
Abstract
Access to recreational and medical marijuana is common in the United States, particularly in states with legalized use. Here, we describe patterns of recreational and medical marijuana use and self-reported health among older persons using a geographically sampled survey in Colorado. The in-person or online survey was offered to community-dwelling older persons aged above 60 years. We assessed past-year marijuana use including recreational, medical, or both; methods of use; marijuana source; reasons for use; sociodemographic and health factors; and self-reported health. Of 274 respondents (mean age = 72.5 years, 65% women), 45% reported past-year marijuana use. Of these, 54% reported using marijuana both medically and recreationally. Using more than one marijuana method or preparation was common. Reasons for use included arthritis, chronic back pain, anxiety, and depression. Past-year marijuana users reported improved overall health, quality of life, day-to-day functioning, and improvement in pain. Odds of past-year marijuana use decreased with each additional year of age. The odds were lower among women and those with higher self-reported health status; odds of use were higher with past-year opioid use. Older persons with access to recreational and medical marijuana described concurrent use of medical and recreational marijuana, use of multiple preparations, and overall positive health impacts.
Introduction
Marijuana use in older persons is growing at a rate that outpaces younger age groups (Lloyd & Striley, 2018; Salas-Wright et al., 2017; Substance Abuse and Mental Health Services Administration, 2013). The 2016 National Survey on Drug Use and Health estimated a prevalence of marijuana use within the past year of 9.0% among adults aged 50%-64% and 2.9% among adults aged ≥65 years; however, this survey does not distinguish between medical or recreational marijuana use (Han & Palamar, 2018). Clinically, medical marijuana has been studied for treatment of chronic pain, chemotherapy-induced nausea and vomiting, Alzheimer’s disease, anxiety, Parkinson’s disease, post-traumatic stress disorder, and epilepsy (Lim, See, & Lee, 2017; Park & Wu, 2017; Whiting et al., 2015). It is also known that some older persons use marijuana for nonmedical or illicit purposes, though only a minority meet criteria for a marijuana-use disorder (Wu and Blazer, 2011). As older persons age, they frequently develop multiple medical conditions and may also experience strains and stresses related to aging such as being a caregiver for another person. In this context, we and others hypothesize that older persons may engage in marijuana use for both medical and recreational reasons (Black & Joseph, 2014). However, no studies have evaluated patterns of use in jurisdictions where medical marijuana and legalized recreational marijuana are both available.
An integrative theoretical foundation is essential for understanding how older persons may choose to use marijuana, whether for medical or recreational purposes. This case builds on clinical psychology theories that frame health beliefs and behaviors, cognitive processing, social and environmental influences, and self-management and determination. Specifically, Becker’s Health Belief Model describes the role of individual perceptions of risk, danger, cost-benefit, and social cues in shaping opinions and cannabis use behaviors among older persons (Becker, 1974; Janz & Becker, 1984). Bandura’s Social Cognition and Learning Theory emphasizes the importance of reciprocal dynamism between the individual, their behaviors, and the environmental factors to affect the individual’s attitudes and behaviors (Bandura, 1977, 1986). From Ajzen and Fishbein, the Theories of Reasoned Action and Planned Behavior inform the understanding of marijuana use decision making of older persons, as well as the clinical recommendation behaviors of practicing physicians (Ajzen, 1985; Ajzen & Fishbein, 1980; Fishbein & Ajzen, 1975).
In 2012, Colorado became one of two U.S. states to legalize retail sales of recreational marijuana to individuals of age 21 and older. Recreational sales started in January 2014. The Colorado Department of Public Health and Environment Medical Marijuana Registry data showed that older persons constituted 21% of registered individuals (Colorado Department of Public Health & Environment, 2018b). However, this medical marijuana registry does not include individuals who use marijuana for recreational purposes. Thus, practicing clinicians do not have accurate data on the prevalence of marijuana use among older persons that is inclusive of both medical and recreational sources. In addition, practicing clinicians do not have studies to inform how people are using marijuana, where they are obtaining it from, why they are using it, or potential positive or negatives effects of marijuana use. Therefore, this study aims to describe the patterns of marijuana use during later life for those who have access to recreational and medical sources of marijuana. The study also assesses predictors and health impact of marijuana use in the past year among older persons. The results of this work aligns with Priority 3 of the World Health Organization’s (2017) “Global Strategy and Action Plan on Ageing and Health” which details the importance of gathering data about older persons and their health patterns and needs in strategic Objective 5.
Method
Design
This is a state-wide, cross-sectional survey to describe patterns of use, reasons for use, and impact on health outcomes associated with past-year marijuana use among older Coloradans aged 60 and above. Given the research focus on understanding an older person’s experiences related to marijuana use, a cross-sectional design was chosen because it prioritizes surveying a larger and more diverse group of participants rather than longitudinally surveying a smaller group multiple times. The study uses a purposive sampling design because the estimated prevalence of marijuana use within the past year among adults aged ≥65 is very low, estimated at less than 3% (Han & Palamar, 2018). Thus, a random sampling of older persons who use marijuana from a population-based sample would be prohibitively large. Participants could complete the survey on paper or online. Online versions collected data directly into an encrypted, secure database (Qualtrics, Seattle, WA and Provo, UT). Research staff entered data from paper versions. A second staff member checked for data accuracy
Setting and Participants
A purposive sample of 274 older persons were recruited from June 2017 through November 2017 from local departments of health, senior centers, wellness and health clinics, state-registered cannabis clubs, and cannabis retail shops and dispensaries located in each of Colorado’s geographically defined 16 areas served by the Area Agencies on Aging (AAAs). This purposive sampling strategy enabled recruiting older persons based on their use of marijuana as well as other key characteristics including place of residence and access to medical cannabis clinics. In particular, by engaging program directors from senior centers and other aging program delivery sites (e.g., congregate dining sites) located within each of the 16 geographically defined AAA, we expected to recruit a sufficient number of older persons who have never used marijuana. By relying on program directors from health and wellness clinic as well as cannabis clubs located across these 16 regions, we expected to recruit a sufficient number of older persons who currently use marijuana for recreational or medical purposes. Inclusion criteria were English-speaking adults who were aged at least 60 years because anyone aged more than 60 can access AAA services. Individuals were encouraged to participate regardless of past history of marijuana use. Recruitment strategies included engaging leadership from AAAs and community programs, distribution of Institutional Review Board (IRB)-approved flyers in community settings, and some dispensaries contacted clients by telephone and posted flyers with the online link. Use of community-based strategies, including distribution online, prevents determination of a survey response rate. Supplemental Figure shows participation from 13 of 16 Colorado geographic AAA regions. Public agencies varied in their willingness to assist with recruitment on what some perceived to be a controversial topic among their constituents. In addition, recruitment may have been limited because communities have local ordinances that restrict marijuana sales.
Survey and Measures
Design of the survey instrument was grounded theoretically in the age-period-cohort paradigm discussed in previous studies (Kaskie, Ayyagari, Milavetz, Shane, & Arora, 2017). A multidisciplinary research team used the paradigm and the integration of clinical psychology theories as introduced to generate survey questions (Kaskie et al., 2017). The survey was piloted and revised based on input from four focus groups of older persons. The final instrument included 83 questions. The estimated time to complete was approximately 30 min. All respondents answered questions on lifetime and past-year marijuana use, demographic characteristics, and health-related questions. The dependent variable is the response to the question, “In the past year, did you use marijuana?” Responses could be “medical purposes only,” “recreational purposes only,” “both,” or “I did not use marijuana in the past year.” Those who reported any marijuana use in the past year completed additional sections on patterns and methods of use (conditional sections depending on whether respondent indicated recreational or medical use). Potential sources of marijuana included the following: retail marijuana store, medical marijuana dispensary, own grown, purchased from someone, or gift. Potential methods or preparations of use included the following: smoking, capsules, vaporizer, edible, cream, liquid tincture, or dabbing. Health-related items included self-report of chronic conditions, use of benzodiazepines or opioids in the past year, individual questions about health outcomes (i.e., overall health and well-being, quality of life, day-to-day functioning, memory, falls/balance, driving, and accidents/injuries), and individual questions about health-care use (i.e., medical visits, emergency department visits, and hospitalization). Standardized rating of health was assessed through Patient-Reported Outcomes Measurement Information System (PROMIS) scores for global health, physical health, and mental health. PROMIS scores were calculated using the recommended scoring method that calibrates each score to a U.S. national mean of 50 and standard deviation (SD) of 10 (Hays, Bjorner, Revicki, Spritzer, & Cella, 2009). The PROMIS global physical health and global mental health had internal consistency reliability coefficients of 0.81 and 0.86, respectively (Hays et al., 2009).
Statistical Analysis
Descriptive statistics included prevalence of past-year marijuana use by three types: recreation, medical, or both. Univariate analyses were conducted to describe the entire sample. Independent variables included age (in years); gender (male, female, and other); education (less than high school or high school graduate, some college, college graduate, and graduate degree); marital status (partnered, divorced/separated, widowed, and never married); retirement status (not retired and retired); being the primary caregiver of someone older than 60 years old in the past year; opioid use in the past year; benzodiazepine use in the past year; and PROMIS scores for global health, physical health, and mental health.
Among past-year marijuana users, patterns of access and methods of use were examined using frequency distributions. Respondents could indicate multiple preparations or sources. Among past-year marijuana users who indicated use for medical purposes, reasons for use (self-reported diagnosis or condition) and health outcomes of marijuana use are described. The frequency of medical conditions indicated by the respondents for which they used medical marijuana and the proportion of individuals who felt that medical marijuana improved, worsened, or led to no change are shown.
To determine group differences for continuous variables (age and PROMIS scores), we used independent sample t tests to compare sample means among respondents who reported past-year marijuana use versus respondents who reported no past-year marijuana use. To determine group differences for discrete variables (gender, education, marital status, retirement status, caregiving status, opioid use, and benzodiazepine use), we used z tests to compare sample proportions among respondents who reported past-year marijuana use versus respondents who reported no past-year marijuana use. Both bivariate analyses were done only for those who responded to the question on past-year marijuana use. A binary logistic analysis model was used to examine correlates of past-year marijuana use. All independent variables included in this analysis were presented to all survey respondents. Participants (14%) were excluded from the multivariate logistic analysis if data were missing. Given the relatively small sample size, only the PROMIS Global Health score (instead of mental health or physical health) was used. Coefficients from this simple logit were converted to odds ratios for meaningful interpretation. A p value of 0.05 or less (two-sided) was considered statistically significant.
All analyses were done using Stata/IC, version 14, software. We used the CHERRIES and STROBE cross-sectional checklists to write this report (Eysenbach, 2004; von Elm, Egger, Pocock, Gotzsche, & Vandenbroucke, 2007).
Results
Sample Characteristics
A total of 274 individuals completed the survey. Table 1 presents sociodemographic and health characteristics for the entire sample. Mean age was 72.5 years (SD = 6.6) with ages ranging from 60 to 94 years. The majority of the sample was female (65%). The sample had relatively high educational level, were partnered, and retired. Although 274 individuals completed the survey, only 196 responded to the question, “In the past year, did you use marijuana?.” Of the 196 individuals who answered, 89 (45%) individuals reported past-year marijuana use. Table 1 shows the differences in respondent characteristics between respondents who used marijuana in the past year versus respondents who did not use marijuana in the past year. Those reporting use were more likely to be younger, partnered, and a primary caregiver to an older person in the past 12 months. Report of past-year opioid use and benzodiazepine use were also higher among past-year marijuana users as compared to nonusers.
Demographic, Social, and Health Characteristics for Respondents, by Past-Year Marijuana Use.
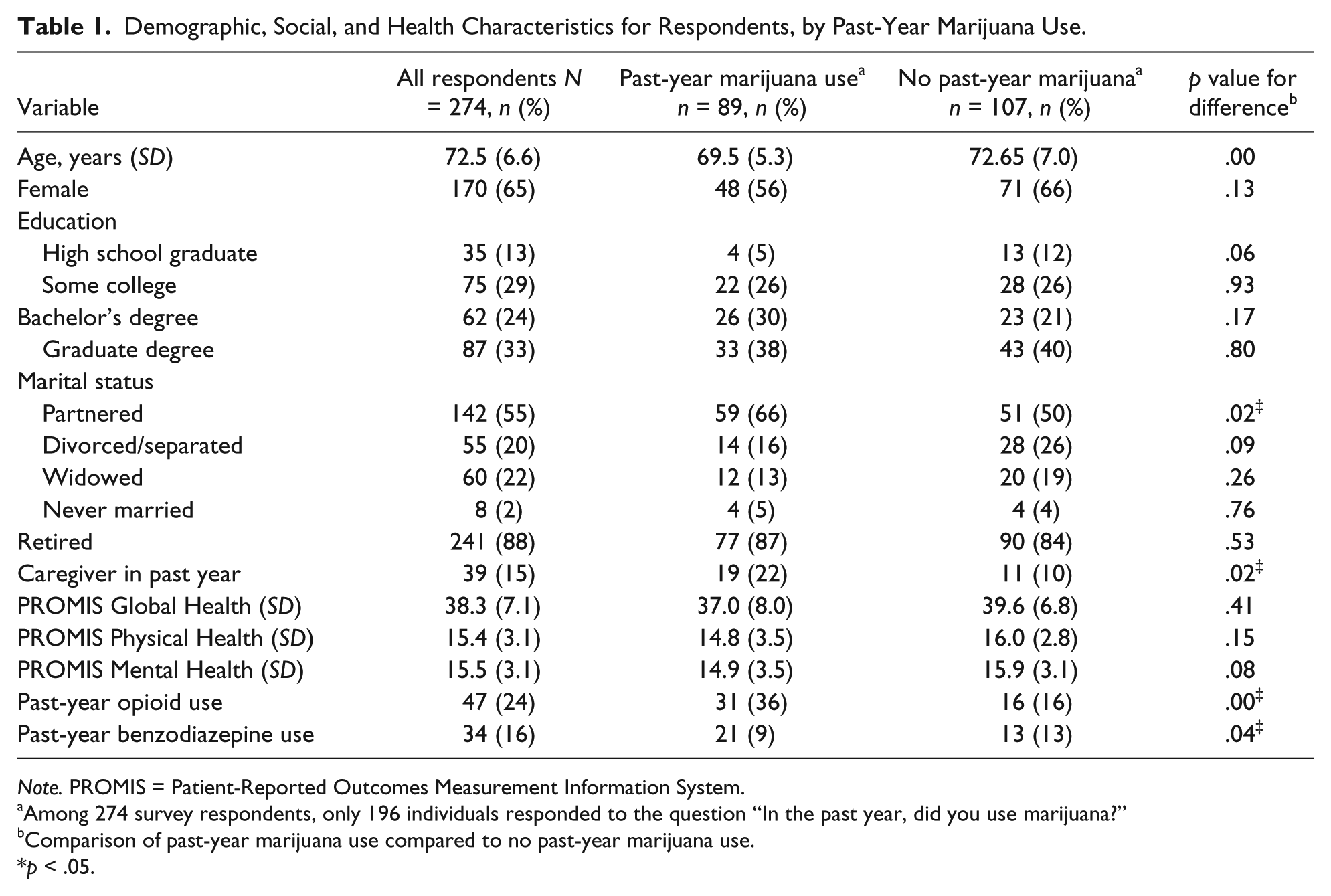
Note. PROMIS = Patient-Reported Outcomes Measurement Information System.
Among 274 survey respondents, only 196 individuals responded to the question “In the past year, did you use marijuana?”
Comparison of past-year marijuana use compared to no past-year marijuana use.
p < .05.
The response rate to the question, “In the past year, did you use marijuana?” was 72%. Since this is the primary outcome, Supplemental Table provides an analysis of the demographic differences between respondents and nonrespondents to the question to examine any bias in nonresponse for this question. On average, nonrespondents were older, had lower levels of formal education, and were more likely to be widowed than respondents.
Patterns of Marijuana Use
Figure 1 shows the distribution of whether respondents had used marijuana in the past year, and if so, whether they used it for medical purposes, recreational purposes, or both. Among past-year marijuana users (n = 89), 48 respondents (54%) reported both medical and recreational purposes. The percent of medical only users was higher than those who reported use of recreational marijuana only. In Figure 2, a majority of past-year marijuana users reported smoking/inhaling as their preferred method or preparation of marijuana use—whether alone or with other methods. In addition to smoking, other common methods of use included edible and topical formulations (creams and ointments). Topical formulations were used by 52% of past-year marijuana users, and this method was for medical rather than recreational use. In general, older persons preferred multiple methods or preparations of marijuana. Only 30% past-year marijuana users reported a single method of use. Methods such as dabbing, capsules, and vaporizers were almost always used with another method.

Reasons for marijuana use.

Methods of marijuana use.
Figure 3 shows the preferred source of marijuana among past-year marijuana users. Unlike methods of use, a majority of older persons reported only one source for obtaining marijuana. The most common sources (whether alone or in conjunction with another source of marijuana) were retail stores, medical dispensaries, and receiving marijuana as a gift. Growing and individual purchase were typically used in addition to obtaining marijuana from other sources.

Method of marijuana access.
Reasons for Medical Marijuana Use
A total of 60 respondents provided reasons for past-year medical marijuana use. Figure 4 shows that respondents typically indicated multiple medical conditions as reasons for medical use of marijuana. Arthritis was the most common condition, for which respondents reported using marijuana, whether alone or in conjunction with another condition. Spinal conditions including chronic back pain, anxiety, and depression were other frequent reasons for medical use of marijuana, although depression and anxiety were almost present with other conditions.
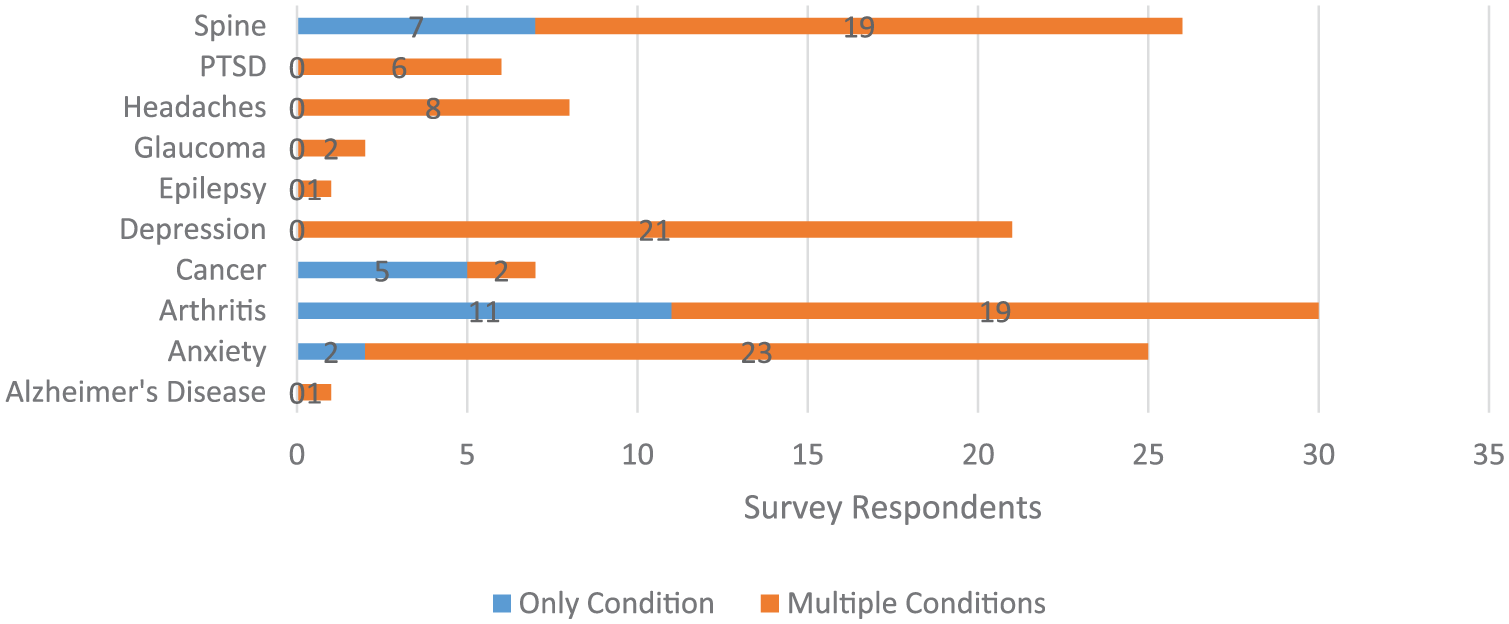
Reasons for marijuana use.
Health Impact of Marijuana
Figure 5 shows that past-year marijuana users frequently reported better overall health and well-being, quality of life, day-to-day functioning, and improved pain. Approximately 40% reported no change in day-to-day functioning. Close to 80% reported improvements in pain. In terms of potential negative health outcomes, Figure 6 shows that most respondents reported no problems with falls/balance, driving, or accidents/injuries related to marijuana use. Notably, about 22% reported “some problems” related to memory loss due marijuana use. Those who reported using opioids and benzodiazepines in the previous year were asked whether marijuana use changed their use of these medications. While sample sizes are small (N = 35 for opioid change respondents and n = 25 for benzodiazepine change respondents), a majority noted that marijuana use led to a reduction or discontinuation of these medications. No respondents reported increased use of opioids or benzodiazepines related to marijuana use. Past-year marijuana users reported no changes in medical visits, emergency department visits, or hospitalization.

Impact of marijuana on health outcomes.

Impact of marijuana use on functional outcomes.
Predictors of Past-Year Marijuana Use
Table 2 provides adjusted odds ratios for individual sociodemographic and health predictors of past-year marijuana use (N = 167). After adjusting for covariates, each additional year of age decreased the odds of using marijuana in the past year. Furthermore, the odds of past-year marijuana use were lower among women (than men) and those with higher self-reported health status as measured by PROMIS Global Health scores. The odds of past-year marijuana use were higher with past-year opioid use (than no past-year opioid use) and trended to higher odds of use with higher levels of educational attainment (than being a high school graduate). Past-year benzodiazepine use was not associated with increased odds of marijuana use in the past year.
Adjusted Odds Ratios Showing Odds of Past-Year Marijuana Use (n = 167).

Note. PROMIS = Patient-Reported Outcomes Measurement Information System.
p < .05.
Discussion
In this survey of community-dwelling older persons which included some people who had used marijuana in the past year and some who had not, 56% of the past-year marijuana users reported using marijuana for both medical and recreational purposes. To our knowledge, this is the first study to provide a detailed description of distinct and varied marijuana use patterns among older Coloradans who have access to medical and recreational marijuana. The patterns of use often included use of more than one preparation of marijuana (smoking, topical and edibles) and common medical conditions included arthritis, pain, anxiety, and depression. Respondents frequently reported positive health impacts from marijuana use. When comparing persons who had used marijuana in the past year compared to those who had not, marijuana use decreased with age, was lower among women, and was lower among those with higher self-reported health status. These factors are similar to other population-based studies in older persons (Black & Joseph, 2014; Lloyd & Striley, 2018).
Given the increasing prevalence of current marijuana use among persons aged 65 years and above (Colorado Department of Public Health & Environment, 2018a), this study has clinical implications. In particular, since older persons described various patterns of marijuana use, clinicians can recognize the importance of asking about whether their patient uses both medical and recreational marijuana, reason(s) for use, preparation(s) of marijuana, and perceived benefits and side effects. In addition, another study found that older persons often reported a desire to access marijuana through a primary-care physician but that they faced obstacles with physician communication such as physician lack of knowledge or unwillingness to discuss marijuana use (Bobitt et al., 2018). This could be one reason why older persons are choosing to use recreational marijuana in addition to medical marijuana. For some patients, use of recreational marijuana may represent poorly controlled medical conditions or symptoms that the patient would like treatment for.
Aligned with a 2017 National Academy of Sciences report describing conclusive evidence of cannabis’ efficacy in treating chronic pain, common reasons for medical marijuana use were pain-related including arthritis and chronic back pain (Institute of Medicine, 2017). In particular, there was frequent use of topical formulations of marijuana, and this was typically for medical rather than recreational use. Although there are few clinical efficacy studies of topical marijuana, given the high prevalence of pain among older persons and potential side effects of systemic medications such as nonsteroidal anti-inflammatory drugs (NSAIDs) and opioids, topical medications may be a safe alternative for effective pain control. However, high-quality clinical research studies are needed before marijuana is recommended as a substitute for opioids to treat pain (Humphreys & Saitz, 2019). Marijuana use for comorbid behavioral health conditions including anxiety and depression was also common, suggesting another reason for routine assessment of marijuana use by general medical and behavioral health practitioners. Given medical marijuana laws have been associated with self-medication for mood or anxiety disorders (Sarvet et al., 2018), clinicians should be aware that access to both medical and recreational marijuana may also increase marijuana use. The relationship between marijuana use for medical and recreational purposes in the context of opioids is clinically important (Choi, DiNitto, Marti, & Choi, 2017). In this study, past-year opioid use was associated with past-year marijuana use. This is consistent with another study that found an association between nonmedical marijuana use and nonmedical opioid use among individuals aged 50 and above (Choi et al., 2017).
Survey participants generally self-reported positive health impacts. Although older persons are susceptible to adverse events related to marijuana use, survey respondents who indicated marijuana use in the past year did not report increased falls, accidents, or injuries. In addition, there was no reported change in health-care utilization, although this was not verified. Therefore, our results are similar to another study of older patients treated with medical cannabis that showed treatment was effective in improving pain and quality of life, and was not associated with serious adverse events (Abuhasira, Shbiro, & Landschaft, 2018). However, this study should be interpreted in the broader context of other studies that have shown marijuana use increases the likelihood of emergency department visits through increased injury risk among adults aged 50 and above (Choi, Marti, DiNitto, & Choi, 2018). In addition, older persons may experience common adverse events due to cannabis use such as dizziness, euphoria, drowsiness, confusion, and disorientation. Because self-report of adverse effects can be affected by sampling or social desirability bias, future studies, and clinical care should use a systematic and routine assessment of potential side effects.
Our analysis also illuminated that despite legalization of both medical and recreational marijuana, survey questions on marijuana use continue to be sensitive. Nearly 30% of the total respondents did not answer the question related to past-year marijuana use, indicating a likely bias among respondents versus nonrespondents. Future studies on outcomes of marijuana use should conduct a detailed analysis of such nonresponse bias and recommend strategies to reduce it.
This study has several limitations. The primary limitations are use of convenience sampling and lack of generalizability. The number of past-year marijuana users for any reason is higher in this sample than in other studies (Colorado Department of Public Health & Environment, 2018b; Han & Palamar, 2018; Reynolds et al., 2018) due to the sampling methods and respondent bias. Since this is a community-based sample of older persons from geographically diverse areas, including a high percentage of rural and frontier-residing persons, a larger population-based study is needed for generalizability. Finally, the medical conditions, use of opioids or benzodiazepines, and health-care utilization outcomes were only self-reported.
In conclusion, surveyed older persons aged more than 60 who have legal access to recreational and medical marijuana described multiple patterns of use of marijuana in the past year, and the majority felt that marijuana use had an overall positive impact on their quality of life. This study has implications for how clinicians ask older persons about their use of marijuana. Clinicians should go beyond asking whether patients use marijuana or not. In particular, detailed questions should inquire about where marijuana is obtained from, reasons for use, and perception of benefits or harms due to use. In addition, these findings suggest the need for clinician education and evidence-based policies to guide shared decision making related to marijuana use in the context of the patient’s preferences and medical needs.
Supplemental Material
Appendices_(1) – Supplemental material for Patterns of Marijuana Use and Health Impact: A Survey Among Older Coloradans
Supplemental material, Appendices_(1) for Patterns of Marijuana Use and Health Impact: A Survey Among Older Coloradans by Hillary D. Lum, Kanika Arora, J. Alton Croker, Sara H. Qualls, Melissa Schuchman, Julie Bobitt, Gary Milavetz and Brian Kaskie in Gerontology and Geriatric Medicine
Supplemental Material
Appendix_1_-_Survey – Supplemental material for Patterns of Marijuana Use and Health Impact: A Survey Among Older Coloradans
Supplemental material, Appendix_1_-_Survey for Patterns of Marijuana Use and Health Impact: A Survey Among Older Coloradans by Hillary D. Lum, Kanika Arora, J. Alton Croker, Sara H. Qualls, Melissa Schuchman, Julie Bobitt, Gary Milavetz and Brian Kaskie in Gerontology and Geriatric Medicine
Supplemental Material
FIGURE – Supplemental material for Patterns of Marijuana Use and Health Impact: A Survey Among Older Coloradans
Supplemental material, FIGURE for Patterns of Marijuana Use and Health Impact: A Survey Among Older Coloradans by Hillary D. Lum, Kanika Arora, J. Alton Croker, Sara H. Qualls, Melissa Schuchman, Julie Bobitt, Gary Milavetz and Brian Kaskie in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
The authors would like to thank Joanna Dukes, MS, for her assistance with manuscript preparation.
Authors’ Note
Hillary D. Lum and Kanika Arora are co-first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Colorado Department of Public Health and Environment. Dr. Lum was additionally supported in part by the National Institutes of Health (K76AG054782).
Ethical Approval
The study was approved by the University of Colorado Colorado Springs (UCCS) Institutional Review Board. All participants were informed of their rights as research participants, voluntarily participated, and were not compensated. Participants could withdraw from the study at any time. This study had a waiver of signed consent because written consent would have been the only identifiable information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.