
Abstract
Introduction
The number of frail people is increasing and there is an unmet need to improve hospital care for this high-risk group of patients (Covinsky et al., 2003). Frailty is considered to be an important risk factor for mortality in hospitalized patients (Romero-Ortuno, Wallis, Biram, & Keevil, 2016). Within hospitals, frailty-screening tools are used to identify patients who may benefit from additional physical or mental care (Schuurmans, Steverink, Lindenberg, Frieswijk, & Slaets, 2004).
Physical aspects of frailty play a major role in the theory behind measuring instruments for frailty. In the biomedical context, frailty is often understood as a physical condition in which the increased risk of illness, dependence, and loss take the upper hand (Markle-Reid & Browne, 2003). This interpretation has its limitations: first, when frailty is only identified as a physical problem, the social context of the patient itself might be neglected. Second, the biomedical concept of frailty provides little direction for what is necessary for good care. Third, as there is still little consensus about which aspects are related to frailty, people with increased frailty are difficult to recognize in this extremely heterogeneous elderly population (Deeg & Puts, 2008).
In the St. Antonius Hospital Nieuwegein, patients are preoperatively screened for frailty with a screening tool called Anesthesia Geriatric Evaluation (AGE). Different questionnaires and functional tests are part of AGE. These questions and tests are largely based on the physical interpretation of frailty. Nevertheless, an attempt is made to assess the whole context of the physical, mental, and social aspects of the patients by asking screening questions regarding cognition, health-related quality of life, and social support systems (St. Antonius Hospital Nieuwegein, 2017). There is still too little knowledge about whether frailty screening leads to better care for the patient. Research on this could improve the care within the St. Antonius Hospital Nieuwegein. A care–ethical perspective might help unveil the limitations of the biomedical interpretation of frailty. Further research into the concept of frailty may play a role in how health care professionals can increase their understanding of frailty in everyday care situations.
Theoretical Framework
The parameters included in AGE are based on three domains: physical, mental, and social (St. Antonius Hospital, Nieuwegein, 2017). Gilardi et al. (2018) argue that a broad consideration of all domains (physical, psychological/mental, and social) is important to investigate the health situation in vulnerable adults. The physical domain of AGE consists of screening for anemia, renal dysfunction, and comorbidities, and an attempt is made to visualize the functional capacity with the “Geriatric 8” including nutrition, weight loss, body mass index (BMI), medication intake, neuropsychological factors, and age (Bellera et al., 2012). The functional capacities are tested by a grip strength test (measurement for muscle decline) and a timed “get up and go” (measurement for mobility) to look at whether optimization of the physical condition is possible or needed before the operation (St. Antonius Hospital, Nieuwegein, 2017). In the mental domain, cognition, delirium risk, depression, motivation, health-related quality of life, understanding, and decision making are included in the analysis. An assessment of cognitive functioning is made with a 6-Item Cognitive Impairment Test (6-CIT; Upadhyaya, Rajagopal, & Gale, 2010). The social domain includes examining the support system of each patient. Duppen et al. (2019) emphasize the importance of the social environment in identifying, preventing, or reducing frailty. Besides using standardized testing, Levana and Deiner (2014) argue that clinical insight is still the best tool for assessing frailty and the needs of an individual.
Several studies claim that a preoperative frailty assessment should play a central role in shared decision making (Huisman, Kok, de Bock, & et al, 2016). According to Saxton and Velanovich (2011), in addition to predicting complications, insight into frailty in surgical patients helps in making choices. The researchers argue that understanding the general condition of the patient is therefore just as important as assessing the physiological factors or organ-specific effects. According to Beyene, Severinsson, Hansen, Hansen, and Rørtveit (2017), a patient-participation process is important in the recovery process after surgery. “Confirming that patients are important in their own recovery process should give them an impression of being autonomous and equivalent, which is essential in the balance between power and responsibility” (Solbjør, Rise, Westerlund, & Steinsbekk, 2011). Sutton, Eborall, and Martin (2015) also indicate that if health care professionals recognize the involvement of patients, they will more often include patients in decisions about treatment. Research by Chow, Rosenthal, Merkow, Ko, and Esnaola (2012) indicates that because the physician is ultimately responsible for the surgical patient, the surgeon must ensure that the patient is fully informed and preoperatively evaluated. This (is said to) allow the patient to make choices and to receive proper care. However, in practice, a patient-participation process seems complicated because it depends on relations and context as well as for professionals to share their power with their patients (Thompson, 2007).
Method
The research method chosen for this research is a form of grounded theory study called QUAGOL: Qualitative Analysis Guide of Leuven (Dierckx de Casterlé, Gastmans, Bryon, & Denier, 2011). In a grounded theory study, an attempt is made to dig deeper into an understanding, action, or process than just the description (Creswell & Poth, 2016). Development of the theory could help in the clinical setting, explain hospital care or provide a framework for further research. The empiric results of this study are divided into themes based on three different questions: How do health care professionals recognize frailty? What are the experiences of health care professionals with AGE? and What are the experiences of patients with AGE?
Case Definition and Research Unit
The research unit consists of patients who participate in AGE and of health care professionals who are involved in AGE or participate in the multidisciplinary consultation at the St. Antonius Hospital, Nieuwegein. The study included eight patients who were screened and eight health care professionals working at the St. Antonius Hospital, Nieuwegein. All patients were preoperatively screened, awaiting surgery for several reasons. The average age of the patients was 70 years, equally divided man and woman. The data collection took place through observations of the screening, observations of several multidisciplinary consultations between health care professionals, and conducting interviews with patients and health care professionals. The multidisciplinary team within the AGE consists of anaesthesiologists, surgeons, physiotherapists, dieticians, pharmacologists, nurses, and geriatricians. The purpose of this team is to discuss the patients included in the screening and together decide on which care or measures are needed.
Data Analysis
Using QUAGOL, analysis and data collection take place simultaneously (Dierckx de Casterlé et al., 2011). The analysis process consists of 10 steps, but methodologically, it is a constant movement between the different phases. QUAGOL is an ordered method but gives the researcher enough room for intuition and creativity (Dierckx de Casterlé et al., 2011). The aim of QUAGOL is to reconstruct the story of the participants on a theoretical level and analyze the concepts found. It is a repetitive process of analysis in dialogue with the data, allowing the researcher to dig deeper and deeper into the concept to be studied (Dierckx de Casterlé et al., 2011). In this research, the analyzing process was carried out by the first two authors. Consensus about the concepts found was achieved by discussing the data multiple times, repeatedly checking the understanding of data and concepts from both authors, which contributed to the depth of the concepts eventually found. The last two authors contributed to the validation of the analysis by reviewing the final concepts found. Within these discussions, the quality, usability, and importance of the data were checked.
Ethical Considerations
Interviews were held with participants during the data collection. Participants gave permission in the form of written consent to use their experiences and interview data for our research purposes. To guarantee the anonymity of the participants, identifying data (i.e., date of birth and address) were omitted. Obtained data will not be shared with third parties during or after the investigation. The review board of the local ethical committee (Medical research Ethics commitee United, number Z19.029) waived the need for informed consent as patients were not subjected to investigational actions. The study was conducted in accordance with the principles of the Declaration of Helsinki (World Medical Association, 2013).
Results
Recognizing frailty
Competence
Health care professionals argue that looking at patients consciously and paying more attention to frailty provides more knowledge and experience about the “vulnerable patient,” making it easier to recognize them. Health care professionals indicate that it is important to gather more competence around frailty to perform the right patient selection. This includes not only sticking to the screening tool but also using their own clinical experience to select patients (Figure 1). “Someone can also be vulnerable in a different way, which is not covered in the questionnaire, but when I feel something is not quite right” (Interview VPD).
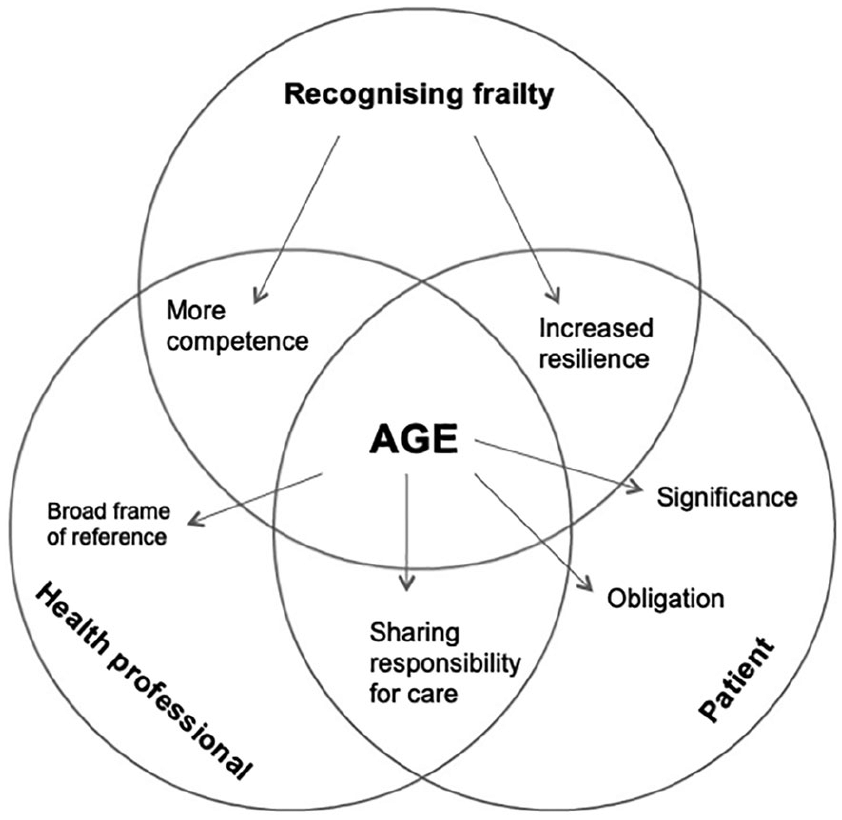
Results displayed in themes.
In addition, the health care professionals indicate that through the multidisciplinary consultation, several health care professionals are involved in the care for the “vulnerable patient,” which means more attention is paid to the patient. The screening seems to provide an extra check on which care is needed after surgery. Due to the involvement of several health care professionals within the multidisciplinary consultation, both the screening and the multidisciplinary consultation are action oriented. People closely work together, so agreements are reached quickly between health care professionals. It does not take long before action takes place. “We reach specific agreements to optimize someone” (Interview VPB). “Not just discussing because we have to discuss, but act upon it” (Interview VPC). The multidisciplinary consultation seems to contribute to a learning process of the health care professional. The health care professionals indicate that because of AGE, more knowledge about frailty is created as well as insight into which interventions are possible and what different choices have to be made. “We try to collect more and more data about what the best options are” (Interview VPD). ‘The MDTM in itself also taught us to implement interventions much earlier” (Interview VPD).
Resilience
Motivation is indicated by the health care professionals as one of the most important aspects of whether someone is vulnerable or not. Motivation for the operation and the will to live increases resilience, the ability to recover from adversity. Health care professionals also base their assessment of how vulnerable someone is on the question of what someone prefers. If his or her self-determination is low, then someone is considered to be extra vulnerable. “What do patients prefer, that is a question we have to ask everyone” (Interview VPB).
According to the care professionals, the screening is an initiation of the patient’s awareness process. By thinking about risks, options, and how vital one is, one starts to think about the preoperative period, the operation, but also about the postoperative period and what is needed during these different periods. Increased awareness can lead to better preparation for complications and the postoperative period. “People become more aware that it is a major intervention” (Interview VPA). Explaining the consequences of not going into surgery in optimized physical condition and emphasizing that people will feel better when they improve their physical fitness seems to raise awareness. “We have to involve them, it has many consequences for them” (Interview VPR) “Appearing well-prepared and focused at the start is very important” (Interview A). Respondents also indicate that the tests and questions can be confronting for patients, which is a good thing according to the health care professional, as this triggers an awareness process. Being more aware of their condition causes the motivation to get better. “People are confronted with failing a test, which makes them aware they have to act upon it” (Interview G).
Experiences of Health Care Professionals
Frame of reference
What many health care professionals indicate as praiseworthy of the multidisciplinary consultation within AGE is that the patient is looked at from a broader perspective. According to the respondents, this is commendable because the parameters surrounding frailty are examined in a joint context. In addition, the health care professionals indicate that the multidisciplinary character of the consultation contributes because everyone looks at the patient from their own point of view. “Everyone has their own area of expertise. By taking into account everyone’s knowledge we can give the right advice to the patient” (Interview VPD). The screening seems to be aimed at prehabilitation: how can someone be improved before going into surgery. “As a result we can apply a more focused intervention” (Interview VPB). The goal is to reduce the chance of complications and increase the chance of a faster or better recovery. Some health care professionals indicate that implementing the whole context of the patient in the screening is therefore of critical importance. “The great thing about this screening instrument is that we really see per person and per situation whether someone is vulnerable yes or no” (Interview VPD).
Sharing responsibility
As an advantage, the health care professionals indicate that AGE ensures that there is a joint responsibility for the patient, and health care professionals can share their concerns about a patient within the AGE-team. “There’s a joint responsibility and therefore everyone has to put an effort into it” (Interview VPC). The multidisciplinary consultation therefore contributes to collaboration between health care professionals. The respondents claim that AGE also ensures there is a shared decision making between the health care professional and the patient with his or her family by discussing the treatment, how someone feels, what the risk factors are and what options are available. “All aspects are highlighted, personal opinion is also taken into account in the clinical setting and in the decision-making process” (Interview VPA).
Experiences of Patients
Obligation
Patients indicate that they see the screening as something the doctor wants. They do not see it as being in their own interest, but they participate because the doctor wants them to do so. “If this gives the green light for the surgeons to operate me” (Interview PTA). “If they want to check and test it, I’ll do that” (Interview PTC). Some respondents feel the screening is something that needs to be done and they feel obliged to meet the expectations of the health care professional. In addition, it seems that patients sometimes feel they have to pretend to be better than they are because they want to have surgery. “Yes, if it is necessary, then it has to be done. I’ve no problems with it” (Interview PTC). “People who know that they are vulnerable, but really want surgery, sometimes have the feeling that they have to stand up for themselves or sell themselves to qualify for an operation” (Interview VPD).
People indicate that they often do not see themselves as vulnerable or weak. They also think they do not have a higher risk of complications and reveal that they do not understand some of the questions that needed to be answered because they felt that they were not applicable to their situation. “‘In my case, I didn’t really need it’ (Interview PTE). Those questions, like ‘can you still get dressed by yourself’ and ‘can you handle your medication intake’, made me think, what on earth are they talking about?” Many people at the screening do not feel vulnerable, nor do they seem to know what this means. They indicate they are certainly feeling well enough to have surgery. “I actually never thought about being vulnerable, I didn’t think I would be” (Interview PTA). “I did not expect that aspects investigated in the screening wouldn’t be good” (Interview PTC).
Significance
Despite the fact that some participants indicate they find the screening unnecessary, other respondents did not experience the conversation as extra stressful. The patients indicate they are in a preparation process for the operation and therefore do not mind having a discussion about motivation, vitality, and treatment. “It’s fine. I’m in a period of preparation, so it feels like the right moment” (Interview PTA). Some patients indicated the screening was their moment to find out a decision was made together with the health care professional. Respondents said that they felt their opinion was heard, and they were taken seriously as a patient. “I was relieved when the doctor told me there was a choice in whether or not to undergo surgery” (Interview PTG). “I felt they also listened to me” (Interview PTB). Patients also indicate they like having an extra check on how they are doing. Due to the screening, it seems as if patients are going into surgery with more certainty. “They know, okay, extra attention is being paid to me, how I will get through this operation” (Interview VPC). “Well the things that are going to happen to me became clearer” (Interview PTB).
Discussion
Competence
Health care professionals in this study indicate that in the process of registering and recognizing frailty, they use not only a screening tool but also their own professional experience. The screening seems to contribute to the creation of more knowledge since more and more nurses, doctors, and other health care professionals are aware of frailty, and it is increasingly integrated into the health care system. In this way, more experience is being accumulated in what is the best care for the vulnerable patient in the clinical setting. According to health ethic Ruddick (1995), moving in a practice or in a care situation, such as AGE, is to accept a connection with someone to eventually achieve a goal. In AGE, this goal ensures that someone will undergo surgery safely by mapping the risks, using an optimization process or making an informed decision within the treatment plan. Ruddick (1995) states that a practice is a social event, in which men can only know what is good if they fully engage in a practice and are aware of all aspects of this practice. Since a universal definition of frailty is still lacking, more competence for health care professionals in recognizing frailty is needed for them to fully engage in the caring practice.
Sharing Responsibility
According to health care professionals, better care is given to the patient when not only more health professionals but also patients are involved within the care process. Each context requires different forms of care. Tronto (1993) states that people have to look at every situation in context because it helps them to understand the different parties involved and the relationships between them. According to health care ethicists, the care recipient knows what is relevant within a situation. AGE tries to involve the patient within the care process. Our findings show that AGE seems to be helping the patient to go into the operation with more motivation and more confidence. According to health care professionals, this is an awareness process triggered by involving the patients themselves and calling upon their own responsibilities. Anderson et al. (2003) state that for optimization, the patients need to be motivated to enter a surgery in a safer way. AGE tries to involve patients, so they take on a more assertive attitude.
Doctor–Patient Relation
A better awareness of the care relationship between patients and doctors in the St. Antonius Hospital, Nieuwegein would give more room for what is relevant for the patient. Health care professionals assume that AGE contributes to a process of shared decision making. They argue that for shared decision making, they have to be able to properly substantiate their considerations to the patient. Even more so, they must ensure that the patient is well informed to give a proportionate chance to the patient so that he or she can make a choice. Nevertheless, this still seems to be difficult in the clinical setting. Many patients indicate that they think the screening is fine “because the doctor wants it” and they often adopt a passive attitude. Godolphin (2009) states that a more active attitude of the patient is often avoided because patients are afraid of a deterioration of the physician–patient relationship. According to Van Nistelrooij, Visse, Spekking, and de Lange (2017) shared decision making is an important process in the doctor–patient relationship but emphasize that within this relationship, there should be room for the human dependence of patients and for outside support. Barry and Edgman-Levitan (2012) argue there should be more room for a less paternalistic attitude from the health care professional. In addition, the data show that sometimes, there seems to be too little scope for a good process of shared decision making because there simply seems no time for it or due to the complexity of the decision.
Multidisciplinary Medical Perspective
Respondents indicate that the multidisciplinary consultation contributes to the screening because everyone looks at the patient with their own expertise. The whole picture of the patient is visualized, and the various health care professionals complement each other. Tronto (1993) endorses this by claiming that multiple perspectives have to be brought together to shape a health care practice. Everyone has a different notion about what good care is, so a broad perspective is essential to decide on the best care. The data show that every health care professional uses their own experience to recognize frailty. Even in this relatively small study, the importance of a multidisciplinary perspective is emphasized.
Within AGE, every perspective that participates in the multidisciplinary consultation tends to be a “medical perspective” on the patient, and because of that, the person may still be seen as a “medical object” instead of a vulnerable person. Health care professionals within this study indicate that they are trying to involve several professionals in AGE to share responsibility for the patient. Walker (2007) states that practices show what is valuable by assigning, accepting, or refusing responsibility. In practice emerges what is fundamentally important. This research shows that there is indeed more involvement of health care professionals in AGE. In spite of this, respondents also indicate that this is still reasonably dependent on how important people feel about it and how involved they feel to be present at the AGE multidisciplinary consultation. As a result, conscious care and attention to frailty could be integrated even further in health care.
Limitations and Strengths
The method description of QUAGOL emphasizes the importance of a group analysis. Despite several proper consultations between all authors, the analysis in this research was mainly performed by the first author and therefore might not be carried out optimally accor-ding to QUAGOL (Dierckx de Casterlé et al., 2011). Regardless of the small size of this study, a number of concepts that have been found are relevant and can be developed further. The entire process of AGE has been presented in this study. This is highly recommended for future research. Follow-up research into the perception of the patient during screening is valuable in how it can be improved. Mapping the complete screening provides added value for (follow-up) research because it reflects on the entire process and the situation of the patient. The QUAGOL method fitted in well and is recommended for future research. By studying patient stories, valuable first-person knowledge about how care is received and how it can be improved is obtained.
Conclusion
Frailty appears to be a concept that is difficult to define, and the results of this study show that there is yet too little knowledge about frailty in the clinical setting. According to the respondents, AGE creates more awareness among health care professionals about frailty and how care can be arranged around it. The intrinsic value of the patient, with his own identity and life story, is valuable in an optimization or treatment process. The data show that giving more responsibility to the patient and confronting the patient with his or her own ability cause a more assertive attitude. In AGE, an attempt is made to achieve a process of shared decision making by involving patients in their care process and making them aware of their abilities and motivation. Nevertheless, the data also show shared decision making is sometimes still asymmetrical and therefore difficult to accomplish. This study has drawn a picture of AGE which indicates interventions can always be used to ensure that patients enter the treatment process in a confident and optimized way. In spite of this, it also shows it is still a paternalistic process of a multidisciplinary team with a medical perspective.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The review board of the local ethical committee (Medical research Ethics committee United, number Z19.029) waived the need for informed consent, as patients were not subjected to investigational actions. The study was conducted in accordance with the principles of the Declaration of Helsinki (World Medical Association, 2013).