
Abstract
Keywords
Introduction
Health care aides (HCAs) are unregulated direct care providers working across the continuum of care (Hewko et al., 2015). They provide care as assigned, assisting patients with activities of daily living, comfort, and safety. The range of care provided depends on the patient population, care setting, knowledge and skills of the individual HCA, legislation, and policy (Brandt, 2014). Alberta Health and Wellness (2001) developed a competency profile for HCAs that includes 40 competencies. Alberta has also developed standardized curriculum for educational institutes that provided HCA training. An environmental scan on Canadian educational standards for HCAs (Canadian Educational Standards for Personal Care Providers: Environmental Scan, 2012) reported that the vast majority of private institutions and all public colleges in Alberta follow the Government of Alberta Health Care Aide Provincial Prototype Curriculum (HCA-PPC), developed in 2005, which outlines 37 modules.
One of the competencies of HCAs is medication assistance. HCAs are commonly involved in medication assistance of several non-oral (ointments/creams, nasal spray, enema) medications. Strain, Maxwell, Wanless, and Gilbart (2011) reported that in 70 out of 113 supportive living (SL) and long-term care (LTC) facilities, HCAs provide medication assistance. However, what counts as “medication assistance” may range from providing creams/ointments to multi-pack medication packages. The delivery of prescribed oral medication is the responsibility of registered nurses (RNs) and licensed practical nurses (LPNs). HCAs also provide assistance in oral medication delivery in supportive living but rarely do this in LTC (Strain et al., 2011). HCAs involvement in oral medication assistances in LTC would improve the utilization of HCAs and maximize health human resources (Hussein & Manthorpe, 2005; Pan-Canadian Planning Committee on Unregulated Health Workers, 2009; Stone, Dawson, & Harahan, 2004; Stone & Harahan, 2010). Appropriate workforce utilization can have many benefits for patients, providers, and the system. The cost of care is also lower where non-regulated health care providers are involved in the care process as compared with facilities where the care is provided by nurses only (MetLife Mature Market Institute, 2010). However, non-nursing (such as HCAs) involvement in medication assistance may result in more medication errors so jeopardize the health of residents (Woods, Guo, Kim, & Phillips, 2010).
A medication error is defined as any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer (National Coordinating Council for Medication Error Reporting and Prevention [NCC MERP], 2012). The risk of medication errors in LTC is an important consideration because a large number of medications are given to residents with significant frailty (Barber et al., 2009).The incidence of medication errors in continuing care facilities is high (Field et al., 2001; Szczepura, Wild, & Nelson, 2011). Studies have reported that medication error rates in continuing care range from 10% to as high as 40% (Young et al., 2008; Zimmerman et al., 2011). There have been particular concerns about increases in medication errors if HCAs are involved in oral medication assistance (Reinhard, Young, Kane, & Quinn, 2006). To address these concerns, it is important to determine the situation of medication errors at LTC facilities where HCAs are already involved in oral medication assistance.
The primary goal of our project was to examine the utilization of HCAs with a particular focus on medication assistance and its impact on patient safety in Alberta, Canada. This article focuses on the error rates at LTC facilities by HCAs and other nursing staff. We also looked at the specific types and severity of errors. The key research question was whether HCAs are likely to make more medication errors when assisting with oral medication compared with other nursing staff.
The study was approved by a local research ethics board in Alberta.
Method
From June 2014 to July 2015, we conducted a mixed method study on HCA utilization in continuing care in Alberta, which included a survey of 320 continuing care facilities and interviews with staff at five facilities. This is the first article of the series on this project and only focuses on the medication error rates and types and severity of errors by nursing staff at LTC facilities using medication incident reporting (MIR) for two LTC sites. Oral medication assistance is defined as “a service provided to clients to ensure medication is taken as intended by the prescriber when the client is assessed as being unable to independently take his or her own medication safely” (Brandt, 2013). This may include opening medication packages and handing over medications to the client for immediate ingestion, application, inhalation, insertion, or injection. The main outcome was the incidence rate and the severity of medication errors ranges from “no apparent harm,” “minimal harm,” “moderate harm,” “severe harm,” and “death” and are defined in the same way at both facilities (see the appendix). We dichotomized severity of harm into “moderate harm” versus all other “less severe harm” categories (“minimal harm,” “no apparent harm,” “close call,” and “hazard”).
We also analyzed Resident Assessment Instrument (RAI) data to assess the health status of the residents in facilities where HCAs were involved in oral medication assistance. We extracted data on residents’ demographics and other health status measuring tools from the RAI 2.0 database, such as the Changes in Health, End-stage disease, and Signs and Symptoms (CHESS) Scale (Hirdes, Frijters, & Teare, 2003), and the Pain Scale, which is a visual analogue scale developed by U.S. nursing homes (Fries, Simon, Morris, Flodstrom, & Bookstein, 2001). In the Index of Social Engagement (ISE) scale, higher score indicates a higher level of social engagement (Mor et al., 1995). We also accessed the same RAI data for two other LTC control sites where HCAs were not involved in oral medication assistance to compare differences in the resident population.
We entered and analyzed data in SPSS Version 19. We performed inferential statistics using the Chi-Square Test and Fisher Exact Test at 95% confidence level; a p value < .05 was considered as significant.
Results
The survey showed that three out of 64 LTC sites (5%) reported the involvement of HCAs in oral medication assistance. We were able to obtain error reports from two facilities (Facilities A and B) with 220 errors reported in total by all health care providers including HCAs. Both were publicly owned facilities. Facility A comprised 44 LTC beds and Facility B had 120 LTC beds. Facility A employed 31 HCAs, four RNs, two LPNs, and a care manager. Facility B employed 76 HCAs, seven RNs, nine LPNs, and two care managers. Medication assistance training was mandatory for HCAs at both facilities. The medication assistance training in Alberta is aligned with Alberta Health and Wellness (2001).
Both facilities involved HCAs in oral medication assistance along with topical medication. All medication deliveries were documented in medication administration records, and any non-administered medications were also recorded. At these facilities, HCAs were involved in two types of medications: (a) basic medications—these refer to non-medicated eye, ear, nasal, cream/ointment preparations, suppositories, and fleet enemas upon assignment by a regulated provider and (b) multi-dose medication package delivery—delivery of regularly scheduled oral medication in multi-dose packages to stable residents.
Table 1 shows the comparison of the health status of residents at the LTC facilities with HCAs involvement and the two control LTC facilities. The comparison shows that the residents were more complex in some aspects at the two LTC sites where HCAs were involved; for example, the average age and the proportion of residents with depression was higher (Table 1).
Comparison of Residents Between Those LTC Facilities Where HCAs Are Involved in Oral Medication Assistance and Those Where HCAs Are Not Involved.

Note. LTC = long-term care; HCA = health care aide; ADL = activities of daily living; CPS = Cognitive Performance Scale; PURS = Pressure Ulcer Risk Scale; ISE = Index of Social Engagement; CHESS = Changes in Health, End-stage disease, and Signs and Symptom; UTI = urinary tract infection.
Chi-square test statistics.
Number of days per week a resident receives injection; residents not getting injections were excluded.
Around 50% of medications were assisted by HCAs at Facility A and around 70% of medications were assisted by HCAs at Facility B. Based on the average number of medications (data not shown), the monthly incidence rate of medication errors was 2.6 per 10,000 medicines administered; the incidence rate for HCAs was 2.4 per 10,000 while it was 3.1 per 10,000 for other health care providers.
Overall, HCAs were involved in 137 (63%) errors, LP/RNs in 77 (35%), and pharmacy in four (2%). The data included errors over a period of 2 years, approximately, from October 2012 to January 2014. Dose omission errors were 61% (n = 134), documentation errors were 1.4% (n = 3), extra dose to resident 2.7% (n = 6), extra dose in package 0.5% (n = 1), incorrect drug 7% (n = 15), incorrect time 5% (n = 12), frequency scheme error 1.4% (n = 3), incorrect narcotic count 0.5% (n = 1), not performed where indicated 4.1% (n = 9), wrong dose strength 3.2% (n = 7), wrong duration 1.8% (n = 4), wrong resident 8.6% (n = 19), wrong storage 0.5% (n = 1), wrong technique 0.5% (n = 1), and others 1.8% (n = 4). Table 2 shows the classification of error rates between HCAs and other health care providers.
Error Rates Between HCAs and Other Health Care Providers Who Were Involved in Medication Support at the Two Selected Long-Term Continuing Care Facilities (n = 218).
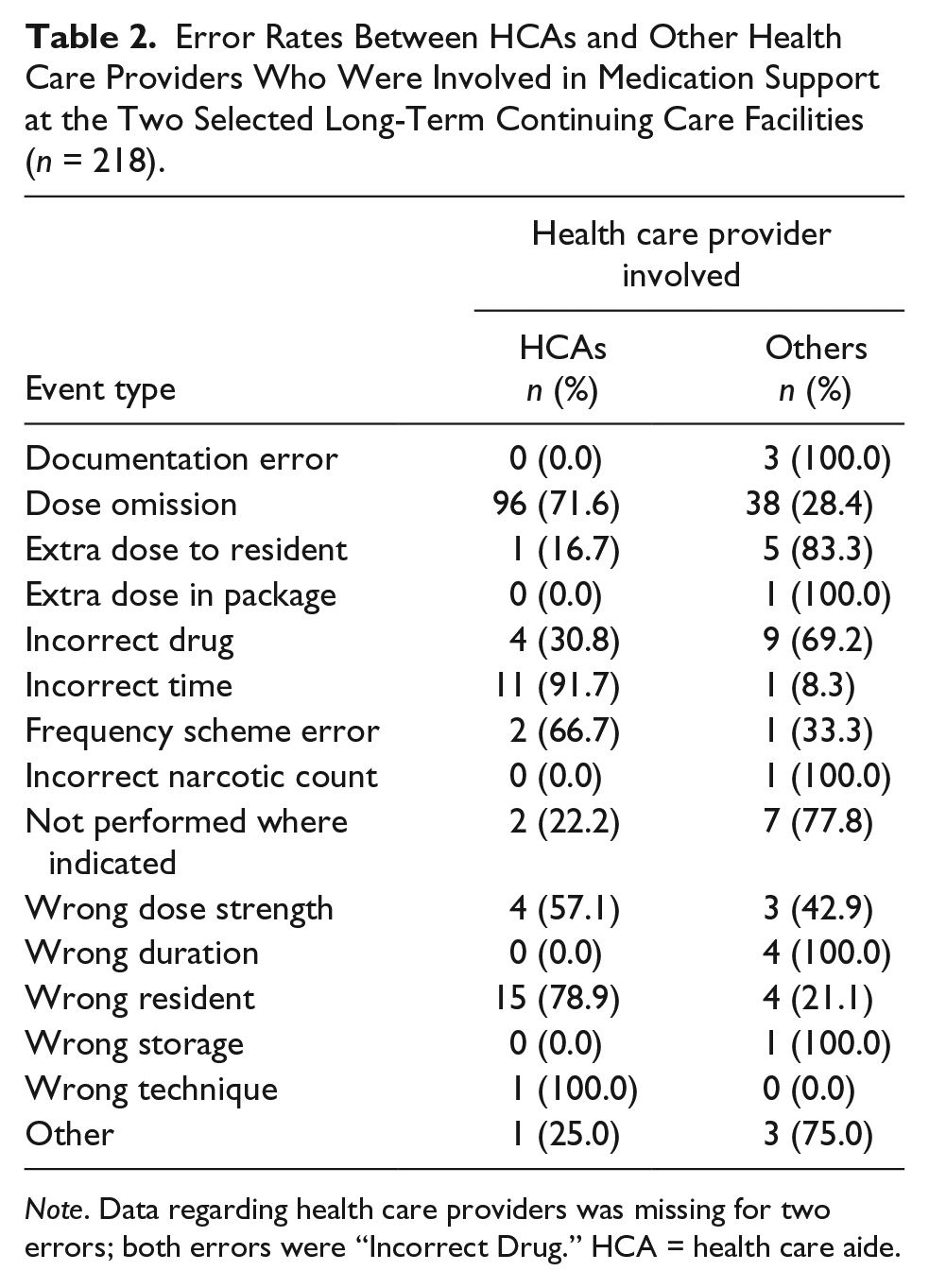
Note. Data regarding health care providers was missing for two errors; both errors were “Incorrect Drug.” HCA = health care aide.
There were no errors of “high severity” during the reporting period. Errors of “moderate severity” were 4% (n = 8), “minimal severity” were 53% (n = 117), and “no apparent harm” were 43% (n = 95). The incidence rate of “moderate severity” errors was 3.6% (95% confidence interval [CI] = [1.7%, 6.8%]) among all errors. The analysis of “moderate severity” versus “minimal/no harm” showed that HCAs were significantly less likely to cause errors of “moderate severity” than all other health care providers (2% vs. 7%, chi-square = 5.1, p value = .04).
Discussion
Our analysis of the medication error reports from two LTC sites contributes important findings to the current understanding of medication assistance by HCAs. The results of this article suggest that HCAs may safely be involved in oral medication assistance in LTC settings under the recommended guidelines (Brandt, 2013). The guidelines state that to involve HCA in oral medication assistance, four conditions must be met: (a) HCA job description must state that medication assistance is included in the HCA roles and responsibilities; (b) employer policies and procedures must specifically describe how medication related tasks are to be done safely, including the type of medication system used and the types of medications with which HCAs can assist; (c) appropriate HCA training is required; and (d) ongoing supervision must be provided, whether direct or indirect, by a regulated health care professional.
We identified dose omissions as the most common error at these LTC facilities. One study conducted on 12 continuing care facilities in the United States reported that the highest type of medication errors in assisted living was the wrong dose (12.9%) and dose omission (11.1%; Young et al., 2008). Other studies have also reported that dose omission was the most commonly occurring medication error in continuing care facilities (Charboneau, Brickley, Rich, & Shelton, 2011; Szczepura et al., 2011).
In our study, HCAs were involved in medication assistance to a higher proportion than other nursing staff. While error rates were very low in our study, they seemed highest for HCAs. When we standardized the denominators (according to the proportion of medicines assisted by HCAs and other nursing staff), the error rate for HCAs dropped slightly below that of the other nursing staff. This finding contradicts assumptions about resident safety issues when HCAs are involved in oral medication assistance. Both sites have implemented automated medication packaging for all medication delivery, which is likely to contribute to this positive outcome as other studies have suggested (Baril, Gascon, St-Pierre, & Lagacé, 2014).
Our study also showed that HCAs were significantly less likely to cause errors of “moderate severity” as most of the errors by HCAs were categorized as “minimal harm” or “no apparent harm.” HCAs are not allowed to deliver some high-risk medicines such as insulin and narcotics, which might have resulted in lower rates of “moderate severity” errors by HCAs; for example, delivering a wrong dose of insulin has more serious consequences than missing a dose of Tylenol. Conversely, HCAs may make fewer errors because they are more careful and do the checks diligently. Our findings are comparable with other studies, which report that error rates are not higher in HCAs compared with nurses if appropriate medication assistance training is provided (Zimmerman et al., 2011). One can argue that the resident population might be less complex at the facilities where HCAs were involved. However, the RAI data comparison showed that the residents were even more complex in certain health aspects at the facilities where HCAs were involved in oral medication assistance. Thus, the complexity of residents’ health status may not be an appropriate reason for not involving HCAs in oral medication assistance in LTC. Nevertheless, we understand that the workload on HCAs would increase by involving them in oral medication assistance that might affect resident care. A recent study by Mallidou, Cummings, Schalm, and Estabrooks (2013) in Canada identified that the workload on HCAs is high and their involvement in other activities affects the quality of direct care provided to residents. If a facility decides to involve HCAs in medication, they should consider hiring more HCAs to prevent any compromise on resident care. The supply of HCAs should also be increased from training schools to meet the demand.
We identified some limitations of the study. First, there is a possibility of under-reporting errors in the error reports. This is a very common issue with self-reporting of incidence. Second, we did not receive error reports from all sites, having to rely on the findings from two sites only, although in the main survey study three LTC facilities reported the involvement of HCAs in oral medication assistance. The other limitation was the possibility that HCAs would not have sufficient experience/knowledge to correctly identify and report medications errors. Despite these limitations, this research can be used as groundwork for further research.
Future studies need to investigate ways in which HCAs can be involved in the oral medication assistance process in LTC settings. Future studies should also capture the perspective of residents and family members about HCA involvement in the oral medication assistance process. Challenges and barriers need to be looked at to change the culture of medication assistance by HCAs.
Conclusion
Our results show that HCA may safely be involved in oral medication assistance in long-term care under the guidelines (Brandt, 2013). Increasing HCA involvement in medication assistance might lead to a cost-effective and efficient utilization of workforce in continuing care facilities. Further research is needed on a larger scale to determine if HCAs’ involvement would affect the safety of residents in LTC facilities and to determine the cost-effectiveness of HCAs’ involvement in oral medication assistance.
Footnotes
Appendix
Definitions of the Severity of Errors.

| Hazard | A hazard or hazardous situation that has been identified as having the potential to escalate to a close call or a harmful event. This hazard exists as a latent condition. For example, a piece of equipment may be difficult to use; the staff may feel that it is potentially error prone. Another example is two similar looking drugs located side by side in a container. |
| Close call | An event or circumstance that has the potential to cause a harmful event but did not actually occur due to corrective action and/or timely intervention. The event did NOT reach the patient. An example is pouring the wrong medication and having taken it to the bedside; the mistake is caught on the last check before giving it to the patient. An inappropriate dosage of a medication is detected before an order is processed. A nurse discovers a patient is allergic to penicillin when checking the name band before hanging the IV penicillin dose. A physician is reading the wrong CT results for the patient that is being examined but notices that the report is not making sense and requests the correct report. |
| No apparent harm | An event or circumstance where at the time of the event or reporting of the event the patient does not appear to suffer any harm but could do so in the future. No physical and/or psychological symptoms are evident and no intervention is required. For example, a patient falls and hits his or her head but no evidence is found of bruising, swelling, or any change in neurological status or cognitive function. A patient received a wrong medication but exhibited no change in symptoms or condition as a result. |
| Minimal harm | An event or circumstance where there is minimal harm to the patient. Minimal adverse effects may include abrasions, skin breakdown, pain, minor burns, bruises, scratches, confusion, emotional distress, and anxiety. These effects may or may not require intervention. Intervention for minimal harm may include x-rays, sutures, physician examination, blood collection, or re-collection and closer observation, even if short-term in nature. For example, a patient received a dose of insulin that was higher than expected; a new order was received and extra food was given to reduce blood glucose levels with a follow-up glucometer check. A patient falls, sustains a bruised and swollen knee, and requires some Tylenol and an ice bag for a few hours but this does not extend the stay in hospital. Extra observation and monitoring may be needed such as an increase in vital signs frequency for the next 4 hr but no overall changes in the treatment plan would be required. |
| Moderate harm | An event or circumstance where there is moderate harm to the patient. Moderate adverse effects may include moderate lacerations, fractures of the extremities, burns, and unintentional heavy sedation. Intervention and extended observation are required. Intervention for moderate harm may include diagnostic testing such as MRI, CT scans with contrast, blood gas analysis, or cross-match for blood products. An event or circumstance causing moderate harm has the potential to prolong length of stay. For example, a patient falls, sustains a fractured arm that is cast, and function recovers through a short period of physiotherapy. A patient is found to have retained a sponge in abdominal surgery, develops an internal infection, and requires a repeat procedure to retrieve the sponge and a 10-day course of antibiotics. A change occurs in the treatment plan to deal with the new symptoms or condition arising from the adverse event. |
| Severe harm | An event or circumstance where there is severe harm to the patient. Severe adverse effects may include anaphylaxis, permanent injury or disfigurement, fractures (other than extremities), or a sudden life-threatening change in vital signs. Immediate, life-saving intervention is required and may include life support and/or an emergency surgical occurrence. For example, during a surgical procedure, the wrong part is inadvertently removed. A patient receives a contrast dye to which he or she had a known allergy and suffers a cardiac arrest. A wrong dose of a medication leads to a loss of hearing. |
| Death | An event or circumstance causing death in which the most likely cause is due to an error that occurred in the course of receiving care. Note that multiple deaths should be entered in separate reporting and learning submissions. |
Note. IV = intravenous; CT = computed tomography; MRI = magnetic resonance imaging.
Acknowledgements
The authors gratefully acknowledge the members of the advisory committee for their advice and constructive feedback throughout the project. We also acknowledge Julia Bicknell for her support in editing the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Alberta Health (Grant 003760).