
Abstract
This study aimed to determine differences in sitting behavior time (SBT) and health-related quality of life (HRQOL) based on application of the transtheoretical model (TTM) to exercise behavior in overseas-dwelling Japanese. SBT, HRQOL, and various sociodemographic factors were measured in 108 Japanese living in Ipoh, Malaysia. Subjects were classified into the non-exercise (NE), preparation (P), and exercise (E) groups. Workday, non-workday, and total-day SBTs were identified by self-reported questionnaire. The mental component summary (MCS) score for HRQOL was also assessed with the Medical Outcome Study 36-Item Short Form Health Survey (Japanese version). Differences in SBTs and HRQOL based on the TTM were calculated by one-way analysis of variance (ANOVA). After adjusting for sociodemographic factors, there were differences in workday (F = 8.19, p < .001), non-workday (F = 5.96, p = .001), and total-day (F = 9.30, p < .001) SBTs and MCS scores (F = 10.29, p < .001). Non-workday (338.6 ± 210.8 vs. 510.5 ± 213.4 min, p < .05) and total-day (376.8 ± 181.1 vs. 511.8 ± 183.3 min, p < .05) SBTs were lower and the MCS score (53.9 ± 9.5 vs. 48.4 ± 9.6, p < .05) for HRQOL was higher in the E group versus P group. These differences in SBT and HRQOL in relation to exercise behavior indicate that promotion of exercise behavior may be an important public health strategy to reduce SBT and increase HRQOL in overseas-dwelling Japanese.
Keywords
Introduction
Recently, in the Asian region, Malaysia has become the preferred country for long-term living by Japanese (Long Stay Foundation), and their number is tending to increase every year. Unfortunately, the obesity rate of Malaysian people has increased by slightly more than three times in the 10 years from 1996 (4.4%) to 2006 (14%) (Khor, 2012). In addition, associated risk factors such as obesity, high blood pressure, and dyslipidemia increase the number of patients with cardiovascular disease (Ghazali et al., 2015).
Several previous studies have shown the promotion of physical activity (exercise, sports, and increased activities of daily living) and exercise behavior to be effective in preventing and improving various diseases such as diabetes, obesity, some cancers, and high blood pressure (Biswas et al., 2015; Oka, Shibata, Ishii, & Miyawaki, 2014). Even if physical activity is regularly promoted, research in America and European countries in recent years has clarified that people with long sitting behavior time (sedentary time as assessed by sitting time) are at increased health risks for death, obesity, diabetes, and cardiac disease (Biswas et al., 2015). Moreover, sitting behavior time per day in the Japanese adult population has been known for a long time compared with that in foreign countries (Bauman et al., 2011). Therefore, it is important not only to promote physical activity in the Japanese lifestyle but also to decrease sitting behavior time to improve health (Oka et al., 2014).
With regard to the health care of Japanese living overseas such as in Kuwait, Toh (1991) reported that Japanese businessmen had to adapt to climatic, religious, cultural, and historical differences, and as a result, stress-related disease occurred in 15.7% of the total subjects examined, and some of the diseases were very severe. Thus, the behavior of Japanese living overseas may be altered because of the stresses of living in a foreign country.
Health-related quality of life (HRQOL) is one of the health care outcomes assessed both in foreign countries and in Japanese populations (Suzukamo et al., 2011). Several aspects of HRQOL can be measured with the Medical Outcome Study 36-Item Short Form Health Survey (SF-36). The eight subscales of the SF-36 were further combined into the physical component summary (PCS) score, the mental component summary (MCS) score, and the role/social component summary (RCS) score (Suzukamo et al., 2011).
There are very few reports investigating the lifestyle, such as sitting behavior, exercise behavior, and mental health status, of Japanese populations living overseas. Especially, there are no investigations, to our knowledge, of sitting behavior times and MCS scores of HRQOL based on exercise behavior.
We thus hypothesized that based on their exercise behavior, Japanese people living in Malaysia might be more sedentary and experience changes in their sitting behavior time and HRQOL in terms of mental health. Therefore, we aimed to investigate the differences in sitting behavior time and HRQOL based on exercise behavior in Japanese living overseas in Malaysia.
Method
Study Design and Population
This was a cross-sectional study comprising a study population of 130 Japanese people aged 20 years or older residing overseas in Ipoh, Perak, Malaysia, in 2015, who consented to participate. The investigation was accomplished with a self-registered questionnaire that was distributed to these 130 participants by local volunteers who later collected the questionnaires after they had been filled out.
Sociodemographic Factors
Sitting behavior time, HRQOL, and sociodemographic factors such as age, sex (male/female), levels of education (⩽12 or ⩾13 years), marital status (married/non-married), occupation (full time or part-time/non-working), alcohol intake (yes/no), smoking behavior (yes/no), and body mass index as obtained from the participants’ height and weight were collected from the self-reported questionnaire and assessed. Sitting behavior time was identified in the self-reported questionnaire by workday, non-workday, and total sitting time per day.
Sitting Behavior Time
The questionnaire survey was based on the Workforce Sitting Questionnaire (Chau, van der Ploeg, Dunn, Kurko, & Bauman, 2011), the reliability and validity of which were confirmed in a previous study in Japan (Ishii et al., 2018). This questionnaire survey is composed of six items related to sitting behavior time in 1 week according to typical life scenarios: driving, transportation, work, television viewing, personal computer/smartphone use, and other leisure time activity. We requested the participants to answer each item for both workdays and holidays for 7 days (1 week). After collecting the questionnaires, researcher calculated the total sitting behavior time as related to the six life scenarios for workdays and non-workdays for 7 days. Next, researcher calculated the total sitting behavior time in minutes/day as total sitting behavior time in minutes/7 days. Thus, we investigated sitting behavior times for the workday, non-workday, and the total day.
HRQOL
HRQOL was assessed with the Japanese version of the SF-36 consisting of 36 items representing eight subscales covering the domains of physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health (Suzukamo et al., 2011). It measures multidimensional properties of HRQOL on a 0 to 100 scale, with higher scores representing higher HRQOL. To compare scores to the normal Japanese population, the SF-36 subscale scores were converted into a deviation score based on scores of the Japanese national norm, which is a mean score of 50 with a standard deviation (SD) of ±10. In the present study, a score of <50 indicates that the specific health concept is below that of the Japanese national norm. We choose the MCS score of HRQOL as the index of mental health in this study.
Evaluation of Exercise Behavior
Exercise behavior was evaluated by the researcher on the basis of the transtheoretical model (TTM) of exercise behavior change (Prochaska, 2002). This model shows individual progression of exercise behavior through five stages: (a) pre-contemplation—not physically active and no intention to change; (b) contemplation—not active but intending to change; (c) preparation—doing some activity; (d) action—regularly active but activity only begun within the past 6 months; and (e) maintenance—regularly active for longer than 6 months. Subjects classified in the pre-contemplation or contemplation stages were assigned to the non-exercise group (NE group), those in the preparation stage to the preparation group (P group), and those in the action or maintenance stage to the exercise group (E group). It was an assignment according to a result of the answers to the questionnaire.
Ethics
This study was approved by the Institutional Committee on Human Research of the Graduate School of Health Sciences, Kobe University (approval no. 412). Informed written consent was obtained from each participant. The present study complied with the principles of the Declaration of Helsinki regarding investigations in humans.
Statistical Analysis
Results are expressed as mean ± SD. First, we compared workday, non-workday, and total-day sitting behavior times and MCS scores of HRQOL based on the three exercise behavior groups with one-way analysis of variance and chi-square and Tukey’s post hoc tests. Second, if there were significant differences in any of the sociodemographic factors, we also used one-way analysis of covariance (ANCOVA) of the sociodemographic factors. We selected confounding factors as those that were significantly different at p < .05 in the bivariate analyses. An alpha (p) value of <.05 was considered to indicate statistical significance. Statistical analyses were performed with IBM SPSS 23.0 statistical software (IBM SPSS Japan, Inc., Tokyo, Japan).
Results
Among the 130 participants, 115 returned the self-registered questionnaire, giving a response rate of 88.5%. Some data of seven of the 115 questionnaires were missing or double answers were given, and these questionnaires were also excluded from the analysis. Therefore, in the final analysis of the population, each index could be analyzed in 108 of the 130 participants (83.1%; Figure 1).
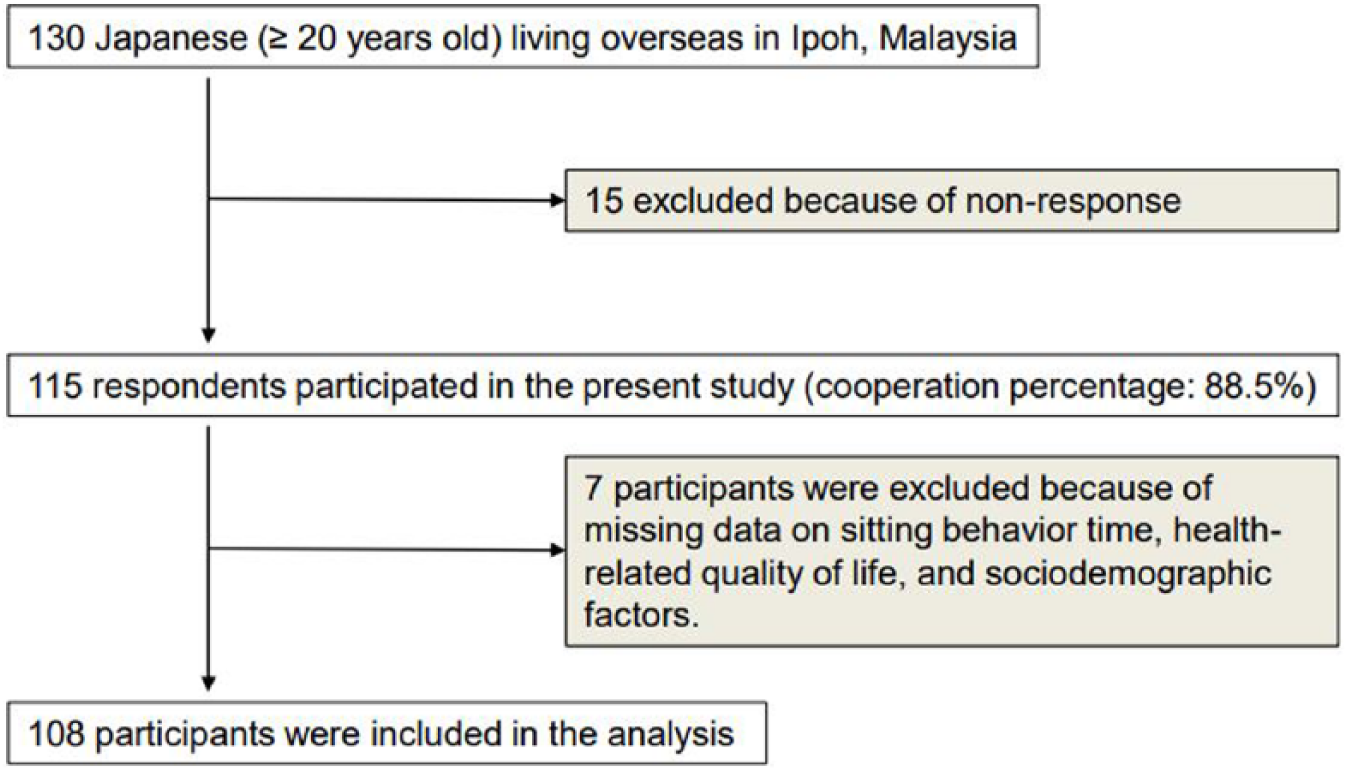
Flow diagram of the participant selection process.
Table 1 shows the sociodemographic factors in the present study. Except for age, marital status, and occupation, there were no significant differences between the three groups.
Sociodemographic Factors of the Study Population.
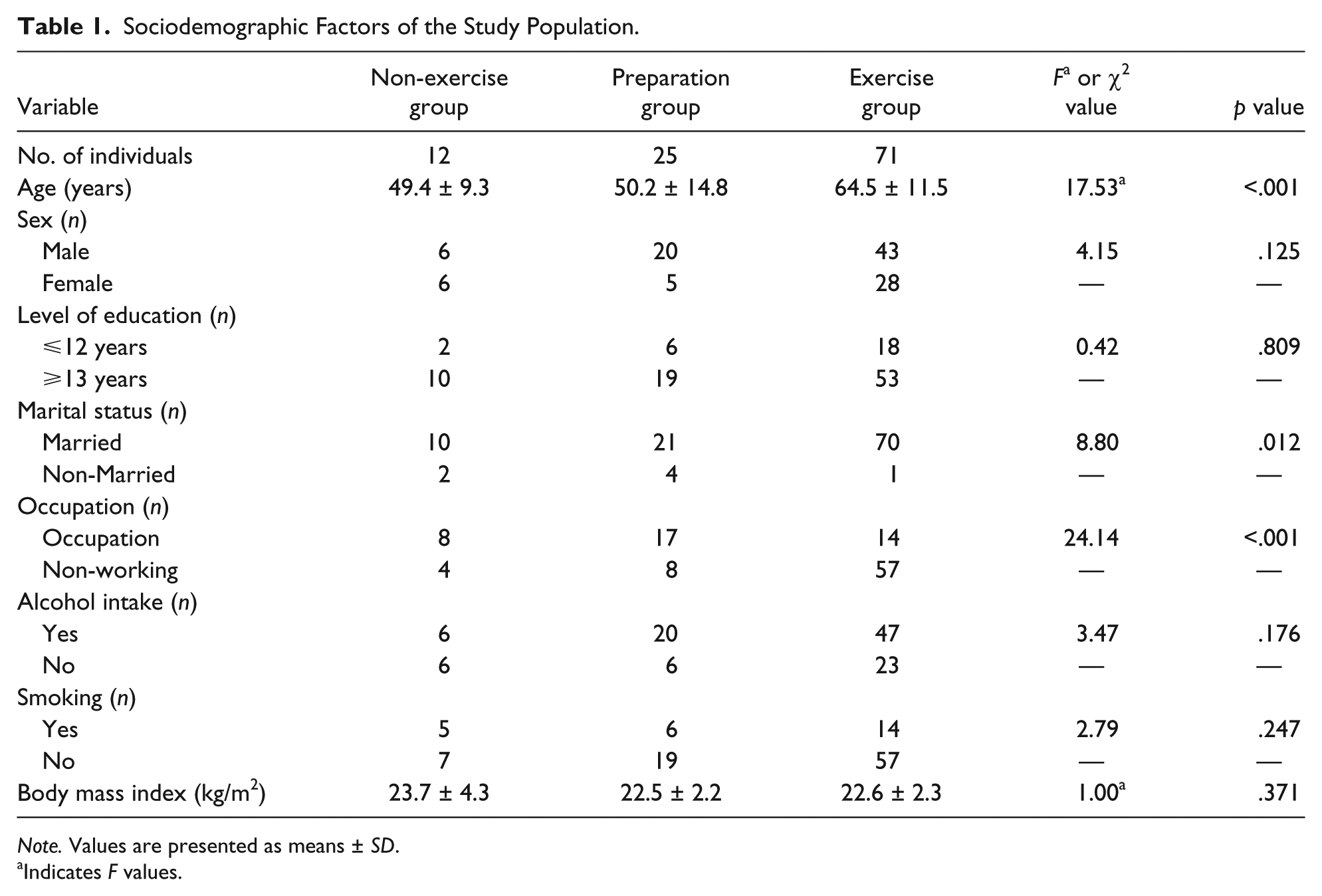
Note. Values are presented as means ± SD.
Indicates F values.
Table 2 shows the differences in workday, non-workday, and total-day sitting behavior times and MCS scores for HRQOL in the three exercise behavior groups. There were significant differences in all of these values in the three groups. Results of Tukey’s post hoc tests showed that workday, non-workday, and total-day sitting behavior times in the E group were lower, and the MCS for HRQOL was higher than that in the P group. Furthermore, the total-day sitting behavior time in the E group was lower than that of the NE group. In addition, MCS scores for HRQOL in the P group were higher than those in the NE group.
Differences in Sitting Behavior Time and HRQOL Based on Exercise Behavior.

Note. Values are presented as means ± SD. HRQOL = health-related quality of life; MCS = mental component summary.
Significant differences in the preparation group vs. exercise group (p < .05).
Significant differences in the non-exercise group vs. preparation group (p < .05).
Significant differences in the non-exercise group vs. exercise group (p < .05).
The differences in sociodemographic factors in the three groups as analyzed with ANCOVA are presented in Table 3. After adjustment for the sociodemographic factors, there were also differences in workday, non-workday, and total-day sitting behavior times per day and MCS scores based on the TTM. Non-workday and total-day sitting behavior times per day in the E group were lower, and the MCS scores for HRQOL were higher than those in the P group. The non-workday sitting behavior times in the E group were also lower than those in the NE group, and the MCS scores for HRQOL in the P group were higher than those in the NE group.
Sitting Behavior Time and HRQOL Adjusted by Sociodemographic Factors.

Note. Values are adjusted for age, occupation, and marital status. Values are presented as means ± SD. HRQOL = health-related quality of life; MCS = mental component summary.
Significant differences in the preparation group vs. exercise group (p<.05).
Significant differences in the non-exercise group vs. preparation group (p<.05).
Significant differences in the non-exercise group vs. exercise group (p<.05).
Discussion
The present study investigated differences in sitting behavior time and HRQOL based on the TTM of exercise behavior in Japanese living overseas in Malaysia. There were significant differences in age, marital status, and occupation in the three exercise groups. After adjustment for the sociodemographic factors (age, marital status, and occupation), there were differences in workday, non-workday, and total-day sitting behavior times and MCS scores for HRQOL based on the TTM.
It was previously reported in cross-national research on weekday sitting behavior time of adults in 20 countries that many Japanese citizens are sitting too much as their sitting behavior time is the longest in the world (median, 420 min/day) (Bauman et al., 2011). Our previous study also reported a total average sitting behavior time of 408.6 ± 190.1 min/day (Izawa & Oka, 2017). However, the present study found significant differences in the workday, non-workday, and total-day sitting behavior times per day as evaluated by the TTM of exercise behavior (Table 2). Therefore, sitting behavior time may differ in relation to exercise behavior.
Significant differences were found in age, marital status, and occupation in the three exercise groups in the present study, and after adjustment for these values, significant differences in sitting behavior times still remained between the groups, suggesting that these factors may be related to sitting behavior time based on exercise behavior. Particularly, as indicated by the P group results by TTM, the movement from preparation to action or maintenance may be very important in reducing the sitting behavior time of Japanese living overseas. There was a tendency for long sitting time during the workday compared with the non-workday in all three groups, especially in the NE and Exercise groups.
Evans et al. (2012) examined the intervention effect of combining the delivery by personal computer of a stimulus (point-of-choice prompt) that urges the interruption of sitting behavior every 30 min and health education on acceptability of the decapacitating behavior. They showed that stimulation was more effective in improving the frequency and duration of sitting behaviors over periods of time longer than 30 min during the workday proportion of the day.
Alkhajah et al. (2012) investigated the use of a workstation (Ergotron, Inc, Eagan, MN) that can allow a worker to easily switch between a working posture of sitting or standing according to their height and job purpose in adults aged 20 to 65 working in companies in Brisbane, Australia. As a result, sitting time in the workplace was 143 min/day, awake sitting time decreased by 97 min/day, the effect lasted for 3 months, and it contributed to the improvement of the subjects’ high-density lipoprotein cholesterol level. However, our research in the present study was not an intervention study, so we could not directly compare with these previous studies. Thus, we may need to consider reducing workday sitting time in workers by interventional and longitudinal study in the future.
Recently, several reports suggested that too much sitting time affects not only physical health but also mental health. Specifically, it relates to such factors as cognitive function, the risk of developing dementia, and HRQOL (Balboa-Castillo, León-Muñoz, Graciani, Rodríguez-Artalejo, & Guallar-Castillón, 2011; Kesse-Guyot et al., 2012; Verghese et al., 2003). In regard to HRQOL, Balboa-Castillo et al. (2011) examined the association between leisure action time per week and HRQOL in 1,097 elderly people (⩾62 years) living in Spain. They found that the length of time spent on leisure activity was significantly related not only to physical health as assessed by the SF-36 but also to low mental health–related factors such as vitality and social life function.
There were significant differences in exercise behavior by TTM adjusted for sociographic factors as well; particularly, these factors in the E group were significantly higher than those of both the NE and P groups. Particularly, the MCS score in the E group was higher than 50 points, indicating that it is over that of the Japanese norm.
Although the present study did not evaluate physical health in relation to HRQOL, the results of mental health in relation to HRQOL may support the findings of Balboa-Castillo et al. In other words, these results suggest that continuing exercise may shorten sitting time and thus contribute to the overall improvement of health.
Because this study is a cross-sectional study, we could not determine a causal relationship between the following two questions: Does continuing exercise reduce sitting time and improve HRQOL, or because HRQOL is high, is sitting time reduced, which leads to the continuation of exercise? The phenomenon may be bidirectional. For this reason, further investigation is needed on the causal relationships in the future.
A recent longitudinal cohort study suggested that stroke survivors were highly sedentary and remained so a year after stroke independent of their functional ability (Tieges et al., 2015). Another recent Japanese collaborative cohort study also suggested that prolonged television watching is a substantial risk factor for mortality from pulmonary embolism (Shirakawa et al., 2016). Therefore, future long-term follow-up in larger populations will be required to evaluate the potential time-related benefits of reducing sitting behavior time.
Study Limitations
Limitations of the present study include its cross-sectional study design and small number of all participants and small group size who completed the self-reported questionnaire. Moreover, there are three patterns of sitting behavior time, those for the workday, non-workday, and the entire day, and the details of sitting behavior time in each life scenario are not clear. Furthermore, this study was carried out in only one city by random sampling, and the questionnaire used was self-administered. Thus, there are also possibilities for recall bias and inaccurate presumption.
In the present study, there were no differences between the sitting behavior time and the MCS score between the NE group and the P group. In addition, there was also no difference in sitting behavior time between the NE group and the E group, respectively. However, we did not investigate these reasons in the present study, so we need to evaluate these in the future study.
Nevertheless, the values for sitting behavior time and HRQOL that were determined may be important in future research and may also represent appropriate workday, non-workday, and total-day sitting behavior time targets for stimulating exercise behavior to improve the HRQOL of Japanese living overseas. These deficiencies should be addressed in subsequent longitudinal studies.
Conclusion
This cross-sectional study showed differences in workday, non-workday, and total sitting behavior times and MCS scores for HRQOL adjusted for sociodemographic factors based on the TTM of exercise behavior. The findings may further reinforce the established importance of sitting behavior time and HRQOL based on exercise behavior, particularly in the “P” group in Japanese living overseas. In addition, we need to consider strategies for stimulating exercise behavior, including sociodemographic factors such as occupation (type and style, etc., of work). The present study results may also be useful for clinicians or community-based health care workers as targets to reduce workday, non-workday, and total sitting behavior times on the basis of exercise behavior.
Footnotes
Acknowledgements
The present study was supported by the participants and the Japanese Association (Mr. Kosuke Tamura) in Ipoh, Perak, Malaysia. We also appreciate the support and encouragement of Mr. Keiichi Izawa (Rien Co., LTD., Iwamizawa, Hokkaido) and Mr. Satoshi Watanabe (St. Marianna University School of Medicine Hospital, Kawasaki, Kanagawa). We express our gratitude to everyone involved in helping with our research.
Compliance With Ethical Standards
Participants received explanations of the research procedures from the researchers.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by a Grant-in-Aid for Scientific research from the Japanese Association for the Promotion of Rehabilitation (Koganei, Tokyo, Japan). Oka is supported by the MEXT-Supported Program for the Strategic Research Foundation at Private Universities, 2015–2019 the Japan Ministry of Education, Culture, Sports, Science and Technology (S1511017).