
Abstract
Introduction
Parkinson’s disease (PD) affects 2% of the adult population above the age of 60 years (Chillag-Talmor et al., 2011). Progressive motor dysfunction leading to dysphagia and immobilization together with autonomic disturbances (Goldstein, 2003), for example, impaired gastric and bladder emptying, may increase the risk for pneumonia (Monteiro et al., 2014) and urinary tract infection (UTI; Katus & Shtilbans, 2014), respectively. Indeed, infections are a leading cause of hospitalizations of patients with advanced PD (Gerlach, Winogrodzka, & Weber, 2011).
Common factors increasing the risk of PD patients for infections and pressure ulcers include impaired mobilization (Skripkina & Levin, 2014), poor personal hygiene, and single or double incontinence (Robinson et al., 2013); both complications have a significant impact on these patients’ prognosis (Bergquist, 2005; Gerlach et al., 2011).
When PD patients are admitted to internal medicine wards due to infection, it is highly important to assess both short-term and long-term prognosis. Such prognostication is essential for decision-making purposes as well as treatment planning and fulfilling professional duty toward patients and families alike. Currently, there are no specific prognostication tools for PD patients hospitalized in these circumstances. Because there are many similarities between the risk factors for infection and risk factors for developing pressure ulcers among PD patients and because the Norton Scale score (NSS) is known to be sensitive in predicting both pressure ulcers development (Bergquist, 2005) and in-hospital complications and mortality (Leshem-Rubinow, Vaknin, Sherman, & Justo, 2013), we hypothesized that it could also serve as a prognostic tool for outcome of PD patients upon hospitalization due to infection.
The aim of the current study was to retrospectively assess the association between the NSS of PD patients upon admission to internal medicine wards with both short-term (e.g., in-hospital mortality, need for mechanical ventilation) and long-term clinical outcomes (e.g., change in discharge destination and 1-year mortality).
Patients and Method
We conducted a retrospective cohort analysis of consecutive PD patients admitted to internal medicine and acute geriatric wards in Sheba Medical Center (SMC), a large tertiary medical center in Israel, between the years 2008 and 2013. The data were retrieved from the computerized registry (medical records) of the SMC. The study was approved by the institutional ethics committee.
Records of patients were included according to the following criteria: (a) diagnosis of PD, ascertained by the coding in the electronic medical record at SMC; (b) chronic treatment with anti-Parkinson medications; (c) age above 30 years at the time of hospitalization; (d) acute hospitalization to internal medicine ward was due to pneumonia, UTI, or both; and (e) valid NSS assessed upon admission. Exclusion criteria included the following: (a) diagnosis of dementia ascertained as recorded in the medical notes and/or treatment with choline-esterase inhibitor or memantine (medications for dementia prescribed prior to index hospitalization), (b) advanced-stage malignant disease, (c) treatment with anti-psychotic medications prescribed prior to index hospitalization, (d) deep brain stimulation (DBS) or any other cranial neurosurgical intervention prior to index hospitalization, (e) diagnosis of Parkinsonism other than idiopathic PD, (f) previously recognized neurological diseases causing neurological dysfunction and\or extra-pyramidal disorders such as progressive supranuclear palsy (PSP), and (g) any medical conditions or medications associated with or causing significant immune compromise.
The rating of the Norton Scale was made by a nurse (in the internal medicine department), pertaining to the patient’s condition at admission. The NSS as well as additional data was retrieved from the patients’ electronic medical records. All available NSS were calculated in accord to accepted components of NSS (Table 1).
Norton Scale for Assessing Risk of Pressure Ulcers.

Note. Calculated as the sum of the scores in all five areas. A score of less than 14 indicates a high risk for pressure ulcer development.
Statistical analysis assessing possible association between the following clinical endpoints and NSS was performed: (a) in-hospital mortality, (b) 1-year mortality, and (c) change in discharge destination (defined as increased/more intensive care facility in any case that the patient arrived from home and was discharged to a nursing home, rehabilitation facility, or was referred to a long-term, sub-acute, hospitalization facility). Associations were calculated using both univariate analysis and multivariate analysis. The p values for analysis of variance (ANOVA) were calculated after adjusting to the main, potentially confounding parameters, known to be significantly associated with survival: (a) gender, (b) age, and (c) plasma creatinine levels.
Results
A total of 528 consecutive PD patients were identified, and their records were reviewed. Four hundred forty-seven patients were excluded from analysis according to aforementioned exclusion criteria. The most common cause for exclusion was dementia (n = 228), followed by treatment by anti-psychotic medications (n = 19). Thirty-one patients were excluded because they were not treated by anti-Parkinsonian medications prior to their hospitalization. Further 152 patients were excluded because of miscellaneous reasons, mostly because of incomplete data, inconclusive diagnoses in their medical records, and missing NSS upon admission.
A total of 81 patients were eligible for analysis, of which 47 (58%) were diagnosed with pneumonia, 45 (55.5%) with UTI, and 11 (13.5%) had both pneumonia and UTI.
Baseline characteristics of all patients included in the analysis are presented in Table 2. Twenty-two (27.1%) PD patients were women and 59 (72.8%) were men (concordant with the known gender ratio in the general PD population worldwide). The mean age was 78.2 ± 8.2 years. The mean NSS on admission was 12.8 ± 3.6 points. The mean duration of hospitalization was 6.2 ± 6.7 days, and the rate of in-hospital mortality was 9.9%.
Patients’ Baseline Characteristics and Clinical Endpoints.
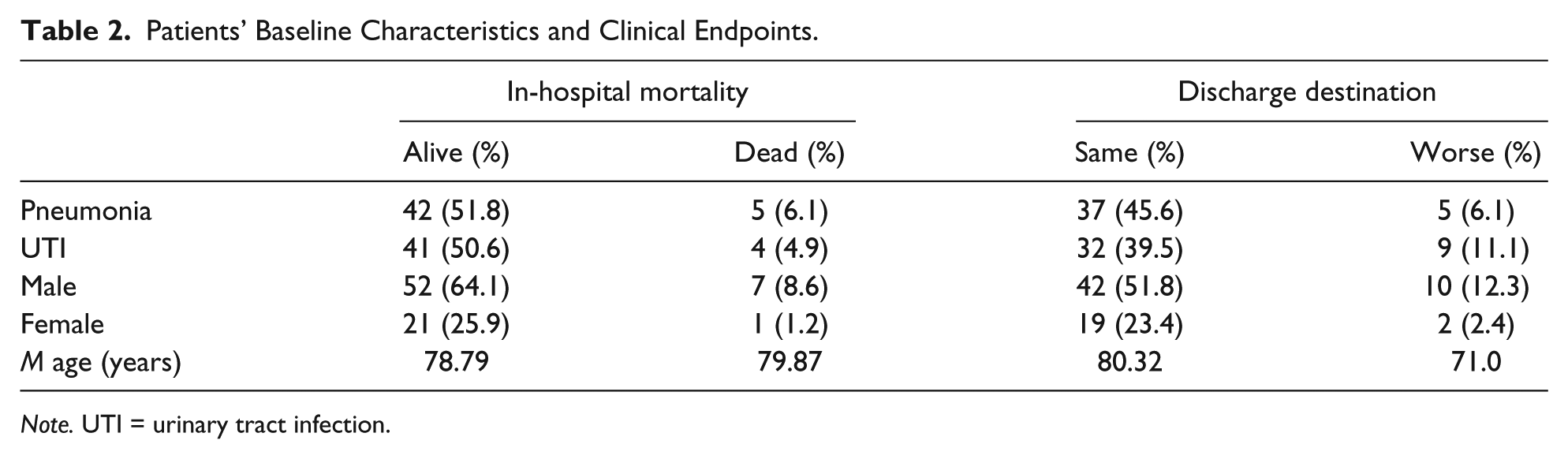
Note. UTI = urinary tract infection.
Figure 1 details the different destinations to which patients were discharged to: 67 patients were admitted from the community, of which only 52 (77.6%) were discharged to their original destination, 1 patient (1.4%) was discharged to a nursing home, 9 patients (13.4%) were discharged to a long-term facility and, 5 patients (7.4%) died during hospitalization. Thirteen patients were admitted from a nursing home, of which only 9 (69.2%) were discharged to their original destination, 2 (15.3%) were discharged to a long-term institution, and 2 (15.3%) died during hospitalization. A single patient who was admitted from a long-term facility died during hospitalization.

Patients’ origin (a) and destination of discharge (b) from hospitalization.
Clinical outcomes that were associated with lower NSS upon admission are described in Figure 2. PD patients who died during hospitalization had significantly lower NSS upon admission (10.0 vs. 13.1, p < .05 by ANOVA, adjusted to age, gender, and serum creatinine level). Worse/more intensive discharge destination was also associated with lower NSS upon admission (10.4 vs. 13.6, p < .01 by ANOVA, adjusted to age, gender, and serum creatinine level). Lower NSS was also found to be associated with increased risk for 1-year mortality (odds ratio = 1.3; 95% confidence interval = [1.09, 1.56], p < .001). PD patients admitted due to pneumonia who deteriorated to respiratory insufficiency leading to mechanical ventilation also had significantly lower NSS (7.3 vs. 13.2, p < .001 by ANOVA, adjusted to age, gender, and renal function).

Clinical outcomes found to be associated with lower Norton Scale score upon admission.
Discussion
PD becomes a major co-morbidity among elderlies hospitalized due to infections. With better treatment available today, many of these frail elderlies will not succumb to infection and are discharged back to their community, nursing homes, or long-term care facilities. It is of utmost importance to better our understanding and foreseeing the prognosis of these patients. The Norton Scale for Assessing Risk of Pressure Ulcers is in widespread use as a prognostic tool for estimating the risk for decubitus ulcers development. As such, it is applied for almost all patients, including those with PD upon admission to internal medicine departments. In the current study, we show that worse clinical outcomes, both in the near and more distant future, are associated with lower NSS in this homogeneous population of patients. It is therefore reasonable to consider using the NSS as a general prognostic tool aside from its original use in the realm of decubitus ulcers prediction. The study results were consistent: Lower NSS was associated with both short-term and long-term survival, with regard to longevity and functional status alike. The authors consider this consistency as another backup to our main outcomes. The authors believe that increased awareness of health care professionals to the short- and long-term prognosis is part of their professionalism. The application of NSS should therefore be a part of the comprehensible evaluation of PD patients during hospitalization (i.e., at a part of discharge planning of both timing and destination).
Limitations of our study stem mainly from the fact that we used rigorous exclusion criteria: Excluding PD patients with dementia and advanced malignancy seemed essential due to the grim effect that these devastating states have on prognosis. Therefore, we were left with a small but homogeneous population of PD patients. Also, our retrospective analysis could only account for association and should be ascertained in further prospective studies.
Conclusion
Lower NSS upon admission of PD patients to internal medicine departments due to pneumonia and/or UTI is associated with worse, short- and long-term clinical outcomes. Adoption of the Norton Scale into the prognostication process of these patients during hospitalization is advisable.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.