
Abstract
Introduction
Urinary incontinence (UI) and nocturia are significant health problems for older adults; the consequences of which can have far-reaching impact on the health system. Whereas UI is “the complaint of any involuntary loss of urine” (Abrams et al., 2010, p. 213), nocturia is the need to wake during sleep to void (Bosch & Weiss, 2010). The prevalence of urinary dysfunction varies by gender and residential setting. For UI, the frequency ranges from 17% to 55% and 11% to 34% among community-dwelling older women and men, respectively (Thom, 1998), and is higher among residents in long-term care (Aggazzotti et al., 2000). Nocturia increases with age, with prevalence ranging from 74% to 77% among older women and 69% to 93% for older men (Bosch & Weiss, 2010). Waking more than twice/night is associated with lower health-related quality of life (QoL; Tikkinen et al., 2010). In the United States, the estimated direct annual associated costs are US$16.3 billion (Wilson, Brown, Shin, Luc, & Subak, 2001) and US$1.5 billion (Holm-Larsen, 2014) for UI and nocturia, respectively. Many of these costs result from falls and fractures, as both incontinence and nocturia increase risk of these injuries (Brown et al., 2000). Specifically, UI (Johansson, Hellstrom, Ekelund, & Milsom, 1996) and nocturia (Asplund, 2006) are risk factors for hip fracture.
Overall control of continence is an interplay between the urethra and the detrusor muscle of the bladder; the pathophysiology of urinary dysfunction can be neurogenic (Ginsberg, 2013) and/or myogenic (Brading, 1997) in origin. Neurogenic urinary dysfunction is commonly a result of damage or disease of the central nervous system that leads to inability of the urethral sphincter to adjust when bladder pressure increases (Ginsberg, 2013). In contrast, myogenic urinary dysfunction results from structural changes to the detrusor smooth muscle leading to increased nerve activity and bladder overactivity (Brading, 1997).
Following surgery, there may be increased risk of urinary dysfunction, possibly due to indwelling catheters (Sorbye & Grue, 2013), but there are other likely causes such as increasing age, health status, and other surgical-related factors (Chiarelli, Byles, Parkinson, & Gibson, 2006; Palmer, Baumgarten, Langenberg, & Carson, 2002). Urinary dysfunction may persist beyond the post-acute period (Chiarelli et al., 2006), placing individuals at risk of further fall-related injury (Chiarelli, Mackenzie, & Osmotherly, 2009), sleep fragmentation (Asplund, 2004), and reduced QoL (Dubeau, Simon, & Morris, 2006). Despite this, UI and nocturia are frequently underinvestigated and managed (Edwards et al., 2011). Contributing to the low management rates is the associated stigma that creates barriers for older adults to seek medical help for their symptoms (Wang et al., 2014). This gap in assessment and reluctance to discuss urinary problems can lead to social isolation (Yip et al., 2013), and instigate or amplify a spiral of mobility loss, with consequences for QoL.
In this study, the assessment of urinary dysfunction was included as part of a comprehensive geriatric assessment to improve mobility among community-dwelling older adults after hip fracture (Cook et al., 2011). Specifically, this article reports the results from the evaluation and management of UI and nocturia as part of a geriatric clinic for older adults after hip fracture. It also describes the associations between UI, nocturia, and QoL.
Method
Participants
This was an analysis of a secondary outcome from a randomized controlled trial testing a follow-up clinic for older adults after hip fracture in Vancouver, Canada (Cook et al., 2011). The study included 53 community-dwelling men and women aged 65 years or older from Metro Vancouver with a recent hip fracture (3-12 months). The exclusion criteria included older adults who, prior to the fracture, were unable to walk 10 m, diagnosed with any type of dementia, and/or older adults who upon hospital discharge moved to a residential care facility. Approval to conduct the study was obtained from the university and local hospital institutional review boards. Study participants provided written informed consent prior to taking part in the study.
Recruitment, Randomization, and Measurement Time Points
Clinicians from three collaborating teaching hospitals assisted with participant recruitment. After enrollment into the study, a registered physiotherapist assessed participants, and then the research coordinator used a web-based system to determine participant group allocation. Randomization was stratified by gender and hospital site, and an independent academic statistical company generated the sequence for randomization to maintain allocation concealment and reduce the risk of bias. The physiotherapist also assessed outcomes again at 6 and 12 months.
Intervention
The full protocol for this study and a description of the intervention is provided elsewhere (Cook et al., 2011). In summary, participants randomized to the intervention (B4) were provided usual care (UC) and a comprehensive geriatric assessment (Panel et al., 2011). The focus was on key elements deemed important and relevant to mobility recovery after hip fracture including, bone health, balance, cognition, and continence. Following the assessment by the geriatrician, participants were offered personalized clinical management strategies. One area for intervention addressed concerns with UI and/or nocturia. If appropriate, participants were referred to a continence nurse for management. Control participants followed the UC pathway including follow-up with their surgeon and family physician, and were offered the follow-up clinic at the end of their participation in the study.
Continence and Nocturia Questionnaire
Participants were asked questions related to UI (Huang et al., 2007) and nocturia (Vaughan et al., 2010) based on previous literature. The questions (and possible responses) for continence are located in Table 1.
UC and Nocturia Questions Asked of Participants at Three Times Points Over the 12 Months (Baseline, 6 Months, and 12 Months).

Note. UC = urinary continence.
QoL
The ICEpop CAPability measure for Older people (ICECAP-O; Coast et al., 2008), a capability and well-being measure developed for use with older adults, was used to capture perceptions of QoL.
Descriptive Measures
Date of birth, gender, number of chronic conditions, and time since fracture were recorded. Height and weight was measured; body mass index (BMI) was calculated as weight (kg)/height (m2).
Statistical Analysis
Participant characteristics were described using mean (standard deviation) or median (interquartile range [IQR]) if data were skewed; categorical and ordinal data were reported as counts and proportions. Point biserial correlations were used to explore the relation between presence of UI and nocturia and overall QoL (ICECAP-O index score) at the three time points. In addition, one-sided Fisher’s exact test was used to explore associations with QoL and the degree of UI frequency and severity, and the number of nightly nocturia occurrences, using Stata v13 (StataCorp, 2015).
Results
Fifty-three participants were recruited to the study: 26 participants were randomized to the B4 group and 27 participants to UC group (Figure 1). During the study, one B4 participant was lost to follow-up and one UC participant discontinued participation before the final assessment time point. There were missing data from one B4 participant and two UC participants: therefore, there were 24 participants in each group who contributed data to these analyses.
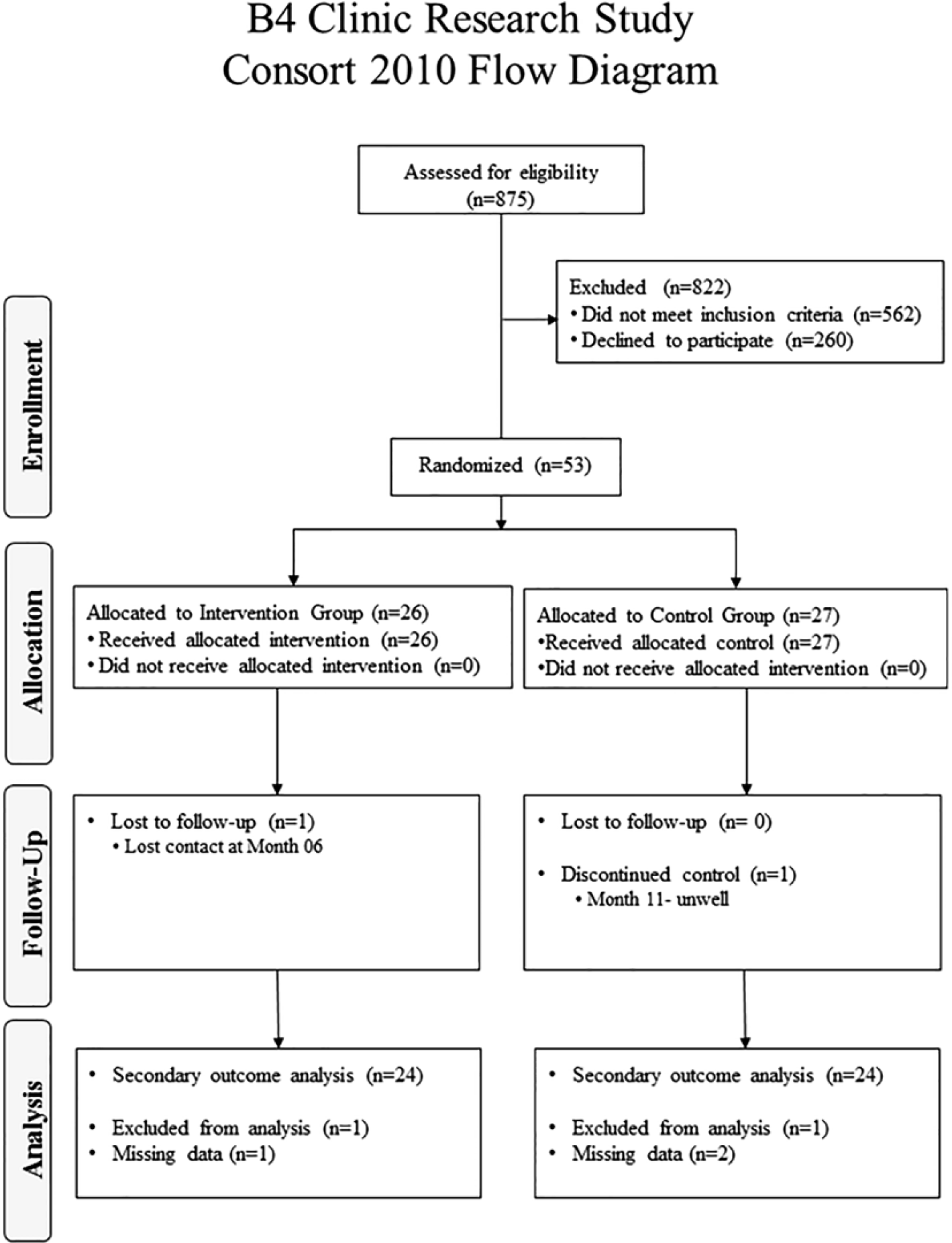
Flow diagram for the B4 study continence variables.
Study participants had an average (SD) age of 79.6 (7.9) years (range = 65-98 years). There were 17 out of 48 (35%) men, they had a median (IQR) BMI of 25.5 (4.8) and were diagnosed with a median (IQR) of 3 (3.5) chronic conditions. At baseline, 21 out of 48 (43.7%) of all study participants reported UI, including nine out of 24 (37.5%) from the B4 group and 12 out of 24 (50%) from the UC group. There were five intervention participants who reported UI at baseline, but did not report UI at midpoint or final assessment. At final assessment, there were four B4 participants with two new cases for a total of six B4 participants who reported UI. There were 10 out of 12 UC participants (who reported UI at baseline) with two new cases, for a total of 12 participants. In the UC group, there were three participants who reported UI at baseline and final assessment, but did not report UI at midpoint. Most study participants reported nocturia at baseline; the number and relative percentage of participants reporting nocturia were similar between the groups and did not change over the course of the study. Based on a review of B4 participants’ charts, four B4 participants were offered a referral to a continence nurse. Table 2 provides a summary of variables of interest across three time points.
Continence Outcomes by Group at Three Time Points.

Note. There were 48 participants who contributed data to these analyses, including 24 participants in each group (control and intervention groups). UC = usual care; UI = urinary incontinence.
Using a one-sided Fisher’s exact test, no statistically significant differences between groups for UI at midpoint (.125, CI = [0.00, 0.360], p = .247) or final assessment (.25, CI = [0.00, 0.515], p = .068) were found. There were no statistically significant differences between groups for the presence of nocturia at midpoint (.042, CI = [0.00, 0.262], p = .500) or final assessment (.083, CI = [0.00, 0.293], p = .350).
A statistically significant association between the presence of UI and QoL (r = −.36; p = .016) was found only at midpoint. Negative coefficients were interpreted as participants who did not experience the presence of UI and had higher QoL (ICECAP-O) scores. There were no significant associations between nocturia and QoL (Table 3).
Associations Between Presence of Urinary Incontinence and Nocturia With Quality of Life Using Point Biserial Correlation Coefficients at Three Time Points, Regardless of Group Allocation.
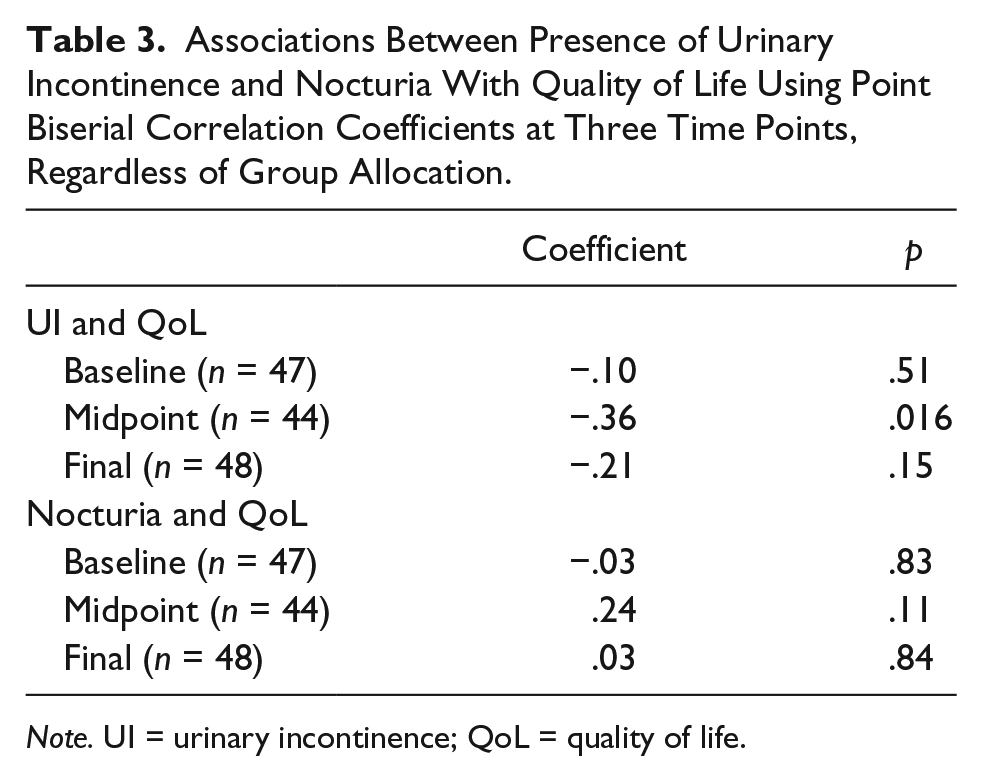
Note. UI = urinary incontinence; QoL = quality of life.
Discussion
The consequences of UI and nocturia can be life changing, and pose negative consequences on physical, social, and emotional well-being (Ramage-Morin & Gilmour, 2013). Older adults with UI are more susceptible to health problems such as falls (Chiarelli et al., 2009), fractures (Asplund, 2006; Brown et al., 2000; Johansson et al., 1996), and may have higher rates of admission to a residential care facility (Thom, Haan, & Van Den Eeden, 1997). At baseline, more than two of every five participants reported UI, and most participants experienced nocturia to varying degrees. A significant statistical association between UI and lower QoL was noted at midpoint. However, there was no difference between groups for urinary-related impairments; this may be due to the small sample size, the intervention, and/or the stigma associated with this health concern, which may have led some participants to underreport their symptoms to research personnel. These data highlight that the identification and management of UI and nocturia remain a major concern among older adults with hip fracture.
Stigma associated with UI (Wang et al., 2014) might prevent older adults from seeking help and taking part in out-of-home activities, leading to increased risk of social isolation, loneliness, and decreased independence (Ramage-Morin & Gilmour, 2013). Many older adults believe that UI and nocturia are a normal part of aging and, therefore, avoid discussing the topic with their doctor (Umlauf, Goode, & Burgio, 1996). Thus, UI is frequently underreported. Despite the fact that UI and nocturia can affect older adults’ health, QoL, and well-being, there have been few studies that focused on addressing UI-related health concerns after hip fracture.
Current evidence suggests a number of ways to manage UI and nocturia including lifestyle advice, physical therapy and pelvic muscle strengthening (Baigis-Smith, Smith, Rose, & Newman, 1989), biofeedback, scheduled voiding, behavioral therapies, medication, and surgical procedures (Abrams et al., 2010). Studies have found that physical therapy and behavioral therapy are effective treatments for UI and nocturia for older adults (Aslan, Komurcu, Beji, & Yalcin, 2008). Study participants in the B4 group were assessed by a physiotherapist who prescribed individualized balance and strength exercises to improve balance, gait, and vestibular function. A recent systematic review noted that a nonspecific exercise program does not change UI symptoms (Bo & Herbert, 2013), which perhaps speaks to exercise specificity and requires that pelvic floor exercises be included within an overall balance and strength routine. Targeted exercise may have benefits beyond addressing bladder retraining. For example, engaging in a regular physical activity program that includes balance and core strengthening could also provide additional safeguards for fall prevention. In addition, studies on healthy community-dwelling older adults found that maintaining an active lifestyle can reduce the risk of developing UI (Bo & Herbert, 2013). For nocturia, there has been limited investigation; however, a small study (n = 30 men) noted a decrease in symptoms and better sleep associated with a walking program (Sugaya et al., 2007).
There are limitations noted with this study. First, this was a small study and the results may not be generalizable to all older adults with hip fracture. Second, participants were community dwelling, which do not represent the full spectrum of older adults with hip fracture. Third, the study was underpowered to detect any changes in UI and nocturia between groups. Other limitations include using a self-report measure to detect participants’ impairments in urinary function and not enquiring about urinary function prior to the fracture. Finally, the study did not document individual recommendations to participants or measure study participant uptake of recommendations from the clinic intervention outside of clinician visit frequency and type. Despite these limitations, the importance of this work is that it highlights the moderate to high prevalence of UI and nocturia in a group of older adults after hip fracture—already a vulnerable group at greater risk of future injuries. These issues must be addressed, including minimizing associated stigma because of the increased risk of falls and fractures, social isolation, and potential institutionalization that can ensue if continence is not managed.
Identifying and managing UI and nocturia (and their consequences) early are key to mitigating health risks, reducing risk of falls and fractures, and potentially improving QoL. As this can be a sensitive topic for some people, strategies are required to address psychosocial concerns for urological health in older adults to make management more approachable for this and other at-risk populations.
Footnotes
Acknowledgements
The authors extend sincere thanks to their study participants for their generosity with their time.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge financial support from the Canadian Institutes of Health Research (CIHR) grant (FRN 99051) and career award support for Dr. Ashe from CIHR, the Michael Smith Foundation for Health Research, and the Canada Research Chairs Program.