
Abstract
Introduction
Falling is a serious health problem for elderly persons. In general, the risk of falling increases with age, and 50% of older people over 80 years old fall once a year (Nikolaus, 2005). The consequences range from light to severe injuries, such as a fracture of the femur (Keegan, Kelsey, King, Quesenbery, & Sidney, 2004; Nguyen, Center, Sambrook, & Eisman, 2001). Fear of falling is another result that is frequently combined with self-limitation of activity and everyday participation that causes decreasing quality of life and increases the risk of falling (Bloem, Steijns, & Smits-Engelsman, 2003). Fall prevention is needed to avoid the negative consequences of falling. Detection of an increased risk of falling is necessary for the implementation of effective prevention programs.
Except for those caused by extrinsic and syncopal factors, locomotive falls comprise the most common type of falls (80%-90%; Zeitler, Gulich, & Schmidt, 2004). A good assessment to detect locomotive falls is important. There is no consensus of which tests are most appropriate in specific situations. Research must clear the validity and reliability of fall risk assessments (Hofheinz & Schusterschitz, 2010), and it is very important to examine the prognostic quality of assessments (Boulgarides, McGinty, Willett, & Barnes, 2003; Deutsches Netzwerk für Qualitätsentwicklung in der Pflege, 2006; Gates, Fisher, Cooke, Carter, & Lamb, 2008; Scott, Votova, Scanlan, & Close, 2007). The Timed Up and Go Test (TUG; Podsiadlo & Richardson, 1991) is a common test in practice and research to assess mobility and fall risk. The advantage of the TUG is that it is easy to perform and does not take a lot of time. But regarding the fall risk prediction, the TUG is discussible. Beauchet et al. (2011) stated in their review that the predictive ability of TUG is limited. Barry, Galvin, Keogh, Horgan, and Fahey (2014) came to the same result for community-dwelling elderly. Schoene et al. (2013) reached the conclusion that the TUG is not useful for healthy, high-functioning older people, but better in less healthy, lower functioning older people. To assess fall risk, a better and more appropriate test than the TUG as single task assessment seems to be necessary.
In more recent research, the inability to perform two or more tasks simultaneously (multi or dual tasking) is regarded as an indicator for a higher fall risk (Quinn & Horgan, 2013; Toulotte, Thevenon, Watelain, & Fabre, 2006; Yamada et al., 2011). These observations could be explained by research results showing that the cognitive capacity for processing information is limited (Hall, Echt, Wolf, & Rogers, 2011; Mirelman et al., 2012; Montero-Odasso, Verghese, Beauchet, & Hausdorff, 2012). Recently published data on dual tasks has led to the development of the TUG with a Dual Task (TUG-DT). The TUG-DT provides more information regarding mobility and fall risk because it measures the cognitive capacity in the performance of a dual task (Gothe et al., 2014; Podsiadlo & Richardson, 1991).
Given the human cognitive system has limited capacities, we propose that simultaneously performing two tasks depends on the capacity of each individual to perform these tasks on a continuum between automatic execution to highly controlled performance. A level of maximum control exceeds the participants attentional capacity, which makes it impossible to perform both tasks simultaneously. The participants therefore prioritises one of the tasks. (Borel & Alescio-Lautier, 2014, p. 95)
Although the TUG-DT is a reliable and valid instrument for measuring mobility (Podsiadlo & Richardson, 1991; Shumway-Cook & Woollacott, 2000), uncertainties remain regarding the quality of the prognostic validity (Shumway-Cook, Brauer, & Woollacott, 2000).
Regarding the theoretical framework, we have made the assumption that a TUG with an additional dual task could be a better assessment to identify fallers among community-dwelling elderly. For this, an evaluation of the TUG-DT with prospective data is necessary. The aim of this work was to examine the prognostic validity of the TUG-DT with a cognitive and manual dual task (TUGcog and TUGman) to assess the risk of fall in elderly people.
Method
Community-dwelling older persons were recruited by means of information letters, posters in doctors’ practices, and get-togethers for elderly people in a community center and therapy center. In total, 130 persons attended a personal informational talk regarding the study in the therapy center. We made appointments for testing with 128 persons, and two persons elected not to participate in the study.
The following inclusion criteria were defined: 60 or more years of age, living at home, able to walk at least 10 meters alone (with or without assistive devices, and without being supported by another person), able to understand simple instructions, without cognitive limitations, and able to carry a glass of water in one hand. The participants in the study must, to their knowledge, have been free of neurological or musculoskeletal diagnoses that could influence the fall risk and the measurement results including a cerebrovascular insult, Parkinson’s disease, a transitory ischemic attack, and cardiovascular problems. The participants provided informed consent.
Procedure
At the baseline, we used an intake questionnaire (the Health and Physical Activity Questionnaire of the Division of Physical Therapy, University of Washington; the Mini Mental State Examination; and the Falls Efficacy Scale–International Version), the BBS, TUG, TUGman, and TUGcog. The questionnaires, the Berg Balance Scale (BBS), and all of the TUG tests were administered in different rooms by three blind raters. The participants did not know the results of their individual tests during the testing day, so that they could not inform the rater. The TUG, TUGman, and TUGcog were assessed 3 times, in random order, after a practice trial by the participants.
In the 1-year follow-up after the baseline exploration, the participants were interviewed by phone monthly with a standardized questionnaire regarding any falls they had experienced, including the causes and circumstances of any falls that occurred. The questionnaire that had been used at the baseline was administered for the follow-up questionnaire to evaluate the occurrence of falls.
Instruments
TUG
For the TUG and TUG-DT assessments, we used an armchair with a seat height of 46 cm and a mark on the floor 3 m away from the chair. After verbal instructions, the participants perform one trial of the TUG. The participant stands up from a chair, walks to the mark 3 m away, turns around, returns to the chair, and sits down again. The participants walk safely, as fast as possible. The instructions given are “Walk as quickly and safely as possible to the marked line, turn through 180 degrees, walk back to the chair, and sit down again.” The command given is “Get ready, go!” The time was recorded with a calibrated digital stopwatch.
TUGman
The performance of the TUGman is identical to that of the TUG; however, as an additional task, the participant carries a glass of water while walking. After standing up from the chair, the participant grasps a drinking glass filled with water (the water surface is 1 cm away from the top of the glass, which is 9.5 cm high with a diameter of 8 cm), which is located on a 70-cm-high table. After walking 3 m back and forth and before sitting down again, the participants return the glass to the table.
The following instructions are given:
Stand up, pick up the glass, and then walk as quickly and safely as possible to the marked line, turn through 180 degrees, walk back to the chair, put the glass back on the table, turn through 180 degrees, and sit down again.
The following command given for the TUG with the manual dual task is “Get ready, go!”
TUGcog
The performance of the TUGcog is identical to that of the TUG; however, the following cognitive task is added: While walking, the participant counts backward in threes from a randomly chosen start number between 60 and 100 to avoid a learning effect.
The following instructions are given:
Walk as quickly and safely as possible to the marked line, turn through 180 degrees, walk back to the chair, turn through 180 degrees and sit down again. In addition, count as quickly and surely as possible backwards in threes from 100. Do not repeat the number you are told to start from, but start with the first result you calculate.
The command given is “Get ready, go!”
Statistics
A receiver operating characteristics (ROC) curve was calculated to analyze the diagnostic validity of the TUG-DT. This method calculates the true positive and false positive for each test value and plots them on a curve. The area under the ROC curve (AUC) could be interpreted as a measure of classification quality of the test. The area could have values between 0 and 1, where a higher value indicates better classification accuracy. The closer the value is to 0.5, the poorer the accuracy of the test is, because the value of 0.5 corresponds to a random classification (Hanley & McNeil, 1982). In the ROC calculation, we used locomotive falls as outcome. The analysis was performed with SPSS, version 19. SPSS calculates the p value with a logistic regression model. A p value <.05 means that the logistic regression classifies the fallers with the help of the empirical data better than by chance. The 95% confidence interval (CI) estimates the interval of the population parameter out of the study data. In case of a ROC curve, the lower bound of the 95% CI should be greater than 0.5. Otherwise, the risk that the real population estimate is not better than a random classification is too high.
Results
In total, 128 people wanted to participate in the study. Eight persons did not meet the inclusion criteria and were excluded from the study; 120 persons were tested at the baseline and participated in the follow-up. Of the participants, 94 (78%) were women and 26 (22%) were men. The participants were 60 to 87 years old, and the mean age was 72.2 years (SD = 6.8 years); 72 participants (60%) lived with a partner, and 40% lived alone. Nearly all of the participants (118) were retired, and one person was still working; one participant did not provide employment information.
In the 12-month follow-up, 44 participants fell, as follows: 27 participants fell once, 12 participants fell twice, four participants fell 3 times, and one person fell 7 times. In total, 76 participants did not fall in the follow-up. Table 1 shows the frequency of different types of falls occurring in the study sample. As expected, most of the falls were locomotive falls, and 37 participants had at least one locomotive fall. For the ROC analysis, only the locomotive falls were used as an outcome. The other types of falls were defined as no falls.
Frequency of Falls in the 12-Month Follow-Up.
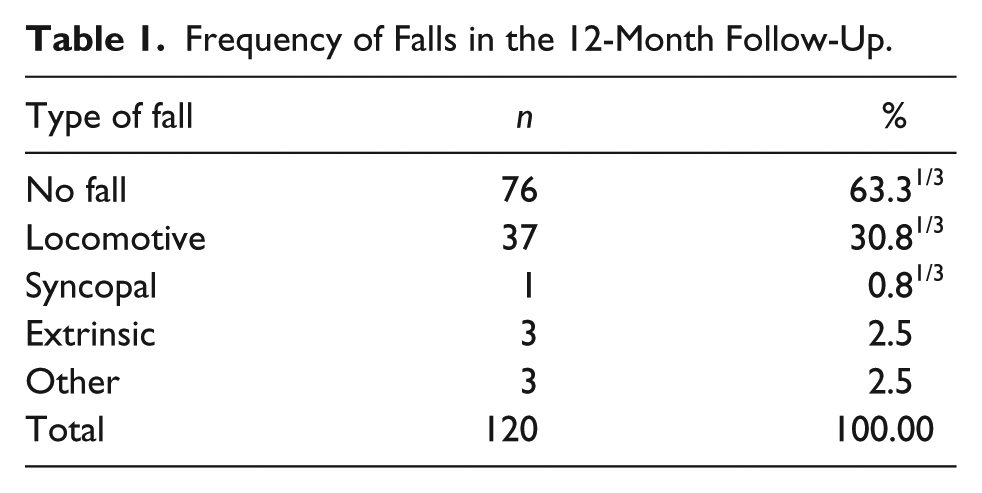
Figure 1 shows the ROC curve for all three tests, and Table 2 shows the statistical values for the ROC curve. The analysis shows satisfactory results for the TUGcog. The area under the curve is 0.65 (p = .008), with a 95% CI = [0.55, 0.76].

ROC curve for the TUG, TUGman, TUGcog.
Area Under the ROC Curve.

Note. ROC = receiver operating characteristic; TUG = Timed Up and Go Test; TUGman = Timed Up and Go Test with manual dual task; TUGcog = Timed Up and Go Test with cognitive dual task.
For the TUGman, the area under the curve is 0.57, with a 95% CI = [0.45, 0.68], which is not significant (p = .256). The TUGman does not have adequate classification power, which is true for the TUG as well. The area under the curve is 0.58, which is not significant (p = .256), 95% CI = [0.47, 0.69].
Table 3 shows the sensitivity and the specificity of the TUGcog for different thresholds. Depending on the desired balance between sensitivity and specificity, an appropriate cut point could be selected. A higher cutoff point increases the specificity, and a lower cutoff point increases the sensitivity.
Sensitivity and Specificity of the TUGcog.
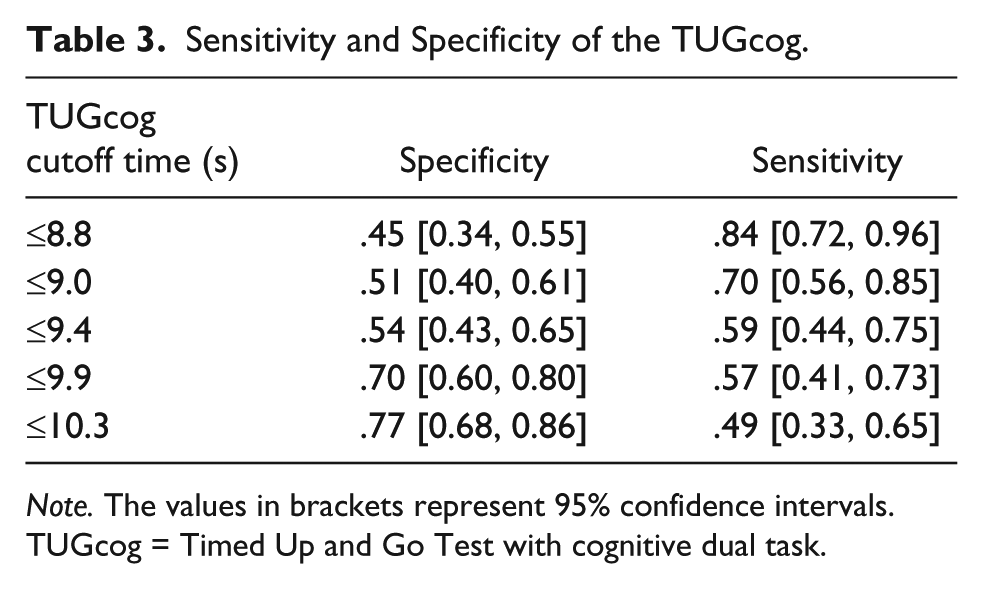
Note. The values in brackets represent 95% confidence intervals. TUGcog = Timed Up and Go Test with cognitive dual task.
Discussion
The main objective of this study was to examine whether the TUG-DT with a manual or a cognitive dual task is a valid instrument for predicting a fall risk for community-dwelling elderly people. Our findings suggest that the TUGcog with a moderate AUC of 0.65 (p < .05) has a better risk prediction for recognizing a higher fall risk in older community-dwelling individuals than the TUG (AUC = 0.58, p = .17) and the TUGman (AUC = 0.57, p = .26).
These findings are different from those of Podsiadlo and Richardson (1991) for the TUG and from those of Shumway-Cook and Woollacott (2000) for the TUG and TUG-DT. This finding could be explained by different samples in each study. Podsiadlo and Richardson (1991) studied 60 people from a geriatric day hospital with many types of diseases (Parkinson’s, cerebral vascular accidents, rheumatoid or osteoarthritis, cerebellar degeneration, past surgeries for hip fractures, and general deconditioning) and 10 active healthy normal volunteers. The study of Shumway-Cook and Woollacott (2000) included 30 persons; 40% of the participants had assistive devices (cane, 23%; walker, 15%; and all of the participants were fallers). In both studies, the investigators used retrospective data. In our study, no devices were used, and prospective data were analyzed.
The limitations of this study are the smaller percentage of men (21.7%) included, and a lower percentage of participants over 80 years old. In our study, the mean age was 72.2 years, in comparison with the study of Podsiadlo and Richardson (1991), in which the mean age was 79.5 years and that of Shumway-Cook and Woollacott (2000), with a mean age of 82.3 years.
Our results show that the TUGcog is a good assessment tool for measuring a risk of falling; however, further research is required. It would be helpful to examine the prognostic validity for different patient groups, including those with a history of stroke and Parkinson’s disease as well as elderly patients in homecare or other diseases and settings. This investigation could clarify which cut points are meaningful for different groups of patients.
Our results show that for elderly community-dwelling persons, the TUGcog is a valid assessment for identifying an increased risk of fall. We suggest 10.0 s as cutoff time for the TUGcog. In this case, we have a good specificity of 0.70 and a sensitivity of 0.57. This finding could help to identify persons at risk and to begin early fall prevention programs to protect this group from negative implications concerning injuries or loss of independence. In our opinion, we can accept the low sensitivity of 0.57, because the false positive patients have no disadvantages, if they participate in a fall prevention program.
The TUGman and the TUG are not able to assess a higher fall risk in our research population. Barry et al. (2014) reached the same conclusions regarding the TUG. The TUGcog is a more challenging task for the elderly; it appears to represent a complex multitask situation in everyday life more effectively than does the TUG or TUGman and could provide earlier detection of limited cognitive ability, which is a cause of falling (Bloem et al., 2003; Woollacott & Shumway-Cook, 2002).
In further research, the prognostic ability of TUG-DT should be examined with different patient groups. It is also necessary to examine different types of dual tasks. It could be that some dual tasks are more difficult to perform than others. This could also influence the prognostic ability of the TUG-DT.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.