
Abstract
Introduction
In the United States, cancer screenings and cancer are common health concerns; cancer is the second leading cause of death (Centers for Disease Control and Prevention [CDC], 2016), and screenings aid in early detection and treatment of cancer to prevent cancer-related mortality (“Cancer Screening Overview [PDQ]–Health Professional Version,” 2016). Older adults face higher cancer incidence and death rates (Berger et al., 2006), and older women, in particular, are at high risk for breast cancer, uterine cancer, ovarian cancer, and cervical cancer (CDC, 2016). However, there are health disparities in cancer and cancer screening behaviors among older minority women (Peek & Han, 2004; “Study Finds Racial and Ethnic Disparities in US Cancer Screening Rates,” 2012), particularly U.S. Chinese older women. First, evidence suggests that cancer screening rates are low for Chinese women (E. S. Chang, Simon, & Dong, 2016) and lowest among older Chinese women above 70 (B. Wang et al., 2013). Researchers have postulated that these low rates may be due to socioeconomic, linguistic, and cultural reasons, such as language barriers, lack of access to services, and traditional beliefs regarding cancer screenings and Eastern medicine practices (J. H. Wang et al., 2009). Second, as among older women in general, cancer is common among Chinese women (Y.-C. Wang, Wei, Liu, Li, & Wang, 2012). Often times, Chinese women with cancer choose to use traditional practices of medicine either in conjunction with or instead of biomedical treatment options (Tsai, Lai, Wu, & Lin, 2014; J. Wang et al., 2014).
Traditional Chinese Medicine (TCM) has been practiced for thousands of years among Chinese women, yet its current application toward health conditions in the United States is poorly understood. TCM, which includes herbal medication, acupuncture, massage therapy, and tai chi, is frequently used as forms of treatment or to maintain health. Among older Chinese adults in the United States, many are foreign-born with low acculturation levels (Dong, Bergren, & Chang, 2015a) and face language and financial barriers that may contribute to their health care choices (L. Chang & Basnyat, 2015; Dong & Bergren, 2016; Dong et al., 2010; Ma, 1999). Within this population, older Chinese women value the applications of TCM (Xu, Towers, Li, & Collet, 2006) and are more likely to use TCM compared with their male counterparts (Dong, Bergren, & Chang 2015b). This suggests that TCM is an especially relevant modality of health practices among older Chinese women in the United States.
Cancer screening, cancers, and TCM are important facets of health for Chinese older women; relationships between them have been found in China and other countries. Existing literature suggests that Chinese women maintain their health and prevent asymptomatic cancers with their own means of TCM use, instead of getting cancer screening (S. C. H. Chang, Woo, Yau, Gorzalka, & Brotto, 2013; Kwok & Sullivan, 2006). Low cancer screening rates may be a result of cultural beliefs toward health, preference for TCM, perceived barriers, lack of health knowledge, and stigma (S. C. H. Chang et al., 2013; H.-Y. Chen, Kessler, Mori, & Chauhan, 2012; Kwok & Sullivan, 2006; J. H. Wang et al., 2009). In addition, evidence suggests that Chinese older women with cancer commonly use TCM (Z. Chen et al., 2008), most likely also due to cultural beliefs and evidence toward its efficacy (Chu et al., 2013; Fan et al., 2014; Yang, Hu, & Liu, 2013). TCM use, especially in conjunction with Western medicine, may be of particular concern as interactions can lead to unintended side effects (“Traditional Chinese Medicine: In Depth,” 2013). However, there is a paucity of community-level data in the United States regarding relationships between cancer screening, cancer, and TCM use among U.S. Chinese older women. Understanding cancer screening and cancer trends with traditional medicine may be helpful in enhancing patient-centered care for this population. To understand and address low cancer screening rates and health practices related to cancer among Chinese women, examining TCM use and its relevance may promote culturally relevant patient-centered care.
Chinese older women in the United States belong to the largest and oldest subgroup of Asians in the United States (Dong, 2014), however, public health efforts for this population remain scarce. This population is growing and aging rapidly (Dong, 2014), which prompts a need to better understand their health outcomes and practices, such as the use of TCM. A comprehensive understanding of screening behaviors, cancer prevalence, and TCM use among U.S. Chinese women may aid in devising interventions to increase cancer screening rates and deliver efficient, culturally appropriate health care. To better understand cancer and cancer screenings’ connection with TCM use among older Chinese women in the United States, this study aims to (a) study sociodemographic associations with TCM use, (b) observe cancer screening and self-reported cancer rates as well as the frequency and type of TCM use within this population, and (c) examine potential associations between those with women’s cancers and TCM use as well as cancer screenings and TCM use.
Method
Population and Settings
The Population Study of Chinese Elderly in Chicago (PINE) is an epidemiological study of U.S. Chinese older adults in the Chicago metropolitan area. Under the supervision of Rush Institute for Health Aging and in collaboration with Northwestern University and other community organizations, 3,157 Chinese older adults (60+ years old) were collected for the study. For this particular study, men were excluded from our sample. This allowed for a sample size of 1,830 women. Trained bilingual research assistants interviewed participants about their health and well-being in Chinese or English while responses were recorded in both languages. This study is approved by the Institutional Review Boards of Rush University Medical Center. (Dong, Wong, & Simon, 2014)
Measurements
Sociodemographics
The interview included basic demographic questions concerning the participants. These questions included age (in years), sex, education level (in years), annual income level, marital status, number of children, household composition (number of people at home), number of years in the neighborhood in which they reside, number of years in the United States, language preference, and country of origin (China, Hong Kong/Macau, Taiwan, or other).
Cancer screening and cancer
Cancer screening, specifically breast and cervical cancer screening, was included to study its impact on TCM usage. Participants were asked if they have ever received a mammography test and if they have had a pap smear test. Responses were coded dichotomously as 0 (no) or 1 (yes). To study the association between U.S. Chinese older women with self-reported cancer and TCM use, participants were asked to identify presence of cancer(s) that were uniquely coded numerically. Only women’s cancers were included in this study (breast, uterine, ovarian, and cervical cancer).
TCM use
TCM use was assessed by asking participants the frequency with which they use TCM if they used any at all in the past year. Questions specified the type of TCM, which included herbal, acupuncture, massage therapy, tai chi, and other forms of TCM. Responses were given on a 5-point scale and coded as 0 = no use, 1 = once in the previous year, 2 = once a month, 3 = once a week, and 4 = once a day.
Data Analysis
After calculating the prevalence of each cancer and TCM use, values generated from the chi-square tests were used to compare women’s cancers and cancer screening methods with different TCM modalities. TCM responses were then recoded coded as 0 (no use) or 1 (TCM use at any rate in the past year). To observe the associations between cancers/screenings and the varying modalities of TCM use, multivariate linear regression models were used to control for possible confounding variables. The model used for analysis adjusted for education, income, marital status, number of children, number of years in the United States, years in a neighborhood, and living situation. Rate ratios (RRs), 95% confidence intervals (CIs), and significance levels were used for multivariate analyses. These analyses were conducted using SAS, Version 9.2 (SAS Institute Inc., Cary, NC).
Results
Sociodemographic Characteristics of Sample According to TCM Use
Altogether, 79% of the sample reported TCM use. Within this sample, herbal remedies were used the most, and tai chi was practiced the least (62.6% vs. 12.9%, respectively). TCM use varied between sociodemographic groups, as shown in Table 1. Herbal TCM users were less likely to have had a higher level of education versus lower level of education (p < .001). Massage therapy users were more likely to have been older than younger (p < .001) and more likely to not be married versus married (p < .001). Tai chi users were more likely to have higher levels of education than lower levels of education (p < .001). Finally, users of other forms of TCM were more likely to have lived in their neighborhoods for less time than more time (p < .01).
Sociodemographic Characteristics of PINE Study Participants According to TCM Use.

Note. p values are based on χ2 statistics. PINE = Population Study of Chinese Elderly in Chicago; TCM = Traditional Chinese Medicine.
p < .05. **p < .01. ***p < .001.
Frequencies of Cancers According to TCM Use
The frequencies of cancer screening and self-reported women’s cancers in relation to types of TCM use are presented in Table 2. U.S. Chinese older women who have received breast cancer screening in the form of mammography tests were more likely to use any TCM than not use TCM (62.0% vs. 50.3%, p < .001). They were more likely to use acupuncture, massage therapy, tai chi, and other forms of TCM than not use TCM. In terms of cervical cancer screening, those who have had a pap smear test were more likely to use TCM than not (44.0% vs. 28.3%, p < .001). They were more likely to use herbal TCM, acupuncture, massage therapy, tai chi, and other forms of TCM than not. Those with breast cancer were more likely to use massage therapy and practice tai chi than not use TCM. For participants with uterine cancer, they were more likely to practice tai chi than not use TCM. Participants with ovarian or cervical cancer were not related to using any TCM at a higher rate.
Frequency of Cancer Screening and Cancer By TCM Use, N (&).

Note. TCM = Traditional Chinese Medicine.
p < .05. **p < .01. ***p < .001.
Associations Between Cancer and TCM Use
Table 3 presents the association between U.S. Chinese older women who have had cancer screenings and TCM use. Table 4 presents the associations between those who have self-reported cancer and TCM use. Both tables present TCM as a continuous outcome and RRs were generated from a model of regressions that adjusted for age, education, income, marital status, household composition, number of children, number of years in the United States, and years in a neighborhood. Breast cancer screening (mammography tests) was associated with higher overall TCM use (RR = 1.27, CI = [1.16, 1.40]), herbal TCM use (RR = 1.15, CI = [1.03, 1.29]), acupuncture (RR = 1.62, CI = [1.21, 2.15]), massage therapy (RR = 2.05, CI = [1.46,2.88]), and tai chi (RR = 1.86, CI = [1.28, 2.69]). Cervical cancer screening (pap smear tests) was associated with higher overall TCM use (RR = 1.38, CI = 1.26, 1.52), herbal TCM use (RR = 1.32, CI = [1.17, 1.48]), acupuncture (RR = 1.66, CI = [1.27, 2.18]), massage therapy (RR = 1.61, CI = [1.17, 2.21]), tai chi (RR = 1.69, CI = [1.19, 2.40]), and other forms of TCM (RR = 1.36, CI = [1.04, 1.79]). The only significant finding for women’s cancers was that those with cervical cancer were less likely to use herbal remedies (RR = 0.42, CI = [0.19, 0.93]).
Associations Between Cancer Screening Prevalence and TCM Use.

Note. Adjusted for age, education, income, marital status, household composition, number of children, years in United States, and years in neighborhood. TCM = Traditional Chinese Medicine; RR = rate ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Associations Between Cancer Prevalence and TCM Use.
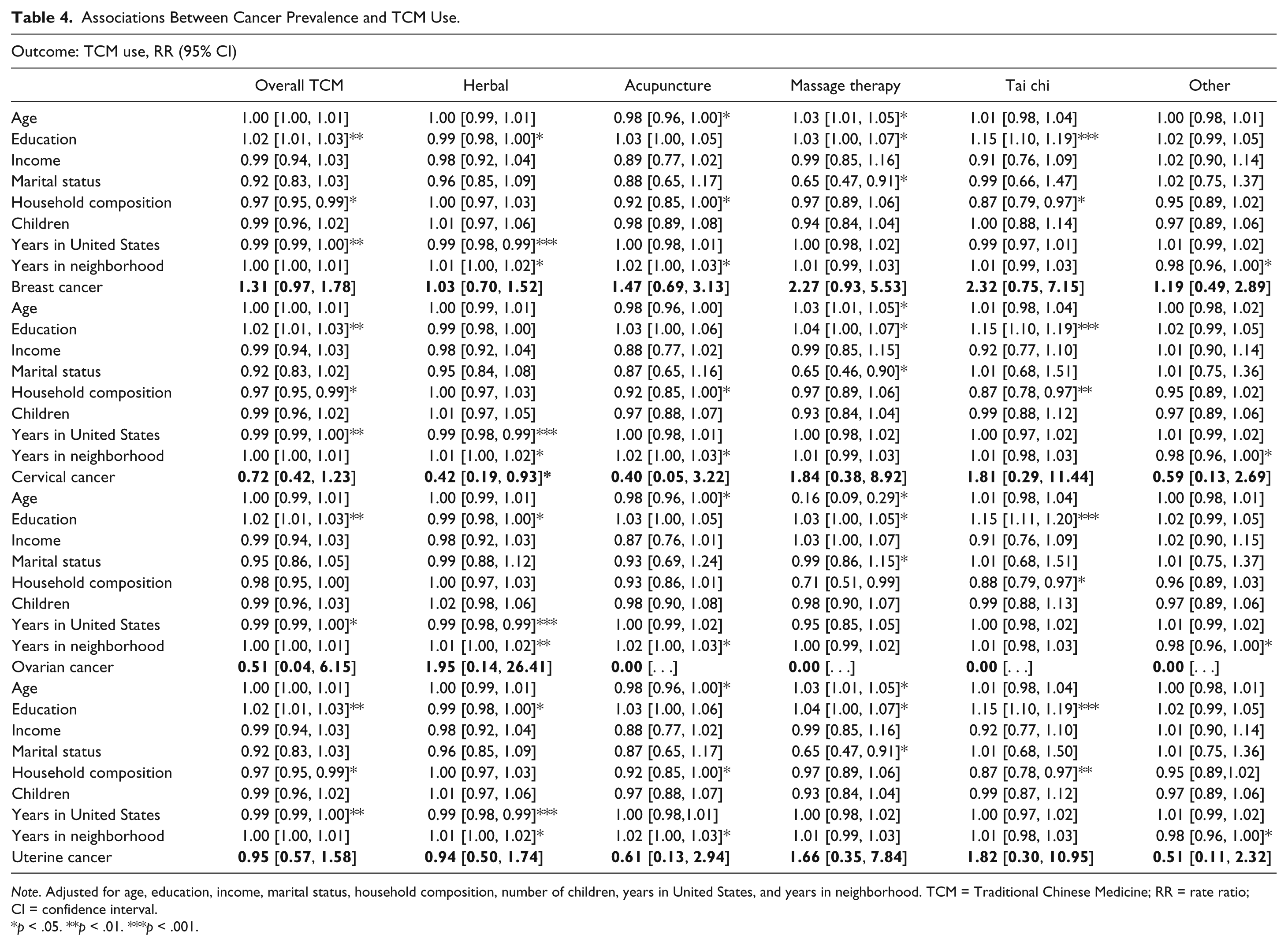
Note. Adjusted for age, education, income, marital status, household composition, number of children, years in United States, and years in neighborhood. TCM = Traditional Chinese Medicine; RR = rate ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Discussion
Our study is the first and largest population-based epidemiological study on older Chinese women in the Chicagoland area that examines the relationship between U.S. Chinese older women’s cancer screening tendencies, cancer, and TCM use. About 79% of our sample used any form of TCM, and women were more likely to use TCM than not if they have a history of cancer screenings. However, breast, cervical, uterine, and ovarian cancer were not associated with overall TCM use. Overall, TCM is commonly used in conjunction with Western medicine, rather than instead of Western medicine.
Our study suggests that women are more likely to use TCM if they have specific sociodemographic characteristics. Those with higher levels of education are more likely to practice tai chi than not practice. Those with lower levels of education are more likely to use herbal TCM than not. Older adults are more likely to receive massage therapy than not receive massage therapy while those who are married are more likely to not use massage than to use massage therapy. These findings contribute to past research that suggests that health practices are related to one’s sociodemographic background, potentially related to cultural beliefs of TCM efficacy and application (Kwok & Sullivan, 2006; B. Wang et al., 2013). However, the association between these factors is unclear as our study did not collect qualitative data on traditional TCM beliefs. Further research is needed to understand how cultural factors of TCM beliefs and sociodemographic characteristics interact, potentially predisposing participants to use TCM. An understanding of TCM use is important for culturally appropriate patient-centered care because TCM application among U.S. Chinese older women is not understood despite its frequent usage. Past literature suggests that TCM contributes to the overall management of cancer patients and could potentially improve care (Hui, Hui, & Johnston, 2006), which emphasizes the need for health professionals to exercise cultural awareness and implement patient-centered care.
Our results demonstrate that older Chinese women who have had breast or cervical cancer screening using mammography tests or pap smear tests are more likely to use TCM than not use TCM. For those who have received a mammography test, they are more likely to use herbal remedies, acupuncture, massage therapy, and tai chi than not use TCM. In regard to pap smear tests, individuals are more likely to use herbal remedies, acupuncture, massage therapy, tai chi, and other forms of TCM than not use TCM. While both Eastern and Western countries practice preventive health, Chinese women often favor the multifunctionality of TCM over cancer screening (J. H. Wang et al., 2009) as it is used as a form of treatment and/or as a means to maintain one’s health (Liu, Sun, & Louie, 2015). Previous literature suggests that TCM is used instead of Western medicine (S. C. H. Chang et al., 2013; Kwok & Sullivan, 2006), however, our results differ from past studies and demonstrate that Chinese older women who have received cancer screenings also elect to use TCM. Rather than solely choosing one, they report utilizing both Eastern and Western health practices. Higher levels of acculturation may contribute to this trend as individuals adopt new health outlooks and norms of health practices. However, acculturation’s role in health practices and TCM use is not explored in our study. Further qualitative research is needed to observe acculturation’s impact on the association between older Chinese women’s cancer screening tendencies and TCM use.
Looking at women’s cancers, our findings suggest that, overall, there is not a significant association between older Chinese women with self-reported cancer and higher TCM use. Alternatively, past research conducted in China and other countries has emphasized the association between presence of women’s cancers and TCM use. Herbal TCM is commonly used as cancer treatment (Z. Chen et al., 2008), yet our results indicate that U.S. Chinese older women with cervical cancer are more likely to not use herbal remedies than to use herbal remedies. This discrepancy may be due to differences in samples. One such example is that TCM is more mainstream and accessible in China and other countries, which may indicate increased likelihood of TCM use. In addition, our sample was drawn from a population study, whereas other studies focused solely on women with cancer; there were relatively fewer participants with specific women’s cancers. It is important to consider these differences and note that our findings are specific to U.S. Chinese older women in the Chicagoland area. Those with women’s cancers are not more likely to use TCM than Chinese older women in general. However, Chinese older women with cancer often use TCM (Dong, Bergren, & Chang, 2015b) in other countries, which warrants further research to explore the context in which TCM is used and reasons for use. These reasons can be compared with cancer symptoms and beliefs, which may elucidate why U.S. Chinese older women with cancer are not associated with higher TCM use in addition to unveiling health trends of TCM use.
Our study has a few limitations. First, the influence of cultural factors (TCM beliefs) on sociodemographic factors, and subsequently TCM use, was not observed. Second, we lack information on reasons for TCM use and other health practices. Third, we cannot apply our findings to other populations; these results can only be applied to U.S. Chinese older women.
Despite these limitations, our study has important implications for future research and health care efforts. There is currently paucity in quantitative and qualitative data concerning reasons for TCM use and how cultural beliefs influence sociodemographics and TCM use. Therefore, future studies should conduct a more thorough review of cultural TCM beliefs and the context in which TCM is used. These studies may unveil other patterns of TCM use, which could establish new standards for physicians when assessing patients and an understanding of TCM applications. Our findings demonstrate that Chinese older women use both Eastern and Western medicine, which prompts the need for physicians to inquire TCM usage to anticipate potential interactions with Western medications. In addition, health professionals could better cater health education in a manner that resonates with this population. Health workshops can help improve community members’ understandings of screenings and health conditions (Dong, Li, Chen, Chang, & Simon, 2013), yet these resources are often underutilized. To increase awareness, past research has suggested incorporating TCM knowledge (X. Wang et al., 2014), however, our findings demonstrate that TCM users already receive cancer screening. This challenges our previous assumption that Chinese women use less Western medicine due to beliefs in Eastern medicine. Therefore, other factors contributing to low cancer screening rates and health education attendance need to be explored, such as inaccessibility, language issues, or health literacy levels. If these barriers are addressed, U.S. Chinese older women may become more receptive to workshops, which can improve health knowledge and potentially their overall health status.
Conclusion
In conclusion, our study found that sociodemographic characteristics and cancer screenings (mammography tests and pap smear tests) are related to TCM use. These results indicate that further research on TCM use is necessary to better understand U.S. Chinese older women’s health practices and factors that may contribute to the use of TCM. In addition, we found that those with cervical cancer are less likely to use herbal medicine. Although those with self-reported women’s cancers are not more likely to have higher TCM utilization, future studies should be conducted to understand how this population differs from others that exhibit an association with TCM use as well as reasons for TCM use. Altogether, our findings and continued research will contribute to a better understanding of TCM use and improve the delivery of health care for this population while fostering a transition to culturally relevant patient-centered care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.