
Abstract
Introduction
Falls are the primary cause of accident-related mortality among older adults, and nonfatal falls are a leading cause of injury and disability in this age group (Hu & Baker, 2010; Stevens, Corso, Finkelstein, & Miller, 2006). Psychological factors (fear of falling) and physiological factors (poor gait and balance) are independent risk factors for falls (Delbaere, Close, Brodaty, Sachdev, & Lord, 2010); however, both need to be addressed in fall prevention (Todd & Skelton, 2004).
Many programs have been developed to address falls in older adults. Some focus on psychological risk factors, using education about risk factors and correcting misconceptions about falls. Randomized controlled trials (RCTs) have demonstrated that education programs can be effective when delivered in the community, with participants reporting improvement in confidence and activity level compared with controls (Smith, Jiang, & Ory, 2012; Smith, Ory, Belza, & Altpeter, 2012; Tennstedt et al., 1998). However, there is only modest evidence for reduction in the number of falls (Smith, Ory, & Larsen, 2010; Tennstedt et al., 1998), and there has been little exploration using objective measures of gait and balance.
Other programs focus on physiological risk factors, through a graduated series of exercises targeting strength, balance, flexibility, and coordination. There are several evidence-based exercise-based programs (Stevens & Burns, 2015); however, fear of falling and building confidence are not always directly addressed in these programs. A recent systematic review concludes that exercise programs confer moderate benefits for reducing fear of falling (Kendrick et al., 2014).
An additional issue to be addressed is whether older adults will participate in fall-prevention programs. Known barriers include pain, health problems, low motivation, lack of perception of need, lack of education about the health benefits of exercise, and transportation (Calhoun et al., 2011; Dickinson et al., 2011; Elskamp, Hartholt, Patka, van Beeck, & van der Cammen, 2012; Yardley et al., 2006). Because studies have shown that ongoing participation is crucial for falls prevention (Wurzer, Waters, Hale, & de la Barra, 2014), the greatest challenge may be the development of programming older adults want to integrate into their lives on an ongoing basis.
As a potential solution to the problem of participation, “joyful movement” has not yet been fully explored. “Joyful movement” can be defined as movement that encourages positive experience: awareness of the body during movement, discovery of the possibilities of movement, and challenging the body. Empirically tested fall-prevention programs tend to focus on reducing fears associated with falling, yet the burgeoning field of positive psychology suggests that reducing negative emotions (e.g., fear) is not the same as cultivating positive emotions (e.g., joy; Siegal, 2014). Dance-inspired methods provide a possibly more joyful, alternative fall-prevention intervention to conventional exercise. A systematic review found quality evidence for the effectiveness of dance-based exercise for falls-relevant outcomes such as strength, endurance, flexibility, balance, and gait (Keogh, Kilding, Pidgeon, Ashley, & Gills, 2009). An approach that emphasizes the enjoyable aspects of movement in combination with a focus on preventing falls may positively affect the interest and ongoing engagement of some older adults.
Fall Stop…MOVE STRONG TM is a community-based program that combines joyful movement with fall-prevention education. Over the years, the program has been hosted at four community sites in New York City. The program is offered at introductory, intermediate, and advanced levels. The objective of the present study is to evaluate the introductory-level classes with respect to (a) the feasibility of implementation and patterns of program use, (b) participant satisfaction, and (c) fall-related outcomes.
Design and Method
Design
The program was evaluated using a one-group pre–post study design. Data were collected on participants enrolling in the introductory-level classes at two time-points: baseline (at the initial class) and post (at the end of the final class). Qualitative feedback was collected at the end of the final session. There was no follow up.
Recruitment
Participants were made aware of the class through on-site advertising, word of mouth, and by physician referral. The program was offered at four sites: Site 1 was a community center providing a range of health and wellness classes. Since 2004, members have been eligible to enroll in the program for a fee. Site 2 was a hospital-based clinic that provides health programming. Since 2010, patients have been eligible to participate at no cost. Site 3 was a naturally occurring retirement community. Site 4 was an affordable independent senior housing program. Since 2013, older residents have been eligible to enroll at these two sites at no cost. For these participants, the program was translated into both Cantonese and Spanish language.
Participants
Participants were community-dwelling men or women age 60 or older who were ambulatory with or without assistive devices. Participants were excluded if they were nonambulatory or had cognitive impairment that prevented them from following simple directions. The study was approved by the Institutional Review Boards of Touro College School of Health Sciences and Mt Sinai Hospital. For Sites 1, 3, and 4, approval was given to review program evaluation data. For Site 2, participants provided written informed consent.
The Program
The Fall Stop…MOVE STRONGTM program adopts a group format with the aim of building motivation and support for staying physically active. The conceptual underpinnings of the program have three interrelated dimensions (see Figure 1). One dimension is finding joy in movement. We have observed that older adults associate movement with pain, injury, or embarrassment. The program promotes more positive associations through movements that engage the whole body in a lively way rather than repetitive exercises targeting individual body areas.
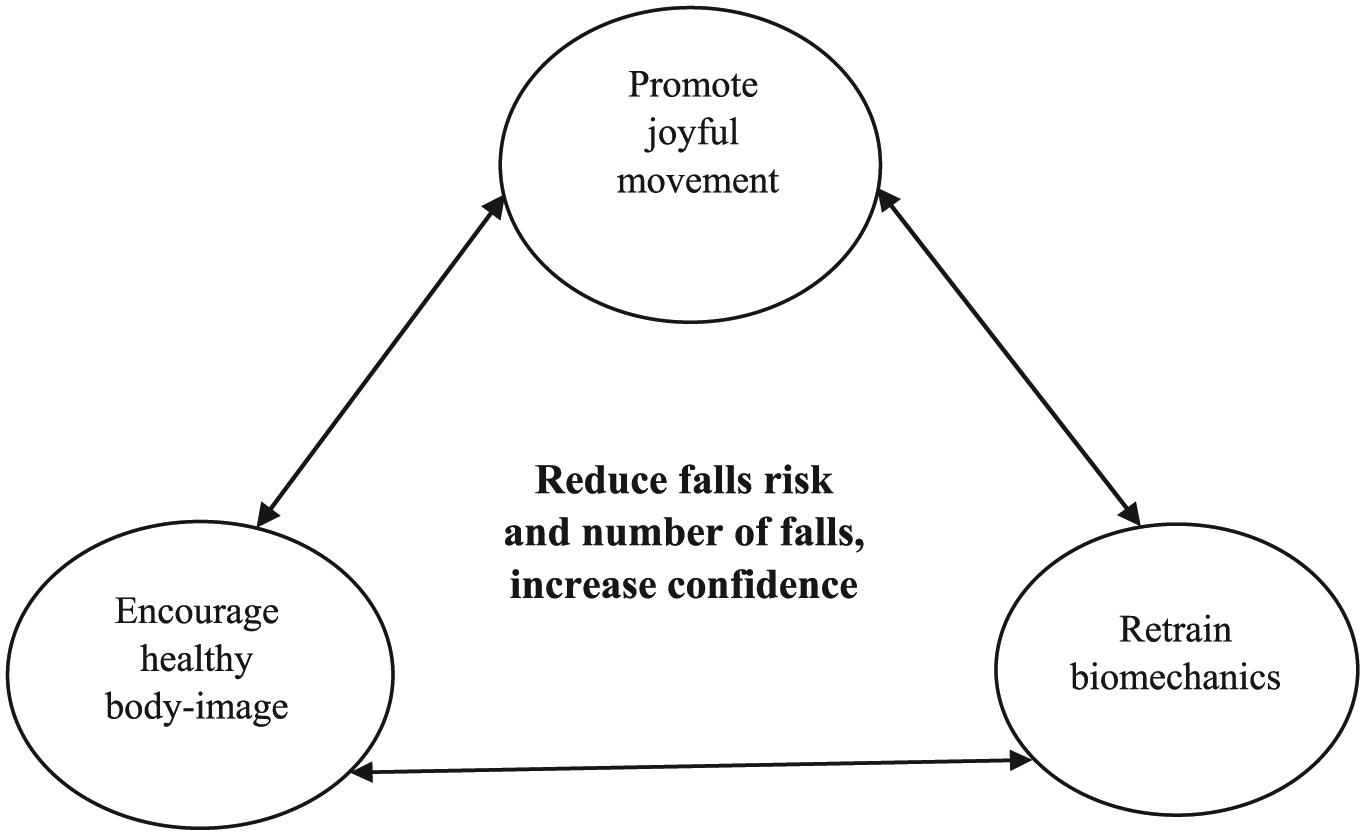
Summary of Goals and Dimensions of the Program.
A second dimension is cultivating a positive body image. Older adults struggle with the physical changes of the body (Ekwall, Hallberg, & Kristensson, 2012). Participants learn to shift away from a self-critical view toward an appreciative view of the body. At every class in the program, participants are directed to take time to reflect on their bodies with gratitude.
The third dimension is retraining the body from head to toe to stimulate functional gains. Each class incorporates sequences of physical movement that target posture, proprioception, and moving in space. These sequences target key challenges that older adults experience in moving safely with confidence, and progress over the classes from a few movements to many, and from relatively simple movements to more complex ones. Illustrations are available from the corresponding author on request.
The introductory curriculum consists of 10 classes, which are held once weekly for 1 hr (see Table 1). During the evaluation period, classes were led in person by a professional dancer and/or an occupational therapist. Classes typically involved 10 to 15 participants. Movements were practiced while standing for the first 30 min of the class, while seated for the next 15 min, and while standing for the remaining 15 min. The introductory class does not incorporate music as this has been found to distract participants from focusing on awareness of movement. The movements are instead taught rhythmically. Three of the classes include education about risk factors for falls and recommended strategies for managing these risks. Participants report as a group on their home practice at the beginning of each class, but there is no formal reporting of homework completion.
Summary of the Content for Each Session of the Program.

Outcome Measures
Baseline and postassessments were administered by the same person: one of the class instructors (an occupational therapist or a dance-fitness expert trained in the administration of these evaluations) or an occupational therapy intern (trained and supervised in the administration of the evaluations).
The Functional Reach (FR) Test
This test (Duncan, Weiner, Chandler, & Studenski, 1990) evaluates balance through measurement of a participant’s ability to extend arms out while standing near a wall and keeping his or her feet flat on the floor and hand at the level of a ruler indicated on the wall. Reach is measured in inches.
The Modified Falls Efficacy Scale (MFES)
This 14-item questionnaire (Hill, Schwarz, Kalogeropoulos, & Gibson, 1996) evaluates confidence in carrying out daily activities without falling. Ratings are completed on a scale from “0” (not at all confident) to “10” (completely confident), and an average is calculated for the scale’s items. In one community-dwelling sample, a mean score of 9.76 was found in healthy subjects, whereas a mean of 7.69 was found in a clinical sample (Hill et al., 1996). Alternate versions of the measure have been found to be good predictors of future falls (Lusardi et al., 2017).
Participants at Site 2 completed two additional measures of falls risk during the program evaluation. One measure, the Four-Square Step Test (FSST; Dite & Temple, 2002), measures dynamic standing balance by having a subject step over low objects and move in four directions. The score reflects time (in seconds) needed to step over sticks without touching them. Taking more than 15 s to complete this test is predictive of recurrent falls. The other measure was The Timed “Up and Go” Test (TUG). This test (Podsiadlo & Richardson, 1991) measures mobility as the time taken by an individual to stand up from a standard arm chair, walk a distance of 3 m, turn, walk back to the chair, and sit down. Taking 13.5 s or longer can be indicative of risk for falls (Barry, Galvin, Keogh, Horgan, & Fahey, 2014). It has been shown to be a strong predictor of fall risk (Lusardi et al., 2017).
Participant feedback
All participants who attended the final class were invited to provide anonymous written feedback to three open-ended questions: “Tell us about the physical benefits of the class,” “Tell us about the psychological benefits of the class,” and “Do you have suggestions to make the class better meet your needs?” It was not possible to assess perceptions at baseline because questions related to the experience of doing the program.
Fall accidents
All participants were asked to report on the number of fall accidents experienced during the 6 months prior to starting the program and any falls that occurred during the period that they were taking the class. A fall was defined as an unintentional movement to the ground.
Statistical Analysis
Descriptive statistics are presented on enrollment, number of program sessions completed, and the number of times participants enrolled in the program.
Participants’ written feedback on the program following completion of classes was analyzed to gauge participant satisfaction. The responses were read by two raters to extract underlying themes. Responses were coded by the raters independently and then reconciled through discussion. Descriptive statistics are presented for key themes.
To evaluate the impact of the program on functional balance and confidence, paired t tests were performed to compare pre- and post-scores for study outcomes: FR and MFES. Effect sizes (Cohen’s d) were computed to assess the magnitude of effects. Exploratory analyses were conducted to evaluate the impact of the program according to clinical deficit by grouping participants according to baseline FR as follows: “High risk”: <6 inches, “Moderate risk”: 6 to 10 inches, and “Low risk”: >10 inches. Furthermore, t tests were conducted for the FSST (seconds) and TUG (seconds) outcome measures at Site 2. Finally, to assess the impact of the program on the incidence of falls (an ordinal variable), McNemar–Bowker’s analysis compared the frequency of falls among participants during the 6-month period before commencing the program with the frequency of falls during the 2.5-month program period. Analyses were not adjusted for the effects of multiple statistical tests. Significance was set at .05.
Results
Characteristics of the Sample
Over the program evaluation period (2010-2014), 215 participants enrolled in the introductory-level program. The distribution of participants across sites was as follows: Site 1 = 54%, Site 2 = 35%, Site 3 = 7%, and Site 4 = 3%. Of these participants, 102 (47%) completed both pre- and post-program evaluations. Table 2 presents background characteristics for the study participants. Additional characteristics of participants at Site 2 were as follows: living alone = 25 (52.1%), taking no prescription medication = 6 (14.6%), taking one to three prescription medication = 18 (43.9%), and taking four or more prescription medications = 17 (43.3%).
Background Characteristics of Study Participants.

Forty-three missing cases.
Nine missing cases.
Valid %, three missing cases.
Valid %, 45 missing cases.
Valid %, one missing case.
Attendance
The majority of participants (94%) were taking the introductory class for the first time. Most (71%) went on to repeat the introductory class. Data on the number of sessions attended were available for 93 participants (43%). The mean attendance was 6.96 sessions (SD = 3.34), and 51 (55%) of participants had an adherence of 80% or more. Data were available for 50 (49%) of the participants who completed both pre- and post-assessments. For this subgroup, mean attendance was 8.94 sessions (SD = 1.88), and 40 (80%) had an adherence of 80% or more.
Adverse and Unexpected Events
There were no adverse or unexpected events related to participation in the program.
Perceptions of the Program
Eighty-six participants (40%) provided written feedback on the program, and key themes extracted from their responses are summarized in Table 3.
Themes Expressed in Feedback by Participants (N = 86).

Because these data involve spontaneous feedback from participants, it should not be assumed that other participants did not experience these benefits.
Fall-Related Outcomes
There were no significant differences in age, gender, or baseline fall risk between participants who completed both pre- and post-program assessments and those who did not. However, participants who had completed both had significantly higher baseline MFES scores (M = 8.62, SD = 1.72) than those who did not (M = 8.02, SD = 2.26), t (197) = 2.103, p =.037.
Participants who completed both assessments showed clinically significant pre–post improvements in FR (d = .60, p < .001) and falls efficacy (MFES; d = 0.17, p < .001). Exploratory t tests indicate that improvement in these outcomes was greatest in the “high risk” group, followed by the “moderate risk group” and then the “low risk group” (see Table 4). Analysis of additional data at Site 2 showed significant improvements on the TUG from pre (M = 14.86 [SD = 9.93]) to post (M = 13.13 [SD = 8.08]), Cohen’s d = 0.17, p < .01, and on the FSST from pre (M = 14.35 [SD = 8.25]) to post (M = 11.30 [SD = 5.31]), Cohen’s d = 2.49, p < .001. Finally, 44 (43.6%) participants reported having had a fall in the 6 months prior to the program, compared with 17 (17%) participants during the 3-month program period (p < .001).
Pre–Post Changes in Functional Reach and Falls Efficacy: Overall and by Falls-Risk.

Note. d = effect size, Cohen’s d = (Mbaseline − Mpost); t = paired t test; CI = confidence interval; FR = functional reach (inches); MFES = Modified Falls Efficacy Scale (average score).
Discussion
This study explores the potential of fall-prevention programming that emphasizes joyful movement to engage older adults in diverse community settings. Although numbers at two of these sites were small, they point to the feasibility of implementing programming in a variety of venues and the capacity of the program to reach a diverse range of ethnic groups. The levels of retention and adherence were at the low end of the range documented in RCTs of exercise-based fall prevention (Stevens & Burns, 2015) but consistent with levels reported in program evaluations (Smith et al., 2010). A unique aspect of this program was that participants had the opportunity to re-enroll. Seventy-one percent of participants did so; this is a conservative number, as others went on to higher-level classes or retook the introductory class after the study period.
A strength of the study is its inclusion of objective measures of balance and mobility. Taken as a group, participants made clinically significant improvements in balance ability and (when assessed) mobility and speed, with gains most apparent in those who initially had lower levels of function. Effect sizes were similar to those found for other exercise interventions, particularly those with a challenge to balance (Gillespie et al., 2012; Sherrington et al., 2016), including Tai Chi (Huang, Feng, Li, & Lv, 2017). These findings are noteworthy given the brief nature of this program’s intervention in comparison with the number and frequency per week of sessions in Tai Chi and other exercise-based interventions (two to three times per week over 12 to 48 weeks; Huang et al., 2017; Sherrington et al., 2016; Stevens & Burns, 2015). The findings also provide preliminary support for the hypothesis that the program is protective against future falls.
The findings also confirmed that older adults can gain a more positive outlook with regard to avoiding falls. Participants showed statistically significant increases in confidence about avoiding falls, with effect sizes comparable with the small to medium ones found for interventions targeting fear of falling (Tennstedt et al., 1998) and for other exercise programs (Kendrick et al., 2014). It is unclear why participants showed only a statistically significant improvement in efficacy when there were clinically significant improvements in function. Future studies should examine the possibility that confidence lags behind physical gains.
Another avenue that warrants future exploration is the question of what types of professional training are appropriate to the teaching of the program. Fall Stop…MOVE STRONGTM can be led by professionals with education or certification in physical therapy, occupational therapy, recreation therapy, or fitness, which is consistent with the requirements for other exercise-based programs (Stevens & Burns, 2015). Since the period of the study, however, the program has been successfully conducted at select locations using a DVD version under the supervision of a nurse or social worker who is trained as a facilitator. Additional investigation of whether participants in this form of the program experience a similar degree of benefit would be useful to establish cost-effectiveness.
Limitations
There are limitations in this study that are associated with real-world implementation. The level of missing data was high given that some participants chose to forgo assessments; thus, selection biases cannot be ruled out. Long-term follow-up data are needed on whether participants maintain gains over time, and whether benefits accrue with increases in dose of classes (i.e., if classes are held more frequently than once a week or with successive instances of enrollment). No data were obtained on participants’ level of social or family support or any barriers to participation. The study also relied on participant report of fall events, which is unreliable; longitudinal follow-up should be conducted in the future to see whether future falls are decreased when assessed by objective measures. Measurement of the fidelity of the program delivery and participant’s compliance with homework would also help illuminate the program’s effectiveness, while a control condition would help clarify whether encouraging the positive experience of movement has benefits above and beyond currently available types of intervention. It would be particularly useful to explore the extent to which program principles (positive experience of movement, cultivating a more positive body image, and retraining biomechanics) underlie the observed benefits. Future efforts should characterize the different elements of joyful movement and specify more precisely how they relate to physical function, falls, and disability (Steptoe, de Oliveira, Demakakos, & Zaninotto, 2014), and also more rigorously evaluate the degree to which clinically meaningful outcomes, for example, improvements in function and independence in daily activities, are attained.
In summary, Fall Stop…MOVE STRONGTM, a community-based program that combines joyful movement with fall-prevention education, significantly increased participant’s falls efficacy and improved their performance on assessments of fall risk. Participant feedback showed a high degree of satisfaction with the program that often led to re-enrollment.
Footnotes
Acknowledgements
The authors wish to thank participants in the Fall Stop…MOVE STRONGTM program. They also wish to thank staff and faculty of participating organizations: Caroline Kohles of the Jewish Community Center of Manhattan, faculty and staff of the Martha Stewart Center for Living at Mount Sinai Hospital, Marcy Simon at Educational Alliance, and Alma Collazo at Linkage House. They wish to thank President of Manhattan Chamber of Commerce Nancy Ploeger; Shikha Mittal and Occupational Therapy Students of Touro College, New York, for their assistance with data entry; Meira Orentlicher, PhD, for research mentorship and support; and Mildred Hird (primary demonstrator and attendance taker). Finally, they thank Naomi Azulay, PT, and anonymous reviewers for their feedback on earlier versions of this manuscript, and Mary-Jane Ojie, PhD, and Crystal Gehr, BA, for assistance with its preparation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Celeste Carlucci is President of Fall Stop . . . MOVE STRONG™. None of the other authors have any disclosures.
Authors’ Note
Preliminary analyses of the data from this study were presented in poster form in March 2010 at the National Council on Aging/American Society on Aging (NCOA/ASA) Aging in America Annual Conference, Chicago, Illinois (“Fall Stop . . . MOVE STRONG™: A Model for a Community Based Fall Prevention & Strengthening Program for Older Adults”); in April 2012, at the American Occupational Therapy Association Annual Conference, Indianapolis, Indiana (“Fall Stop . . . MOVE STRONG™: A Successful Community Based Fall Prevention Program”); in May 2012 at the Annual Scientific Meeting of the American Geriatrics Society, Seattle, Washington (“Fall Stop . . . MOVE STRONG™: To Reduce Fall Risk Among Community Dwelling Older Adults”); in a short course form in April 2011 at the NCOA/ASA Aging in America Annual Conference, San Francisco, California
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for a portion of the Fall Stop . . . MOVE STRONG™ program was provided by a grant from the Manhattan Chamber of Commerce to the Senior Fall Prevention Institute and Mount Sinai Hospital, New York.