
Abstract
Introduction
Good balance is essential for upright stance and for most daily living activities. Balance requires that the CNS receives and integrates the position of different body segments, as well as their relationship with each other and the surroundings. When healthy humans stand unperturbed on a solid surface in a well-lit surrounding, most of the input to the central nervous system (CNS) is received from the somatosensory system and less from the visual and vestibular systems (Horak, 2006; Peterka, 2002). With increasing age, however, the integrity of the somatosensory, visual, and vestibular systems declines, resulting in sensory impairments as well as gait and balance disturbances (Horak, 2006; Lord, Clark, & Webster, 1991). The combination of senescent decline in organ function and higher disease prevalence in balance control systems predisposes elderly to balance impairment, increased fall risk, and dependency (Lord, Ward, Williams, & Anstey, 1994; Nnodim & Yung, 2015).
Somatosensation in the feet, being the boundary between the body and the ground, plays an important role in controlling upright stance (Kavounoudias, Roll, & Roll, 1998). The somatosensory system includes both the tactile system, associated with sensations of touch and pressure and more complex sensations like vibration, and the proprioceptive system, which is associated with sensations of muscle length and tension, joint angles, and changes in these angles. Plantar-surface touch and vibration sensation is known to decrease as a function of higher age (Kenshalo, 1986; Perry, 2006; Wells, Ward, Chua, & Inglis, 2003). The sensory thresholds in older adults are hypothesized to be much higher due to changes in receptor morphology, reduction of receptor density, decreased elasticity of the skin, and decreased nerve conduction (Kenshalo, 1986). Severely diminished foot somatosensation contributes to balance deficits and increased fall risk (Kars, Hijmans, Geertzen, & Zijlstra, 2009; Lord et al., 1994; Richardson & Hurvitz, 1995). Accordingly, when evaluating impaired balance control in older adults, assessing the somatosensory system is an important parameter.
Touch sensation can be determined by clinical screening using a simple cotton swab or a single 10-g monofilament, to more precise tactile pressure sensation thresholds (TPSTs) testing with multiple Semmes–Weinstein monofilaments (Dros, Wewerinke, Bindels, & van Weert, 2009; Patel, Magnusson, Kristinsdottir, & Fransson, 2009; Perry, 2006). Vibration sensation can be clinically assessed using a tuning fork or, more accurately, by using a biothesiometer to determine vibration perception thresholds (VPTs; Patel et al., 2009; Temlett, 2009). Balance can be effectively evaluated in the ambulatory care setting using a combination of scalar well-validated questionnaires, dedicated history-taking, and functional balance tests based on postural activities and movements which occur during everyday life (Nnodim & Yung, 2015).
Despite these numerous well-known balance tests, little is known about the impact of tactile pressure and vibration sensation impairment on functional and subjective balance problems in healthy aging. Therefore, the objective of this study is to enhance the comprehension of the risk of falling in older adults. In doing so, the aim was to better understand how the decline in somatosensation in the lower limbs in relatively healthy older adults and elderly influences functional and perceived balance problems.
Method
Forty relatively healthy community-dwelling older adults were recruited for a multimodal balance enhancing exercise program (BEEP) to be performed regularly for 6 weeks in a single-arm crossover study. A minimum age of 60 years and walking without aid was required to participate. Six subjects could not complete the study because of atrial fibrillation, intra-articular knee infection, personal loss, clinical depression, pneumonia, and busy holiday schedule. Thus, thirty-four 60- to 78-year-old subjects (M = 69 ± 5), 53% women and 41% still in part- or full-time employment, underwent a thorough medical examination including medical and trauma history (Hafstrom, Malmstrom, Terden, Fransson, & Magnusson, 2016). Written informed consent was obtained from all participants before the tests. They were informed that they could stop the tests and participation in the study for any reason and without explanation. The number of subjects in the cohort met the appropriate sample size, which was also balanced against resources available (i.e., volunteers).
The present study was designed to capture both quantitative (e.g., TPSTs and VPTs) and qualitative measures (e.g., questionnaires) before the subjects began the BEEP intervention. Analyses were performed to determine the extent to which peripheral sensation and age could explain perceived and functional balance impairments. The study was approved by the local ethics committee and performed in accordance with the revised version of the Helsinki declaration.
Assessment of Peripheral Sensation
TPSTs were assessed with the Semmes–Weinstein pressure aesthesiometer (Touch-Test™ Sensory Evaluators, 20-piece Kit, Stoelting Co., USA). Subjects lay supine with eyes closed (EC) and were instructed to indicate when they felt the filament in contact with the glabrous skin on the first toe (Dig-I), the fifth toe (Dig-V), or heel pads. TPST for the different sites were determined in randomized order using the staircase technique from three ascending and descending steps described by Lord, Menz, and Tiedemann (2003). An average of the measurements from the three sites of each foot was recorded as the TPST.
VPTs were assessed with a biothesiometer (Model EG electronic BioThesiometer, Newbury, OH, USA) that generates 120 Hz vibrations in varying amplitude (measured in µm). Vibration was applied on the selected bony points of the tibial tuberosity two fingers below the patella (Tibia), the medial distal end of the first metatarsophalangeal (MTP-I) bone, the lateral distal end of the fifth metatarsophalangeal (MTP-V) bone, and on the pads of the Dig-I, Dig-V, and the heel (Goldberg & Lindblom, 1979; Patel et al., 2009). Three readings in ascending and descending intensity using the staircase technique were made until the subject could no longer feel the vibration. An average of the smallest perceived amplitude recorded at the six sites from each foot was recorded as the VPT.
Functional Balance Tests
One-leg standing time (OLST) was assessed with subjects standing barefoot on solid surface (floor) or compliant surface (double-folded 2 cm thick exercise mat), with eyes open (EO) or closed (EC) up to 60 s, or until they put their foot down or repositioned the standing foot. The best attempt of three was recorded (Bohannon, Larkin, Cook, Gear, & Singer, 1984; Hafstrom et al., 2016). Functional balance, mobility, and gait performance was evaluated with five tests: Berg Balance Scale (BBS), habitual speed walking 30 m, performing a modified step-stool test, Timed Up and Go (TUG) test, and Figure-8 test (Berg, Wood-Dauphinee, Williams, & Maki, 1992; Bohannon, 1997; Hafstrom et al., 2016; Hess, Brach, Piva, & VanSwearingen, 2010; Shumway-Cook, Brauer, & Woollacott, 2000).
Questionnaires
A battery of questionnaires was administered to evaluate the subjective functional balance ability as well as level of physical activity (Hafstrom et al., 2016). The impact of dizziness and unsteadiness on quality of life was measured with the Dizziness Handicap Inventory (DHI; Jacobson & Newman, 1990). The Hospital Anxiety and Depression Scale (HADS) was administered to detect suspicion of depression, anxiety, and emotional distress (Zigmond & Snaith, 1983). Self-perceived balance ability and dizziness were measured with the Activities-Specific Balance Confidence (ABC) scale (Powell & Myers, 1995). The Human Activity Profile (HAP) questionnaire was used to measure physical fitness (Davidson & de Morton, 2007). The mean physical activity pattern was also evaluated with the Mattiasson-Nilo (M-N) questionnaire (Mattiasson-Nilo et al., 1990).
Statistical Analyses
Normality of data distribution was checked using Shapiro–Wilk. Correlations were analyzed with the Spearman’s rho tests as some values were not normally distributed. In addition, the effects of age, tactile pressure sensation, vibration sensation, and their interaction on functional balance tests and questionnaire outcome were analyzed using the generalized linear model (GLM) univariate ANOVA (stepwise forward). Values are reported as mean ± standard deviation unless otherwise stated. Statistical analysis was performed with SPSS 23.0 software (SPSS, Chicago, IL) and significance level was set to <.05.
Results
Demographics
Although the subjects considered themselves as relatively healthy, many of them had one or more chronic medical conditions (M = 2.2 ± 1.4; range = 0-5; Table 1). The mean number of drugs taken per subject was 2.3 ± 2.5 (range = 0%-11%) and 10% of the subjects presented with major polypharmacy (>five drugs). None of the subjects were on opioids. One took neuroleptic medication, five took antidepressants, and six took regular medication against insomnia.
Medical History of 34 Subjects.
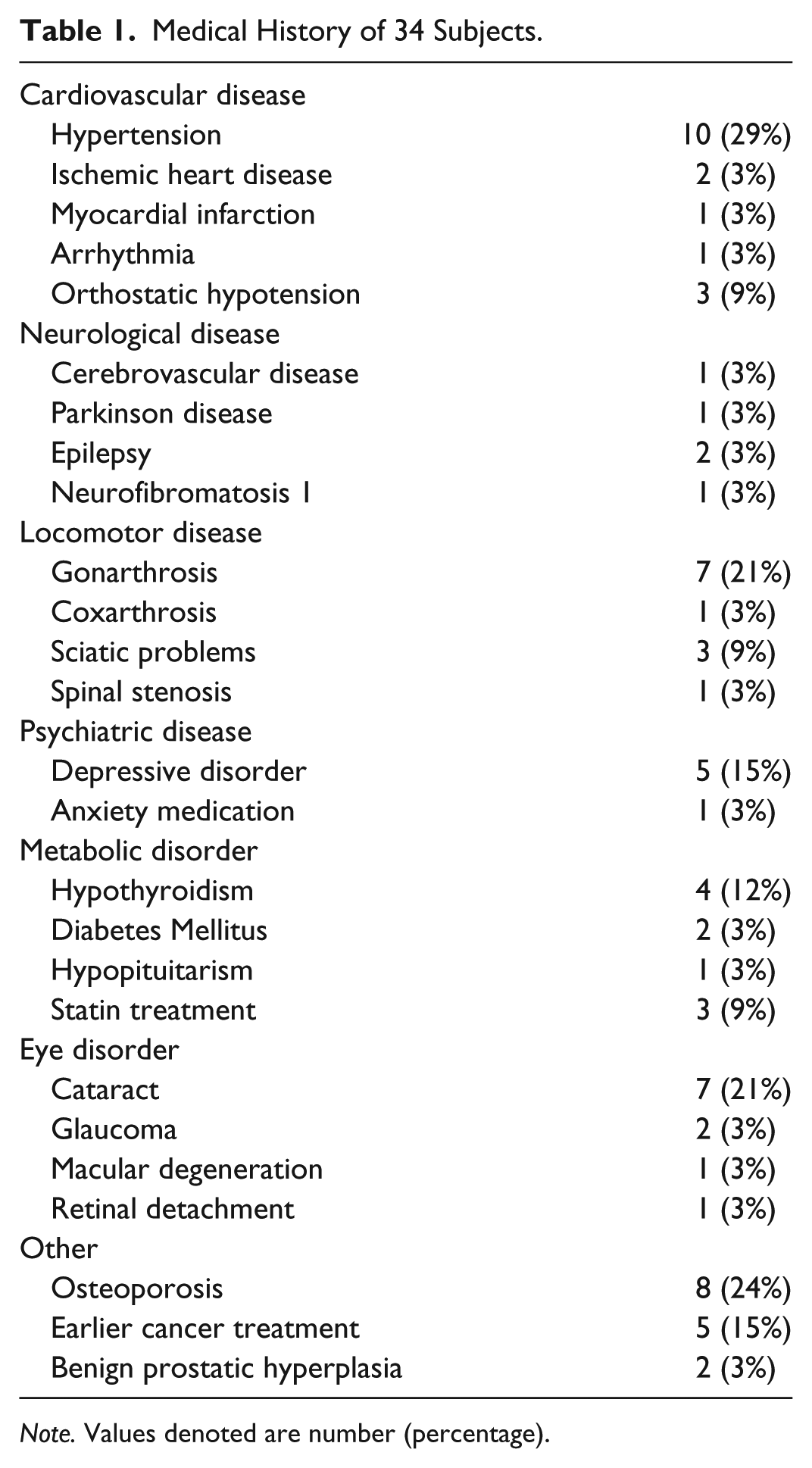
Note. Values denoted are number (percentage).
Demographics; outcome of tactile pressure and vibration sensation tests, OLST, and other functional balance tests; and questionnaire results are shown in Table 2.
Demographics, outcome of tactile pressure sensation, vibration sensation, OLST, and other functional balance tests, as well as questionnaire results for 34 subjects.

Note. BMI = body mass index; TPST = tactile pressure sensation threshold; VPT = vibration perception threshold; OLST = one-leg standing time; EO = eyes open; EC = eyes closed; TUG = Timed Up and Go; DHI = Dizziness Handicap Inventory; HADS-A and D = Hospital Anxiety and Depression Scale; ABC = Activities-Specific Balance Confidence Scale; HAP = Human Activity Profile; M-N = Mattiasson-Nilo questionnaires.
Tactile Pressure Sensation
As shown in Table 3, TPSTs had a significant main effect on OLST when subjects were standing with EO on the right foot both on solid (p = .007) and on compliant surface (p = .020). Higher TPSTs correlated with significantly shorter ipsilateral OLST on solid surface with EO and EC, as well as with EO on compliant surface (p ≤ .001; Figure 1). The correlations were stronger for the right than for the left foot (Table 3).
Correlations Between Tactile Sensation, Vibration Sensation, and Age With the Outcome of Functional Balance Tests and Questionnaries.

Note. Significant correlation factors and p values are depicted in bold. OLST = one-leg standing time; EO = eyes open; EC = eyes closed; TUG = Timed Up and Go; BBS = Bergs Balance Scale; DHI = Dizziness Handicap Inventory; HAP = Human Activity Profile; M-N = Mattiasson-Nilo questionnaires; TPST = Tactile pressure sensation threshold; VPT = vibration perception threshold; GLM = general linear model.

Tactile perception sensation threshold (TPST) plotted versus ipsilateral one leg standing time (OLST) with eyes open (EO) on solid and compliant surfaces, as well as with eyes closed (EC) on solid surface along with the respective linear trend lines. Maximum OLST limit was set to 60s. All data is shown for both legs of 34 subjects.
TPSTs also had a significant main effect on speed walking (p = .001) and performing the Figure-8 test (p < .001), as well as the outcome of the M-N questionnaire (p = .027) (Table 3). Higher TPSTs correlated with significantly lower BBS scores, as well as walking slower, both 30 m and in the Figure-8 test (p ≤ .044). Higher TPSTs also correlated with significantly higher DHI scores (p = .036). Higher TPSTs was associated with significantly higher weight (rho = 0.553; p = .001) and body mass index (BMI; rho = 0.462; p = .006) of the subjects. There were no significant differences in TPST means between the right and left foot (p = ns).
Vibration Perception
As shown in Table 3, VPT had a significant main effect on ipsilateral OLST when subjects were standing with EO on solid surface (p = .026), especially on the left foot where VPT alone explained 18.1% of the variance (p = .012). Higher VPTs correlated with significantly shorter ipsilateral OLST when subjects stood on solid surface on with EO (p = .002) and with EC (p = .003), as well as on compliant surface (p = .020) (Figure 2 and Table 3).

Vibration perception threshold (VPT) plotted versus ipsilateral one leg standing time (OLST) with eyes open (EO) on solid and compliant surfaces, as well as with eyes closed (EC) on solid surface along with the respective linear trend lines. Maximum OLST limit was set to 60s. All data is shown for both legs of 34 subjects.
VPT had a significant main effect on BBS scores (p = .007) and the outcome of DHI questionnaires (p = .011), where VPT itself in both cases explained about 20% of the variance (Table 3). Higher VPTs also correlated with significantly poorer BBS scores (p = .012) and slower speed in the Figure-8 test (p = .031), as well as higher DHI scores (p < .001) (Table 3). Higher VPTs correlated with significantly higher weight of the subjects (rho = 0.447; p = .008), but not with BMI. There were no significant differences in VPT means between the right and left foot (p = ns).
Age
With EC, age was the only factor with significant main effect on OLST, especially for the left foot where age alone explained 31.4% of the variance (p = .001; Table 3). Age also affected OLST when standing with EO. Age and ipsilateral VPT explained 49.8% of the variance on solid surface (p < .001). Age and ipsilateral TPST explained 20.6% of the variance on compliant surface (p = .002; Table 3). Age also had significant main effect on the outcome of the HAP questionnaire, explaining 26.7% of the variance (p = .002). Age had no significant effects on any of the other functional balance tests or questionnaires (Table 3).
Significant correlations were found between higher age and shorter OLST when subjects were standing on solid surface with EO and EC, as well as with EO on compliant surface (p ≤ .008; Table 3). Higher age also correlated with significantly lower scores in BBS, as well as slower speed walking and performing the Figure-8 test (p ≤ .035; Table 3). Higher age correlated with significantly poorer HAP scores (p = .003), but not with significantly higher TPSTs, VPTs, or BMI.
Subjective Balance Difficulties
Eight of the 34 subjects (24%) had DHI scores indicating perceived balance problems, four subjects had more than 16 points and four others more than 34 points, indicating mild respective moderate balance handicap problems. Six of the eight subjects had VPTs more than 15.0 µm, and the mean VPTs of all eight were significantly higher (20.4 ± 8.9 µm) compared with the 26 subjects who did not indicate perceived balance problems (9.6 ± 7.0 µm) (p < .001). VPT was the only factor with significant main effect on the outcome on DHI where it explained 19.1% of the variance (p = .011). Significant correlations were found between higher DHI scores and higher VPTs (p < .006), as well as higher TPSTs (p = .036) (Table 3).
Other Questionnaires
All subjects except three had normal HADS-A scores. Two had scores indicating mild anxiety and one indicating moderate anxiety. This latter subject was not the same subject who had an earlier known and well-medicated anxiety disorder (Table 1). All subjects had normal HADS-D scores, except one whose score indicated mild suspicion for depression. No significant associations between TPST, VPT, or age were found with the outcome of the HADS-A, HAD-D, or the ABC questionnaires.
Discussion
Identifying factors associated with impaired perceived and functional balance control in older adults and elderly can provide essential information for developing imbalance and fall accident intervention strategies. This cross-sectional study reveals important associations between somatosensation, perceived balance problems, and functional balance control. The findings suggest that the degree of somatosensation in the lower limb can be more important than chronological aging for both functional and perceived balance control in relatively healthy older adults and elderly. In addition, the results support that relatively healthy older adults, just like healthy younger adults, predominantly rely on their somatosensory system when they are in a lightened environment (Horak, 2006; Peterka, 2002). Five noteworthy outcomes will be discussed.
First, higher age was not associated with significantly poorer tactile pressure and vibration sensation. This finding was unexpected as aging leads to a decline in mechanical properties of the skin, as well as cutaneous receptor density, morphology, and physiology (Kenshalo, 1986; Peters, McKeown, Carpenter, & Inglis, 2016; Shaffer & Harrison, 2007). Morioka et al. (2012) found a significant correlation between age and somatosensation in subjects between 2 and 92 years old. Thus, the non-significant correlation between age and TSPT or VPT in our cohort might be explained by the rather narrow age span (60-78) and maybe by the subjects being relatively healthy.
Second, vibration sensation had a significant effect on BBS. This finding is notable. It has been suggested that 70-year-old community-dwelling persons are likely to have BBS scores close to the maximum (56), just like our cohort (Downs, Marquez, & Chiarelli, 2014). Given the documented BBS ceiling effect (Boulgarides, McGinty, Willett, & Barnes, 2003), one must be careful to conclude that vibration sensation is a fall risk predictor for those who score high on BBS. Furthermore, our cohort demonstrated fairly good correlation between BBS and VPT, TPST, and age. This outcome is in line with BBS scores deteriorating by about 0.7 points per year and becoming more variable beyond 70 years of age (Downs et al., 2014).
Third, poorer tactile pressure sensation meant slower walking speed and Figure-8 tests. This is expected given that individuals with diabetes and other peripheral neuropathies have a harder time walking quickly (Dingwell, Cusumano, Sternad, & Cavanagh, 2000). Interestingly, however, comparatively small variations in TPST in our relatively healthy subjects had a significant impact on walking speed. Someone with slightly lower sensation in the feet may be hesitant to walk as fast as someone who has somewhat better sensation. This assumption is corroborated by our finding that subjects with poorer somatosensation had more perceived balance difficulties as expressed by DHI scores.
Fourth, with visual information available, poorer tactile pressure and vibration sensation resulted in significantly shorter unipedal stance time on both solid and compliant surfaces. On solid surface, OLST for each foot showed nuances that deserve mentioning. For the right foot, tactile pressure sensation and age were the main influencing factors determining standing time. Right-sided hand and foot dominance is known to increase with age and has been described in 94% of older adults (Kumar, Misra, Suman, Suar, & Mandal, 2010). As such, one can infer, for the dominant foot, tactile pressure sensation is “trained up” and prioritized over vibration sensation, as touch uses slow adapting receptors that deteriorates less with aging than the faster adapting receptors used for vibration sensation (Kenshalo, 1986; Perry, 2006; Wells et al., 2003). For the left foot, however, vibration sensation was the main determinant for unipedal stance on solid surface, but explained much less of the variance compared with the right foot. A possible explanation is that individuals use a more balanced collection of adapting strategies for the potentially weaker and less trained nondominant foot.
On compliant surface, tactile pressure sensation and age explained less of the ipsilateral unipedal stance variance than on solid surface. This down reweighting of proprioceptive input when support surface compliance increases is in line with prior studies (Patel, Fransson, Lush, & Gomez, 2008; Peterka, 2002; Schut, Engelhart, Pasma, Aarts, & Schouten, 2017). However, TPST was the only main factor for the right (predominant) foot, while age was the only main factor for the left foot. OLST is a known predictor for injurious fall accidents risk (Vellas et al., 1997). The foot dominance, the firmness of the standing surface, and the influence of age, tactile pressure, and vibration sensation seem to strongly predict OLST and, therefore, fall risk. In an earlier study, we could show that when the same subjects performed a BEEP regularly for 6 weeks, they improved their unipedal stance ability on solid surface by more than 30% and over 50% on compliant surface (Hafstrom et al., 2016). We have not yet, however, analyzed how tactile pressure and vibration sensation influenced the OLST improvements from the BEEP.
Fifth, the poorer the somatosensation, the more perceived balance difficulties the subjects expressed. Associations between somatosensation and DHI outcome is, to our knowledge, a novel finding. Vibration sensation and, less strongly, tactile pressure sensation were significantly correlated with higher DHI scores. In line with earlier studies, no significant associations between DHI and age could be shown (Ardic, Topuz, & Kara, 2006; Loughran, Gatehouse, Kishore, & Swan, 2006). Our results might reflect that older adults with an incipient slightly diminishing somatosensory input from the lower limbs can be cognitively aware and worried of this decline. The reduced sensitivity should eventually result in adequate reweighting with subsequent changes in postural control strategies (Peterka & Black, 1990). Many of the subjects (24%) in our study group had DHI scores indicating mild or moderate balance problems. This is in corroboration with many other studies showing that elderly often are worried about balance problems and “dizziness” with a consequential fear of falling (Delbaere, Close, Brodaty, Sachdev, & Lord, 2010; Nnodim & Yung, 2015). The DHI questionnaire originally was designed to quantify the handicapping effect of dizziness or balance problems imposed by vestibular system disease. It has, however, also been used for subjects with dizziness and balance problems of other origins (Ardic et al., 2006; Fielder, Denholm, Lyons, & Fielder, 1996; Jacobson & Newman, 1990). We did not investigate if TPSTs, VPTs, and age had had significant associations with the three different DHI domains representing functional, emotional, and physical aspects of dizziness and unsteadiness (Jacobson & Newman, 1990). Our results do, however, support that clinicians might consider reduced somatosensation as a cause for mild anxiety and depression problems in older adults presenting with balance difficulties. Thus, if a relatively healthy patient presents with balance problems, and has a normal physical and vestibular exam, health care professionals should be encouraged to administer the DHI questionnaire, perform at least the OLST test (eyes open on solid surface), and measure VPTs and TPSTs if possible. The rationale for this is that relatively greater impairment in vibratory sense and ability to maintain unipedal stance may identify those who are at a higher risk for falls (Richardson & Ashton-Miller, 1996).
One can question if our subjects are representative of the study objectives as they had volunteered for participating in a balance training intervention (Hafstrom et al., 2016). They considered themselves relatively healthy and appeared to be highly functioning, though many of them had several concurrent medical conditions. The range of their OLST with EO is in line with those in the literature for older adults (Morioka et al., 2012). Therefore, we decided to also include the two subjects with well-regulated diabetes mellitus and the one with neurofibromatosis. Thus, the cohort can be considered rather representative for a large group of active elderly. An important limitation to the study is that other factors than somatosensation and age, such as BMI, muscle strength, reaction time, vision, and pain, may have played a role for perceived and functional and balance, but were not analyzed in our study (Tiedemann, Sherrington, & Lord, 2005).
Conclusion
The findings reveal important links between somatosensation and several measures of postural stability and balance control in relatively healthy older adults. Impaired somatosensation sensation in the feet appears disadvantageous for the ability to balance on one foot and for mobility function as measured by BBS, speed walking, and Figure-8. Furthermore, significant associations between poor vibration sensation and subjective balance impairments is, to our knowledge, a novel finding. The results imply that somatosensation is important for perceived balance control as measured with DHI and that somatosensation in the feet might be more important than chronological aging for balance control. The findings have important implications when assessing balance impairment and impending fall risk in older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Part of this research was funded by a grant from the Acta Oto-Laryngologica foundation to the author.