
Abstract
Keywords
Introduction
In response to the increasing number of people with dementia (PwD), different types of (respite) services have been put in place for PwD living at home and their family caregivers, including adult day services (ADS) centers. These initiatives aim to offer a structured and meaningful day program to PwD, including health, social, and nutritional services, and by doing so, to provide support and relief to family caregivers (de Bruin, 2009; Fields, Anderson, & Dabelko-Schoeny, 2014; Leitsch, Zarit, Townsend, & Greene, 2001). As such, ADS attendance by PwD may improve outcomes in both participants and their family caregivers for instance in terms of emotional wellbeing, problem behaviours, caregiver burden, and social participation (Fields, Anderson, & Dabelko-Schoeny, 2014; Dabelko-Schoeny & King, 2010; Gaugler et al., 2003b).
Traditionally, long-term care and support services, such as ADS centers, had a strong medical-somatic orientation, with an emphasis on the treatment of reversible impairments. Gradually, a shift has taken place to a more psycho-social approach of care, focusing more on the consequences of the illness. In dementia care, this approach entails a move to more person-centered care focusing on well-being, remaining strengths, and the preservation of the individual’s sense of identity (Finnema, Droes, Ribbe, & van Tilburg, 2000; Taft, Fazio, Seman, & Stansell, 1997). As a result of this paradigm shift, innovations in dementia care have taken place including new types of small-scale and homelike ADS facilities. In these facilities, PwD are encouraged to participate in meaningful activities as part of their normal daily life and integrated in a daily routine (de Bruin, Oosting, van der Zijpp, Enders-Slegers, & Schols, 2010; Kane, Lum, Cutler, Degenholtz, & Yu, 2007; Verbeek, van Rossum, Zwakhalen, Kempen, & Hamers, 2009).
An example of an innovative small-scale, homelike ADS in the Netherlands is the green care farm (GCF). GCFs combine agricultural activities with care services for a variety of client groups, including PwD (de Bruin et al., 2009; de Bruin et al., 2010). They offer access to several (outdoor) environments including gardens, farm yards, stables, and green houses, and stimulate PwD to engage in activities such as caring for animals, sweeping the farm yard, going for outdoor walks, gardening, and preparing meals (de Bruin, 2009; de Bruin et al., 2009). There are currently about 1,100 green care farms in the Netherlands, about 15% of which are open to PwD. Green care farming is not a typically Dutch phenomenon. Also in countries including Norway, Belgium, England, and the United States, the number of GCFs is gradually increasing (Haubenhofer, Elings, Hassink, & Hine, 2010).
Small-scale, homelike care environments may be valuable for PwD in terms of social engagement and involvement in meaningful activities (De Rooij, Luijkx, Declercq, & Schols, 2010; Verbeek et al., 2014). Presently, limited research has been performed on GCFs for PwD. Consequently, it is unknown whether they have similar values as other types of small-scale, homelike environments. Therefore, the aim of this study was to increase our understanding of the value of GCFs for PwD living at home, specifically in terms of social participation. The reason to focus on social participation was that there are indications that social participation of PwD is often restricted due to the consequences of their illness. They tend to have difficulties with maintaining social relationships and with participating in activities, and as such, to remain engaged with society (Alzheimer’s Society, 2013; van der Roest et al., 2007). Because a lack of social participation may have a detrimental effect on health and well-being (Bath & Deeg, 2005; Levasseur, Richard, Gauvin, & Raymond, 2010; Mendes de Leon, 2005), insight into facilities that may maintain participation, and thus may have a positive effect on people’s health and well-being, are considered of importance.
In gerontology, there is a growing interest in social participation and associated concepts. Despite this interest, there is no agreement around a common definition. Several concepts such as social engagement, civic engagement, community involvement, community participation, and social connectedness are associated with social participation, or are used interchangeably with this concept (Anderson & Dabelko-Schoeny, 2010; Johnson & Mutchler, 2014; Levasseur et al., 2010). In our study, we defined social participation as personal involvement in society (e.g., social interactions, recreational activities) and/or participation with a direct benefit for society (e.g., paid employment, volunteer work; Hoeymans et al., 2005).
Method
Study Design and Procedures
This qualitative descriptive study was performed between November 2012 and November 2013. Semi-structured interviews were conducted with dyads of PwD living at home and their family caregivers. We distinguished three groups: (a) PwD who attended day services at a GCF (GCF group), (b) PwD who were on a waiting list (WL) for day services at a GCF (WL group), and (c) PwD who attended day services in a more traditional ADS setting, in this study, operationalized as a facility affiliated with a residential home (i.e., regular day care facility; RDCF group).
In line with our overarching aim, specific objectives that were addressed in this study were:
– To gain insight in the characteristics of PwD and their family caregivers of the three groups;
– To understand the factors associated with initiating adult day services of the three groups;
– To understand the factors associated with selecting the day services setting of the three groups;
– To identify the value of adult day services in terms of specific domains of social participation of the three groups.
To understand the value of GCFs in terms of social participation, we made two types of comparisons:
the GCF group versus the WL group; by doing so, we aimed to determine the potential added value of GCFs for PwD in terms of social participation; and
the GCF group versus the RDCF group; by doing so, we aimed to detect potential differences between both types of day services services with regard to the values attributed to either type of service in terms of social participation.
Our study proposal was submitted to a medical ethical review committee in the Netherlands. Considering the nature of our study, no formal approval was deemed necessary.
Data Collection
Participants were recruited, using purposeful sampling, via care professionals at 10 GCFs and 5 RDCFs in the Netherlands. These professionals provided contact details of eligible participants with permission of the participants concerned. Participants received an information letter that fully explained in lay terms the purpose of the study and what was expected of them. The letter stipulated that their involvement was voluntary, and that they could choose to withdraw at any time with no adverse effects to themselves.
Willingness to participate was discussed with the family caregiver of the PwD. Via this procedure, we enrolled 47 participants. In addition, we put an invitation to participate in the study on the website of a Dutch patient organization for PwD. This resulted in four additional participants. In all, we conducted 51 interviews. To take diversity across the participants into account, we approached GCFs and RDCFs from different regions in the Netherlands and encouraged the care professionals to enroll PwD with varying characteristics (e.g., sex, age, marital status, length of day care attendance). Response rates in the different groups were 91% (GCF group), 26% (WL group), and 41% (RDCF group). Most important reason for non-response in the WL and RDCF groups was the burden of participation. Family caregivers expected that participation would be too stressful for either themselves or their relative with dementia.
Participants were visited at home, and interviews were conducted face-to-face. The interviews lasted approximately 1 hr and were individually performed by three researchers of our team (A.S., C.C.M.M, S.R.dB.). To standardize the data collection procedure, 13 interviews were performed by pairs of researchers. At the start of the interview, we explained how we would handle their data and how their confidentiality would be maintained. We repeated that they could choose to withdraw at any time with no adverse effects to themselves, and verified whether they understood their involvement. The interviews were audiotaped with the interviewees’ permission and transcribed verbatim.
For most interviews, PwD and their family caregivers were interviewed at the same time to give family caregivers the opportunity to either add to or elaborate on the answers given by their relative. In the interviews, we tried to get an answer of the PwD first. In case they were less capable to answer our questions coherently or at all, we turned to family caregivers as a proxy. Three interviews in the WL group and one interview in the GCF group were conducted by proxy only, because the interview would be too burdensome for the PwD. We excluded one interview from the GCF group because a family caregiver was unable to give reliable answers to our questions during the interview.
The interviews covered the following topics:
factors related to initiating day services; reasons to initiate day services in terms of social participation,
factors related to selecting the day services setting; reasons to select either a GCF or RDCF
social participation of PwD including (i) current social participation. For the GCF and RDCF groups, we focused both on the days people were at the ADS center and the days they were not; and (ii) experienced or expected value of day services by PwD in terms of social participation. For the GCF and RDCF groups, the questions regarding this item pertained to the actual experiences of PwD, whereas the questions in the WL group pertained to their expectations. Our operationalization of social participation was based on the definition of Hoeymans et al. (2005), which comprises eight domains: paid employment, volunteer work, family caregiving, membership of an association (e.g., church, sports and hobby clubs, elderly association), cultural activities (e.g., visiting a museum or theater), recreational activities (e.g., walking or cycling), social contacts, and community involvement (e.g., keeping track of the news through reading newspapers, watching the news). In addition, we collected quantitative information on general characteristics of the PwD and their family caregivers (e.g., age, marital status, agricultural background).
Data Analysis
The framework analysis method was used to analyze the data (Boeije, 2005; Bradley, Curry, & Devers, 2007; Gale, Heath, Cameron, Rashid, & Redwood, 2013). The development of the analytical framework (i.e., the code structure) was guided by the principles of a deductive as well as an inductive approach (Bradley et al., 2007). Predetermined codes were used for the development of the initial framework. Additional codes for the analytical framework were developed by reading several interview transcripts and establishing the relevance and coherence of recurring themes. When no new themes emerged from the data, the analytical framework was finalized. The framework was then used by three researchers (A.S., C.C.M.M, S.R.dB.) to assign codes to relevant passages of the interview transcripts (Boeije, 2005; Gale et al., 2013). The researchers checked the others’ coded transcripts and discussed differences to reach consensus. To organize the coded transcripts and sort the data according to themes, a computer program for qualitative data analysis (i.e., ATLAS.ti 7.1.3) was used.
Results
General Characteristics
People with dementia
The GCF and WL groups contained more male PwD with a lower mean age than the RDCF group (Table 1). The majority of the PwD in the GCF and WL groups was married and had a spousal caregiver with whom they lived, whereas in the RDCF group, the majority was widowed and had a non-spousal caregiver with whom most of them did not live. The majority of PwD in the GCF and WL groups lived in a rural area or village, whereas in the RDCF group, the majority were city dwellers. The proportion of PwD with a farming background was higher in the GCF and WL groups than in the RDCF group. The proportions of PwD with a medium or high educational level were higher in the GCF and WL groups than in the RDCF group. About half of the PwD in all groups had an occupational background in the agricultural/environmental sector or in the technology sector. The mean number of self-reported years with dementia was lower in the GCF group than in the WL and RDCF groups. The length and frequency of day services attendance were lower in the GCF than in the RDCF group.
Characteristics of the Study Population, Distinguishing People With Dementia Attending Day Services at a GCF, on a WL for Day Services at a Green Care Farm, or Attending Day Services at RDCF and Their Family Caregivers.
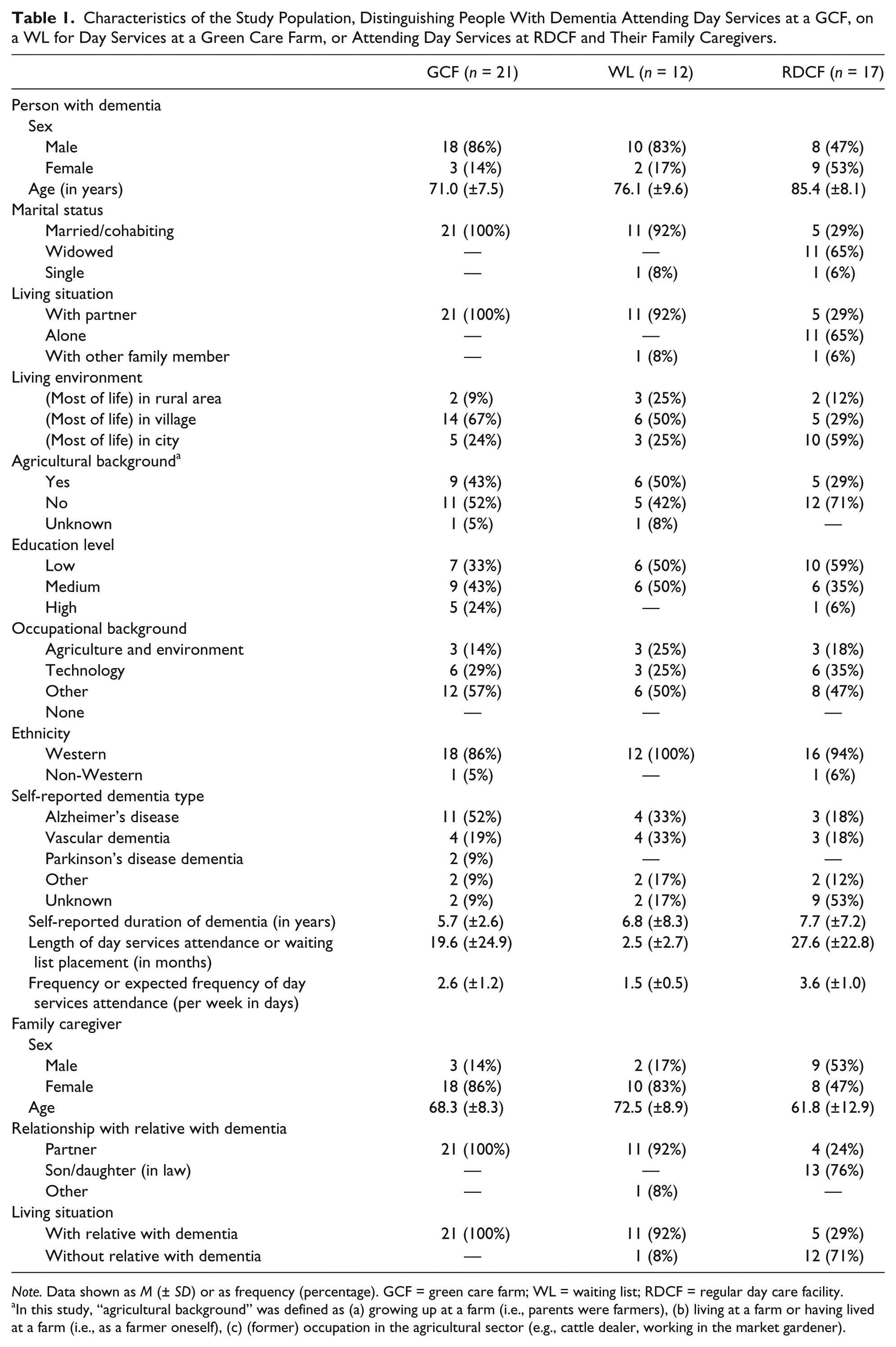
Note. Data shown as M (± SD) or as frequency (percentage). GCF = green care farm; WL = waiting list; RDCF = regular day care facility.
In this study, “agricultural background” was defined as (a) growing up at a farm (i.e., parents were farmers), (b) living at a farm or having lived at a farm (i.e., as a farmer oneself), (c) (former) occupation in the agricultural sector (e.g., cattle dealer, working in the market gardener).
Family caregivers
Both in the GCF and WL groups, the majority of family caregivers were female spouses living with the PwD (Table 1). The GCF and WL groups contained more female caregivers than the RDCF group. Mean age of the family caregivers in the GCF and WL groups was higher than in the RDCF group.
Factors related to initiating day services
In all groups, day services were, above all, initiated for the PwD. In terms of social participation, the most important reason was enabling social interactions.
Yes, I like it that I can go to the farm twice a week. I still remember calling them [the GCF] at a certain point, well, if there was a vacancy I would really like to come, because I felt a bit lonely to be honest. Well, you are at home all day and I am taking out the dog. But that was it, I didn’t see anyone anymore. (PwD from the GCF group)
In all groups, stimulation of activities was also mentioned as a reason to initiate day services, in particular by family caregivers whose relatives with dementia did hardly initiate any activities themselves. Enabling participation of PwD in useful and meaningful activities was mentioned as a third reason, particularly by members of the GCF and WL groups and their family caregivers.
The majority of caregivers in the GCF and WL groups indicated that day services were also initiated for themselves. In the RDCF group, this was mentioned by only a few, mostly spousal, caregivers. Reasons were similar in the three groups, that is, reducing caregiver burden, enabling own activities and social interactions, and increasing freedom. Particularly, family caregivers that experienced change in their social participation due to the illness of their relative, the majority belonging to the GCF and WL groups, often said that day services were initiated to enable their own activities and social contacts. As a family caregiver put it,
Well, it became too much for me. I babysit some children and then I would have to give that up. And I would really regret that, because I would lose all my social contacts. There would be very little left. And I really appreciate it, that we have come to this solution. (Family caregiver of a PwD from the GCF group)
Family caregivers in the WL group indicated more often that day services were initiated for themselves than family caregivers in the GCF group. This may be related to the fact that their relative did not attend day services yet, and that, therefore, the sense of urgency was higher than among family caregivers whose relative already attended day services. As the daughter of a caregiver in the WL group stated,
Well, day services were initiated to relieve my father from caregiving [who was taking care of his wife with dementia]. It allows him the freedom to do something else for a day.
Factors related to selecting the day services setting
Family caregivers in the GCF and WL groups stated that factors related to selecting the day services setting, the characteristics of their relative played a very important role. Several caregivers mentioned that their relative liked to be outdoors and physically active, and was fond of animals and gardening. According to the respondents, GCFs were therefore more appealing, considering the offered activities, the presence of animals, the spacious and outdoor environment, and the atmosphere. As such, in the GCF and WL groups, day services in a farm setting were a deliberate choice. Several PwD in these groups indicated to prefer day services at a GCF to day services in a RDCF.
The green care farm because of its relaxed atmosphere and we don’t want her to associate it with a nursing home. Because she has indicated that she wouldn’t go to a nursing home, ever. And because this is more in line with her past home situation. (Family caregiver of a PwD from the GCF group) Because this is what I like. I’ve always done a lot of work for farmers and market gardeners, and this [the green care farm] is what I really I like. So that decision wasn’t too difficult. And I’ve never regretted it for a moment. (PwD from the GCF group)
A number of PwD and caregivers in the GCF and WL groups stated that they/their relative wanted to attend day services only at a GCF, and not at a RDCF. Reasons given were their (relative’s) dislike of the RDCF’s institutional environment, the activities offered there, and the expectation that they would not connect with the other participants there. As such, the RDCF would not or insufficiently meet their needs and capacities. Some of the family caregivers therefore said that they would have postponed or not initiated day services at all, if day services had been available at RDCFs only.
Well, we have been there to check it out [at the RDCF]. Well, it really is not his cup of tea, to sit there and to play bingo or to do craft work. It is not like him. He is an outdoor man, he has always worked outdoors. One can’t simply say to people like him “please, sit there and stay there.” So this [the green care farm] was a very good solution. (Family caregiver of a PwD from the GCF group) Not yet, anyway, because then he has to spend all day indoors and to play games or something. Particularly because he would have to be indoors, we don’t like that at all . . . . (Family caregiver of a PwD from the WL group)
In the RDCF group, the selection of the day services setting seemed less deliberate and more pragmatic. The interviews revealed that family caregivers and their relatives with dementia did not compare different types of day services settings, as was done in the GCF and WL groups. Unlike the GCF and WL groups, PwD from the RDCF group could not explicitly tell why an RDCF had been selected. None of the family caregivers from the RDCF group mentioned that their relative’s characteristics had played a role in their considerations. They had just followed the advice of the health professional who was managing the process (e.g., case manager, community nurse). In retrospect, they believed that day services at a RDCF were more in line with the preferences of their relative with dementia than at a GCF. Reasons were that the RDCF was nearby, that their relative liked the offered activities, such as singing, chatting, and crafting, that their relative disliked farms and the countryside, or that there was no GCF nearby.
It was all arranged by the health professional of the mental health care organization . . . .we didn’t do anything . . . he said “I think this will suit your husband best.” (Family caregiver of a PwD from the RDCF group) Because it is nearby. We used to drive past the facility; we saw the big logo of [the healthcare organization], we asked for some information, made some phone calls . . . . (Family caregiver of a PwD from the RDCF group)
Some people in the RDCF group said that they were not familiar with the GCF or had not considered it. In their opinion, the RDCF satisfied their wishes.
Family caregivers in all groups said that they considered it important that their relative liked attending day services. Particularly, spousal caregivers explained that they were more willing to let their partner attend an ADS centre and felt less guilty to participate in society, through paid employment and social interactions with family and friends, knowing that their partner enjoyed day services.
I know him so well, that I know that he wouldn’t be as happy at a regular day services center [as at a green care farm], and then it is harder for me to say “You have to go there, because I have to go to work.” (Family caregiver of a PwD from the GCF group)
Social Participation of People With Dementia
GCF group versus WL group
In both the GCF and WL groups, excluding the days of day services attendance at the farm, social participation of PwD encompassed similar activities. The most important domains of social participation were social interactions with family and friends, recreational activities (e.g., walking, cycling), and membership of an association (e.g., church, elderly association, sports club, choir). The interviews revealed that dementia often leads to decreased social participation, because PwD have difficulties with having a conversation or because friends and families do not know how to talk with someone with dementia. The consequences of dementia further made volunteer work or membership of an association difficult or no longer possible.
Comparing the GCF and WL groups as to social participation, including the days of day services attendance at the farm, we observed that GCFs seem to have an added value in this respect. Based on the experiences of the GCF group with the GCF and the expectations of the WL group, we observed that GCF day services were valued for enabling social participation in domains other than “social contacts,” “recreational activities,” and “membership of an association,” that is, the domains “paid employment” and “volunteer work.” Some PwD and/or their family caregivers indicated that the GCF gave PwD (or would give them in case of the WL group) the opportunity to do volunteer work or to have paid employment. Some family caregivers indicated that their relatives thought that they had a proper job or were doing volunteer work (or would, in case of the WL group). Some PwD did not realize that they were attending a day services facility because of the normal daily life (farm) environment. Family caregivers said that they did not want to change this perception because of the dignity of their relative.
So, he now thinks that he is working somewhere else. Even his former colleagues drop by at the farm for a cup of coffee every now and then. (Family caregiver of a PwD from the GCF group)
Other PwD from the GCF group and their family caregivers were less explicit with regard to the domains of social participation but said that the GCF gave them something to do, made them feel useful and meaningful, and made them feel “part of something.” They thought that the type of activities at the farm were (socially) relevant and appreciated how they were approached at the farm. PwD from the GCF group, for instance, said that they worked in the garden or stable (e.g., plucking weeds, repotting plants, sweeping), took care of the animals, did outdoor activities (e.g., painting sheds, logging, making fences), or helped to prepare meals (e.g., getting vegetables from the garden, cutting vegetables, setting the table). They liked to help other participants at the farm to feel responsible for something and to be appreciated. According to family caregivers, at the farm, their relatives were allowed to do what they liked to do and that their remaining capacities were addressed.
I feel useful, it is good for my self-esteem. I am being appreciated, and so are the things I am doing. I have something to offer, to other people, to the soil, to the fruits. Yeah, I like that. (PwD from the GCF group) And the fact that you are working with your hands, and are enjoying yourself. And that you have the feeling that you are doing a proper job. People are not being kept busy, but they do something meaningful. I think that is really important. (Family caregiver of a PwD from the GCF group)
GCF group versus RDCF group
As in the GCF group, in the RDCF group, main domains of social participation were social interactions with family and friends and recreational activities, excluding the days of day services attendance. Compared with the RDCF group, PwD in the GCF group were more often member of an association. As in the GCF group, also in the RDCF group, it was said that dementia often leads to decreased social participation. Compared with the GCF group, less people in the RDCF group participated in society other than the activities offered by the RDCF.
Comparing the GCF and RDCF groups as to social participation, including the days of day services attendance, we noticed that both groups indicated that day services attendance resulted in more social interactions and gave them a sense of belonging. The interviews revealed that interactions were mostly with other day services participants and that people enjoyed and appreciated these contacts. Some people mentioned to find it pleasant to be in a group of “equals.” Others mentioned that the RDCF made them feel useful, for instance, because they could help other participants at the day services facility or could support the health professionals by serving coffee to other participants. Other contacts involved health professionals of the day services facility and the farmer/farmer’s wife. People from both the GCF and RDCF group liked to collaborate with them and to listen to their stories.
Yes, and then in the morning the farmer comes to me and says “Come on P. I have something to do for you.” And then I start with that . . . , often together with him. (PwD from the GCF group) Yeah, this M. [health professional at the day care facility] is wonderful, he can do things I can do as well. And there are people telling stories and then he says “do you know so and so as well?” and they respond “yeah, that was a nice person.” And in that way there is contact. (PwD from the RDCF group)
Some PwD from the GCF group additionally mentioned to have had contact with volunteers living nearby the farm with whom they had coffee, prepared meals, or went cycling or biking.
We also observed differences between the values that were attributed to both types of services in terms of social participation. The interviews for instance revealed that RDCF day services were, in addition to social interactions, valued for enabling social participation in the domain “recreational activities,” whereas GCF day services were additionally valued for enabling social participation in the domains “paid employment” and “volunteer work.” The RDCF group was further less explicit about the value they attributed to the activities offered at the day services facility. Those PwD and their family caregivers who were more explicit about the value of day services gave other reasons for it than the GCF group. People in the RDCF group, for instance, indicated to find the (recreational) activities (such as crafts work, gymnastics, playing games, memory training) fun and enjoyable or to appreciate it that there was sufficient variation in the activities offered. The GCF group was more explicit about the value of day services. They indicated, as discussed above, to find the activities meaningful as they gave them a sense of belonging and made them feel able to contribute to something.
Discussion
This study explored the value of day services at GCFs for PwD living at home in terms of social participation. It is one of few studies that evaluated the benefits of ADS centers for PwD taking a qualitative approach. Our study suggests that both day services at GCFs and RDCFs make PwD feel that they are still part of society. However, the domains of social participation that are addressed by both types of day services facility differ. The most important domains of social participation addressed by RDCFs were social interactions and recreational activities, as was also observed in an earlier qualitative study on ADS (Dabelko-Schoeny & King, 2010). GCFs additionally addressed the domains “paid employment” and “volunteer work.”
An explanation for these findings may be differences in the environmental features of GCFs and RDCFs. Features such as the physical design of the care environment play an important role in the types of activities that are offered to PwD (de Bruin et al., 2010; Verbeek et al., 2009). In this study, we observed differences in the activities of PwD at GCFs and RDCFs. This may also explain why the value of day services, in terms of social participation, differed between both groups. Also, differences between the client populations of GCFs and RDCFs may explain the observed differences. Characteristics such as sex and age may influence people’s preferences and capacities. Although some may prefer to participate in social interactions and recreational activities, others prefer to be involved in domestic activities or activities in line with their former occupation (Manthorpe & Moriarty, 2014). Consequently, also, the value attributed to these activities differed. It is less likely that dementia severity played a role in the observed differences in the value of day services. An earlier study (De Bruin, Oosting, Tobi et al. 2012), suggested that cognitive functioning and (I)ADL functioning were comparable between PwD attending day services at a GCF and PwD attending day services at a RDCF.
Arguably, this study may have been more about values and perceptions of social participation than about social participation per se. The majority of social interactions and recreational activities at the RDCF, for instance, takes place in a long-term care setting. PwD nevertheless indicated that the interactions and activities gave them a sense of belonging to society. Also, working at the farm is not truly paid employment or volunteer work. Still, PwD do not feel they are in a care setting but rather that they are in a normal daily life setting. This is mainly due to the fact that the activities at the farm are part of the daily routine of the farm. As such, PwD think they make a meaningful contribution to society.
As in earlier studies, we observed that the majority of the population of RDCFs were females (Gaugler et al., 2003a; Mossello et al., 2008; Schacke & Zank, 2006), while the majority of the population of GCFs were males and generally younger (de Bruin, Oosting, Enders-Slegers, & Schols, 2012; de Bruin et al., 2009). In line with the study of Manthorpe and Moriarty (2014), our study suggests that males prefer different activities that seem useful and support their identity. Males seem to be less inclined to attend day services in a traditional ADS setting because these services do match their preferences and competences less well. PwD and their family caregivers from the GCF and WL groups indicated that, if day services at a GCF would not have been available, they would have postponed or not initiated day services at all. Day services at GCFs may therefore be considered an important addition to more traditional ADS centers.
Methodological Considerations
This qualitative and explorative study contributes to understanding the value of day services for PwD in terms of social participation, in particular of day services at GCFs. There is no agreement on the definition of social participation and a large variety of definitions and methods for measuring social participation is used. Some of these definitions operationalize social participation as the number of social contacts and activities, other definitions as the meaning of social contacts and activities (Baum, 2000; Guillen, Coromina, & Saris, 2011; Kawachi, Bruce, Lochner, & Prothrow-Stith, 1997; Levasseur et al., 2010; Lindström, Hanson, & Östergren, 2001). On the basis of the definition of Hoeymans et al. (2005), we obtained insight into which domains of social participation were addressed by day services. Although we did not ask after the frequency and duration of the different activities, this study may well provide a starting point for a quantitative follow-up study in which this information should be included to quantify the value of day services.
Semi-structured interviews were conducted with a purposeful selection of three groups of PwD and their family caregivers, which varied in size. However, because the current number of interviews allowed for data saturation, consequences for our findings are likely to be limited. The response rate in the GCF group was high compared with that of the WL and the RDCF groups. Several families approached for the WL and RDCF groups refused participation because they thought that it would be too stressful over and above the stress experienced due to dementia (of their relative). Selection bias should therefore be taken into account, because families with overburdened family caregivers may have been underrepresented in this study. It should further be noted that care professionals at the GCFs and RDCFs enrolled most of the participants for our study, which also may have caused selection bias. Although they were requested to ask all eligible PwD, they may have been reluctant to ask families they knew to be overburdened, less motivated to participate in research, or less positive about day services. Nevertheless, by including respondents from rural and urban regions in the Netherlands and taking variation in personal characteristics into account, we intended to create a representative sample of day services users. We therefore believe to have obtained a reliable insight into the experiences and expectations regarding the value of day services for PwD in terms of social participation.
It should further be noted that, due to the fact that we often interviewed PwD and their family caregivers at the same time, answers provided by one subject may probably have been conditioned by the presence of the other subject. This may be considered as a limitation of our study. At the same time, however, it should be noted that the input of the PwD varied across the interviews, and that the input of family caregivers was often necessary to collect reliable and complete data. From an earlier study among PwD attending day care at a GCF or RDCF in the Netherlands, we learned that the average minimal mental state examination (MMSE) score in these groups was around 20, implying that cognitive impairment was mild to moderate (de Bruin, Oosting, Tobi, et al., 2012). Still, it was not always easy to understand their answers nor were they not always able to answer our questions. We then had to rely on the answers family caregivers gave on their behalf.
Recommendations
Although our study has been performed in the Netherlands, its findings are considered of international value. In an increasing number of countries, as in the Netherlands, due to health system reforms, the responsibility for several health and social care services is shifted from the central government to municipalities. As such, municipalities are responsible for supporting vulnerable citizens, such as PwD and their family caregivers, to sustain independent living and social participation (Hacker, 2009; Kroneman, Cardol, & Friele, 2012; Nowak et al., 2013; Pavolini & Vacarelli, 2012). Hence, municipalities have to know which types of ADS are valuable for PwD in terms of social participation and how these different types address the different domains of social participation. This is of particular importance because our study, in line with earlier studies (Alzheimer’s Society, 2013; van der Roest et al., 2007), suggests that, due to dementia, people have difficulties in maintaining social relationships and in participating in activities.
Based on our findings, we recommend municipalities to take diversity in the preferences and competencies of PwD into account, particularly because it has been suggested that day services utilization is still rather low due to feelings of guilt among family caregivers and insufficient alignment between characteristics of ADS centers and preferences of PwD and their family caregivers (Dutch Alzheimer’s Association, 2014). It may therefore be desirable to make an inventory of the needs and preferences of their citizens with dementia and align ADS centers with these preferences. Health and welfare professionals who refer PwD to ADS centers are recommended to discuss different options for day services with PwD and their family caregivers. Further research may support decisions on which facilities are most suitable for whom, not only in terms of needs and preferences, but also in terms of participant outcomes (e.g. social participation, wellbeing, behavioural problems etc.). Particularly because the domains are expected to be associated.
Although GCFs may positively contribute to social participation of PwD, it is not feasible to deliver ADS at GCFs everywhere because GCFs are not evenly spread across regions and countries. Moreover, the need for day services at a GCF may also vary across municipalities, regions, and countries. However, certain valued characteristics of GCFs (e.g., meaningful activities, outdoor activities, physical activity, green environment) may also be implemented in more traditional ADS settings. This will enable a diverse supply of day services activities, and better alignment between ADS centers and preferences of PwD. This is of particular importance because it is increasingly being recognized that the care environment should be seen as a relevant component of dementia care. Environmental features (e.g., small-scale and homelike features, physical design, access to nature/outdoor spaces, presence of animals) and meaningful activities may positively affect PwD in terms of enhanced quality of life and well-being, and less behavioral problems (Day, Carreon, & Stump, 2000; de Bruin et al., 2010; Kane et al., 2007; Verbeek et al., 2009). Further research is necessary to identify which elements may be implemented in regular ADS settings, and which facilitators and barriers are to be expected.
Conclusion
GCFs are valuable in terms of social participation for a particular group of PwD, of whom some would have postponed or not initiated day services at all, if day services had been offered at RDCFs only. Matching characteristics of ADS centers to the preferences and capacities of PwD is of importance. Diversity in ADS centers is therefore desirable.
Footnotes
Authors’ Note
Annerieke Stoop and Claudia C. M. Molema equally contributed.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dutch Ministry of Economic Affairs (through the Netherlands Organization for Health Research and Development [Grant 72801.0001] and the Dutch Alzheimer’s Association [Grant WE.03-2011-05]).They played no role in the design and execution of the study, the data analysis, or writing of the manuscript.