
Abstract
Hearing loss may affect critical domains of health and functioning in older adults. This article describes the rationale and design of the Studying Multiple Outcomes After Aural Rehabilitative Treatment (SMART) study, which was developed to determine to what extent current hearing rehabilitative therapies could mitigate the effects of hearing loss on health outcomes. One hundred and forty-five patients ≥50 years receiving hearing aids (HA) or cochlear implants (CI) were recruited from the Johns Hopkins Department of Otolaryngology-HNS. A standardized outcome battery was administered to assess cognitive, social, mental, and physical functioning. Of the 145 participants aged 50 to 94.9 years who completed baseline evaluations, CI participants had significantly greater loneliness, social isolation, and poorer hearing and communicative function compared with HA participants. This study showed that standardized measures of health-related outcomes commonly used in gerontology appear sensitive to hearing impairment and are feasible to implement in clinical studies of hearing loss.
Introduction
Hearing loss is a highly prevalent chronic health condition that affects nearly two thirds of adults aged 70 years and older in the United States (Lin, Thorpe, Gordon-Salant, & Ferrucci, 2011). Studies have demonstrated that hearing loss is independently associated with social isolation (Kramer, Kapteyn, Kuik, & Deeg, 2002; Strawbridge, Wallhagen, Shema, & Kaplan, 2000), poorer health-related quality of life (Chia et al., 2007; Ciorba, Bianchini, Pelucchi, & Pastore, 2012; Dalton et al., 2003), decreased cognitive functioning (Lin, 2011; Lin, Thorpe, et al., 2011; Lin et al., 2013), incident dementia (Lin, Metter, et al., 2011), poorer physical functioning as indicated by increased odds of falling (Lin & Ferrucci, 2012), reduced walking speed (Li, Simonsick, Ferrucci, & Lin, 2013; Viljanen et al., 2009), and hospitalization (Genther, Frick, Chen, Betz, & Lin, 2013). Given the increasing prevalence of hearing loss with the aging of the population, understanding whether hearing rehabilitative treatments could affect health-related domains that are known to be associated with hearing loss in epidemiological studies is important.
The Studying Multiple Outcomes After Aural Rehabilitative Treatment (SMART) study was initiated in 2011 at Johns Hopkins to evaluate the impact of hearing treatment on a broad range of functional domains in older adults and to serve as a model for future studies and clinical trials. The primary objective of this study was to evaluate the cognitive functioning of individuals with hearing loss before and after intervention with a hearing aid (HA) or cochlear implant (CI) using a standardized neurocognitive battery. In addition, we measured social, communicative, mental, and physical functioning of individuals with hearing loss before and after HA and CI intervention. We hypothesized that HA and CI use are associated with improvements from pre- to postintervention in cognitive and physical functioning, social isolation, health-related quality of life, communication, and depressive symptoms.
In this article, we provide a description of the rationale and design of the SMART Study, including cohort characteristics, recruitment methods, outcome assessment, as well as preliminary results from baseline data. A website providing our protocols and test forms has been designed to facilitate broader use of these outcome measures among researchers in otology and audiology (http://www.linresearch.org/for-researchers.html).
Method
Study Participants
We recruited patients from the Johns Hopkins Department of Otolaryngology-HNS who presented for evaluation for HA or CI. Patients who fulfilled the following criteria were eligible for the study: (a) ≥50 years of age, (b) English-speaking, (c) receiving a HA for the first time (or with minimal [<1 hr/day] prior use) or receiving a first CI, (d) diagnosed with postlingual hearing loss, (e) aural-oral verbal communication as primary communication modality, and (f) signed informed consent to participate in baseline and subsequent follow-up assessments. We were not able to characterize the exact duration of hearing loss as it is rarely possible for participants to determine the exact onset of their hearing loss. Participants were asked to complete three study visits: (a) baseline evaluation, (b) 6-month follow-up, and (c) 12-month follow-up. Baseline neurocognitive evaluations took place before receiving HA fitting or CI activation or on the day of HA/CI issuance. Baseline assessments for functional questionnaires were administered before or within 1 to 2 weeks of HA or CI issuance. Questionnaire data from 10 participants were dropped from analysis due to late responses.
From August 5, 2011, to January 17, 2014, we enrolled 145 participants (out of 564 eligible patients who presented to the Johns Hopkins Listening Center) in the study. Most common reasons for not participating in the study included lack of interest, time constraints, transportation limitations, and feasibility of returning for follow-up visits. All study participants were provided with a parking voucher (US$8 value) and a meal voucher (up to US$10 value) at each study visit. Study participants also received an additional 1 year extended warranty on their hearing device, provided by the respective HA (Phonak, Oticon, Starkey, Unitron, Widex) or CI (Cochlear America, MED-EL Corp., Advanced Bionics) companies. All study procedures were reviewed and approved by the Johns Hopkins Institutional Review Board (Baltimore, Maryland; Study Number: NA_00045877).
Treatment of Hearing Loss
Study participants received HA or CI according to routine clinical care at Johns Hopkins. For individuals fitted with HAs, decisions as to type of technology, unilateral versus bilateral fitting, and fitting procedures were determined by the individual audiologist and patient. CI surgeries and pre- and postoperative fitting and programming were performed by the staff of the Johns Hopkins Listening Center. Decisions as to which CI technology to use and fitting procedures were made individually between the implant audiologist and the patient.
Cognitive and Functional Assessments
Neurocognitive testing was performed by an experienced psychometrist accustomed to working with older adults and using a standardized protocol and neurocognitive battery, as presented in Table 1, Part A. Due to length of the neurocognitive testing and the need to schedule this testing with a dedicated psychometrist, only 74 individuals completed the neurocognitive battery before or on the day of HA and CI issuance. There were no differences in demographic characteristics between these two groups across any of the variables listed in Table 2 (data not shown). All tests were presented using stimulus booklets with written and verbal instructions, and all tests were specifically chosen to be nonauditory tests of cognition to avoid confounding by audibility. Age-adjusted z scores were generated for all neurocognitive exams (except for the National Adult Reading Test) to differentiate between cognitively impaired individuals and noncognitively impaired individuals. An individual was considered cognitively impaired if at least two of the six z scores were below −2.0 or at least three z scores were below −1.5. Social, communicative, and mental and physical health functioning were assessed using self-administered questionnaires at baseline and at 6 and 12 months after intervention for all participants (Table 1, Part B).
Neurocognitive and Other Functional Assessments, SMART Study.

Note. Refer to http://www.linresearch.org/for-researchers.html, for links to references, coding forms, and scoring instructions. SMART = Studying Multiple Outcomes After Aural Rehabilitative Treatment. PCS = Physical Component Score; MCS = Mental Component Score; ND = network diversity; PSN = people in social network; SF-36 = 36-item short form; IQ = intelligence quotient. UCLA = University of California, Los Angeles.
Score interpretation is based on z scores (derived from a normative table that is used to compare z scores, t scores, and percentiles). Cognitive impairment is defined by the following criteria: (a) at least two z scores are below −2.0 or (b) at least three z scores are below −1.5.
For ages <70: Total score ≤24 is considered cognitively impaired.
Indicates time for discontinuation of task.
Demographic Characteristics of HA and CI Participants, SMART Study.

Note. Mild hearing loss: PTA >25 and ≤40 dB. Moderate hearing loss: PTA >40 and ≤60 dB. Severe or greater hearing loss: PTA >60 dB. HA = hearing aids; CI = cochlear implants; SMART = Studying Multiple Outcomes After Aural Rehabilitative Treatment; IQR = interquartile range; PTA = Pure Tone Average.
PTA (measurement of hearing ability).
Statistical Analysis
Data were collected and managed using REDCap electronic data capture tools hosted at Johns Hopkins University (Harris et al., 2009). Continuous variables are presented as median (interquartile range [IQR]) and summarized using the Wilcoxon rank sum test, and categorical variables were compared using Fisher’s exact test. Significance testing for all analyses was two-sided with a Type I error of 0.05. Statistical analyses and graphs were generated using STATA 12 (STATA Corp, College Station, TX) and R Version 3.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
The demographic characteristics of the SMART study cohort are summarized in Table 2. Of the 145 participants aged 50 to 94.9 years (median = 70.3, IQR = 63.7-78.4) who completed baseline evaluations, 81 were receiving HAs and 64 were receiving a CI. Participants were primarily White (89.7%) with some college education or greater (81.4%). With the exception of hearing loss severity, education, and employment status, we did not observe any differences in demographic characteristics comparing HA and CI participants.
Table 3 shows results from baseline neurocognitive evaluations. Compared with CI participants, HA participants scored higher on the Benton Visual Retention Test (BVRT; p < .01), the Delis–Kaplan executive function system (D-KEFS) verbal fluency test (p = .01), and the Salthouse Comparison Test (p < .01). Higher scores on these three tests suggest higher level of cognitive functioning. Eight participants (HA = 4, CI = 4) scored either below −2.0 on two of the six z scores (excluding the National Adult Reading Test) or below −1.5 on at least three z scores and thus were considered cognitively impaired. The median Verbal intelligence quotient (IQ) among all participants was 107.3 (IQR = 97.5-114.5) with no differences observed between the two treatment groups (p = .17).
Neurocognitive Evaluation Outcomes Comparing HA and CI Participants.

Note. A total of 71 participants were excluded in this analysis as they received treatment prior to the date of cognitive testing. HA = hearing aids; CI = cochlear implants; SMART = Studying Multiple Outcomes After Aural Rehabilitative Treatment; NART = National Adult Reading Test; IQR = interquartile range; FCSRT = free and cued selective reminding test; D-KEFS = Delis–Kaplan executive function system; IQ = intelligence quotient.
Calculated using the following equation: Verbal IQ = 128.7 −(0.89 × number incorrect on the NART).
As displayed in Table 4, University of California, Los Angeles (UCLA) Loneliness Scale scores were lower in HA participants (median = 33, IQR = 27-39) relative to CI participants (median = 41, IQR = 32.5-49), with higher scores reflecting greater degree of loneliness. CI participants also reported greater degree of hearing handicap and functional impact on the Hearing Handicap Inventory for the Elderly-S (HHIE-S), with nearly 58% (n = 37) of CI participants indicated the presence of severe emotional and situational handicap due to their hearing impairment, more than double the rate reported in HA participants (23.5%, n = 19). CI participants also had higher scores on the revised Quantified Denver Scale (QDS) of Communication Function (median = 18, IQR = 14-21) relative to HA participants (median = 13, IQR = 8-16.5; p < .01), with higher scores indicating greater difficulties in communication due to hearing loss.
Social, Communicative, and Functional Outcomes Comparing HA and CI Participants.

Note. A total of 10 participants were excluded in this analysis due to questionnaires returned after the cutoff date. HA = hearing aids; CI = cochlear implants; IQR = interquartile range; GDS = Geriatric Depression Scale; HHIE = Hearing Handicap Inventory for the elderly; QDS = Quantified Denver Scale; UCLA = University of California, Los Angeles.
Higher scores indicate greater degree of loneliness; 30-40 = normal range; >60 suggests severe loneliness.
Higher scores indicate greater degree of depression; <5 suggests no depression, ≥5 and ≤ 10 suggests mild depression, ≥11 suggests severe depression.
Higher scores indicate better physical health functioning; U.S. population norm: M = 50, SD = 9.95, range = [4-71].
Higher scores indicate better mental health functioning; U.S. population norm: M = 50.0, SD = 10.0, range = [2-74].
Higher scores indicate number of social roles that the participant has regular contact (i.e., at least once every 2 weeks) with at least one person.
Higher scores indicate greater total number of people with whom the participant had regular contact (i.e., at least once every 2 weeks).
Higher scores indicate greater degree of hearing handicap and functional impact, Scores 0 to 8 indicate no handicap, Scores 10 to 24 indicate mild to moderate Handicap, and Scores 26 to 40 indicate significant handicap.
Higher scores indicate greater communication difficulties in adults with hearing impairment.
Figure 1 demonstrates exploratory graphical analyses of the association between degree of hearing impairment and neurocognitive scores by treatment group. A general downward trend was observed between hearing thresholds and cognitive performance on the BVRT, free and cued selective reminding test (FCSRT), D-KEFS Stroop Test, and the Salthouse Comparison Test. Overall, neurocognitive exam performance declined with greater hearing loss. As shown in Figure 2, scores on the UCLA Loneliness Scale, Geriatric Depression Scale (GDS), HHIE, and QDS were higher with greater levels of hearing loss, with higher scores indicating poorer psychosocial functioning. Figure 2 also demonstrates that individuals with greater hearing loss reported having fewer total number of people with whom the participant had regular contact as measured by the Social Network Index. Importantly, these graphical analyses are not adjusted for confounders and are meant to be only exploratory in nature for presenting the characteristics of the baseline cohort and the study design.
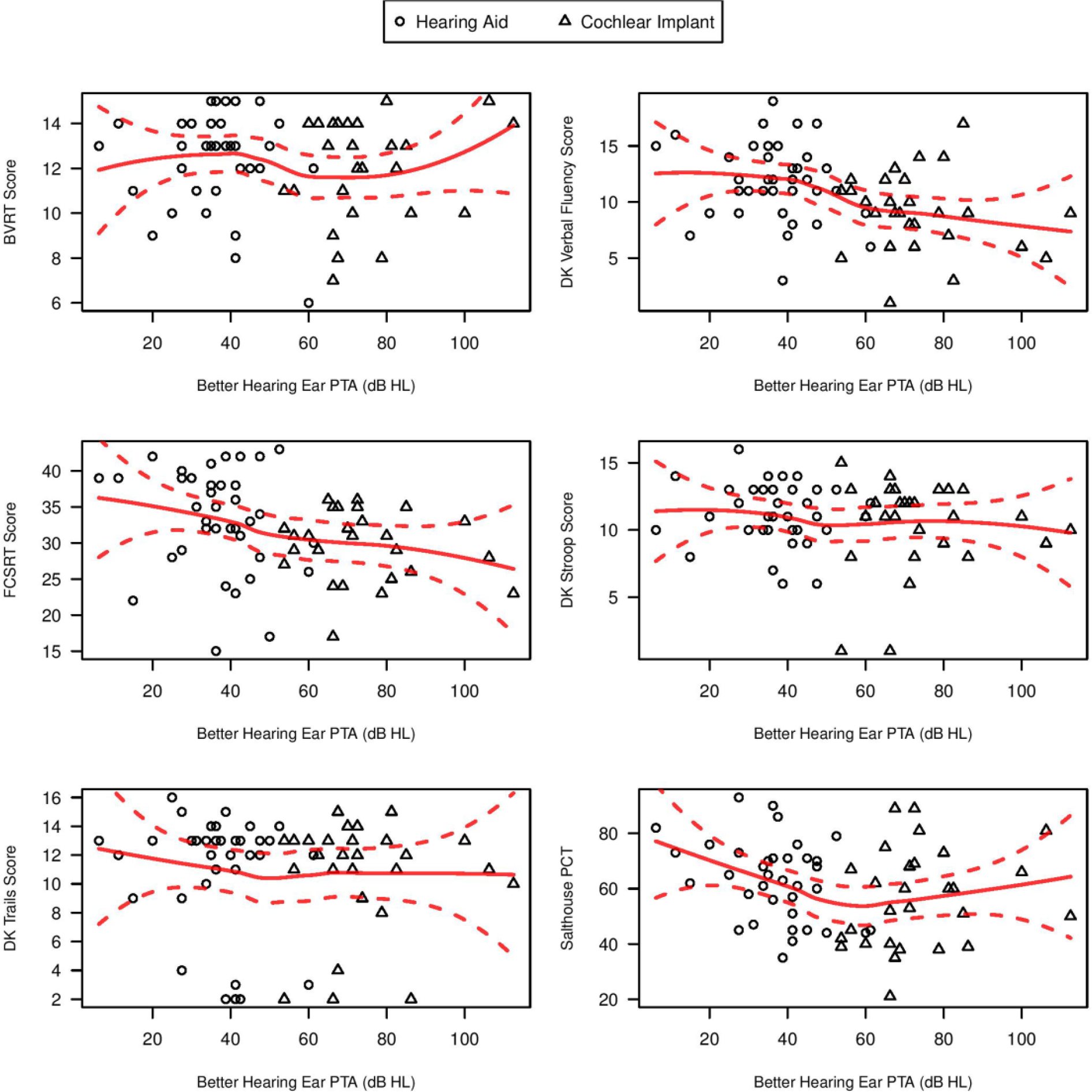
Exploratory graphical analyses of hearing thresholds with baseline neurocognitive test scores.
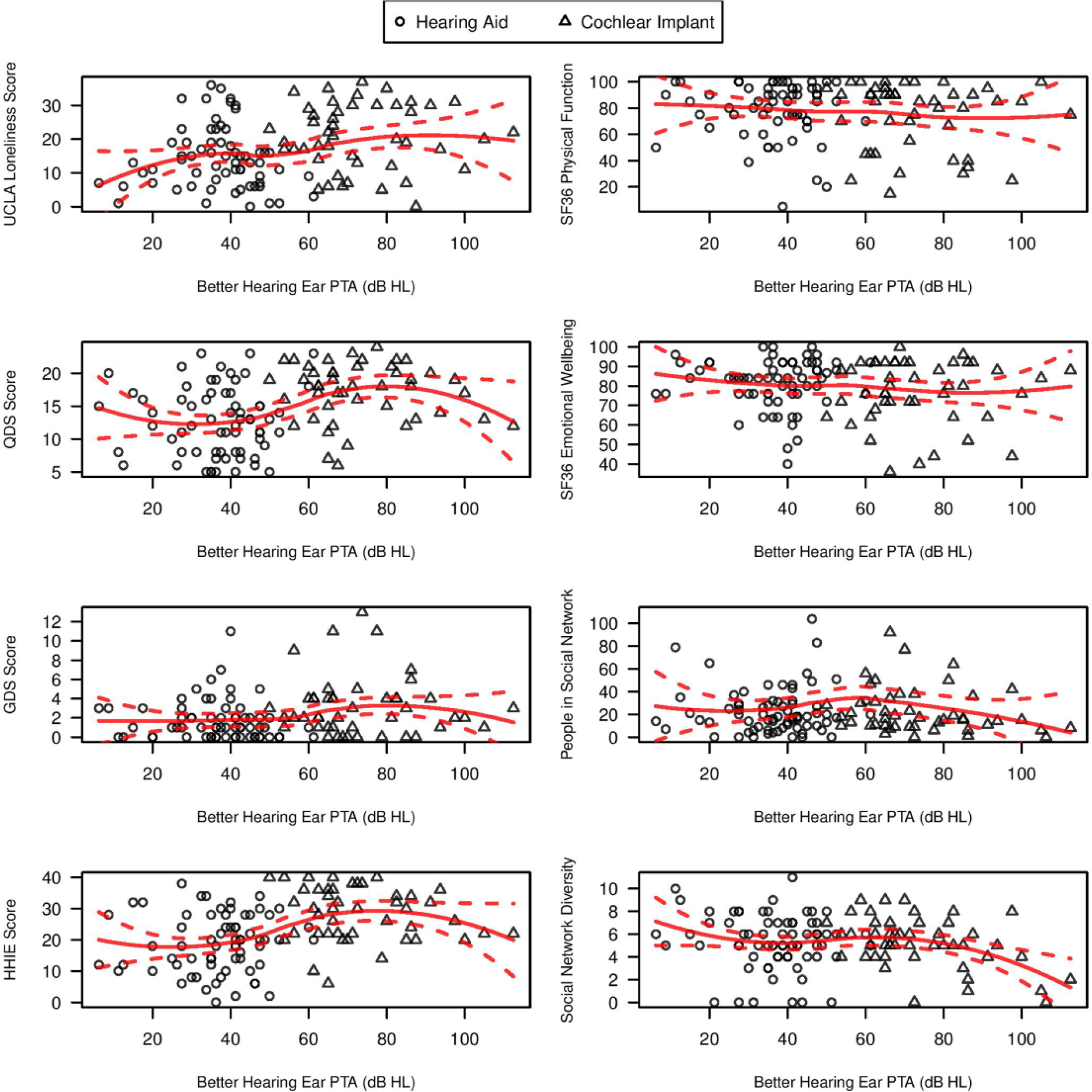
Exploratory graphical analyses of hearing thresholds with baseline functional test scores.
Discussion
There is a limited understanding of the impact of hearing loss treatment on domains of health and functioning in older adults beyond speech and communication. In the current report, we provide an overview of the design and study procedures of the SMART study that will investigate changes in the health functioning of older adults from before to after hearing loss treatment. Our baseline results support the feasibility of gathering diverse functional outcome data on older adults receiving treatment for hearing loss. Importantly, including such outcome measures in future studies investigating the benefits of hearing loss treatment (e.g., bilateral vs. unilateral cochlear implantation) may be critical to establishing the broader impact and importance of hearing rehabilitative therapies in the context of other medical treatments.
Previous studies have found an association between HA use and improvements from pre- to postintervention in health-related quality of life in adults with hearing loss. A randomized controlled trial by Mulrow et al. (1990) found that participants who received HA treatment had improvements in depression (as measured by the GDS), lower social and emotional dysfunction (as measured by QDS), and lower communication dysfunction (as measured by HHIE) compared with participants who were placed on waiting list for treatment. Other studies also found that HA use was associated with reduced emotional and social impacts of hearing loss as measured by the HHIE (Humes, Garner, Wilson, & Barlow, 2001; Stark & Hickson, 2004; Yueh et al., 2001). One study using the 36-item short form (SF-36) showed improvements in social functioning post-HA fitting compared with pre-HA fitting status (Joore, Potjewijd, Timmerman, & Auteunis, 2002). Compared with previous studies on HA outcomes in older adults, the SMART study examines both cognitive and physical functioning as additional and important factors in the assessment of health-related quality of life after hearing rehabilitation.
One recent study also found quality of life improvements after cochlear implantation in 28 prelingually deafened adults as measured by the Glasgow Benefit Inventory and Health Utility Index (Straatman, Huinck, Langereis, Snik, & Mulder, 2014). However, there is currently limited research on the effect of cochlear implantation on broad health-related outcomes in older adults. Thus, a major strength of the SMART study is the inclusion of CI users in determining pre-and posthearing treatment outcomes. In addition, the SMART study uses surveys consistent with those utilized by previous studies that have looked at the effect of hearing treatment on quality of life.
The design of the SMART study has limitations. In particular, the study consisted of a convenience sample of participants presenting for routine clinical care at Johns Hopkins. With many participants living >1 to 2 hr from Johns Hopkins, we did not have the resources that would be required to provide transportation costs and other financial incentives needed to bring all study participants in for a dedicated baseline study visit (i.e., only 145 of 564 potentially eligible participants enrolled).Therefore, not all participants were able to have neurocognitive testing performed before or on the day of CI or HA issuance (71 of 145 participants), and some baseline assessments for functional questionnaires took place shortly after CI or HA issuance. We do not believe this limitation would substantively bias our baseline results given that even participants with baseline study visits performed within 1 to 2 weeks of CI activation or HA issuance would have had minimal experience with their device so as to affect baseline outcomes which query function over the preceding month.
Another limitation of the SMART study is our inability to infer causality of treatment with HA or CI on any changes in neurocognitive or functional outcomes that may be observed. However, results observed in the SMART study will be informative for a definitive clinical trial that is currently being planned in conjunction with the National Institute on Aging. The overall design of the SMART study and the outcome measures that are currently being implemented will also help inform other hearing clinical studies.
Given the increasing prevalence of hearing loss and the consistently low prevalence of HA use, it is important to examine a broad range of outcomes to better demonstrate how hearing treatments can mitigate downstream effects of hearing loss. Through the SMART study, we are able to examine a comprehensive list of health-related outcomes in adults undergoing hearing treatments. Findings from this study could provide a better understanding of the potential impact of aural rehabilitative treatments on the functioning and health status of older adults.
Footnotes
Acknowledgements
The authors thank the following companies for providing a 1-year extended warranty on SMART (Studying Multiple Outcomes After Aural Rehabilitative Treatment) study participants’ hearing devices: Phonak, Oticon, Starkey, Unitron, Widex, Cochlear America, MED-EL Corp., and Advanced Bionics.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Lin reports being a consultant to Cochlear Ltd, on the Scientific Advisory Board of Pfizer and Autifony, and serving as a speaker for Amplifon and MED-EL. No other author reported any disclosures.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant 1K23DC011279 from the National Institute on Deafness and Other Communication Disorders, with further funding from the Triological Society and the American College of Surgeons through a clinician scientist award, and from the Eleanor Schwartz Charitable Foundation.