
Abstract
Introduction
Measuring multiple family member perceptions raises a family science research challenge. Few research studies have included multiple family members. Family congruence research has primarily focused on dyadic relationships of caregiver and care-receiver or resident and staff member (Carter & Carter, 1994; Chappell, 1998; Horowitz, Goodman, & Reinhardt, 2004; Sollie & White, 1997; Tucke & Whitlatch, 2002). Measuring congruence beyond dyadic relationships addresses this family science research gap and contributes to this body of literature because study findings suggest multiple family members, including the resident, do not always perceive resident quality of life alike.
The challenges to define, conceptualize, interpret, measure, and improve quality of life are difficult because “quality of life” is subjective and people identify fundamentals they feel are important to their own quality of life (Aalgaard Kelly, 2013; Challinger, Julious, Watson, & Philp, 1995; Lawton, 1997). Studying family congruence with multiple family members involved in nursing homes is important because a resident’s perception of quality of life varies from their family members’ perceptions. This variation has implications for nursing home expectations and experiences. However, if family members do not agree on the definition of quality of life, then consensus in perceptions and definitions are harder to obtain. Therefore, family congruence regarding quality of life is important to the long-term well-being of family elders.
For this study, the definition of quality of life was a complex set of constructs that defined and outlined the existence of an individual. Conceptual definitions of quality of life originate primarily from two different realms, a medical framework (i.e., historical roots of quality of life literature) and a social science framework (i.e., multidimensional view of quality of life; Lawton, 1991). Guse and Masesar (1999) suggested, “One of the issues in quality of life research is the concept itself. Broadly speaking, quality of life encompasses all areas of human life: environmental and material components and physical, mental, social and spiritual well-being” (p. 528).
Quality of life family congruence (QOLFC) in nursing homes is an important family gerontological issue. Few older adults and their family members look forward to needing help with daily living. Most people want to maintain their independence and not depend on formal or informal long-term care. Older adults are living longer, affecting the need for long-term care service options, influencing the number of families involved with long-term care. Decisions regarding what type of long-term care to select are permeated with emotional, social, and financial complexities for older adults and their families. Ensuring the best possible quality of life is just one goal for long-term care. Adding to the complexity of decision making are the expected variations in family member perceptions with the experience and quality of nursing home life. For several reasons, QOLFC is important to study and further understand. Little is known about how three family members perceive quality of life in the nursing home and the importance to each because it serves as a benchmark in the nursing home industry. QOLFC is also important because if perceptions are not similar among family members, than obtaining improvements to quality of life are not obtainable (Aalgaard Kelly, 2007).
Older adults and families often choose the nursing home when a medical crisis arises, when they perceive they have no other options, or when they find they need around the clock care. The older adult may have no choice but to move from his or her home into an institutional setting. Many Americans feel there really is no place like home (Administration on Aging, 2006, 2012). Making the decision to enter into a nursing home might not be an older adult’s or their family members’ first choice.
The increased number of people affected by long-term care is growing in the United States and in other parts of the world (Markeson, 2003; Quadagno, 2014; Savy, Sawyer, & Warburton, 2014). Population projections include a 38.8% increase in persons aged 64 to 84 between the years 2010 and 2020 (U.S. Census Bureau, 2003, 2004). It is expected by the year 2030, 20% of Americans will be 65 years of age and older (U.S. Census Bureau, 2004), and by 2050, all surviving baby boomers will be over the age of 85 (U.S. Census Bureau, 2014). With this projected increase, it is necessary and critical to focus research on older adults’ and baby boomers’ perceptions of nursing homes. Therefore, understanding older adult expectations and perceptions as well as those of their adult children is important to prepare for future changes in long-term care.
Nursing home residents and family members have a stake in quality nursing home care (Aalgaard Kelly, 2007; McKee, Houston & Barnes, 2002). Families are advocates for their family members living in the nursing home If an outside family member perceives the issues differently than the resident, the outside person might not be an accurate advocate for the resident, possibly resulting in a worse situation for the resident at the nursing home.
The family system is important because perceptions of the nursing home experience vary (Gaugler, 2005; Quadagno, 2014) and the majority of family members involved with relatives before nursing home placement are also involved after placement (Freedman, 1996; Friedemann, Montgomery, Maiberger, & Smith, 1997; Janzen, 2001). Usually, multiple family members are involved in preserving continuity for family members through participation in formal and informal involvement at the nursing home (Friedemann et al., 1997; Gaugler, 2005; Janzen, 2001; Pruchno, Burant, & Peters, 1997). Involved family members include spouses, siblings, children (e.g., adult children, usually), grandchildren, and significant others (Janzen, 2001). Although many family members are involved, variations in family involvement (i.e., in type and amount) exist across families.
Researchers from one study stated, “Institutionalization of a family member represents a significant, often traumatic, event in the history of families” (Friedemann et al., 1997, p. 527). At the point of institutionalization, family members begin to let go of some of their responsibilities and relinquish them to a long-term care facility. Family caregivers who place their family member in a nursing home often experience various emotions such as guilt, sadness, sense of failure (i.e., as a caregiver), and relief from the caregiving burden (Iwasiw, Goldenberg, Bol, & MacMaster, 2003). However, families continue to stay involved with their resident family member (Aalgaard Kelly, 2013; Friedemann et al., 1997; Gaugler, 2005).
This study utilized data drawn from a larger study originally intended to learn about nursing home residents’ quality of life, called Measurement, Indicators and Improvement of the Quality of Life (QOL) in Nursing Homes (Kane, Kane, Giles, Lawton, Bershadsky et al., 2000). The original project was funded by the Health Care Financing Administration (HCFA; that is, Centers for Medicare and Medicaid Services or CMS), and the School of Public Health, University of Minnesota.
Theoretical Frameworks and Development of Conceptual Model
Two systemic theoretical frameworks influenced the conceptual model development, family systems and human ecological theory (Bronfenbrenner, 1979; Bubolz & Sontag, 1993; East, Bubolz, & Sontag, 1993; Hawley, 1986; Whitchurch & Constantine, 1993; White & Klein, 2002). Systems frameworks allowed the examination of multifaceted aspects of QOLFC, with the elder, their family members, and the nursing home environment. Several assumptions of systems frameworks influenced the development of the model because “Systems theories seek to explain the behavior of complex, organized systems of all sorts—from thermostats to missile guidance computers, from amoebas to families” (Whitchurch & Constantine, 1993, p. 325).
Three key assumptions of general systems and human ecological theories were important to the proposed model development: “1) that systems theories can unify science; 2) that a system must be understood as a whole rather than in component parts; and 3) that human systems are unique in their self reflexivity” (Whitchurch & Constantine, 1993, p. 328).
The Conceptual Model diagram (see Figure 1) illustrated how family and the subsystems were examined to understand QOLFC. The family-level dependent variable, referred to as “quality of life family congruence” or “QOLFC” was depicted on the far right side of the model diagram. The square around the QOLFC outcome and represents each family as a system (i.e., three individual perspectives). The dependent variable was guided by the theoretical assumption that the “whole” family is important and not just one individual or some parts. Human ecological theory was depicted in the conceptual model with a circle for each ecological system level. The interaction of the ecosystems (i.e., microsystems) was depicted by the circles and the three arrows intercepting. Factors of each ecosystem level are listed within the corresponding circle. The ecosystems in combination were examined to understand whether and how they influence QOLFC, illustrated with arrows pointing one-way from three circles to the family congruence outcome.

Conceptual model: Quality of life family congruence in nursing homes.
Family Congruence Conceptual Definition
The conceptual definition of congruence in this study was the level of agreement among two or more individuals in their perceptions (Horowitz et al., 2004). Family congruence explored and measured to understand individual family member perceptions and perceptions in combination with one another, with an overall quality of life outcome. QOLFC was based on each person’s perceptions and was highly influenced by the environment in which he or she lived (Boss, Doherty, LaRossa, Schumm & Steinmetz, 1993; Kane, 2001). The conceptual definition of perceptions used in the study was “. . . the process by which environmental information is registered by the senses, organized and made available for use” (Melson, 1980, p. 263, in Bubolz & Sontag, 1993). Perception was defined as how one responds to stimuli in his/her environment by attaching personal and cultural meaning (Aalgaard Kelly, 2007). Therefore, perceptions are subjective to the individual both in meaning and interpretation.
Quality of Life Overall Conceptual Definition
The conceptual definition of quality of life for this study was informed by Lawton’s (1983) definition. He stated, “Quality of life is the multidimensional evaluation, by both intrapersonal and socio-normative criteria, of the person—environment system of an individual in time, past, current, and anticipated” (Lawton, 1983, p. 6). Lawton’s conceptual definition was particularly relevant to this study because of the complex multidimensional examination of quality of life as a concept. There were many approaches to conceptually define aspects of quality of life (Stewart & King, 1994); this study focused on multiple dimensions of quality of life. Various life situations and experiences affected and contributed to one’s perspective of quality of life, “good” quality of life, and what one perceived was important to quality of life. QOLFC was the outcome examined.
Research Questions
The following research questions and hypotheses guided the current study:
Hypotheses
Six hypotheses were developed from the research questions and supported from relevant literature.
Method
Study Design and Data
Data for this study were drawn from a larger study, titled Measurement, Indicators and Improvement of the Quality of Life (QOL) in Nursing Homes, funded by the HCFA, with the School of Public Health, University of Minnesota (Kane et al., 2000). The original data were collected longitudinally in two waves from 40 facilities in five states, including California, Florida, Minnesota, New Jersey, and New York. Two modes of data collection for the original project were utilized: face-to-face interviews with residents and mailed questionnaires to family members. The original study included data collection of resident interviews, staff interviews about the resident, family member questionnaires about the resident, direct observation, and resident records. A stratified sampling procedure was used to include residents with high and low cognitive functioning based on MDS-derived scores with a total of 1,988 residents were included in the sample (Kane et al., 2000).
Sub-Sample Selection and Size
Four criteria were applied for sub-sample selection in the current study. The criteria included (1) nursing home residents that could self-report, (2) nursing home residents with complete data, (3) family-level data including two family members with complete data, and (4) nursing home policy factors available. First, criteria were applied to include only those resident participants who could self-report. As stated previously, nursing home residents both with high and low cognitive functioning were included in the original sample. However, the sub-sample only included those residents who could self-report and provide complete answers to the questions, resulting in a sub-sample of nursing home residents with potentially moderate to high cognitive functioning and verbal skills, based on the MDS-derived scores used with original data collection methods.
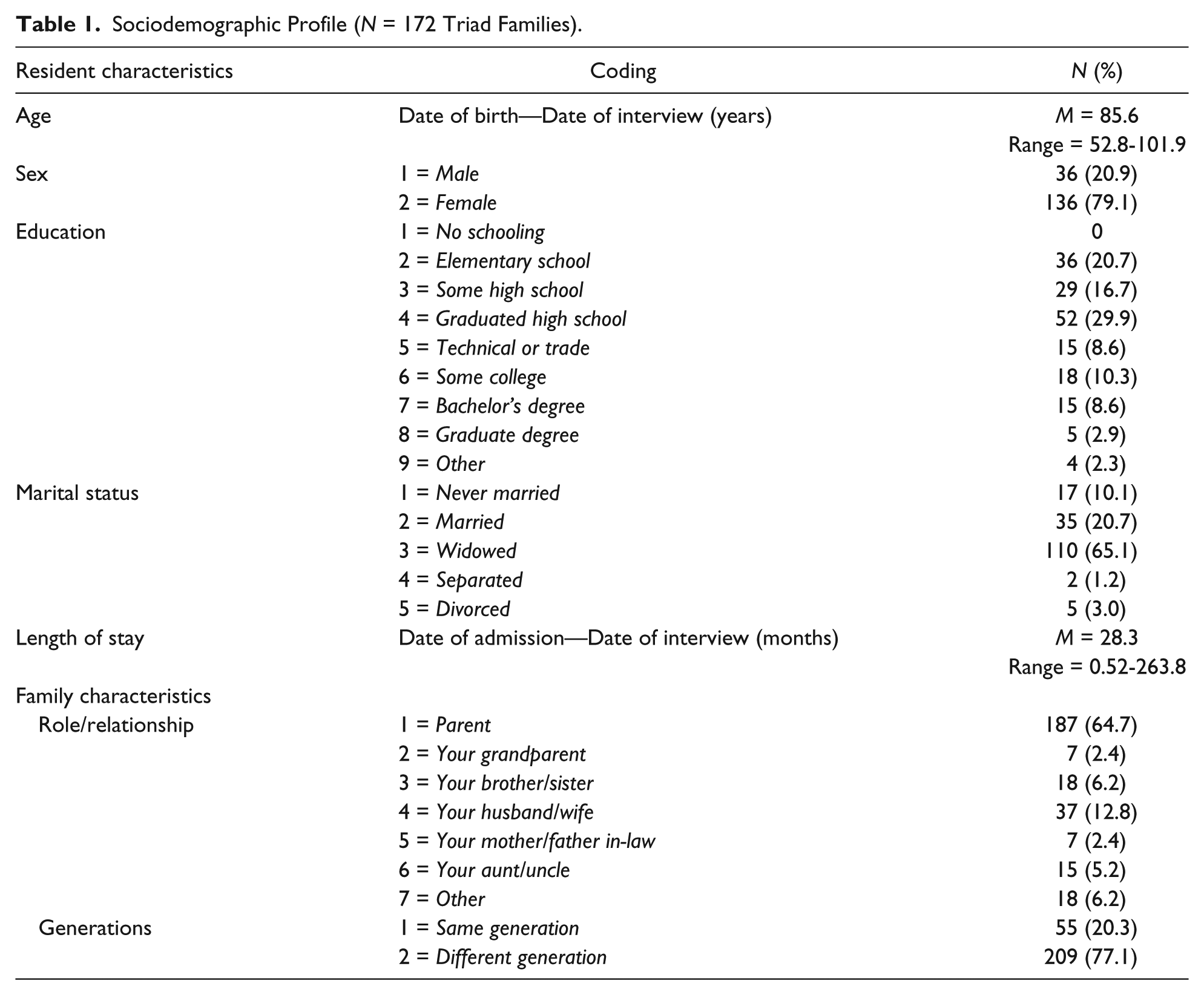
Criteria 2 and 3 included residents with complete data at the individual level and two-person family level (i.e., the majority of families only had one family complete the questionnaire inhibiting inclusion in this study). This comprised a family-level unit of analyses for the study (Larson & Olson, 1999). The final study sample included families with complete data from all three family members for all conceptual model variables, including the nursing home policy variables (i.e., criteria four). The study data were collected in Wave 1 from original resident interviews and from family member questionnaires. The present study sample included 172 families, which consisted of residents and two family members with complete data. The total sample of 172 families included 516 individual family members. Two family members living outside of the nursing home facility were asked a variety of questions about their resident family member, specifically addressing aspects of quality of life. In addition, residents living in the nursing home were asked about their perceptions of their quality of life. There was little racial or ethnic diversity in the sample. Information was collected about resident’s background and characteristics (see Table 1).
Sociodemographic Profile (N = 172 Triad Families).
Measurement of Variables: Operational Measures
Multisource measures
All measures in the model were multisource measures with the exception of five measures in the resident ecosystem component. A multisource measure originated from more than one respondent and then was combined statistically or theoretically to create a new variable (Larson & Olson, 1999; Wampler & Halverson, 1993). Therefore, the dependent variable and independent variables were complex constructs. A “multiplist perspective has become, without question, the standard by which quantitative measures are now evaluated” (Wampler & Halverson, 1993, p. 182) in recent quantitative family social science research (Larson & Olson, 1999; Wampler & Halverson, 1993). Multisource or multplist perspectives can strengthen resident care and life by having potentially more accurate information for decision making. This is especially important for older adults in long-term care who have high rates of impaired cognition both at move in and throughout the duration of their residency.
The model concepts were grounded in the literature, which provided support for why the concepts were valid measures because each has been significant with older adults (Farber, Brod, Feinbloom, 1991; Janzen, 2001). Reliability criteria for each concept included a score above .500, which was recommended as a guideline in the social sciences (Davenport, 2003).
Dependent Variable: Quality of Life Overall
Overall quality of life was measured using 12 items using a multisource 4-point scale. Each member within the triad was asked 12 items: Considering your (relative’s) life at this nursing home, how would you rate the quality of your (his or her) life here in each of the following 12 areas: (a) Feeling physically comfortable, (b) Doing as much for yourself as you want, (c) Having the privacy that you want, (d) Having choice and control in your daily life, (e) Feeling your dignity is respected, (f) Having interesting things to see and do, (g) Feeling life is enjoyable, (h) Following your own interests and preferences, (i) Having good friendships and relationships, (j) Feeling secure and safe, (k) Meeting your spiritual and religious needs, and (l) Your life as a whole. Response categories were 1 = excellent; 2 = good; 3 = fair; and 4 = poor. The 12 items were summed to create a continuous index that ranged from 12 to 48. The alpha reliability score for the 12-item quality of life scale was α = .946. Cronbach’s alpha was statistically reliable for the 12-item scale and suggested high reliability in the social sciences (Davenport, 2003).
Dependent Variable: QOLFC
Family congruence was measured with the following orthogonal data analytic approach (i.e., by combining scores from each member of the triad family). First, each family member’s perception on 12 items of quality of life was examined and summed (scored 12-48). Second, the absolute difference between each of the three family members was configured (i.e., each dyad), and finally, the three difference scores were summed within each family to measure the range of congruent perceptions on resident quality of life (Horowitz et al., 2004; Pruchno et al., 1997).
The summed overall quality of life score informed the creation of a measure for QOLFC by using absolute differences (see Figure 2). Each dyadic family relationship (i.e., resident and primary family member, resident and secondary family member, and primary and secondary family member) had a computed absolute difference score. Next, the three difference scores of each family triad were summed creating an index score. The absolute difference summed scores were interpreted in the following way: The higher the difference score, the more incongruent the family triad. Conversely, the lower the absolute difference score, the more congruent the family triad.
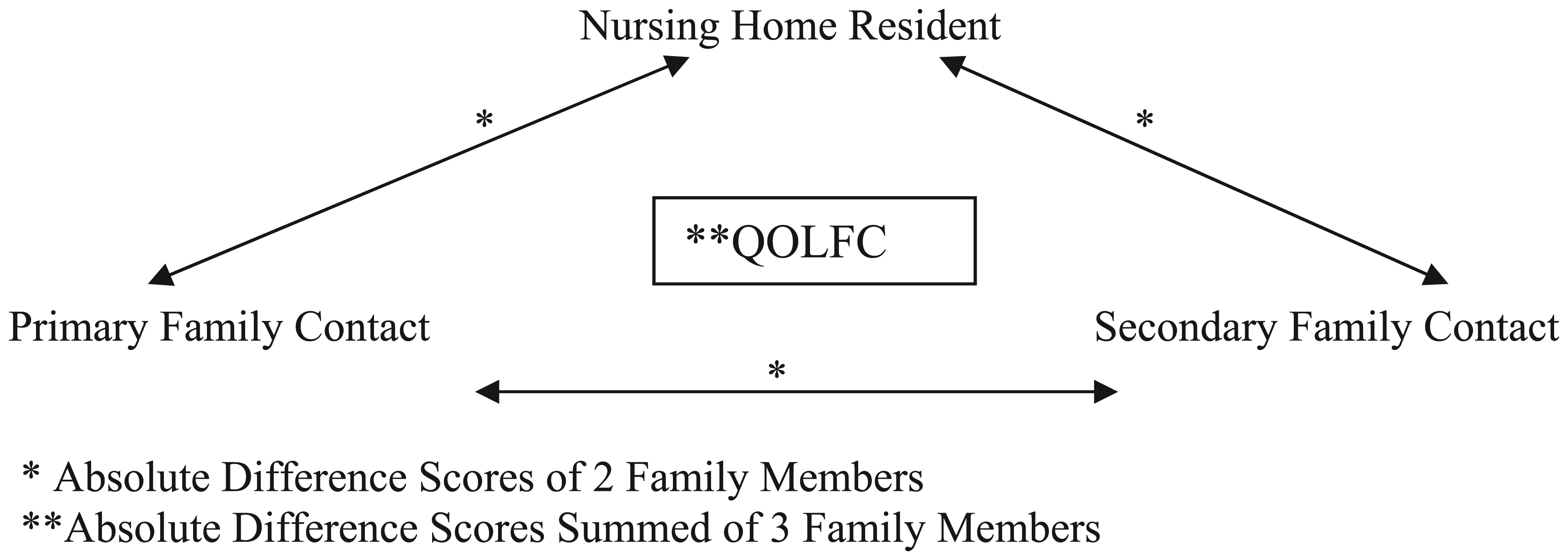
QOLFC dependent variable outcome.
Absolute difference scores represent the magnitude of the differences between elder and each family member, as well as the magnitude of difference between each of the family members. However, absolute difference scores do not show the direction (i.e., positive or negative direction) of the difference in perceptions because the scores retained the positive value of the two informants’ differences (Horowitz et al., 2004; Pruchno et al., 1997).
There were advantages to examine and measure congruent perceptions of family members using absolute difference scores. The score represented the original value of each perception and can be used as an independent variable without confounding the dependent variable. According to Horowitz et al. (2004), “Congruence scores are unique variables that represent the relative standing of the two original scores of the individuals to each other and, thus, they can be completely independent of these original scores” (p. 537). This multivariate analytical method allowed interpretation of triadic differences and non-convoluted measures.
Analysis
Descriptive statistics were run on each independent and dependent variable in the model to determine whether there was sufficient variability in the sample. For the bivariate analysis, first, dyadic differences were measured using interclass correlations to access the difference in perceptions within each family. Second, absolute difference scores were computed and added together which created a triad family congruence score for quality of life. Next, various analyses such as interclass correlations, t tests (i.e., for continuous variables), and analyses of variance (ANOVAS; that is, for categorical variables) were run to determine whether significant differences existed among independent variables and the dependent variable.
The range of family congruence for each outcome influenced how the dependent variable, QOLFC, was created for further analyses. The decision was to retain a continuous variable based on the summed triad difference scores of quality of life. Constructing the continuous QOLFC variable was a sound starting point for a triadic family variable because the difference scores were well dispersed (Aalgaard Kelly, 2007; Howell, 1999).
Bivariate relationships were run and examined to understand whether relationships existed among each of the variables in the model. A test for multicollinearity was run to identify any high intercorrelations among the model predictor variables. The tests for collinearity helped to understand the effects of each variable within the model. Spearman’s Rho correlation and Pearson’s Intercorrelation results are reported to indicate whether a problem was present with multicolinearity within the model (Howell, 1999). If there was high or reasonably high correlation (r < .50) between model variables, it was important to consider how this would affect the multiple regression analyses. Correlations not exceeding .80 were not considered a problem.
Linear regression
Hierarchical linear regression was completed to test the model as a whole (Howell, 1999). Interpretations for a favorable result, accepting the null hypothesis, were identified through the pseudo R2 values to identify goodness of fit as the model builds (Model 1: R2 value to Model 2: R2 value to Model 3: R2 value).
Each ecosystem component was entered as a set with the specific factors explored in each level. This statistical analyses technique provided results of how each set of variables independently influenced family congruence as well as in combination with each other. The model blocks were entered in a three-step, hierarchical procedure. The first block entered as a set, included the independent variables of family intergenerational dynamic factors (generational composition and family involvement). The next two blocks were mediating variables. In the second block, resident personal and social-psychological factors of sex, age, length of stay at the nursing home, psychological well-being, cognitive function, and distance to relative were entered. The final block included the nursing home policy factors of invitation to care conference and family council meeting. The remaining four hypotheses examined which blocks of the model (i.e., ecosystem component) explained variation in QOLFC.
Results
Descriptive and Bivariate Results
QOLFC and Hypothesis 1
QOLFC was measured by first computing a summed quality of life score for each resident and family member. The range of the 12-item quality of life scale was from 12 to 48. Residents within the family triads had higher overall perceptions of their quality of life (M = 37.7) than the other two family members, Family Member 1 (M = 33.4) and Family Member 2 (M = 32.9). Significant differences were found among all three family members’ perceptions (p = .000).
Next, absolute differences were computed for each dyad within the family (i.e., dyad scores: Resident–Member 1; Resident–Member 2; Member 1–Member 2). When the resident was one member of the dyad, the difference scores were higher between resident and Family Member 1 (M = 7.67) and resident and Family Member 2 (M = 7.84) compared with differences between Family Member 1 and Family Member 2 (M = 5.54). This suggests family members living outside the nursing home had more congruence in their perceptions of resident quality of life than the congruence between family member and the resident. Similar to the quality of life scores, the absolute differences of the three dyadic combinations were significantly different (p = .000).
Finally, the three absolute difference scores within each family triad were summed to create the dependent variable, QOLFC. The summed score ranged from 0.0 to 60.60 with a mean of 21.19 and a median of 19.20. This wide range of dispersion justified using a continuous dependent variable for analyses. QOLFC is interpreted from high to low congruence in the following way: Smaller difference scores signify higher QOLFC and greater difference scores signify lower QOLFC. For example, a congruence score of 2 signifies greater QOLFC than a congruence score of 40.
Hypothesis 1 predicted that perceptions of the resident and two family members would differ from each other on Resident’s quality of life. Results of bivariate analyses comparing means of each quality of life index score perception indicated significant differences among resident (M = 37.7), t(171) = 72.12, p = .000 (two-tailed), d = .52, Family Member 1 (M = 33.4), t(171) = 55.04, p = .000 (two-tailed), d = .61, and Family Member 2 (M = 32.9), t(171) = 55.35, p = .000 (two-tailed), d = .59. The expected relationship was supported in the analyses; therefore, Hypothesis 1 was accepted.
Independent Variables
Family intergenerational dynamic factors
Family intergenerational dynamics included family generational composition, formal family involvement, informal family involvement, and overall family involvement (see Figure 2). In this sample, there were more mixed-generation families in which at least one family member was of a different generation than resident (n = 140, 81.4%). Less than one fifth of the sample (n = 32, 18.6%) were families in which resident and family members were all within the same generation.
With regard to family involvement measures, lower scores signify more involvement. This was done to be consistent with the interpretation of QOLFC scores. The mean for formal family involvement was 2.7 with a range from 1.0 to 6. 0. The mean score for informal family involvement was 19.96 with a range from 6.0 to 28.0. For overall family involvement, the mean was 22.62 with a range of 6.00 to 31, suggesting relatively low overall involvement of the families in the sample.
Bivariate analyses of the relationship among family intergenerational dynamic variables and the dependent variable, QOLFC, revealed significant relationships for three of the four independent variables. Generational composition, formal family involvement, and overall family involvement were significantly related to QOLFC; however, informal family involvement was not related to QOLFC. The dependent variable, QOLFC, ranged from high to low; therefore, the lower the family triad score, the higher quality of life congruence; conversely, the higher the family score, the lower the QOLFC.
Generational composition
Generational composition was significantly related to QOLFC (r = .05, p = .05). The bivariate results suggest that mixed-generation composition families had higher QOLFC than families within the same generation. The predominance of families with mixed-generational composition (81.4%), compared with families whose members were within the same generation (18.6%), may have implications for interpretation of these results.
Hypothesis 2 predicted families with mixed-generational composition would have lower QOLFC compared with same generation families. As previously reported, generational composition was found significantly related (M = 1.19), t(171) = 39.86, p = .000 (two-tailed), d = 1.19. Contrary to the relationship hypothesized, mixed-generational composition families were more congruent in their perception of QOLFC than families whose members were within the same generation. Hypothesis 2 is not supported.
Formal and informal family involvement
Formal family involvement was significantly related to QOLFC (r = .17, p = .05). Families with more formal family involvement compared with less-involved families had higher QOLFC. Conversely, families with lower formal family involvement had lower QOLFC. Informal family involvement was not significantly related to QOLFC (r = .11, p = .12).
Hypothesis 3 predicted that families with more informal family involvement than formal family involvement would have higher QOLFC. Formal family involvement, F(1, 171) = 4.93, p = .03, was found to be significantly related to QOLFC; however, informal family involvement was not, F(1, 171) = 2.32, p = .129. The higher QOLFC was greater with more formal family involvement than with lower formal family involvement. These results suggested that families with more formal family involvement also had higher QOLFC. Informal family involvement was not significantly related to QOLFC in the bivariate relationships. Therefore, Hypothesis 3 was not accepted because informal family involvement was not significantly related to QOLFC even though formal family involvement was.
Overall family involvement
When formal and informal family involvement was combined, overall family involvement was significantly related to QOLFC (r = 16, p = .05). This suggested that families who were more involved overall were more congruent in their perception of resident quality of life than those who had less overall involvement in the resident’s nursing home.
Hypothesis 4 predicted that families with more overall family involvement would have higher QOLFC than those with less overall family involvement. Overall family involvement was found to be positively significantly related to QOLFC, F(1, 171) = 4.18, p = .04. Results suggested QOLFC was greater for those families with more family involvement than with less family involvement. Therefore, Hypothesis 4 was supported because families with more overall family involvement had higher QOLFC than those families who were less involved in the nursing home.
Mediator Variables
Resident personal and social-psychological factors
Resident personal and social-psychological factors included sex, age, length of stay at the nursing home, psychological well-being, cognitive functioning, and distance to relatives (see Table 1). In this sample, the majority of residents were female (79.1%) versus male (20.9%). Resident age ranged between 52 and 101 years of age (M = 85.62) with 26.8% between the ages of 52 and 80, 39.9% between ages 81 and 90, and 33.3% older than 91 years of age. Length of stay at the nursing home ranged from 0.53 to 263.79 months (M = 28.21) with the majority of residents (59.5%) having lived more than 1 year at the nursing home. The mean score of resident’s psychological well-being was 29.34, and scores ranged from 13.00 to 40.00. Resident cognitive functioning ranged from 0.00 to 5.00 with a mean of 1.89. The majority of families (72.3%) had family members who lived within an hour from the resident at the nursing home.
Bivariate analysis of the resident personal and social-psychological factors and the dependent variable, QOLFC, revealed significant differences for two variables, sex and cognitive functioning. Age, length of stay, psychological well-being, and distance to relative were not significantly related to QOLFC.
Sex
The sex of the resident was significantly related to QOLFC, (M = 1.79), t(171) = 57.56, p = .000 (two-tailed), d = 1.79. Families of female residents were found to have significantly higher QOLFC than families of male residents.
Cognitive functioning
The level of Resident’s cognitive functioning was significantly related to QOLFC, F(1,171) = 9.363, p = .003. Results indicated that the higher the cognitive functioning of the resident, the higher the QOLFC.
Age, length of stay, psychological well-being, and distance to relative
Age, length of stay, psychological well-being, and distance to relative were not significantly related to QOLFC.
Nursing Home Family Input Factors
Nursing home family input factors included mediator variables in the model: invitation to care conferences at the nursing home and invitation to family council meetings. Nursing home family input factors were measured by combining two family members’ responses to each of these items. This created a three-item categorical variable for each factor (i.e., both yes, one yes–one no, both no). For the most part, family members were invited to participate in a care conference, 75.6% reported both family members had been invited and another 19.8% reported at least one family member had been invited. The invitation to family council meetings results were more dispersed than were those for invitation to care conference. In about a third (33.7 %) of the families, both members were invited to family council meetings; in another third (34.9%), one member had been invited and the other had not; and in just less than a third of the families (31.4%), neither member had been invited.
The results of the bivariate analysis indicated that both invitation to care conferences and family council meetings were significantly related to QOLFC. These results suggest significant differences in QOLFC between family members who were not invited to a family council meeting and those who were, and those who were invited to care conferences and those who were not.
Invitation to care conference
Those who were invited and those who were not invited were significantly different in terms of their QOLFC, t(171) = 30.86, p = .000 (two-tailed), d = 1.29. Family members who were invited to participate in a care conference had higher QOLFC.
Invitation to family council meeting
The invitation to family council meeting was also significantly related to QOLFC, t(171) = 32.34, p = .000 (two-tailed), d = 1.98. Family members who were not invited to participate in a family council meeting had lower QOLFC than those who were invited.
The family intergenerational dynamic variables that were significantly related to the dependent variable, QOLFC, were (a) generational composition, (b) formal family involvement, and (c) overall family involvement. Only informal family involvement was not significantly related to QOLFC. Mediator variables of resident personal and social-psychological factors significantly related to QOLFC were (a) resident’s sex and (b) cognitive functioning. Mediator variables that were not significantly related to QOLFC were age, length of stay, psychological well-being, and distance to relative. In the nursing home family input factors component of the model, both invitation to care conference and invitation to family council meeting were significantly related to QOLFC.
Multivariate results
To test the QOLFC model, linear hierarchical regression was used. Prior to running the multivariate analyses, correlation tests for multicollinearity were examined to identify whether relationships existed between model variables. Only two variables had high intercorrelations (r = .96) which could affect model analysis because of exceeding the recommended problem level (r = .80). The variables to keep in consideration when including and/or eliminating variable(s) in the model were overall family involvement and informal family involvement (r = .96). Overall family involvement was removed from the multivariate analyses because of the high multicollinearity.
The model components were each entered in variable block sets starting with Step 1: Family intergenerational dynamic factors; Step 2: Family intergenerational dynamic factors and Resident personal and social-psychological factors; and Step 3: Family intergenerational dynamic factors, Resident personal and social-psychological factors, and Nursing Home Family Input Factors. The QOLFC model tested using linear hierarchical regression explained 36.3% of the variance with QOLFC. Goodness of fit of the model was determined by the increase in R2 values, also called the coefficients of determination (i.e., measuring the strength of the relationship), with the addition of each component, from Step 1 (R2 = .202) to Step 2 (R2 = .356), to Step 3 (R2 = .363; see Table 2). These results modestly suggest that QOLFC was influenced by all three model components. However, a large percentage of the variance (63.7%) remains unexplained.
Hierarchical Linear Regression Analysis for QOLFC Model (N = 172).

Note. QOLFC = quality of life family congruence.
p < .05. **p < .01.
When family intergenerational dynamic factors were entered alone, it significantly predicted QOLFC, F(3, 172) = 2.318, p = .078, R2 = .202; however, as indicated by the R2, only 20% of the variance in QOLFC could be explained. When resident personal and social-psychological factors were added in addition to family intergenerational dynamic factors added from Step 2, significantly improved the explained variance, F(9, 172) = 2.542, p = .009, R2 = .356. Finally, when both family intergenerational and resident personal and social-psychological factors were added in addition to nursing home family input factors from Step 3, significance improved the explained variance, F(11, 172) = 2.151, p = .020, R2 = .363. Although each step built significantly to improve variance, Step 1 explained the most. The R2 change from Step 1 to Step 2 (ΔR2 = .154) indicates that 15.4% additional variance explained in QOLFC. The R2 change from Step 2 to Step 3 (ΔR2 = .007) contributed less than 1% of additional variance explained. However, the F change in both Steps 2 and 3 was statistically significant suggesting that variables added in both Steps 2 and 3 significantly improved on the model. Step 1 or the family intergenerational dynamic factors, when entered, contribute the most to QOLFC (see Table 2)
To examine the individual factors that contributed to QOLFC, an examination of results in each step was necessary. To reject or accept the last two study hypotheses, several results were examined to identify those factors that were the strongest contributors to QOLFC. All three models were examined because in the full model none of the family intergenerational factors were significant as contributors to QOLFC. Formal family involvement, Informal family involvement, and generational composition were all related to QOLFC but were not significantly related when other factors were considered in the full model (Step 3).
Hypothesis 5 predicted that of the family intergenerational dynamic factors, family involvement would explain more of the variation in QOLFC than generational composition. Family involvement was found to be significantly related to QOLFC (β = .17, p = .05). Generational composition was not found to be significant in Model 1. However, generational composition was significantly related to QOLFC in bivariate analyses, but lost the effect when other factors were considered in the regression model. Therefore, Hypothesis 5 is accepted because family involvement did explain more variation in QOLFC than generational composition (see Table 2).
Hypothesis 6 predicted the combination of family intergenerational dynamic factors while controlling for resident and nursing home factors would influence outcomes of QOLFC. The analyses results supported Hypothesis 6, F(11, 161) = 2.151, p = .05, because the combination of family intergenerational dynamic factors while controlling for resident personal and social-psychological and nursing home factors influenced outcomes of QOLFC (see Table 2).
Mediator Variable Results
Resident personal and social-psychological and nursing home family input factors
Of the resident personal and social-psychological and nursing home family input factors, only cognitive functioning was significantly related to QOLFC. QOLFC was higher for more cognitively functioning residents than for lower cognitively functioning residents (β = 1.92, p = .002). These results suggested that families of residents with higher cognitive functioning have higher QOLFC suggesting these families were more likely to similar perceptions of resident quality of life. In Model 2, the only significant factors were formal family involvement and cognitive functioning, and, in Model 3, only cognitive functioning remained significantly related to QOLFC.
Adjusted model analyses
An adjusted hierarchical linear regression model was run to further investigate the significance change with formal family involvement significance in Model 2 to Model 3. Formal family involvement may have lost significance in Model 3 because of the high correlation between formal family involvement and invitation to care conference at the nursing home (r = .706, p = .000). Therefore, hierarchical linear regression was run again by removing the variable, invitation to care conference from Step 3.
Results of the adjusted analyses indicated that the Step 3 significantly improved the explained variance, F(10, 172) = 2.133, p = .014, R2 = .359. Although each step built significantly to improve variance, Step 1 still explained the most. The R2 change from Step 1 to Step 2 (ΔR2 = .154) indicates that 15.4% additional variance was explained in QOLFC. The R2 change from Step 2 to Step 3 (ΔR2 = .003) contributed less than 1% of additional variance explained and even less explained variance from the tested conceptual model. Formal family involvement was significantly related to QOLFC in the adjusted model (β = 1.93, p = .01), suggesting that the invitation to care conferences confounded the significance in the conceptual model analyses.
Discussion: Summary and Interpretation
The study found that examining QOLFC from a family systems perspective of multiple family voices was important. Specifically, a conceptual model examining QOLFC including social-psychological resident factors and nursing home family input factors held merit and some variance was explained. The following section will provide more context and depth of the study’s findings, limitations, and contributions.
The current study supported the use of a family system’s approach when studying families and aging because congruence in quality of perceptions was different depending on which combination of family members was examined. It is imperative that studies go beyond dyadic relationships to include multiple perspectives within the family to fully understand the phenomenon that is being examined (Aalgaard Kelly, 2007;; White & Klein, 2002). In this current study, three family members’ perceptions of quality of life provided closer to a “whole” family voice (Aalgaard Kelly, 2007). Multiple family members’ perspectives should be considered when decisions are made generally about aging issues and particularly about nursing home care.
The second research question asked whether resident personal and social-psychological factors and nursing home family input factors mediated the relationships among family intergenerational dynamic factors and QOLFC. First, it was hypothesized that families with mixed-generation composition would have lower QOLFC compared with families whose members were all within the same generation. It turned out that this was not the case. Same generation families actually had lower QOLFC than families with mixed-generation composition. This finding contradicts previous research studies that looked at of family structure or generational composition and resident and family member perceptions in long-term care (Alwin & McCammon, 2003; Pruchno et al., 1997). A possible explanation for this divergence could be that generational composition in this study included three family members, not just two. Including more perspectives increases the complexity of the relationship and could account for lower congruence within the triad.
Second, family involvement was expected to explain varying degrees of congruence in family members’ perceptions of quality of life. It was predicted that families with more family involvement would be more congruent than their less-involved counterparts. The current study found that this was the case: More family involvement overall contributed to more QOLFC. This is consistent with the family involvement literature in various long-term care settings (Friedemann et al., 1997; Gaugler, 2005). Family involvement continues after nursing home placement and is enmeshed in the nature of family systems (Caron, 1997; Gaugler, 2005; Janzen, 2001). Therefore, it makes sense that family members who are more involved with the nursing home are more similar in their perceptions of the resident’s quality of life.
Third, the study found that different types of family involvement affected family congruence about the resident’s quality of life. Even though families reported more informal family involvement, they did not contribute to greater QOLFC. This finding was opposite to the predicted relationship in this study as well as what has previously been reported in the literature (Gaugler, 2005; Guse & Masesar, 1999; Noels et al., 2001). Formal family involvement, however, was significantly related to QOLFC. A possible explanation for these results is that structured opportunities for families to interact with the resident and each other foster effective communication and social interaction, thus leading to the possibility that members of a family are more likely to be on the same page when it comes to evaluating their family member’s life in the nursing home setting. These findings support the idea that type rather than amount of family involvement leads to greater QOLFC.
Fourth, overall family involvement was expected to have a greater impact on family congruence than generational composition. Findings confirm that this was the case. Family involvement was significantly related to QOLFC, while generation composition was not. This is encouraging because family involvement is voluntary while generational composition is a given; thus, family members can increase their level of involvement in the nursing home setting and thus improve their ability to assess the resident’s feelings about life quality.
Evidence was found that resident cognitive functioning was important to congruent family perceptions of resident quality of life. Families in which the resident was cognitively functioning had higher QOLFC. This raises challenges for families because the majority of nursing home residents have some form of dementia or dementia-related illness (Markeson, 2003; McKee, Houston, & Barnes, 2002). As residents develop greater degrees of dementia, their cognitive functioning decreases and thus their ability assess their quality of life diminishes.
Finally, this study explored new theoretical ground by including three dimensions of the family ecosystem; family intergenerational dynamic characteristics, resident personal and social-psychological characteristics; and nursing home input characteristics. A test of the full model revealed two critical components that contributed to QOLFC. Study findings provided important evidence for increasing and promoting formal family involvement in the nursing home setting if families are to accurately perceive the resident’s quality of life. First, formal family involvement accounted for 20% or the largest portion of the variance in congruence. Second, cognitive functioning mattered when assessing quality of life. This resident factor accounted for 16% of the variance in QOLFC.
These two factors together suggest that early formal family involvement when the resident is more likely to be at their highest level of cognitive functioning is critical for families’ assessment of their family member’s quality of life in the nursing home. Future research could examine how changes in formal family involvement and resident cognitive functioning affect QOLFC over time.
It should be noted that only one factor, resident cognitive functioning, was a significant predictor of QOLFC in the full model that was tested. In addition, only one family intergenerational factor, formal family involvement, influenced QOLFC. However, this was only when the nursing home mediating variables were removed from the model. Formal family involvement was significantly related to QOLFC when “invitation to care conference” was removed. One explanation for this is that nursing home policies usually mandate care conference meetings with family members, whereas fewer nursing homes use family councils. This difference could explain why the care conference meeting factor was highly correlated with family involvement and the family council meeting factor was not. Finally, it should be noted that nursing home family input factors accounted for only 1% of the variance in QOLFC. This suggests that it is especially important to consider family intergenerational factors such as family involvement along with resident personal and social-psychological factors such as cognitive functioning when evaluating the quality of life of nursing home residents.
In summary, this study proposed that QOLFC would be influenced by family intergenerational dynamic factors, while mediating for resident personal and social-psychological factors and nursing home family input factors. Results indicated that slightly more than one third of the variation in QOLFC was explained by the tested model. Specifically, formal family involvement and resident’s cognitive functioning were the two most influential variables. It is important to note, however, that approximately 64% of the variance was not explained by the tested conceptual model, suggesting key explanatory factors were not included in the model in the current study.
Limitations Summary
Study limitations related to study design, sample, data collection, constructs, and measures are discussed, and suggestions for future research are addressed. The study was designed knowing that there are limitations inherent when using secondary data. First, the sample size ended up being smaller than desired because complete data were needed for all three members of the family triads to construct the family-level measures of family involvement, invitation to care conference and family council, and QOLFC.
Second, the inclusion of all factors identified in the literature to affect quality of life or family congruence was not possible with the data available. It should be noted that the original CMS data set was designed to test quality of life measures, not family congruence. Missing data for key resident characteristics such as marital status, education levels, and religious affiliation prohibited the use of these variables for statistical analyses. Key family member characteristics such as sex, age, educational level, and religious affiliation were not included in this data, making it impossible to test a more comprehensive model of QOLFC. Future research could include demographic characteristics of all family members within the family system.
Third, sampling criteria for the original data collected limits generalizability of the results of the current study. Exclusion of nursing home residents with high cognitive impairment does not accurately reflect the general nursing home population and a sampling bias may have influenced results. Study participants voluntarily filled out the mailed questionnaire. Participating family members could have been more involved with the resident prior to moving to the nursing home compared to family members who did not participate and chose not to complete the questionnaire. Future research could include family member relationship characteristics both before, at, and after move in to the nursing home to control for this and potentially providing more familial relationship factors within families.
A fourth study limitation was that the data were cross-sectional. A guiding assumption of family systems theory is that systems are heuristic and ever changing, and therefore, the assumption was not met because the cross-sectional nature of the data did not allow for an examination of changes over time. If data were longitudinal, changes in family members’ and residents’ perceptions could be studied.
A final imitation was with the measure used to assess family involvement. The original data set included no direct measure of family involvement; therefore, an index was created using three items. One item used in the family involvement index, frequency of visits, had a limited response range for coding. Specifically, the option “more than once a week” limited the ability to consider and measure a wider range of response for frequency of visits.
Contributions Summary
The current study contributed to a better understanding of the complex family relationships involved when a member needs nursing home care. The study’s unique contributions included an examination of a family-level measure of quality of life congruence involving multiple members’ perspectives. This provided empirical evidence for how three family members with different perceptions can be combined to study the “whole” family, congruence, and quality of life.
Findings highlighted the need for nursing homes to provide structured opportunities for family involvement. Results also reinforced the idea that family members will be able to more accurately assess their family members’ nursing home quality of life if they themselves are actively engaged in formal activities of the nursing home environment. With the increase in an aging population and family demand for high quality long-term care, challenges will continue to grow in scope and intensity. This study will contribute to the overall understanding of what is needed if families are to respectfully and effectively care for their aging family members.
This study has implications for professionals, residents, and families involved in the nursing home as a long-term care option. The findings indicated families who were more involved with the resident at the nursing home had higher QOLFC than those families who were less involved. This participation included involvement in care conferences and family councils meetings have. Therefore, nursing home policies and programs could be designed to promote family involvement in these activities.
Cognitive functioning was a factor of resident and family member congruence. Because cognitive impairments are correlated with age, it is important that nursing home staff promote family involvement prior to, at the time of, and after move in to the nursing home. Involved families more accurately perceive the resident’s quality of life. Therefore, they can more effectively advocate on the resident’s behalf. It is especially important to promote family involvement before resident cognitive functioning declines.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.