
Abstract
Growing research suggests regular physical activity as a strategy for reducing risk of Alzheimer’s disease (AD); however, there is little research available regarding public messages about the connection between physical activity and brain health. This study aimed to (a) examine the volume and content of regular physical activity and brain health messages being distributed by national organizations, and (b) explore how informal caregivers perceive and comprehend brain health messages. Methods included (a) a content analysis of 155 online documents related to physical activity and aging that were located on national physical activity organizations’ websites, and (b) a thematic analysis of transcripts and observer notes from two focus groups with 10 informal caregivers recruited at a support organization for AD caregivers in the southeastern United States. Content analysis results revealed limited information about the physical activity and brain health connection. Focus group results revealed that caregivers had limited exposure to information about the physical activity and brain health connection and were concerned about the credibility of this information. Further research is needed regarding brain health and physical activity messages and the potential benefits of collaboration among physical activity organizations, researchers, and health care professionals in delivering consistent and credible messages to the public.
Introduction
The American demographic is rapidly changing. In 2014, adults 65 years and older made up 14.5% of the U.S. population, a number expected to rise to more than 20% over the next three decades (Administration on Aging, Administration for Community Living, 2015). Related to this rise in the aging population, the impact of Alzheimer’s disease (AD) is growing. One in 10 Americans above age 65 have AD, accounting for more than 5.5 million people in 2018 (Alzheimer’s Association, 2018). In addition to being a major health issue and the sixth leading cause of death in the United States, the economic value of unpaid caregivers for persons living with AD is estimated to be over US$232 billion (Alzheimer’s Association, 2018). As baby boomers continue to age, it is projected that the incidence of AD and economic costs related to AD will increase exponentially by 2050 (Alzheimer’s Association, 2018).
As there is currently no cure for AD, most health promotion initiatives focus on increasing awareness and reducing risk of the disease. For example, growing research points toward regular physical activity as a strategy for reducing risk of AD. The latest 2018 National Physical Activity Guidelines indicated that physical activity may lower the risk of cognitive impairment and dementia (U.S. Department of Health and Human Services, 2018). According to the American College of Sports Medicine Position Stand on Exercise and Older Adults, “cardiovascular fitness and higher levels of physical activity reduce the risk of cognitive decline and dementia” (Chodzko-Zajko et al., 2009, p. 1521). A recent systematic review uncovered an inverse relationship between physical activity and risk of AD that leisure-time physical activity was particularly protective against AD (Stephan, Hongisto, Solomon, & Lonnroos, 2017). However, the review also indicated that the risk of bias and limited breadth of study design hinder scientists’ ability to connect detailed physical activity recommendations to reduced AD risk. Relatedly, the processes and mechanisms mediating the relationship between physical activity and reduced rate of cognitive decline are also unclear (Kennedy, Hardman, Macpherson, Scholey, & Pipingas, 2016). Therefore, despite growing evidence on the presence of a physical activity–brain health connection, current evidence gaps prevent national physical activity guidelines from including specific recommendations (e.g., type, duration, intensity) for exercise as a risk reduction mechanism for AD (Stephan et al., 2017). This lack of clarity in recommendations may contribute to the varied perceptions about the role of physical activity on brain health among older adults (Price et al., 2010; Wilcox et al., 2009).
Although there is a strong body of research examining the overall messages communicated about brain health and disease prevention strategies (Friedman et al., 2009; Friedman, Laditka, Laditka, & Price, 2011; Hunter et al., 2017; McGough, Kirk-Sanchez, & Liu-Ambrose, 2017), there is far less information available describing messages about physical activity and brain health specifically. Rose, Friedman, Marquez, and Fernandez (2013) examined the content of both English and Spanish versions of AARP The Magazine, a magazine publication for adults above age 50, and found that there were very few articles describing an association between physical activity and brain health. Media coverage about AD has not been commensurate with the scientific evidence on AD risk reduction behaviors (Friedman et al., 2011). In addition, previous research indicated that most adults lacked detailed information about AD disease and did not perceive themselves as very knowledgeable (Anderson, Day, Beard, Reed, & Wu, 2009). Results from a large, multistate qualitative study indicated that ethnically diverse older adults did not recall reading or hearing about brain health in the media (Friedman et al., 2009). Research suggests that practitioners need to develop relevant and understandable messages geared to specific audiences and to disseminate these messages across multiple channels (Price et al., 2010). A survey published in 2013 by the Pew Research Center reported that 59% of adults look online for health information, including 54% of adults aged 50 to 64 and 30% of adults aged 65 and older (Fox & Duggan, 2013). Although many people use the Internet as a source of health information, no study has examined brain health–physical activity messages communicated online. This study served as the first comprehensive review of online content about the physical activity and brain health connection disseminated by organizations involved in physical activity promotion.
This study aimed to (a) examine the volume and content of regular physical activity and brain health messages being distributed by national organizations, and (b) explore how informal caregivers perceive and comprehend brain health messages that they receive.
Method
There were two components to this study: (a) a content analysis of 155 online documents related to physical activity and aging that were located on national physical activity organizations’ websites, and (b) a thematic analysis of transcripts and observer notes from two focus groups with 10 informal caregivers recruited at a support organization for AD caregivers in the southeastern United States.
Content Analysis
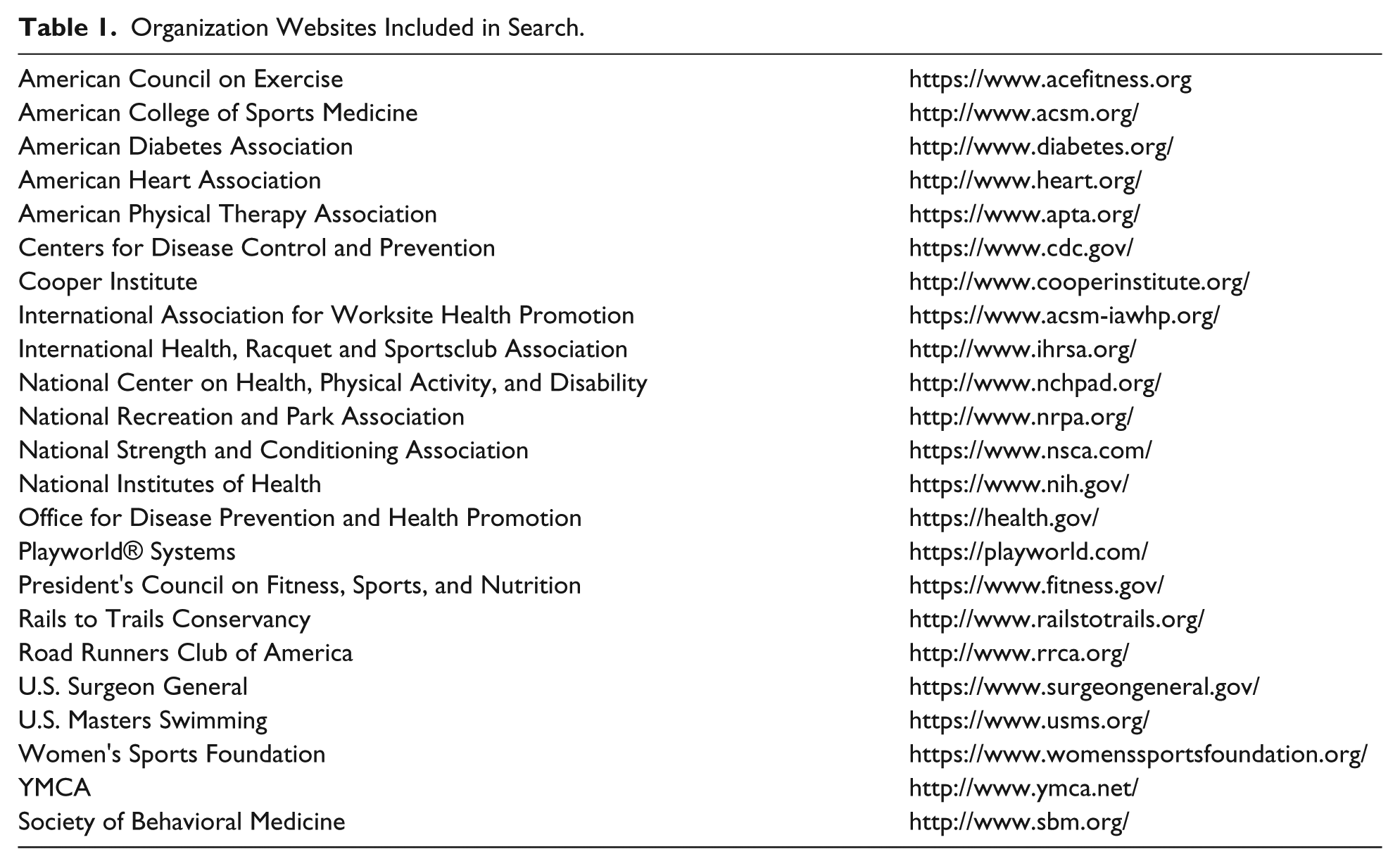
A sample of available materials was collected on February 1, 2017, by searching the web pages of national physical activity or fitness organizations. Organizations searched (presented in Table 1) included partners and affiliate organizations of the National Physical Activity Plan Alliance (NPAPA). The NPAPA is a nonprofit coalition of organizations working together to ensure that efforts to promote physical activity in the United States are guided by a comprehensive, evidence-based strategic plan (NPAPA, 2016). Participating organizations have a vested interest in the promotion of physical activity as a means of improving public health. Additional national sources, federal agencies, and collaborating organizations, representing key players in the physical activity and public health field, were added such as the Office of the Surgeon General and the National Institutes of Health. A total of 23 organizations were included in the web-based search.
Organization Websites Included in Search.
Sampling
Using the search functionality of each website, a search was conducted using the following terms: “aging,” “seniors,” and “older adults.” Searches on websites that did not focus on physical activity specifically included the following amended search terms: “physical activity and aging,” “physical activity and seniors,” and “physical activity and older adults.” Consumer research indicates that more than 95% of web traffic generated from Google searches originates in the first two pages of results (Chitika, 2013). Therefore, documents appearing on the first two pages of results generated by the website search function were included for an initial review. Online documents and web pages were excluded if they (a) were published before 2008 (the date of the latest Physical Activity Guidelines for Americans release); (b) took visitors to a link off the original website to another source or were located behind a firewall requiring registration; (c) only contained links to other pages with no substantive text content (e.g., images) or were a small portion of a discussion forum; (d) were a complete research article, continuing education or certification course offering, or an advertisement for a webinar or event; (e) were interactive or video content; or (f) focused on a disease not related to brain health or focused on children or nutrition. Up to five relevant results for each term, selected in the order they appeared in search results, were included. A total of 155 documents were included in the final sample.
Variable coding
Materials were evaluated using a comprehensive codebook that was developed based on previous content analysis research on organ donation messages and cognitive health messages (Friedman, Laditka, Laditka, & Mathews, 2010; Friedman et al., 2011; VanderKnyff, Friedman, & Tanner, 2015). The codebook focused on three main areas: (a) credible information, (b) physical activity messages and recommendations, and (c) brain health connection. Credible information examined the presence of expert quotations, formal citations, and nonformal citations (i.e., hyperlinks or mention of specific scientific research). Codes regarding physical activity messages and recommendations quantified the type of messages included (e.g., prolonging life, disease prevention, treatment, quality of life improvements). Brain health codes included identification of terms (AD, brain health, cognitive function, cognitive decline, dementia, staying sharp) and phrases (caregiving experience, improved quality of life, prevention, risk reduction) being used within the sample documents and description of an explicit connection between physical activity and brain health. Document length and publishing organization were also coded.
Interrater coder reliability was assessed on a 20% subsample of the web pages/document (n = 31) by two authors (K.O. and W.T.). Cohen’s kappa statistic (Cohen, 1960) ranged from .729 to 1.00, indicating “almost perfect” coder agreement (Landis & Koch, 1977). Discrepancies in coding were discussed, clarifying criteria were established, and documents were recoded as needed to reach “almost perfect” agreement. The first author coded the remaining documents.
Analysis
We used descriptive statistics (nonparametric frequencies and percentages) to assess coded variables. We also tested whether mention of a direct connection between brain health and physical activity differed by the use of specific terminology (e.g., dementia, AD, cognitive function) and by the type of publishing organization (e.g., university or research institute, physical activity organization, government entity, disease-specific organization, aging-specific organization) using chi-square tests or Fisher’s exact tests. The level of significance was set to p < .05. All the analysis was performed using SPSS 24 (IBM Statistics for Windows, Armonk, NY).
Focus Groups
Recruitment
Focus group recruitment took place at a support organization for informal caregivers of individuals with AD located in the southeastern United States. Working through employees of the organization, researchers used announcements at caregiver support groups, informational flyers, and individual in-person requests to recruit participants. A total of 10 individuals participated in the two focus groups. Participants were between 56 and 86 years of age, primarily White (80%), female (70%), and retired (90%). The group was highly educated that all participants were college graduates. Information about their care recipient’s diagnosis or disease status was not collected.
Data collection
Two focus groups were conducted at the same caregiver support organization where participants were recruited. Each focus group session was approximately 1 hr in length. A moderator guide was developed based on the research questions and reviewed by two outside caregiving experts prior to the session. Topics of discussion included caregivers’ health information–seeking behaviors, how information about physical activity and brain health affects their physical activity behaviors, and preferred sources of information. Each focus group session was recorded and transcribed verbatim. The university’s institutional review board approved this research protocol. Each focus group participant provided written informed consent prior to participation.
Analysis
A thematic analysis was applied to the qualitative data (transcripts and observer notes) to analyze and identify patterns in the data. The transcripts were first read to familiarize the researchers with the discussions. During the second reading, the primary author performed line-by-line open coding of the transcripts to identify frequently emergent codes (Strauss & Corbin, 1998). Two authors (K.O. and D.B.F.) discussed the initial codes for clarity and agreement. The primary author then identified common themes and representative quotations. All coding was completed by hand. The identified themes and quotations were then reviewed and confirmed by a third member of the research team (W.T.) for additional consensus. Repeated verification throughout the qualitative analysis process ensured rigor and validity of findings (Morse, Barrett, Mayan, Olson, & Spiers, 2008).
Results
Content Analysis
More than half of the documents were published by physical activity organizations (38.7%) or government entities (20.0%). Other publishing organizations included medical organizations (11.0%), disease-specific organizations (e.g., American Diabetes Association; 8.4%), and universities and research institutions (7.1%). More than half of the documents were less than 1,000 words, with 28.4% between 250 and 500 words and 37.4% between 500 and 1,000 words.
Credible information
About 41% of the total sample included quotes or accounts from experts, 31.6% included formal citations to scientific research, and about half (51.6%) included nonformal citations (such as hyperlinks or mentions of scientific research).
Physical activity messages and recommendations
Messages connecting physical activity and improved quality of life were present the most, in 58.1% of the total sample. Another popular message, found in 47.1% of the sample, described physical activity as a means of disease prevention. Other messages included physical activity–related research or clinical trials (23.2%), as a treatment for disease (21.9%), and as a means of prolonging life (18.7%). More than half of the materials (51.6%) included nonformal citations, 31.6% included formal citations, and 40.6% included quotes or accounts from experts.
Brain health connection
The presence of brain health terminology was low (13.5%) and use varied. Terms such as cognitive function (7.1%), dementia (6.5%), AD (5.2%), cognitive decline (3.2%), brain health (2.6%), and staying sharp (2.6%) were present in the analyzed documents. Only 12.9% of all materials presented an explicit connection between physical activity and brain health. The way in which an explicit connection was described varied greatly, including, but not limited to, the following:
“cognitive improvements in terms of fitness”
“physical activity, such as swimming, regular walking, and even dancing, may substantially reduce the risk of Alzheimer’s disease in older individuals.”
“exercise can keep your brain sharp”
“. . . physical activity [has] shown benefit on cognition, mood, and quality of life in individuals with AD or MCI (mild cognitive impairment)”
“well-designed [resistance training] circuit . . . that would . . . also stimulate cognitive function or a psychological benefit”
Documents that included at least one brain health term were significantly more likely (66.7%) to make the explicit connection between physical activity and brain health, χ2(1, N = 155) = 62.48, p < .001. It is notable, however, that one third of the documents including at least one brain health term still did not explicitly connect physical activity and brain health.
Content explicitly linking physical activity and brain health varied significantly by publishing organization, χ2(5, N = 155) = 12.351, p = .030. Research institutions published the highest proportion of documents that made the explicit connection between physical activity and brain health (27.3% of content published by research institutions made the connection, N = 3), followed by physical activity organizations (21.7%, N = 13) and government sources (9.3%, N = 3).
Focus Groups
Qualitative analysis of the focus groups revealed two main themes: (a) limited exposure to information about physical activity and brain health, and (b) concerns regarding consistency and reliability of physical activity and brain health information.
Limited exposure to information
Focus group participants mentioned several primary and preferred health information sources, including in-person support organizations, the Internet, newspaper, television, physicians, magazines, books, and direct mail pamphlets. Many participants reported not hearing much from the media about the connection between physical activity and brain health. One participant described, “[not] hear[ing] a lot about the direct connection, I think the media certainly pushes exercise. You can pick up anything and hear about exercise, but I don’t see an emphasis on brain health.” Despite this perceived lack of exposure, participants expressed knowledge of the physical activity and brain health connection when prompted. Participants shared, “If you don’t do much of any physical activity, your brain starts to deteriorate . . . the more active you are the better you are mentally” and “Physical activity is pretty vital . . . if you are unable to engage in physical activity, or if you are unwilling to do anything other than being a couch potato . . . you’re setting your body up for all kinds of physical problems and the brain, most importantly, because I think the brain constantly needs to be challenged.”
Perceptions about consistency and reliability of messages
Participants expressed hearing or finding inconsistent messages about physical activity and brain health indicating that “. . . the information . . . is so varied. Some of it will say aerobics are better for your brain, others will say strength training is better for your brain.”
They shared skepticism about the validity and reliability of the brain health information they encountered. Participants expressed viewpoints such as “I don’t know how to determine if it’s reliable. That’s part of the problem; I don’t have that competence myself” and “So I’m very skeptical about a lot of the things I read, because it changes every 6 months, and so you have to be very careful about reading all this stuff . . . .”
Participants also communicated the importance of finding consensus among information sources sharing brain health information due to inconsistent messages. Representative quotes were as follows: “It’s also important to have a second opinion, third opinion” and “. . . look for consensus in whatever you’re trying to understand.”
There were repeated discussions of credentialed professionals (e.g., physician, therapist) and the role these individuals play in their information-seeking behaviors. Participants had high degrees of trust and comfort with the information they received from credentialed professionals. For example, “I look for professionals who are doing it, licensed in what they are doing. They know what they are doing. They have testimonials that this is working for some people.”
Comparable Findings
The emergent themes from the focus groups are mirrored in the content analysis results (Table 2). Both content analysis and focus group findings indicated limited availability of information about the connection between brain health and physical activity, along with variability and inconsistency in the information. Common caregivers’ perceptions supported the results of the content analysis regarding availability of information about the brain health and physical activity connection. Information sources and perceived credibility also occurred in the results.
Comparable Findings Across Focus Groups and Content Analysis.

Discussion
The current study examined the volume and content of physical activity and brain health messages distributed by national physical activity organizations and explored how informal caregivers perceive and comprehend brain health messages. Findings of the study demonstrated limited information about the connection between physical activity and brain health within online content published by national physical activity organizations. The presence of brain health terminology was low, and only 12.9% of sample explicitly presented the connection between brain health and physical activity. This aligns with previous research on physical activity and brain health messages from traditional and other online media sources (Friedman et al., 2010; Friedman et al., 2011; Rose et al., 2013). Findings of the study also demonstrated that research institutions were more likely than other organizations to present this connection, as were documents that included at least one brain health term. Future research is needed to develop messages related to physical activity and brain health connection and to engage communities, practitioners, and researchers in message dissemination.
Findings from the focus group suggest caregivers’ concerns about consistency and reliability of physical activity and brain health information, which is consistent with findings from previous qualitative work that revealed confusion related to the connection between physical activity and brain health, and caregivers’ uncertainty and skepticism regarding specific recommendations and validity of information being promoted in the media (Wilcox et al., 2009). As focus group participants struggled to determine information validity and reliability, credible information sourcing could be valuable. Caregivers in the focus groups craved for credible information from trusted experts in the field and indicated a preference for receiving health information from health care professionals, a sentiment echoed in existing research (Zulman, Kirch, Zheng, & An, 2011). More information is needed on public perceptions of brain health information being delivered by physical activity experts, both within and outside the traditional health care field.
Further research will be required to understand how to best craft messages surrounding physical activity and brain health for clarity and receptivity. The limited amount of clear information connecting brain health and physical activity might be indicative of the evolving research landscape surrounding the issue. As evidence of the connection, underlying mechanisms, and specific recommendations about the physical activity and brain health connection continue to develop, messages will change and evolve. Public health and other organizations that promote physical activity should continue to include evidence-based statements in materials and programming (Martin Ginis et al., 2017) and refrain from suggesting conclusions that have yet to reach consensus. The National Academies of Sciences, Engineering, and Medicine (2017) reported that existing modest, but inconclusive, evidence connecting physical activity and reduced risk of cognitive decline is insufficient to support public health campaigns encouraging behavior adoption. While evidence about the physical activity–brain health connection itself must grow, so must our understanding of the messaging and perceptions of the connection. It is important to better understand how messages connecting physical activity and brain health influence behavior before messages can be disseminated for the specific purpose of changing physical activity behaviors in aging and caregiver populations.
This study has limitations, including small size and homogeneous demography of focus groups, the limited terminology used for the content analysis search, and the limited scope of organizations included in the content analysis. Focus group findings emerging from this highly educated, predominantly female small group may not be applicable to other more diverse groups. Limiting the search terms to those connected specifically with “physical activity,” rather than “exercise,” reduced the overall sample size, and also likely prevented certain relevant documents from being part of the coding and analysis. The content analysis examined a range of national physical activity organizations, and geographically localized sources were not captured in this study. Further research to understand messages shared by local organizations and direct health care professionals is needed, especially in light of focus group participants’ reliance on these local sources of information. Despite these limitations, this is the first study to examine brain health messages within online publications from primarily physical activity–related sources. The use of two methodologies, content analysis and focus groups, provided unique information on how we can improve organizations’ current messaging about the physical activity and brain health connection to meet the information and resource needs of AD caregivers.
This study has implications for future practice. The lack of specific information related to physical activity and brain health expressed in the focus groups, along with the limited information uncovered in the content analysis, provides the opportunity for new partnerships in public health practice. Physical activity organizations/specialists, aging and brain health researchers, and medical professionals can collaborate to engage communities in health promotion programs and ensure common, consistent messages are delivered regarding the physical activity and brain health connection.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC) or South Carolina Department of Health and Human Services (SC DHHS).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is the result of work conducted by the Centers for Disease Control and Prevention (CDC)-funded South Carolina Healthy Brain Research Network. The CDC Healthy Brain Research Network is a Prevention Research Centers program funded by the CDC Alzheimer’s Disease and Healthy Aging Program through cooperative agreement U48/DP005000-01S7. This work was also partially supported by a contract from the South Carolina Department of Health and Human Services (SC DHHS): A20190088.