
Abstract
The conceptual framework, targeting of older adults, and content of a targeted geriatric trauma consult (GTC) performed by geriatricians at a Level 1 trauma center are highlighted. The GTC is designed to optimize patient care through comprehensive assessment and to interrupt the disablement process. In a performance improvement study, fellowship-trained and certified geriatricians conducted the GTC in 98 patients ranging in age from 68 to 100 years. Most common recommendations by the geriatricians were for transitions of care (e.g., home health, skilled nursing facility, hospice), changes in medications (e.g., antihypertensives, antidepressants/antipsychotics), advanced care planning, and specialist referral. Targeted GTC performed by a geriatrician is an efficient approach to comanagement of complex older trauma patients, in contrast to mandated geriatric team consultation. In settings of value-based care, GTC by a geriatrician has potential to reduce patient disability and health care costs compared with usual care of older trauma patients.
Trauma is the seventh most common cause of mortality in the United States among adults aged 65 years and older (Minino, Anderson, Fingerhut, Boudreault, & Warner, 2006). With aging of the American population, the incidence of hospitalization for trauma among older adults is increasing. Furthermore, the rate of fractures and other injuries is higher for adults aged 85 years and older compared with those aged 65 to 84 years (Kochanek, Murphy, Xu, & Tejada-Vera, 2016). Preinjury physical frailty and cognitive impairment determine postinjury functional recovery and survival among geriatric trauma patients (Maxwell et al., 2016). The older trauma patient is characterized by a higher rate of multiple chronic conditions, dementia, frailty, and limited prognosis (Harvey, Mitchell, Brodaty, Draper, & Close, 2016). Clinical studies demonstrate improved quality of care and improved outcomes of geriatric trauma when patients with hip fractures are assessed and managed by a team of geriatricians and trauma surgeons (Fallon et al., 2006). In particular, orthogeriatric care models have demonstrated, in clinical trials and systematic reviews, improved mortality and functional outcomes among older patients with hip fracture (Grigoryan, Javedan, & Rudolph, 2014; Kristensen, Thillemann, Soballe, & Johnsen, 2016). Geriatric consultation and proactive geriatric trauma consultation services are growing more common in the United States abetted by clinical guidelines that address geriatric trauma management (American College of Surgeons, 2012). Previous studies have focused on orthopedic–geriatric comanagement or consultation primarily for patients with hip fractures. Most studies included mandated geriatric consultation and were often conducted in safety-net hospitals or academic medical centers (Fallon et al., 2006; Wong et al., 2017). In these settings, geriatricians or hospitalists are part of a multidisciplinary team that conducts a geriatric assessment using commonly employed measures or tools. This evaluation requires completion of various measures (instruments) and is time-consuming. In the fast-paced setting of the acute care hospital, completion of this comprehensive assessment is often impractical or imposes additional burdens on patients and caregivers.
Previous studies of geriatric consultation in hospitals suggest that effectiveness is greater when consults are targeted at patients most responsive to the intervention (Winograd, Gerety, & Lai, 1993). The need to target consults is further demonstrated by a negative study on clinical outcomes of mandated geriatric consultations for trauma patients (Dugan, Burns, Baldawi, & Heidt, 2017). Costs and time efficiencies might be improved by targeting consults at patients deemed to be complex by the trauma surgeons and likely to benefit from consultation. Although previous studies have provided summaries of the types of medical issues evaluated by a geriatric consult team on trauma patients, none have explored the specific recommendations made by board-certified and fellowship-trained geriatricians during trauma consultations on older patients, not including hip fractures, to the referring trauma surgeons.
We had the opportunity to initiate an inpatient geriatric medicine trauma consult service in 2015, at a Level 1 trauma service in a hospital affiliated with Eastern Virginia Medical School (EVMS). Prior to its inception, the consult service criteria for referral from the trauma surgeons were agreed upon and only patients aged 75 years and older thought by the trauma surgeons to benefit from consultation were referred to the geriatrics service. The geriatricians performing the consultations are fellowship trained and board certified in geriatric medicine. The trauma surgeons are board-certified surgeons and, like the geriatricians, are full-time faculty at EVMS. As experienced geriatricians, the physicians inculcated into the consult practice the principles of comprehensive geriatric assessment, which are reflected in their recommendations. The geriatricians are able to rapidly assess the patient’s functional status, mobility, socioeconomic status, mental/cognitive health, and goals of care (patient preferences, advance directives, prognosis). By training, geriatricians are oriented to interdisciplinary collaboration with other health professionals.
As this was a new consultation service, the geriatricians conducted a performance improvement evaluation based on the first 118 patients (98 met eligibility criteria) seen in consultation to better characterize the reasons for the consult and the range of recommendations made to the trauma team (the “black box” of consultation). The Institutional Review Board at EVMS ruled the performance improvement study as nonresearch.
Conceptual Framework
The conceptual framework of the geriatric consultation was the prevention of the disablement process, a concept commonly applied to gerontological research. The disablement process, extrapolated to the acute care of hospitalized trauma patients, relates pathology to impairments, functional limitations, and disability (Verbrugge & Jette, 1994). In the main model, pathology includes diagnoses of disease and relevant comorbid conditions; type and severity of injury; impairments including dysfunctions and abnormalities in specific body systems; predisposing demographic, social, lifestyle, and behavioral characteristics; functional limitations, including restrictions in performance of basic physical and mental actions including ambulation and psychological coping mechanisms; and disability in daily activities, self-care, and socialization. The framework of the disablement process has demonstrated the importance of functional limitations as an intermediary factor in the disablement process (Lawrence & Jette, 1996). The disablement process relates closely to the International Classification of Impairments, Disabilities and Handicaps (Bickenbach, Chatterji, Badley, & Ustun, 1999) and the International Classification of Functioning, Disability and Health (World Health Organization, 2001). Functioning and disability are adversely affected by injuries and illnesses affecting body functions and structures (e.g., with multiple traumatic fractures) and further exacerbated by contextual factors both environmental (e.g., hospital room, sleep deprivation, limited mobility) and personal (e.g., patient motivation). Physical impairments (e.g., traumatic fracture, delirium) can result in disabilities that limit independent performance of normal community activities.
The goal of geriatric consultation of hospitalized trauma patients is to recognize the potential interventions effectively preventing impairments, functional limitations, and ultimately disability. Consultation also considers patients’ preferences for care, their short-term and long-term goals of medical care, and their prognosis for recovery from serious injury such as traumatic brain injury. Often this requires interview with family members and specifically the patient’s medical power of attorney or next of kin.
Method
Study design was a retrospective chart review. Eligible patients were aged 75 years and older admitted to the trauma service and seen in consultation by internal medicine specialists, fellowship trained and certified in geriatric medicine, at the discretion of trauma surgeons. The eligible population did not include patients with a principal diagnosis of hip fracture but did include patients with other fractures, burns, extensive/multiple fractures, and traumatic brain injury such as subdural hemorrhage. Two patients below age 75 were seen at the surgeons’ special request. Charts of patients were included in the study if they contained the following elements: reason for consult, history of present illness, past medical history, past surgical history, medications, review of systems, physical examination, summary assessment, and recommendations. Of 118 patient charts, 20 did not contain full consultation notes as some did not contain all elements, leaving 98 complete notes available for evaluation.
The consultations were performed at Sentara Norfolk General Hospital, a Level 1 trauma center in Southeastern Virginia with a catchment area extending to northern North Carolina. All geriatricians and trauma surgeons have full-time faculty appointments at EVMS in Norfolk, Virginia.
Consultation Referral
The trauma surgery service called the geriatric medicine office with the referral for consultation. Information about the patient included the following: patient’s name, room number, date of birth, reason for consult, and stat or 24-hr request. The geriatrician reviewed the electronic medical record to obtain available information about the patient’s principal diagnosis, medical history, diagnostic and laboratory test results, family contact, presence of an advanced directive, and code status (e.g., “Do not resuscitate”).
Consultation Note Content
Consultation notes summarized assessment and key recommendations with generally less than 10 specific recommendations. The note briefly summarized the history of present illness, relevant past medical and surgical history, home and current medications, personal and social history, targeted physical examination, and relevant laboratory studies. The patient’s goals of care, both short term and long term, were identified in conversation with patient and family and were included in the consultation note. The geriatrician reviewed assessment and recommendations with the trauma team of surgeons, residents, and advance practice providers and remained available for follow-up consultation. The analysis, however, is limited to the initial consultation by the geriatrician.
Geriatric Assessment
Through review of the electronic medical record, interview of the patient, and the medical power of attorney for health care or next of kin, a geriatrician gathered information that is routinely included in a comprehensive geriatric assessment (Reuben & Rosen, 2009; Table 1). The geriatric assessment domains, ascertained primarily by medical interview, chart review, and bedside evaluation of the patient, uncommonly employed validated assessment instruments. Patient examination, documentation, counseling and education of patient and family, and feedback to the trauma team were usually completed within 60 min. On occasion, at the trauma team request, a geriatrician wrote orders but otherwise did not provide comanagement.
Components of Geriatric Assessment by Geriatrician Consultants.

Note. ADL = Activities of Daily Living.
Data Analysis
Descriptive data included the reason for the consult, clinical characteristics of patients, including comorbid conditions, medication appropriateness, trauma type, and type of consultant recommendations to the trauma team.
Results
Patients at the time of consult ranged from 68 to 100 years of age with a median of 84. Of the 98 patients, the trauma type was subdural hematoma/hemorrhage in 46%, extremity fracture in 17% of patients, other fractures in 44%, and burns in 3%. Information on reasons for consult was unstated in three records. Five consult requests were made for multiple reasons, for example, polypharmacy and medical assessment. The analysis is reported based on the primary/first listed reason. Most common recommendations were for transitions of care such as home health, skilled nursing facility or hospice, blood pressure medication changes, discontinuation or change of antidepressants/antipsychotic medications, advanced care planning, and specialist referral. Less commonly, recommendations were to implement a do-not-resuscitate order, initiate a family meeting/discussion, change the management of diabetes mellitus, and make a social work referral (Figure 1). Potentially inappropriate medications were identified using the American Geriatrics Society’s Beer’s list criteria (American Geriatrics Society, 2015). Potentially inappropriate medications were identified in 23% of records. The most frequent comorbid condition was dementia (32%), while some form of cognitive impairment, usually delirium or stupor, was present in 50%. Impairment in baseline performance of instrumental activities of daily living was present in 55% of patients. Significant comorbid conditions are listed in Table 2.
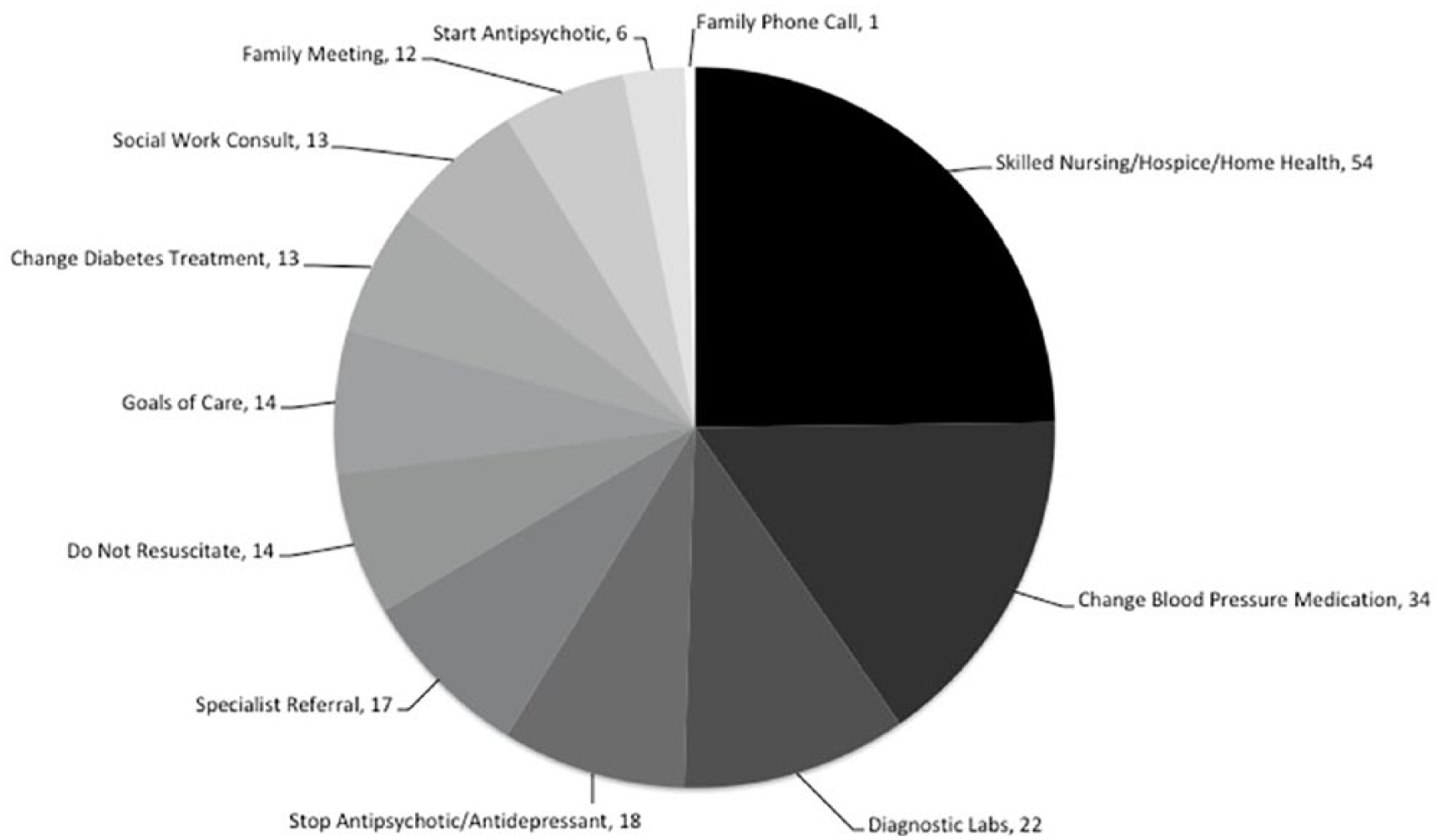
Geriatrician consultants’ recommendations to trauma team.
Common Comorbid Conditions in 98 Patients.

Note. Total exceeds 100% because some patients had more than one condition.
Commonly, goals of care discussions were initiated after the geriatrician’s consultation, often by the geriatrician. In-person meetings were conducted whenever feasible; otherwise the family member/medical power of attorney was called at home. The conversation reviewed immediate expectations for prognosis and outcomes, and long-term patient goals of care.
Discussion
In this performance improvement analysis, a geriatrician consultation was able to efficiently evaluate older adults with traumatic injury using the principles of comprehensive geriatric assessment with the goal of preventing functional limitations and disability (disablement) while also considering short-term and long-term patient prognosis. Our analysis provides insight into the content of geriatric consultation by specific indications for the consultation, the types of medical conditions seen in this population, and the heterogeneous list of recommendations made by the geriatricians to the surgical team. While we did not track patients following transitions of care, the feedback we received informally from the surgeons was uniformly positive. This performance improvement study has helped the geriatricians to modify the format of the consultation note to highlight “Key” recommendations up front in the consultation note that are of critical importance to the surgeons. Patient safety and quality of care are of high priority to the trauma team, and most of the recommendations made by the geriatricians addressed these areas of priority.
Previous studies demonstrate the value of a geriatric assessment of trauma patients. In one Canadian study of patients aged 65 years or older who received a mandatory geriatric consultation, efficiency of the consultation collaboration could be achieved through a three-step evaluation and improvement process, thereby demonstrating a method of quality improvement once a protocol is established. In that study, 88% of recommendations provided by the consultants were implemented by the trauma team demonstrating that collaborative effort with geriatrics consultants is valued by trauma surgeons (Wong et al., 2017).
Our consultation emphasized medication evaluation, advanced care planning and transitions of care, and focused recommendations to the trauma team. While other studies of trauma consultation have described the use of mandated instruments and screening tools, experience in outpatient and other settings suggests that in clinical settings lengthy and potentially burdensome evaluations are not feasible or practical. In our model of consultation, a fellowship-trained and experienced geriatrician inculcates the geriatric assessment into the bedside evaluation of trauma patients, many of whom are very frail, have fall-related injuries, and are at high risk of repeated falls and possible long-term care institutional placement. Gathering the appropriate information from a comprehensive assessment is valuable to help weigh the risks and benefits of procedural treatments (e.g., drainage of subdural hematomas) and in turn helps to identify goals of care. Frailty, impaired physiological reserve, plays a role in determining the planning and course of treatment and an understanding of outcomes relevant to older trauma patients. Frailty predicts postoperative complications, mortality, risks of postacute facility transition, length of stay, and length of intensive care unit stay (Orouji Jokar et al., 2016). Undergoing a surgical procedure is a significant stressor for a vulnerable (frail) older adult.
Multiple preexisting comorbid conditions and cardiovascular, nervous, renal, and musculoskeletal conditions present additional complexity in caring for the older trauma patient (Brooks & Peetz, 2017). For example, occult hypotension may be seen in as many as 20% of geriatric trauma patients (Salottolo, Mains, Offner, Bourg, & Bar-Or, 2013). The physiological response to trauma may be blunted by common medications prescribed to older adults that can compromise physiological and cognitive function. Most commonly, we observed the use of medications with anticholinergic and sedative-hypnotic properties as most likely inappropriate for older adults with serious traumatic injury. Many of the patients were taking these medications prior to hospitalization. The geriatricians could counsel patients and family caregivers about the risks of these medications and suggest plans to taper and discontinue them.
The limitations of our study include the lack of a control group (trauma care without geriatrician consultation). As this was a performance improvement analysis and we modified our assessment process and medical documentation as a result, the study could not determine the effectiveness of the consultation to prevent the disablement process or to evaluate quality of life and functional status following patient recovery. While previous research and clinical guidelines support the potential value of a geriatric consultation, the results of this analysis are difficult to generalize to hospital settings where there are no fellowship-trained and board-certified geriatricians. However, many of the Level 1 trauma centers are affiliated with academic medical centers where there are departments or divisions of geriatric medicine. The current study is novel in identifying the components of the geriatric consultation (the “black box”) and the potential efficiency of consultation done by a geriatrician in contrast to studies looking at a team of health professionals who conduct mandated consults. Future studies of the clinical effectiveness of geriatricians in this setting are warranted based on the potential to be invaluable to trauma surgeons and patients and to determine costs as health care payments in the country transition from fee-for-service to value-based care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.