boredom and lack of motivation are causes of exercise cessation (Janssen & Stube, 2014). Many of our participants reported that the semi-recumbent vibration exercise was an enjoyable experience and expressed the wish to continue to exercise. Several but not all of the participants expressed that they felt improvements in their health and that they would like to continue to engage in this type of exercise. None of the participants disliked the training. The future analysis of examined physical/muscle function tests and muscle mass assessment used will assess whether this vibration exercise not only led to the observed exercise enjoyment and perception of health benefit but also a potential improvement in muscle parameters.
This study has several limitations. The small sample size and the number of drop-outs limit generalizability of these findings. Nonetheless, this semi-recumbent vibration exercise is considered feasible within the study population. We have focused mainly on the safety and feasibility of semi-recumbent vibration exercise. It may be possible that other aspects that have not been investigated in this study have influenced the retention rate and adherence to the exercise program such as personal circumstance, specific illnesses, interaction with a trainer, or scheduled sessions. All training sessions were conducted by a trainer; this interaction may have contributed to the reported exercise enjoyment. Another limitation is that possible placebo effect resulting from the participants’ knowledge they were participating in a study may have increased motivation to exercise, thereby positively influencing measures of adherence and compliance. However, the placebo effect was minimized by the participants’ lack of knowledge about their group assignment.
In conclusion, this study demonstrates that semi-recumbent vibration exercise is safe, feasible, and well-tolerated in a cohort of RCAC residents with impaired physical function. The findings that this training was enjoyable and subjectively improved health perception are promising. Future exercise studies in such individuals may need to expect lower retention and adherence rates than among community elders largely due to concomitant illnesses and exercise time requirements. However, the shorter time requirements of vibration exercise could prove to be helpful in this regard.
Footnotes
Acknowledgements
M.H.T. was a substantial contributor to data acquisition, analysis, and interpretation, and drafting the manuscript, was the primary author, and takes responsibility for the integrity of the data analysis. E.S., J.L., and D.K. helped with data acquisition, analysis, and interpretation of the data. N.B., C.R.K., and B.B. were substantial contributors to the conception and design of the work and data analysis and interpretation. All authors contributed to revising the work and approved the final submission of this manuscript. The authors gratefully acknowledge funding from the Extendicare Foundation for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the Extendicare Foundation.
IRB protocol/human subjects approval numbers
Health Sciences Institutional Review Board
University of Wisconsin–Madison
Study ID number: 2015-0480