
Abstract
Introduction
The use of remote monitoring systems (RMS) for delivering care is increasing in many chronic diseases (e.g., diabetes, cancer) and offers potentially effective vehicles for circumventing the challenges associated with frequent decompensation in patients with chronic heart failure (HF) (Chaudhry et al., 2007; Clark, Inglis, McAlister, Cleland, & Stewart, 2007; Kleinpell & Avitall, 2005). However, there is a paucity of studies that examine the usability (i.e., learnability, accessibility) and acceptability (i.e., satisfaction with the program) of these systems in older adults with chronic HF. Specifically, emerging RMS-based interventions often fail to address older adults as potential end users and to recognize their information needs and issues of acceptance and usability in the context of aging (Demiris et al., 2013). The physiological changes associated with aging (e.g., reduced cognitive, perceptual, and psychomotor abilities) and experiences of usability may affect the interface between the person and the computer system and will likely affect the acceptance and adoption of RMS by older adults with chronic HF and potentially enhance or deter successful implementation of RMS. Thus, it is vital to consider these age-related changes when designing RMS for seniors to increase the likelihood that the demands of technology fit the user’s capabilities (Chomutare, Fernandez-Luque, Arsand, & Hartvigsen, 2011).
The current study was conducted to (a) evaluate the feasibility of recruiting older adults (≥55 years) to participate in a study to test the use of RMS to monitor and transmit health data (e.g., weight, blood pressure, heart rate, symptoms), receive alerts and reminders, and obtain feedback from a health care provider; and (b) assess perceived usability and acceptability of an RMS-based intervention in a group of older adults with chronic HF using a mixed-methods approach. The overall goal of this undertaking was to identify problems or flaws in the system and design of an RMS as perceived by potential end users.
Method
The initial RMS platform for the current study was designed using the principles of community-based participatory research (CBPR), which is defined as
a collaborative approach of social investigation wherein all those involved (e.g., older adults and families, health-care providers, members of the health care community) contribute to the creative thinking and planning that goes into the research project and the intervention that may be the object of the project. (Flaskerud & Anderson, 1999, p. 340)
The CBPR model has a structure, a set of principles, and a staged implementation approach assuring equal participation and leadership of community and academic partners while promoting capacity development and productivity (Flaskerud & Anderson, 1999). Three patient volunteers who represented the target population were invited to work with the research team that included a nurse scientist, an advanced practice nurse with expertise in chronic HF disease management, a cardiologist, and two professors with expertise in bioengineering and computer science to design the RMS platform. This team served as the advisory board and was tasked with selecting culturally and age-appropriate features to include in the RMS. Over a period of 4 months, the team met four times to go over key features and components of the RMS platform and reviewed drafts of the instructional guide for readability and accuracy of content. All members of the advisory board had the opportunity to use the RMS platform and provide additional feedback regarding usability and acceptability prior to the actual testing of the system in a sample of older adults with chronic HF.
The following features of the RMS platform were tested in the current study: (a) automated monitoring of health parameters (e.g., weight, blood pressure, and heart rate), (b) disease related alerts and reminders, and (c) Computer Assisted Personal Interview, a software that enables survey completion using the RMS. The RMS platform (i.e., WANDA B), which was previously described in another paper (Suh et al., 2011), integrated the use of artificial intelligence methods along with advanced computational models and computer vision techniques (Kouris et al., 2010). Participant data were collected through a 3G wireless connection and transmitted to the web-server via Bluetooth and a phone line connection (Figure 1). Answers to daily SMS questionnaires were also stored in the database where it was accessible by a health care provider (e.g., nurse practitioner) in real time (Suh et al., 2010). The appropriate institutional review board approved the protocol.

A framework of cyber-education feedback system.
Once the RMS platform was designed, perceptions related to usability and acceptability were gathered from a sample of older adults with chronic HF who were purposively selected to include a fairly diverse cohort of potential end users (N = 21). Patients who were admitted to the hospital for acute HF decompensation were referred by their cardiologist to the research team who made an appointment to meet with the patients and their family prior to discharge to explain the study to them. If patients agreed to participate, they were asked to sign an informed consent. These participants were provided with the RMS device and accessories and instructed on the use of the different features (i.e., verbal instructions). They were also given an instructional booklet (i.e., written instructions) describing the use and function of each component. Participants were given access to the RMS platform for 12 weeks and instructed to transmit their daily weight, activity, and blood pressure information and complete the symptom assessment questions. Data from participants were used to provide them with tailored guidance to promote self-management behaviors. When alerts were triggered (i.e., biometric measures or responses were outside the pre-set limits), a health care provider who was an advanced practice nurse with expertise in HF disease management called the patient to assess the condition and obtain more information. The advanced practice nurse collaborated with the participants’ primary care provider on a management plan and facilitated appropriate actions (e.g., reset thresholds, limited advice, timely provider outpatient visit, or emergency department evaluation). This process helped support a collaborative partnership between the research team, the cardiologists, and the participants (Anker, Koehler, & Abraham, 2011).
Data Collection
Sociodemographic (i.e., age, gender, race/ethnicity, marital status, level of education, employment status, type of insurance) and clinical data (i.e., New York Heart Association functional class, comorbidities, medications, body mass index, and ejection fraction) were assessed at baseline using the Demographic and Brief Clinical History Instrument.
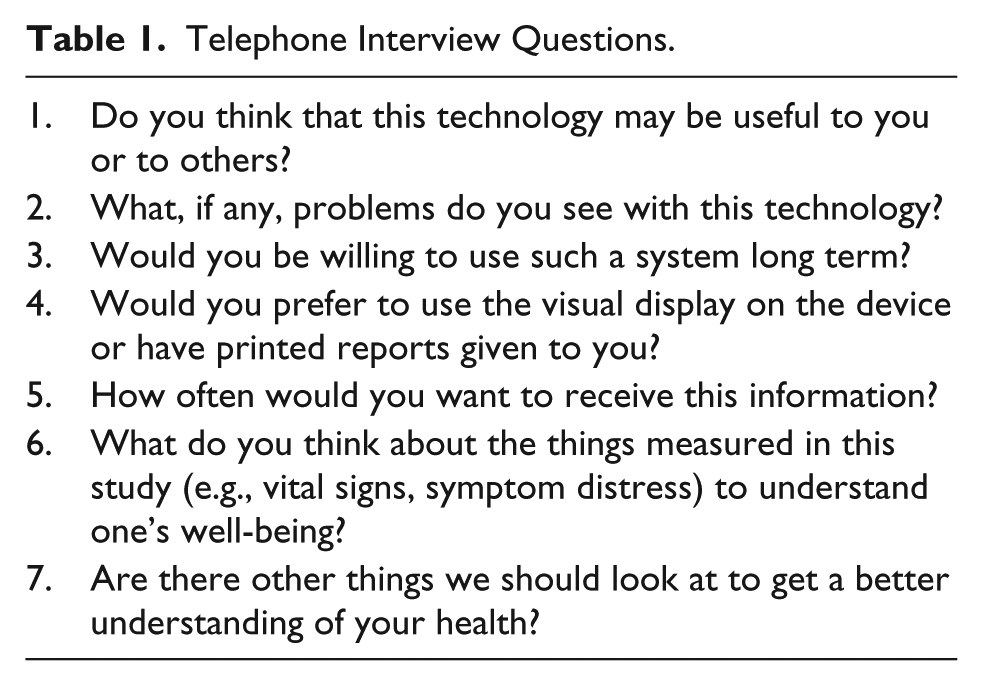
Three types of measures were collected after 12 weeks. First, objective information on number of daily transmissions completed over 12 weeks were collected. Second, participants completed surveys using the survey feature of their RMS device (Computer Assisted Personal Interview); they reported on usability and acceptability of the RMS device using a scale of 1 to 5 (1 = strongly disagree; 5 = strongly agree). Information was also collected on degrees of difficulty experienced with using the RMS, time and level of assistance required to use RMS, and level of satisfaction with the RMS platform using a scale of 0 (none) to 3 (a lot). Last, participants completed a 1:1 telephone interview with the researcher to describe their experiences with the RMS using a selected set of questions (Table 1); the telephone interview lasted an average of 15 to 20 min.
Telephone Interview Questions.
Data Analyses
Statistical analyses were carried out using SPSS for Windows (version, 20.0, SPSS, Inc, Chicago, IL). Descriptive statistics (M ± SD and median with interquartile range for continuous variables and proportions for binary variables) were used to characterize the study population and describe participants’ perceptions of usability and acceptability of RMS. Measures of frequencies were used to describe perceived difficulty and satisfaction with using RMS. Interview data were reviewed for common themes.
Results
Twenty-one patients with a mean age of 73.1 ± 9.2 years and mean ejection fraction of 27.3 ± 6.7 participated in the study. The average time since HF diagnosis was 5.2 ± 2.1 years. A majority of participants were female (52.4%) and married (57.1%). Ethnic/racial breakdown for the sample was 19% Hispanic, 52% Caucasian, and 29% African American. A little less than a third of the participants (29%) had a high school education or less, and 42.9% of the participants reported an annual income below US$15,000. The New York Heart Association Class for patients was Class II (66.7%) and Class III (33.3%). Thirty-three percent (n = 7) reported not having a smartphone or computer at home and no previous computer experience.
All 21 participants initiated the use of RMS and transmitted their health data and symptom distress responses within 1 week of discharge. Seventy-one percent transmitted daily health data for the 12-week study duration; 14% transmitted data ≥75% of the time, and another 14% transmitted data <75% of the time, with one participant only transmitting data for 3 days of the 12 weeks. The average scores for various descriptive statements related to the usability and acceptability of the RMS are summarized in Table 2; overall usability and acceptability of the RMS were 4.08 ± 0.63 and 4.10 ± 0.56, respectively (range 1-5). Seventy-three percent reported having no difficulty or little difficulty, and 90% were moderately and extremely satisfied with using the RMS; 95% felt the self-monitoring required “very little” or “no” amount of their time (Table 3).
Usability and Acceptability Data (N = 21).

Note. Values given as average score: 1 = strongly disagree; 5 = strongly agree.
Patient Perceptions Related to Use of RMS (N = 21).

Note. RMS = remote monitoring systems.
Interview data showed that most of the patients (76%) characterized self-monitoring procedures as something helpful for themselves and for others. All participants felt the feedback they received from the health care provider related to their health data was very helpful toward assisting them with a better understanding of their heart condition and treatment plan. They appreciated having the time to discuss their options with a person who was knowledgeable and open to helping them with self-care management. A majority of the patients (90%) were strongly interested in using RMS in the future; however, 71% expressed the desire to have a bigger monitor to see their health data and complete the surveys and 86% reported wanting to receive their health data in written format versus visual display on the RMS. Three of the older participants indicated that their family members helped them with daily transmission because they could not see the visual display or did not want to learn how to use the RMS; they suggested integrating an audio reporting of their health data. More than half (57%) felt that daily symptom reporting was too intensive and was the least liked aspect of the RMS experience; 9.5% did not understand the need for daily transmission of health data and associated alerts and reminders. One quarter (19%) reported the desire to have someone from the research team help set up their RMS device at home.
Discussion
Despite tremendous progress in chronic HF management, the prognosis for older patients continues to be characterized by worse outcomes (Riegel et al., 2002). Poor adherence to medical recommendations remains a substantial problem in older adults who must follow a multi-component treatment regimen that includes daily weights, symptom recognition and reporting, improved diet and physical activity, medication adherence, and stress management (Evangelista et al., 2003). Older patients may exhibit poor adherence as a result of lack of adequate social support or financial resources or inadequate knowledge about HF self-management, or may fail to adhere to therapeutic regimens because of low health literacy or language barriers (Evangelista et al., 2010). Data show that inadequate health care provider follow-up, poor patient–provider communication, and failure to promptly seek medical attention when symptoms occur are also preventable factors leading to HF readmissions in older patients (Bennett et al., 1998). Thus, the design and testing of RMS platforms to support self-management strategies may potentially enhance chronic HF disease management efforts in this high-risk population (Demiris et al., 2013).
Our findings indicate that older adults suffering with chronic HF, with limited computer skills, were open to learning how to use RMS platforms for self-monitoring, receiving alerts and feedback, and completing surveys. This is in contrast to a study where older adult participants found the concept of self-monitoring unfamiliar and this influenced a narrowed interest in the use of wellness self-monitoring tools (Huh, Le, Reeder, Thompson, & Demiris, 2013). Our findings validate the potential benefits of using RMS to boost chronic HF disease management efforts for older adults by offering potentially effective vehicles for circumventing the challenges associated with limited access to health care facilities due to geography, infirmary, and limited resources (Schneider, van Osch, Schulz, Kremer, & de Vires, 2012). An RMS platform such as the one we tested in the current study supports a more dynamic connection between patients and health care providers and improves self-care by monitoring health data, communicating health reminders, and providing feedback, as confirmed by our participants. These findings have been confirmed in several large-scale clinical trials confirming the effectiveness of RMS on improving outcomes through early detection and management of clinical events in a variety of other cardiac populations (Crossley, Boyle, Vitense, Chang, & Mead, 2011; Ricci et al., 2013; Varma et al., 2010). Clearly, care facilitated by RMS has the potential to enable early detection of key clinical symptoms indicative of worsening overall health and allows health professionals to offer surveillance and advice, and triggers early implementation of strategies to enhance adherence behaviors (Wakefield et al., 2009).
More recently, the use of RMS in health care has received overwhelming interest among health care organizations, government agencies, and policy makers (Kaufman, 2010). The potential contribution of the RMS on self-management in older adults with HF seems huge, given that a majority of Americans have mobile phones and android tablets (Darkins et al., 2008). However, several challenges on the use of RMS in this population have remained and emerged from our study, including the need to account for changes associated with aging and loss of control (Lai, Kaufman, Starren, & Shea, 2009; Wade et al., 2011). Chronological aging is associated with natural physical and cognitive changes, which starts to become noticeable at 45 years of age (Wagner, Hassanein, & Head, 2010). Progressive visual impairment as well as slower processing of visual information begins in the early 40s (Charness et al., 2010). Like vision, hearing declines with age and approximately 20% of those between 45 and 54 years old begin to have some form of hearing impairment (Charness et al., 2010). Psychomotor skills also vary by age and with certain medical conditions. Motor skills required to complete computer tasks may diminish with age (Wagner et al., 2010). Cognitive changes include shorter attention span (selection, divided and automated response), decline in memory (short term, working, and long term), and impaired learning ability (Charness et al., 2010). Poor physical capacity and fatigue are also very common among patients with moderate to severe HF, and this also affects learning. We carefully took these factors into consideration in assessing RMS functionality. However, data from the current study support the need for additional changes including a bigger visual display and audio feedback. Likewise, our research team is cognizant of the need to reduce the expectation of having older patients transmit their health data and symptom distress information every day based on valuable input from the participants.
Study Limitations and Future Work
There are several important limitations to our findings. First, we had a small sample, which limits the strength and generalizability of our conclusions. However, we were able to reach our target enrollment of approximately 50% women and 20% from Hispanic or Latino ethnic group to allow us to fully represent these minority groups in this study. Second, enrollment in the study was based on a convenience sample of patients willing to participate in the study, resulting in a sample that was probably skewed toward patients with a more favorable view toward RMS even before their participation. Third, some patients’ perspectives had to be obtained retrospectively, following the completion of their participation in the study, which may have led to recall bias. Fourth, because of the lack of a control group and the possibility of selection bias, our findings should be viewed as hypothesis-generating and in need of testing in long-term, randomized, controlled trial. In addition, future work designed to draw conclusions about feasibility and acceptability of RMS should incorporate a larger sample. Investigating other relevant outcomes, such as clinical history (e.g., length of time since HF diagnosis, number of hospitalizations in the months prior to study enrollment, functional status, symptom burden, etc.), may also be useful for future research. Likewise, additional research on patient adherence to use of RMS with an emphasis on factors responsible for patient nonadherence to use of RMS should be further investigated (Varma et al., 2015). Future studies should also incorporate a longer follow-up to capture continued use or nonuse of RMS. Finally, the need to verify the data transmitted by RMS is of utmost importance (Parthiban et al., 2015).
Conclusion
Despite the proliferation of RMS to support HF disease management, empirical evidence of the efficacy of RMS to supplement self-care programs remains controversial. There are a limited number of well-designed, multicenter randomized controlled trials (RCT) to guide policy on the use of RMS and limited data to sustain these programs over time (Chaudhry et al., 2007). Lack of awareness among clinicians and researchers of the potential benefits of RMS limits the use of this care delivery model (Kleinpell & Avitall, 2005). The current study was conducted to evaluate the feasibility of recruiting older adults to participate in a study to test the use of RMS to monitor and transmit health data, receive alerts and reminders, and obtain feedback from a health care provider and to evaluate perceived usability and acceptability of an RMS prototype designed for older adults with chronic HF. The use of RMS can potentially provide older patients with access to health information and feedback and promote daily patient engagement, self-care, and self-efficacy. We utilized a mixed-methods approach to obtain feedback and input from end users; the reiterative process for tapping older adults’ perceptions of usability and acceptability allowed us to maximize the positive elements of the RMS design, implementation, and operation that have not been addressed in previous research in this subgroup of patients with chronic HF. Data from our study will lay the foundation for the design of algorithms and data mining technologies for reasoning, temporal modeling, and detection of patterns that can be adopted to refine existing RMS to meet the needs of older adults with HF.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung, and Blood Institute—National Institutes of Health or the National Institute on Aging.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge funding from the National Heart, Lung, and Blood Institute (1R01HL093466-05) and University of California, Los Angeles, Resource Centers for Minority Aging Research/Center for Health Improvement of Minority Elderly (RCMAR/CHIME) under National Institute on Aging (P30-AG02-1684, PI, C. Mangione).