
Abstract
Keywords
Introduction
Population aging is a global phenomenon affecting both developed and developing countries. Colombia, with its more than 45 million inhabitants, currently faces a rapid demographic transformation, with the proportion of people more than 60 years old expected to increase from 10% to 20% in 2050 (Departamento Administrativo Nacional de Estadística, 2017). This demographic shift can be explained by better living standards and improvements in both preventive and curative health care. Simultaneously, the main causes of death have shifted from infectious diseases toward age-related chronic diseases (Gomez & Curcio, 2016).
World Health Organization (WHO), in its report on aging and health (WHO, 2015), emphasized the need for a paradigm shift in the health of older adults, insisting that diseases do not have a preponderant impact on the lives of older people (Young, Frick, & Phelan, 2009), and proposing to shift from the epidemiologic approach, based on multimorbidity and exclusively on medical diagnoses toward a focus on the functioning of elders in their environment (WHO, 2015). This paradigm shift has been influenced, among other things, by the concern on aging well and achieving successful aging (SA); Petretto, Pili, Gaviano, & Pili, 2017). With the progression of global aging, the shift toward a positive discourse about aging, including healthy, successful, or active aging, has been encouraged and has become more evident.
Despite a lack of agreement, one particular conceptualization of SA has dominated the scientific discourse in this area. According to the criteria of Rowe and Kahn (1987, 1997), SA includes remaining free of disease, disability, and risk factors for disease; retaining high physical and cognitive functioning; and remaining actively engaged. This definition has been heavily critiqued (Holstein & Minkler, 2003; Katz & Calasanti, 2015; Martinson & Berridge, 2015; Rubinstein & de Medeiros, 2015; Stowe & Cooney, 2015). Thousands of reports have been written on the concept and its components, and more than 100 variations of the original model have been proposed (Rowe & Kahn, 2015).
The prevalence of SA is highly variable. In elderly Europeans, a prevalence of 8.5% has been reported, ranging from 1.6% in Poland and 3.1% in Spain to 21.1% in Denmark (Hank, 2011); the prevalence is 10.9% in the United States (Kaplan, Strawbridge, Camacho, & Cohen, 1993) and 10% in Taiwan (Li et al., 2014). Given the differences in the concept and its operationalization, Depp and Jeste (2006), in an extensive review of SA studies, both cross sectional and longitudinal, found that when functionality was used as a criterion, the prevalence was 27.2%; however, when cognitive and physical competences were included, the prevalence ranged from 3% to 95%. Fernandez-Ballesteros et al. (2010) analyzed separate and combined indicators of SA and found that the prevalence ranged from 15.5% to 41.4%, depending on the simple or multidimensional definitions used.
Absence of diseases has been identified as the most exigent criterion for establishing SA (Martinson & Berridge, 2015). Some studies have concluded that SA may be possible even for those with chronic diseases (Young, Frick, & Phelan, 2009) and disabling illness (Young et al., 2009). Kok, Aartsen, Deeg, and Huisman (2015) conclude that omitting this factor from SA model results in definitions that are less heavily biased toward biomedical functioning.
Findings on the role of gender in SA are also controversial. Several studies found no gender differences in SA (McLaughlin, Connell, Heeringa, Li, & Roberts, 2010; Strawbridge, Wallhagen, & Cohen, 2002). In contrast, Strawbridge et al. (2002) found that a substantially higher percentage of women than men met the Rowe and Kahn’s definition, whereas a Chinese study found that men were more likely to be successful agers.
Being married (Arias-Merino, Mendoza-Ruvalcaba, Arias-Merino, Cueva-Contreras, & Vazquez Arias, 2012; Meng & D’Arcy, 2013; Nosraty, Sarkeala, Hervonen, & Jylhä, 2012) was associated with SA. Income had a protective effect on SA (Chaves, Camozzato, Eizirik, & Kaye, 2009; McLaughlin et al., 2010). These findings contrast with the results for developed countries, where income has not been observed as an important predictor of SA (Meng & D’Arcy, 2013). The role of education as a factor related to SA is also controversial. Depp and Jeste (2006) found no differences according to educational level; thus, the educational level is an independent predictor of SA in other studies (Arias-Merino et al., 2012; McLaughlin et al., 2010; Pruchno, Wilson-Genderson, Rose, & Cartwright, 2010).
SA occurs when an individual uses adaptive mechanisms and spiritual resources to compensate for physical limitations and environmental challenges (Young et al., 2009). In qualitative studies, older adults consistently mention financial security and spirituality when asked to explain what SA means to them (Hilton, Gonzalez, Saleh, Maitoza, & Anngela-Cole, 2012).
There are few studies about SA in Latin America. A research in western Mexico, which used data from the SABE (abreviated from Spanish name as: SABE = Salud, Bienestar y Envejecimiento) study and applied the Rowe and Khan model as basis, reported an SA prevalence of 12.6%, with the proportion decreasing with increasing age. Another study in Brazil, which specified healthy and independent elderly in the inclusion criteria, found a prevalence of 62% (Arias-Merino et al., 2012).
In Colombia, a study carried out among peasant elders reported that they were sick, disabled, poor, without a pension, and with a low level of education (Gómez, Curcio, Orjuela, & Ramírez, 1998). Given these conditions, the authors asked the following: Can we talk about SA in Colombian rural elderly people? (Gomez & Curcio, 2000).
An analysis focused on a new health paradigm (functional ability) and a multidimensional approach to SA should be the starting point for policies and interventions that promote well-being. Knowledge of the indicators, prevalence, and factors associated with SA has important implications in determining the best approach to promote it in the aging population.
By using data from a prospective longitudinal study of adults more than 65 years old in Manizales, this study aimed to estimate the prevalence of SA in a cohort of older people in the Colombian Andes Mountain, and to identify the most important indicators related to SA that should be considered in primary health care toward establishing strategies that would keep the elderly highly functional for as long as possible.
An assessment of the national prevalence of SA will be a constructive addition to the literature. First, it is important to observe the prevalence of SA in developing countries with more recent and well-measured population-based data. Such information will provide a general profile of SA in the Colombian Andes Mountain population. Second, a detailed examination of SA by using the modified model of Rowe and Kahn may provide a basis for redefining the concept and suggesting appropriate changes in individual criteria for SA in less developed countries.
Method
Study Design
This is a cross-sectional, descriptive, and correlational study.
Participants
This research was carried out as part of a longitudinal International Mobility in Aging Study (IMIAS; Zunzunegui et al., 2015). Baseline data collected in Manizales (Colombia) in 2012 were used. The sample was stratified by sex and included 200 men and 200 women. The participants were randomly selected from the population in the city. The inclusion criteria were (a) between 65 and 74 years old, (b) without severe cognitive impairment (fewer than four errors in the orientation section of the Leganes cognitive test; de Yébenes et al., 2003), and (c) able to walk without the help of another person, either with or without the use of an assistive device. Among the 400 participants, 311 answered the questionnaires and had complete data in all the considered covariates and, thus, were included in the analysis.
Measures
Successful aging
Based on the conceptualization of SA by Rowe and Kahn and subsequent studies, SA in the current work encompassed indicators in four domains: physical, cognitive, emotional, and social functioning. Participants who met the criteria in all four indicators were categorized under “SA.” The single indicator of SA was operationalized as follows.
High physical functioning
Two indicators were used: the Short Physical Performance Battery (SPPB) with scores ranging from 0 to 12 (Gómez, Curcio, Alvarado, Zunzunegui, & Guralnik, 2013), in which participants with a score >10 were considered to have high physical functioning (da Camara, Alvarado, Guralnik, Guerra, & Maciel, 2013); and absence of disability, measured as nondifficulty in performing each of the six basic activities of daily living (ADLs; i.e., walking across a room, dressing, bathing or showering, eating, getting in or out of bed, and toileting; Nagi, 1976). Respondents with appropriate physical functioning based on both indicators were considered to have met the first criterion for SA.
High cognitive functioning
Cognitive impairment was measured by using the Mini-Mental State Examination (MMSE) (Tombaugh & McIntyre, 1992). The MMSE score was calculated by using the sum of correct answers (0-30 points) and dichotomized. The cutoff point was 24 (Kochhann, Varela, Lisboa, & Chaves, 2010).
High emotional functioning
The Center for Epidemiologic Studies–Depression (CES-D) scale was applied. This is a screening tool consisting of 20 items related to depressive symptoms. Scores range from 0 to 60, with scores ⩾16 indicating high probability of being depressed (Radloff, 1977). High emotional functioning was defined as absence of depression.
High social functioning
The IMIAS-SNSS (IMIAS Social Networks and Social Support) instrument, which measured both the social networks and the emotional support provided by different types of social ties, was used. These items consist of information on four types of ties: friends, children, extended family, and partner. The support includes feeling loved and listened to, self-perceived usefulness, and satisfaction (Ahmed et al., 2018). Higher scores indicated SA.
Independent variables
Age, gender, education, marital status, profession, income, satisfaction with income, living arrangements, chronic conditions, self-rated health, and spirituality were included in the analysis. Age was categorized as 60 to 74 years and 75 years or older. Education was classified as elementary school/illiterate, high school, and above high school. Marital status options included single, married, widow, and divorced or separated. Living arrangement (range = 0-9) was dichotomized into living alone versus living with one or more persons. Occupation was categorized into manual and nonmanual. Income level was grouped into a set of two variables indicating the extreme poverty line (less than US$1 daily) or the level above it as the reference category (Curcio, Henao, & Gomez, 2014). Sufficiency of income was self-reported as the answer to the following question: To what extent is your income sufficient to make ends meet? Possible responses were very sufficient, sufficient, and insufficient (Grundy & Holt, 2001).
Chronic conditions
The participants in the IMIAS were asked whether a doctor or a nurse has ever told them that they have any of the following chronic diseases: cancer, chronic lung disease, diabetes, hypertension, osteoarthrosis/arthritis, osteoporosis, heart disease, and stroke. Respondents who reported having any of these diseases were classified as having a chronic disease.
Self-rated health
The participants were asked, “Would you rate your health as very good, good, fair, poor, or very poor?” Self-rated health was classified as good if the respondents answered “very good” or “good” and as poor if the respondents answered “fair,” “poor,” and “very poor” (Pérez-Zepeda et al., 2016).
To assess spirituality, we used one item (spiritual connection) from the Brief Multidimensional Measure of Religiosity/Spirituality (John E. Fetzer Institute, 2003): “I think about how my life as part of a larger spiritual force.” The answers were set on a 4-point scale (1 = a great deal, 2 = quite a bit, 3 = somewhat, and 4 = not at all) and categorized into high and low for the analysis.
Statistical Analysis
The characteristics of the participants were described by using the means and standard deviations (SDs) for continuous variables and the frequencies and percentages for categorical variables. Comparison of categorical variables were determined using chi-square tests, and comparison of continuous variables were analyzed with two-tailed independent t tests.
The prevalence of SA was calculated by applying the SA index constructed with the use of previously defined criteria. To identify the factors associated with SA, variables were selected based on the strength of the associations. The odds ratio (OR) and 95% confidence intervals (CIs) were calculated; p ⩽ .05 were considered statistically significant. The Hosmer–Lemeshow test was used for testing the goodness of fit. Statistical analyses were conducted using SPSS version 23.0 statistical package (SPSS Inc., Chicago, IL, USA).
Results
Characteristics of the Population
Table 1 shows the participant characteristics according to sex. The mean age of the sample was 69.1 years (SD = 2.8 years). According to the inclusion criteria, 51.7% were women. The mean level of education was 5.8 years; 82.6% had attended lower than primary school. The level of education was low in both sexes but lower in women than in men. Among the men, 70.7% were married; 41.6% of the women were widows (p < .000). These gender differences are also statistically significant in single marital status.
Participant Characteristics by Sex.

MMW = Montly Minimun Wage: US$250.
Poor = none or less than 1 MMW, medium = 1 MMW, medium high and high = 2 or more MMW.
The majority of the population (82%) had a manual occupation; 23.5% had no income, and 50.5% had a poor-level income. A greater proportion of women had no income, those who did had a lower income compared with their male counterparts. Regarding living arrangement, 87.4% lived with their partners and other people. Optimal self-rated health was reported by 52.7% of the sample; the self-rated health was better in men that in women, without statistically significant differences. Of the sample, 85.3% considered themselves as very spiritual, with differences between sexes (p = .001).
The percentage of respondents who reported having no chronic conditions was 23.2%, with the proportion being slightly higher in men (p = .002). The most prevalent chronic conditions were hypertension (56.9%), osteoarthritis (28.4%; differences between sexes, p = .000), and heart problems (18%).
Successful Aging
The percentage of participants who met the criteria for SA was calculated. Table 2 shows the percentage of respondents who met each SA criterion as well as all the criteria. A higher proportion of the sample met the criteria of high cognitive functioning (90.7%) and absence of disability (73.3%); 87.8% of the sample also met the criterion of social engagement. In total, 24.4% of the participants met all the criteria for SA, without differences between sexes. In general, women showed higher physical and cognitive functioning and social engagement.
Percentage of Older Adults Who Meet Each SA Criterion and All the Criteria.

Note. SA = Successful Aging; SPPB = Short Physical Performance Battery; CES-D = Center for Epidemiologic Studies–Depression. MMSE= Mini-Mental State Examination
Table 3 shows the percentage of the elderly population who accomplished each marker of SA. The variables found to be associated with SA in the bivariate analysis were sex (p = .003), educational level (p = .005), marital status (p = .001), income level (p = 0.001), self-rated health (p = .000), spirituality (p = .000), number of chronic diseases (p = .001), and absence of chronic conditions (p = .008).
Percentage of Participants Who Satisfy the Indicators of SA by Sociodemographic Characteristics.
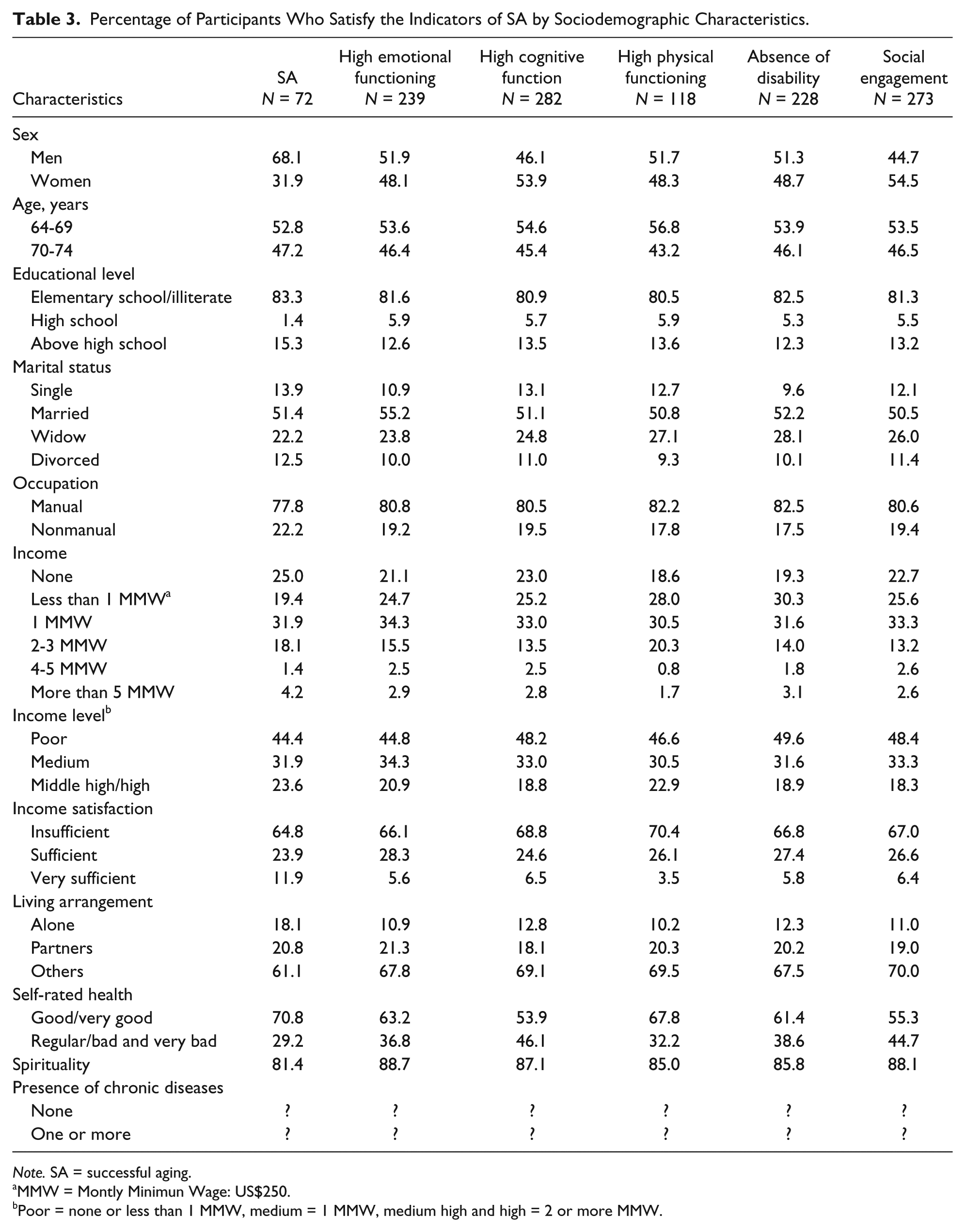
Note. SA = successful aging.
MMW = Montly Minimun Wage: US$250.
Poor = none or less than 1 MMW, medium = 1 MMW, medium high and high = 2 or more MMW.
The factors predictive of SA were good and very good self-rated health, middle–high/high income level, absence of chronic conditions, married status, high educational level, high and very high spirituality, and female sex. The model explained 75.6% of the variance (Table 4).
Multivariate Logistic Regression Model of SA.
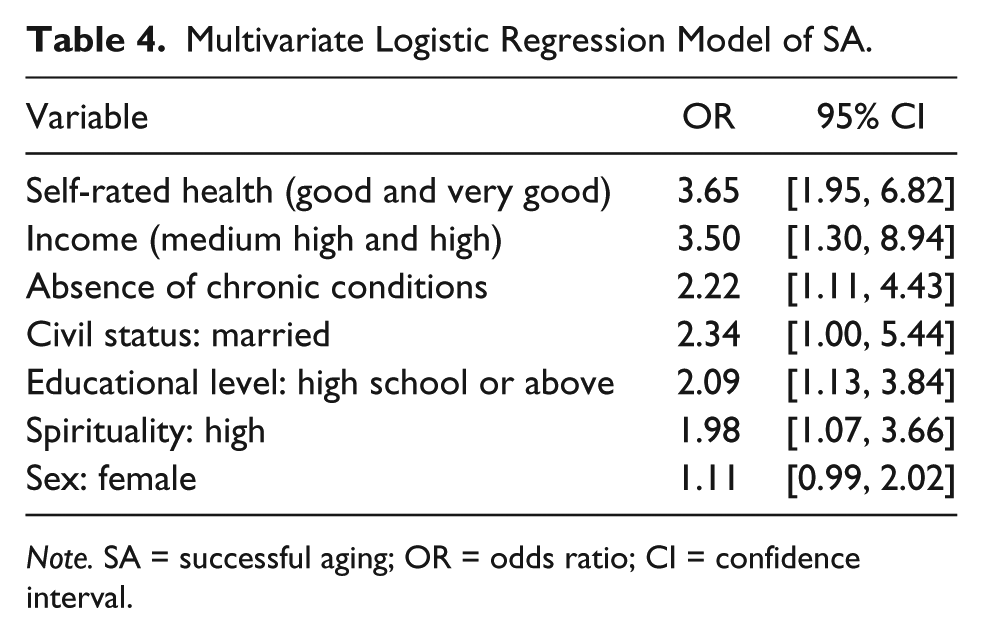
Note. SA = successful aging; OR = odds ratio; CI = confidence interval.
Discussion
The prevalence of SA among older people of the Andes Mountains in Colombia was assessed. The results showed that the prevalence of SA in people 65 to 75 years old was 24.4%. The following independent predictors were established: good and very good self-rated health, middle–high/high income level, absence of chronic conditions, married status, high educational level, and high spiritual level.
The findings on SA prevalence are similar to those reported in other studies (Depp & Jeste, 2006; Peel, McClure, & Bartlett, 2005), although there may be differences due to the SA criteria and measurement instruments used. Other studies that were based on the criteria of Rowe and Kahn found 12.6% (Arias-Merino et al., 2012) and 13.2% (Li et al., 2014) of prevalence of SA.
The factors found to be associated with SA were age, sex, education, and marital status in the Mexican study (Arias-Merino et al., 2012), and education and occupation in the Chinese research (Li et al., 2014). This reinforces the importance of sociodemographic factors in SA, as indicated in the present results. In a longitudinal study (Fernandez- Ballesteros, Zamarrón et al., 2010), separate and combined indicators were analyzed, and the prevalence ranged from 15.5% to 41.1%, depending on whether simple or multidimensional definitions were used.
The differences in the prevalence of SA between respondents with and without chronic conditions might be attributed to the large number of comorbidities. In the Colombian SABE study, 85.1% of older people reported having more than one chronic condition (multimorbidity); Ministerio de Salud y Protección Social, COLCIENCIAS, Universidad del Valle, Universidad de Caldas, 2016). Absence of diseases has been identified as the most exigent criterion for establishing SA (Martinson & Berridge, 2015). Moreover, it has been pointed out that the model of Rowe and Kahn might be designed for developed countries and high-income populations and, therefore, might not be applicable to medium- and low-income groups (Strong, Mathers, Leeder, & Beaglehole, 2005). Furthermore, if absence of chronic diseases is a key feature in the Rowe and Kahn model, then such a model is almost impossible to achieve in adverse socioeconomic conditions, which predominate in low- and medium-income populations, such as in Colombia (Strong et al., 2005). Finally, some studies have concluded that SA can coexist with diseases and functional limitations if compensatory mechanisms are used (Young et al., 2009).
The concept of self-rated health has been widely accepted as a sensitive and confident measurement of general health status (Idler, Kasl, & Lemke, 1990; Kaplan, Barell, & Lusky, 1988; Lee, 2000). It is influenced by physical function, presence of diseases, existence of disabilities and functional limitations, and cognitive function (Idler et al., 1990; Kaplan et al., 1993; Martin, Palmer, Rock, Gelston, & Jeste, 2015; Tamayo-Fonseca et al., 2013). Many researchers have suggested that other aspects, such as social support and religiosity, also affect self-rated health (Caetano, Silva, & Vettore, 2013; Jervelund et al., 2017; Peterson & Martin, 2015; Ponce, Rosas, & Lorca, 2014). Thus, the existence of a relationship between SA and self-rated health is not surprising. In this study, about half of the sample rated their health as good or very good; a similar ratio has been reported in other works (Kaplan et al., 1988; Tamayo-Fonseca et al., 2013). There are few studies about self-rated health in older people in Colombia. Gómez, Curcio, and Matijasevic (2004) showed that half of the community-dwelling older population in Manizales considered themselves healthy. Another study in Cali (Colombia) showed that 60% of the sample reported good self-rated health; after 1 year of follow-up, older people with bad self-rated health were found to have greater health problems, incidence of geriatric syndromes, and more frequent health service attendance (Ocampo-Chaparro et al., 2013). The Colombian SABE survey (Ministerio de Salud y Protección Social, COLCIENCIAS, Universidad del Valle, Universidad de Caldas, 2016) reported a similar proportion of respondents (51.3%) with very good and good self-rated health. Most were of high socioeconomic status, came from urban areas, and had high educational level.
Consistent with prior research (Arias-Merino et al., 2012; Nosraty et al., 2012), this study shows that marital status is an independent predictor of SA. This finding reinforces the protective role of marriage in older people’s health. Several explanations have been proposed for this result, such as that marriage provides social and economic support, the selection of the healthiest individuals who might marry or remain married, and better behaviors and health habits among married people (Arias-Merino et al., 2012).
The importance of religiosity in Colombian older people has been previously reported. A study carried out in Cali showed that 97.8% of respondents had some type of religion and that 93% prayed at least once daily (Ocampo, Romero, Saa, Herrera, & Reyes-Ortiz, 2006). Older people who engage in religious activities have been found to have better physical and mental health and to live longer than those without religious activities (Koenig et al., 1999). Different mechanisms of how religion may positively influence health have been proposed, such as that people who have more religious activities have better social support networks, better adherence to medical treatments, and lower depression, anxiety, and stress rates (Ocampo et al., 2006).
A multicentric study on religiosity and spirituality in older women in the United States (Vahia et al., 2011), which aimed to assess spirituality and its association with SA, specifically with high cognitive and functional performance, concluded that spirituality was associated with a specific demographic profile: lower educational level, lower income, and lower likelihood of being married or engaged. Also numerous studies have reported an association between spirituality and several positive health outcomes, including longevity (Glass et al., 1999); lower mortality (because of better health practices; Strawbridge, Shema, Cohen, & Kaplan, 2001); better adaptability to, and faster recovery from, chronic illnesses (Koenig, George, & Peterson, 1998; Koenig et al., 1999); higher self-esteem (Murray-Swank et al., 2006); lower depression rate (Maselko, Gilman, & Buka, 2009; Murray-Swank et al., 2006; Reyes-Ortiz Gilman, & Buka, 2008); lower alcohol and tobacco abuse (Edlund et al., 2010); better life quality; and higher cognitive performance (Hill, Burdette, Angel, & Angel, 2006; Reyes-Ortiz et al., 2008).
Education is well recognized to have an impact on health and lifestyle and to reflect socioeconomic status. In this study, high educational level was found to predict SA. The role of education as a factor related to SA is controverted. Most of the studies assessed by Depp and Jeste (e.g., Depp & Jeste, 2006) found no differences according to educational level, whereas other works, including the present research, found a higher prevalence of SA in people with high education and high income; thus, educational level is an independent predictor of SA (Arias-Merino et al., 2014; Li et al., 2012; McLaughlin et al., 2010; Pruchno et al., 2010). Education may be considered as a mediator of SA through several pathways: better cognitive function, better occupational opportunities, and better income with increasing educational level. There is evidence indicating that low educational level is a risk factor for cognitive impairment related to aging (Alvarado, Zunzunegui, Del Ser, & Béland, 2002); it is also related to adverse socioeconomic conditions, low brain reserve or occupational activities with minimal demands, and low cognitive stimuli (Gõmez, Zunzunegui, Lord, Alvarado, & García, 2013). This is evidenced in the present study by the low educational levels and main occupational activities of the participants: housewives and farmers. Li et al. (2014) showed that the prevalence of SA was higher in people with nonagricultural occupations than in farmers; the differences might be related to inequity in access to basic public services, especially education.
Education has been further recognized to have a mediator effect on life quality and income. Thus, differences in education during the life course increase the gaps in the elderly and increase the risk of having lower life quality. In particular, a higher educational level has been reported to strengthen the association between higher income and less disability, suggesting that people with higher educational levels have more economic benefits (Abellán, Rodríguez-Laso, Pujol, & Barrios, 2015). A study in Brazil (Chaves et al., 2009) showed that income has a protective role in SA. The authors postulated a contrast between their findings and those in developed countries, in which income does not play a predictive role, concluding that in developing countries, income becomes an inequity marker and, therefore, may be a determinant of SA.
Regarding sex, some studies have shown inconsistent patterns between men and women. However, the results seem to be dependent on the model applied (Teixeira & Neri, 2008). For example, McLaughlin et al. (2010) found no gender differences in SA prevalence but reported a higher probability of SA in women after controlling for sociodemographic variables. The present work found a marginal result. On one hand, the ratio of women with SA was lower than that of men, although this difference was not significant in the regression model. This finding may be explained, first, by the similar ratio of women and men in the present study, which is very uncommon: The ratio of women is usually higher (2 to 1). On the other hand, men have a higher disease rate, less depression, higher level of physical function, and less ADL dependence than women; thus, it is necessary to establish whether the criteria and indicators are different for men and women.
Despite the numerous criticisms on SA, several contributions have been recognized, especially those focused on the positive aspects of aging. An assessment in other groups of older people and in different contexts in Colombia is necessary to prove the applicability of the present findings in other populations. Longitudinal studies are also needed to identify synergisms between the domains and how they can contribute to each other, with the purpose of creating an index applicable in primary care services that would help in identifying predictive factors of SA in older people and promoting strategies to ensure high functionality levels for as long as possible.
This study has several strengths, including being the first to establish the prevalence and determinants of SA in Colombian elderly. The identification of factors related to SA leads to the establishment of a profile of community-dwelling older people that includes being healthy; having high mental, emotional, and physical functioning; and being decidedly engaged in life through stable interpersonal relationships and participation in meaningful activities. Furthermore, based on the construction of SA indicators and a differentiated analysis including/excluding the presence of diseases, the impact on SA was determined. Disease is one of the domains that is almost unrestrictedly present as a criterion for defining SA; however, it is included as an independent variable, leading to confusion between the defining criterion of SA and its determinants, which, according to Fernandez-Ballesteros et al. (2004), is equivalent to confusing the explained with the explanation. The randomization of the sample is another strength of the present work, making it possible to generalize the results to the entire population.
One of the limitations of this study is its transversal design, which does not allow establishing cause–effect relationships between the variables. Another limitation is the participants’ age range of 65 to 74 years, which could mean that the results might not be generalizable to individuals older than 75 years or to institutionalized frail elders.
Conclusion
The prevalence of Successful Aging in Colombian elderly is low: One out of 10 people older than 65 years shows SA when presence of diseases is included in the criteria, compared with one out of four people when such an item is excluded, that is, in elderly who have high functionality levels and are socially engaged. The identification of predictive factors allows distinguishing this population in primary care services and promoting strategies to ensure high functionality levels for as long as possible.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Canadian Institutes of Health Research Institute of Aging, New Emerging Team, gender differences in immobility (grant no. AAM 108751), and The Vicerrectoria de Investigaciones y Posgrados, Universidad de Caldas (grant no. 0391816). The funding sources had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; the preparation, review, or approval of the article; and the decision to submit the article for publication.