
Abstract
Introduction
Convergence insufficiency (CI) is a neuromuscular deficiency of binocular eye alignment (Grisham, 1988) characterized by a reduction in the degree of convergence or the inability to maintain the necessary convergence of the eyes on a near target while keeping this target single, clear, and comfortable to look at. CI is associated with a wide range of symptoms, such as eyestrain, headaches, blurred vision, fatigue, sleepiness, difficulty concentrating while reading, and double vision (Lavrich, 2010). Two earlier studies have reported that a clinical diagnosis of CI was more frequent in patients with Parkinson’s disease (PD; Lepore, 2006; Repka, Claro, Loupe, & Reich, 1996). More recently, it was reported that both CI-related symptomatology and a clinical diagnosis of CI were more prevalent in individuals with versus without PD (Irving et al., 2016).
The therapy of choice for CI consists of orthoptic treatment (OT; Scheiman & Wick, 2014). Its success rate is high (Grisham, 1988) and has been documented in pediatric (Scheiman, Mitchell, Cotter, Kulp, Rouse, et al., 2005), young adult (Scheiman, Mitchell, Cotter, Kulp, Cooper, et al., 2005), and older adult populations (Birnbaum, Soden, Cohen, 1999; Wick, 1977). Unfortunately, OT for CI has never been evaluated in PD, even if it has been suggested that “the effectiveness of vergence exercises to improve convergence” in these patients seemed warranted (Almer, Klein, Marsh, Gerstenhaber, & Repka, 2012).
We present a case series of two older adults with PD in whom OT decreased the signs and symptoms of CI.
Method
In an earlier study investigating CI in PD, 25 (31.3%) of 80 PD participants received a diagnosis of symptomatic CI and were offered OT. Seven participants accepted therapy, three abandoned therapy, and two were lost to follow-up. This report thus presents a case series of the two participants who completed OT for their symptomatic CI. The protocol was approved by the research ethics committee of our institutions and participants signed an informed consent form.
Positive symptomatology was based on a global score of ≥21 on the Convergence Insufficiency Symptom Survey (CISS-15) questionnaire (Rouse et al., 2004; Scheiman, Mitchell, Cotter, Kulp, Cooper, et al., 2005). The CISS-15 measures the frequency and severity of CI-type symptoms and has been shown to be a valid and reliable instrument for CI treatment outcomes (Rouse et al., 2004). A positive diagnosis of CI was based on the following criteria (Rouse et al., 2004): (a) exophoria at near at least 4 prism diopters (Δ) greater than at far, (b) receded near point of convergence (NPC) break of ≥6 cm, and (c) insufficient positive fusional vergences (PFV) at near (see Figure 1 for explanations).
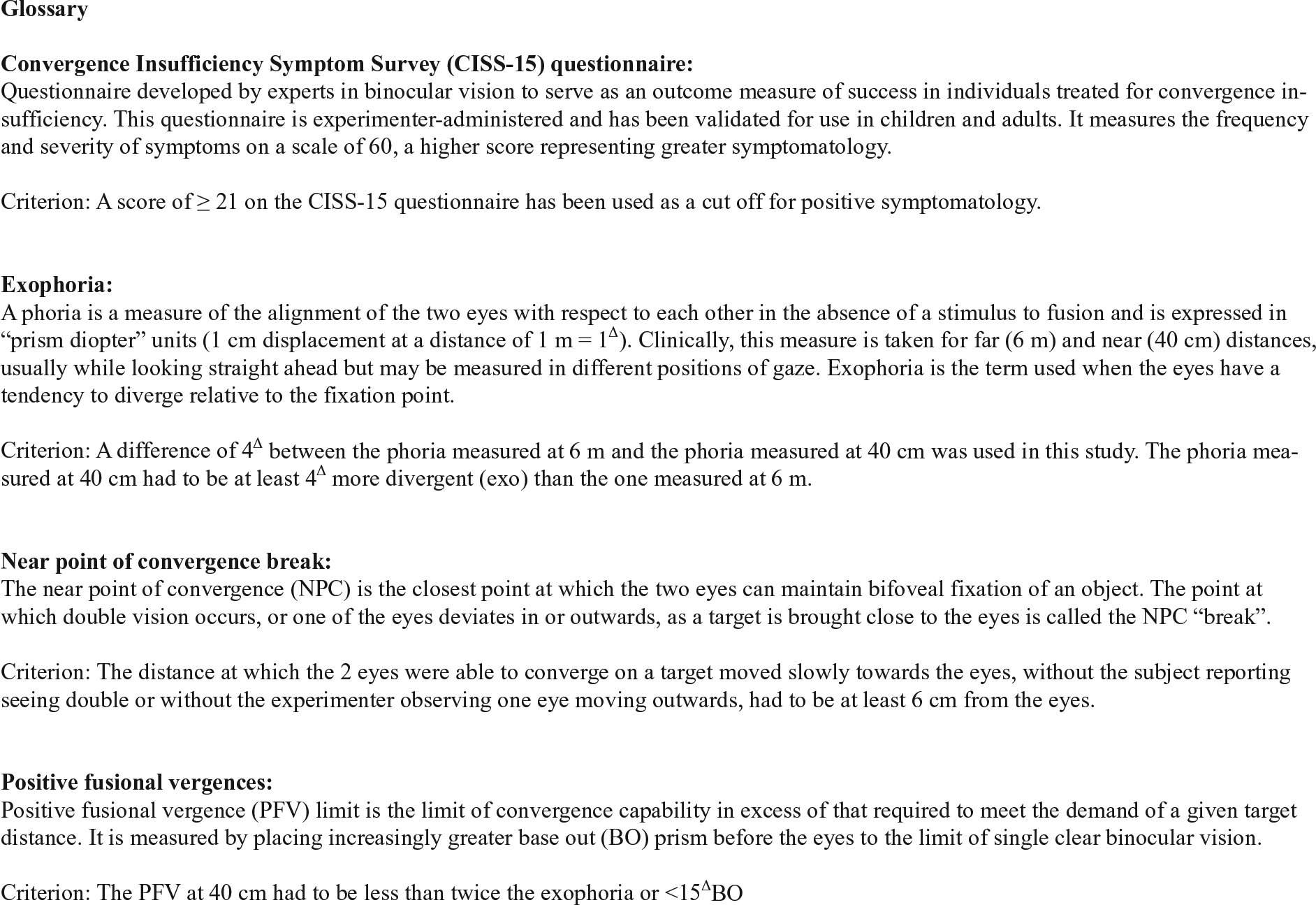
Glossary of terms and explanation of criteria used to define convergence insufficiency in this report.
The CI-specific OT program used in the participants had a duration of 8 weeks. The treatment consisted of three home-based exercises: pencil pushups, Brock string, and variable vectograms. The exercises were to be done 5 days/week, 3 times/day for 10 min each time (i.e., 2 min: pencil pushups; 3 min: Brock string; 5 min: variable vectograms). Participants were instructed to spread the exercise sessions throughout the day, at times when they felt less fatigued. Participants were given a daily log/diary to record progress and time spent doing exercises. A phone appointment was conducted every week to ensure that all was going well and to answer any questions participants may have had. A follow-up appointment was conducted 1 and 2 months after the beginning of therapy. During these visits, diagnostic tests for CI were performed, that is, horizontal phorias at 6 m and 40 cm, PFV at 40 cm, and NPC, 3 times each, and the average represented the value for each test. The CISS-15 was also administered, the exercises and log/diary reviewed and corrected if required, and the next phase of exercises provided and explained. Finally, a 6-month period of reinforcement therapy (RT) was offered, during which training sessions were reduced to once per day 5 days per week for the first month and then one session twice per week for the remainder of the reinforcement period.
Results
Case Presentations
Case 1
The first participant was a 68 years old married man with PD diagnosed 6 years ago, having multimorbidity (n = 6) and polymedication (n = 17). He used to enjoy reading but stopped doing so because it became too uncomfortable. He was therefore highly motivated to undergo treatment, with the help of his wife who was very supportive. He was very diligent in doing his exercises, and it was only at the end of the 2-month period that he felt the benefits. His reading improved and words were clearer. The clinical findings indicated that he improved by 8.3 cm on the NPC, 9.3Δ on the PFV, and 14 points on the CISS-15 (Table 1). He was satisfied with the results obtained and, for that reason, declined RT. A phone call 3 months later indicated that things remained stable for him, and he was still happy to read and even bought a digital tablet. A phone-administered CISS-15 gave a score of 15. Although the CISS-15 is not validated specifically for phone-administration, it was performed that way to get an idea of the participant’s level of symptomatology post-treatment.
Key Clinical Findings Showing the Improvement in Symptomatic CI Pre- Versus Post-Treatment for the Case Series.
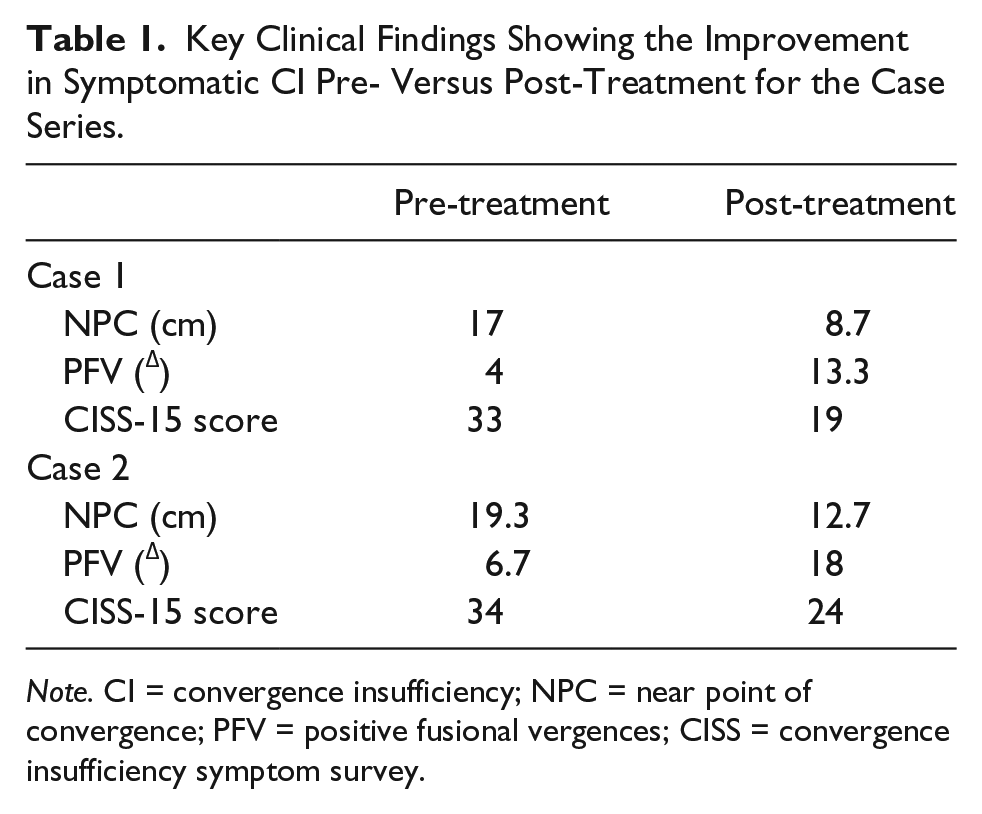
Note. CI = convergence insufficiency; NPC = near point of convergence; PFV = positive fusional vergences; CISS = convergence insufficiency symptom survey.
Case 2
The second participant was an 80 years old married man with PD diagnosed 5 years ago, with comorbidities (n = 3) and several medications (n = 7). He liked reading the newspaper, but had been realizing that his “left eye goes away” when doing so, which disturbed him. He did not report diplopia. He was very motivated to do OT, knowing that he would receive support from his wife and from the OT team. After 1 month of therapy, he felt his two eyes were working well together, and on completion of OT, he was able to read the newspaper. He readily accepted RT to consolidate what he had gained through treatment. The clinical findings indicated that he improved by 6.6 cm on the NPC, 11.3Δ on the PFV, and 10 points on the CISS-15 (Table 1). This participant called 3 months after his last visit to indicate that he had performed RT for 2 months after which he abandoned because of health problems. At that time, he was still doing well from a vision standpoint, and a phone-administered CISS-15 gave a score of 22.
Discussion
To our knowledge, this is the first report of OT for PD individuals having symptomatic CI. The clinical findings and subjective report of the participants presented here indicate that OT was successful in decreasing the signs and symptoms of CI. These results thus indicate that PD is not a contraindication to OT for CI and that it can be offered to those having symptomatic CI. However, in spite of a 31% prevalence of symptomatic CI in PD (Irving et al., 2016), we also found that the uptake and compliance for treatment is rather poor, with only 7 out of 25 patients agreeing to undergo treatment, and 2 out of 7 completing treatment. Those who abandoned the treatment generally reported that manifestations of PD rendered them too fragile and too tired to want to pursue OT on a regular basis. Although limited, the positive outcomes obtained in our two participants provide evidence for the need of further research in the area. Our data suggest that it would be worthwhile to screen patients for CI as soon as a diagnosis of PD is made and offer OT to those who have symptomatic CI. It might be that at an early stage of PD, with less burden from the disease, compliance to treatment could improve. It is clear also that patients need to be highly motivated and to have strong support at home and from the treating team.
It has been suggested that PD may play a role in the oculomotor control of convergence. An earlier report indicated that one patient with PD had CI during his “off” period and that it cleared up under levodopa therapy during his “on” period (Racette, Gokden, Tychsen, & Perlmutter, 1999). A more recent study investigating dopaminergic medication on ocular function in PD patients indicated that although the degree and amplitude of convergence were better in the “on” versus “off” states of the disease, convergence ability remained poorer in PD patients than in controls even in the “on” state (Almer et al., 2012). This study further indicated that if dopaminergic treatment helps, the convergence ability fluctuates, therefore complicating the clinical management of CI. Although CI in PD may be exacerbated by dopamine deficiency, the fact that dopaminergic therapy could help restore the exodeviation at near in the single case, and provided a better degree and amplitude of convergence during the “on” versus “off” states in the other PD patients, indicates that the anatomical structures responsible for convergence are intact. Furthermore, in a large majority of PD patients with CI, neuroimaging showed no structural brainstem changes (Lepore, 2006). The present report thus complements these studies, showing that it is possible to improve convergence with OT in symptomatic PD individuals. This was demonstrated by a greater ability to converge, an increase in the fusional range of convergence and a decrease in symptomatology. Furthermore, subjectively, these participants still benefited from OT for at least 3 months post-therapy, that is, the time of our last communication. In future research attempts to confirm our results in a wider PD population, efforts should be devoted into finding the most effective OT modality for these individuals. This could be to carefully select patients for whom symptoms have a large impact on quality of life, decrease the daily session time, do group-training within movement disorder clinics, or make it part of another overall exercise program, for example.
Conclusion
The results presented here are novel as this case series show that OT for CI in PD is possible. Further research is required to confirm these results in a wider PD population. Careful attention on proper patient selection and measures to improve compliance will be necessary. In the meantime, the positive results obtained in these two cases should encourage clinicians to consider OT (a therapy with no/minimal risk) for CI in patients with PD whose quality of life is affected by this binocular dysfunction.
Footnotes
Authors’ Note
This study was approved by Institut universitaire de gériatrie de Montréal (CER IUGM 12-13-008), Centre hospitalier de l’université de Montréal (CER CHUM: 12.154), Montreal General Hospital Research Ethics Committee (12-321 GEN), and University of Waterloo (UW ORE 18408).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research grants from the Comité aviseur pour la recherche clinique (CAREC) at the Institut universitaire de gériatrie de Montréal (IUGM), the Canadian Institutes of Health Research (grant #123462) and the Canadian Optometric Education Trust Fund (COETF).