
Abstract
Introduction
Nearly half of U.S. adults aged 65 or older reported a disability in 2010 (Brault, 2012). Disability is operationally defined as the inability to perform activities of daily living (ADLs), which include basic activities such as walking, bathing, and dressing, and instrumental activities such as managing finances and taking medications (Gold, 2012). The inability to perform these daily tasks often precludes independent living (Wiener, Hanley, Clark, & Van Nostrand, 1990). Age is a potent predictor of ADL impairment (Guralnik, Ferrucci, Simonsick, Salive, & Wallace, 1995; Kamiyama et al., 1999), likely secondary to the physical, cognitive, and sensory impairments that accrue with increasing age (Guralnik et al., 1995; Ostir, Markides, Black, & Goodwin, 1998).
One such sensory system whose function declines with age is the vestibular system (Agrawal, Carey, Della Santina, Schubert, & Minor, 2009; Ishiyama, 2009; Jonsson, Sixt, Landahl, & Rosenhall, 2004). The vestibular organs detect head rotations and translations, as well as orientation of the head with respect to gravity. Vestibular impairment leads to dizziness and imbalance owing to gaze and postural instability (Whitney, Marchetti, Pritcher, & Furman, 2009), and has been associated with an increased risk of falls (Agrawal et al., 2009; Herdman, Blatt, Schubert, & Tusa, 2000; Whitney, Hudak, & Marchetti, 2000). Individuals with specific vestibular disorders such as benign paroxysmal positional vertigo have been observed to have difficulty carrying out ADLs (Cohen & Kimball, 2000). However, whether changes in vestibular function associated with age play a role in age-related ADL impairment is unknown.
The current study uses data from the National Health and Nutrition Examination Survey (NHANES) to evaluate the association between vestibular function and ADL impairment in the U.S. population. NHANES is a large-scale survey that conducted balance testing on more than 5,000 individuals between 1999 and 2004. In addition, detailed information regarding the ability to carry out basic and instrumental ADLs was collected. We hypothesized that vestibular dysfunction, which contributes to imbalance and walking difficulty, would impair the ability to carry out ADLs. This study offers critical insight into the broader consequences of age-related vestibular loss on outcomes of substantial public health significance, including functional capacity, independence, and disability.
Method
Study Population
NHANES is an ongoing cross-sectional survey of the U.S. civilian, noninstitutionalized population (available from http://www.cdc.gov/nchs/nhanes/nhanes_questionnaires.htm). The 1999 to 2004 NHANES performed balance testing on a nationally representative sample of adults aged older than 40 years. A total of 31,126 individuals aged 1 to 85 years took part in NHANES from 1999 to 2004; 9,078 were eligible for balance testing. Participants were excluded from the balance testing protocol if they were aged younger than 40 years, unable to stand on their own, were having dizziness sufficient to cause unsteadiness, weighed more than 275 pounds, had a waist circumference that could not accommodate proper fitting of the standard-sized safety gait belt, needed a leg brace to stand unassisted, or had a foot or leg amputation. Of the eligible adults, 1,797 participants (19.8%) were excluded from balance testing due to inability to stand unassisted. Of the remaining 7,281 participants, 1,330 (18.3%) were further excluded due to safety concerns and participant refusal, further reducing the sample size to 5,951. Included participants were more likely to be younger and White. Sample weights for the combined 6-year sample were used per National Center for Health Statistics (NCHS) guidelines (Johnson et al., 2013).
Vestibular Testing
Vestibular testing consisted of the Modified Romberg Test of Standing Balance on Firm and Compliant Support Surfaces. Test Condition 4 was designed to test vestibular function exclusively: Subjects had to maintain balance on a foam-padded surface (to obscure proprioceptive input) with their eyes closed (to eliminate visual input), thereby relying exclusively on vestibular information to maintain upright stance. Test failure was defined as a subject (a) needing to open the eyes, (b) moving the arms or feet to achieve stability, or (c) beginning to fall or requiring operator intervention to maintain balance within a 30-s interval. We categorized participants as having vestibular dysfunction if they did not pass Test Condition 4. Of the 5,951 balance testing participants, 271 (4.5%) did not pass prior test conditions and did not participate in Test Condition 4. An additional 100 participants (1.7%) had missing data for Test Condition 4. An additional 563 participants were excluded because they had missing ADL data. The final sample size was 5,017 participants. Further vestibular testing procedure details are available at http://www.cdc.gov/nchs/data/nhanes/ba.pdf.
ADLs Assessment
Questions related to performing ADLs were part of the larger NHANES survey on physical functioning, which has been found to have good internal consistency, content, and construct validity (C. Cook & Pietrobon, 2006; C. E. Cook et al., 2006). Participants were scored as 1 = no difficulty, 2 = some difficulty, 3 = much difficulty, and 4 = unable to do for each of 19 specific basic and instrumental ADLs. A composite ADL score was computed by adding all the individual ADL scores together, with higher numbers indicating greater levels of ADL disability (for a maximum score of 76 = 19 items × 4 points). The composite score was rescaled by subtracting 19 from the maximum score to allow the index to have a minimum value of zero, ranging from 0 (no impairment) to 57 (complete impairment on all ADLs). The total number of ADL impairments was calculated by adding up each individual ADL impairment. Impairment for each individual ADL was defined as having much difficulty or unable to perform for that particular ADL. Each individual was given a score from 0 to 19, representing the number of impairments out of the 19 ADLs. There were 563 participants (10.1%) with vestibular data that had missing data on ADL.
Demographic and Health-Related Variables
Race-ethnicity was grouped as non-Hispanic White (hereafter, “White”), non-Hispanic Black (hereafter, “Black”), Mexican American, or Other. Education was grouped as less than high school, high school diploma (including General Educational Development [GED]), and beyond high school. Six participants had missing education data. Smoking pack-years were computed based on number of years smoked and number of cigarettes smoked per day, and participants were divided into categories including never smoked, less than 20 pack-years of smoking, and more than 20 pack-years of smoking. There were substantial missing data (N = 260) on the quantity of tobacco smoked, so a separate category was made for “ever smokers with unknown pack-years” (no participants ended up with missing data). Hypertension was defined based on physician diagnosis, use of antihypertensive medication, an average systolic blood pressure more than 140 mmHg or an average diastolic blood pressure more than 90 mmHg at the time of examination (9 participants had missing data). Diabetes was defined based on physician diagnosis, use of antihyperglycemic medication, an 8-hr fasting glucose more than 126 mg/dL, or a nonfasting glucose more than 200 mg/dL (95 participants had missing data). Stroke was defined based on physician diagnosis (7 participants had missing data).
Audiometric and Visual Acuity Measures
Pure-tone average hearing thresholds at the frequencies 0.5, 1, 2, and 4 kHz were computed in the better hearing ear (3,452 participants had missing data). Nonrefracted visual acuity was coded as 20/20 (20), 20/30 (30), 20/40 (40), 20/50 (50), 20/60 (60), 20/70 (70), 20/80 (80), 20/200 (200), 20/200+ (666) in the better seeing eye (103 participants had missing data).
Statistical Analysis
The main outcome of interest was ADL impairment. The predictor variables were vestibular dysfunction, demographic variables, and health-related variables. The study population was stratified into age groups (40-49 years, 50-59 years, 60-69 years, and older than 70 years). Mean ADL impairment scores and total number of ADL impairments were compared across demographic and health-related variables in bivariate analyses using one-way ANOVA. Multiple linear regression models using fixed effects were developed by including basic demographic and health-related factors that are known to influence ADL impairment and that maybe associated with vestibular dysfunction (Louie & Ward, 2011). The models for the composite ADL impairment score and the total number of ADL impairments met the assumptions of linear regression in the following ways: (a) the models were linear when observed values were plotted against predicted values, (b) there was no multicollinearity of the predictor variables as assessed by the variance inflation factors, and (c) there was equal variance of the residuals when they were plotted against the predicted values. The composite ADL impairment score and total number of ADL impairments, however, were not normally distributed, even after log transformation of the variables. We also evaluated the association between vestibular dysfunction and impairment in each of the individual ADLs using multiple logistic regression. For these analyses, we defined ADL impairment as having “much difficulty” or “unable to perform” the particular ADL.
Structural equation models were developed to evaluate whether vestibular function mediated the association between age and ADL impairment. Parallel mediation by visual impairment, vestibular dysfunction, and hearing loss was considered. Structural equation models were adjusted for demographic and health-related variables.
All statistical analyses were conducted with Stata Version 13 (College Station, TX).
Results
A total of 5,017 participants were included from the 1999 to 2004 NHANES (Table 1). The mean age of the study population was 57.9 years (range 40-85 years). The mean ADL impairment score was 2.0 (range 0-44) and the mean number of ADL impairments was 0.5 (range 0-16). Mean ADL impairment scores were significantly higher among participants with vestibular dysfunction in bivariate analyses (3.0 vs. 1.4, p < .0001; Table 1). Individuals with vestibular dysfunction had a higher number of ADL impairments (0.6 vs. 0.3, p < .0001; Table 1). Females had a significantly higher mean ADL impairment score and total number of ADL impairments, compared with males, and higher education was significantly associated with lower ADL impairment. Heavy smoking was also associated with a significantly higher mean ADL impairment, as was a history of hypertension, stroke, diabetes, hearing loss, and visual impairment (Table 1). In addition, there was no significant difference in ADL impairment score or number of ADL impairments by race/ethnicity.
Population Characteristics and ADL Impairment. a
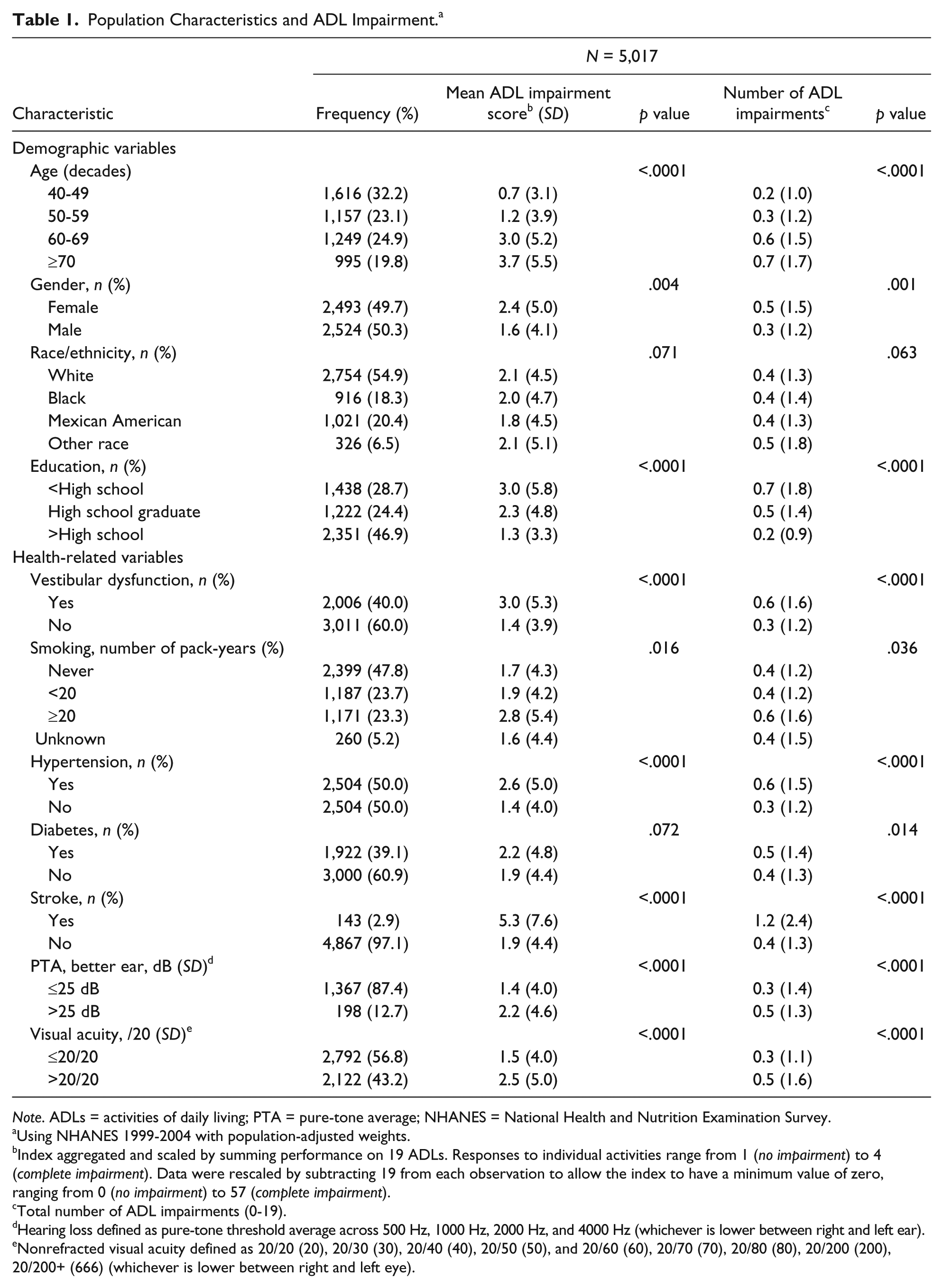
Note. ADLs = activities of daily living; PTA = pure-tone average; NHANES = National Health and Nutrition Examination Survey.
Using NHANES 1999-2004 with population-adjusted weights.
Index aggregated and scaled by summing performance on 19 ADLs. Responses to individual activities range from 1 (no impairment) to 4 (complete impairment). Data were rescaled by subtracting 19 from each observation to allow the index to have a minimum value of zero, ranging from 0 (no impairment) to 57 (complete impairment).
Total number of ADL impairments (0-19).
Hearing loss defined as pure-tone threshold average across 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz (whichever is lower between right and left ear).
Nonrefracted visual acuity defined as 20/20 (20), 20/30 (30), 20/40 (40), 20/50 (50), and 20/60 (60), 20/70 (70), 20/80 (80), 20/200 (200), 20/200+ (666) (whichever is lower between right and left eye).
We evaluated the association between vestibular dysfunction and ADL impairment score using multivariable linear regression (Table 2). Individuals with vestibular dysfunction were significantly more likely to have a higher ADL impairment score in adjusted analyses (β = .75, 95% confidence interval [CI] = [0.36, 1.14]). We also evaluated the association between vestibular dysfunction and the total number of ADL impairments using multivariable linear regression models (Table 2). We observed that individuals with vestibular dysfunction were more likely to have a higher total number of ADL impairments (β = .21, 95% CI = [0.09, 0.33]. The vestibular dysfunction coefficient was comparable with the influence of heavy smoking (β = .21, 95% CI = [0.06, 0.36]) and hypertension (β = .10, 95% CI = [0.02, 0.18]) on ADL impairment. The association between vestibular loss and composite ADL impairment score by age category was evaluated to see if associations differed by age. We observed that associations were significant across age categories with the exception of age 60 to 69 years, β = 1.00 (p = .008) for ages 40 to 49 years, β = .56 (p = .034) for ages 50 to 59 years, β = .34 (p = .440) for ages 60 to 69 years, and β = 1.07 (p < .0001) for ages ≥70 years. Similarly, with respect to total number of ADL impairments, we observed that associations were significant with the exception of the 60- to 69-year-old age category, β = .25 (p = .069) for ages 40 to 49 years, β = .25 (p = .001) for ages 50 to 59 years, β = .04 (p = .703) for ages 60 to 69 years, and β = .27 (p = .005) for ages ≥70 years.
Multivariable Regression Model of the Association of Vestibular Dysfunction With ADL Impairment Score and With Total Number of ADL Impairments. a
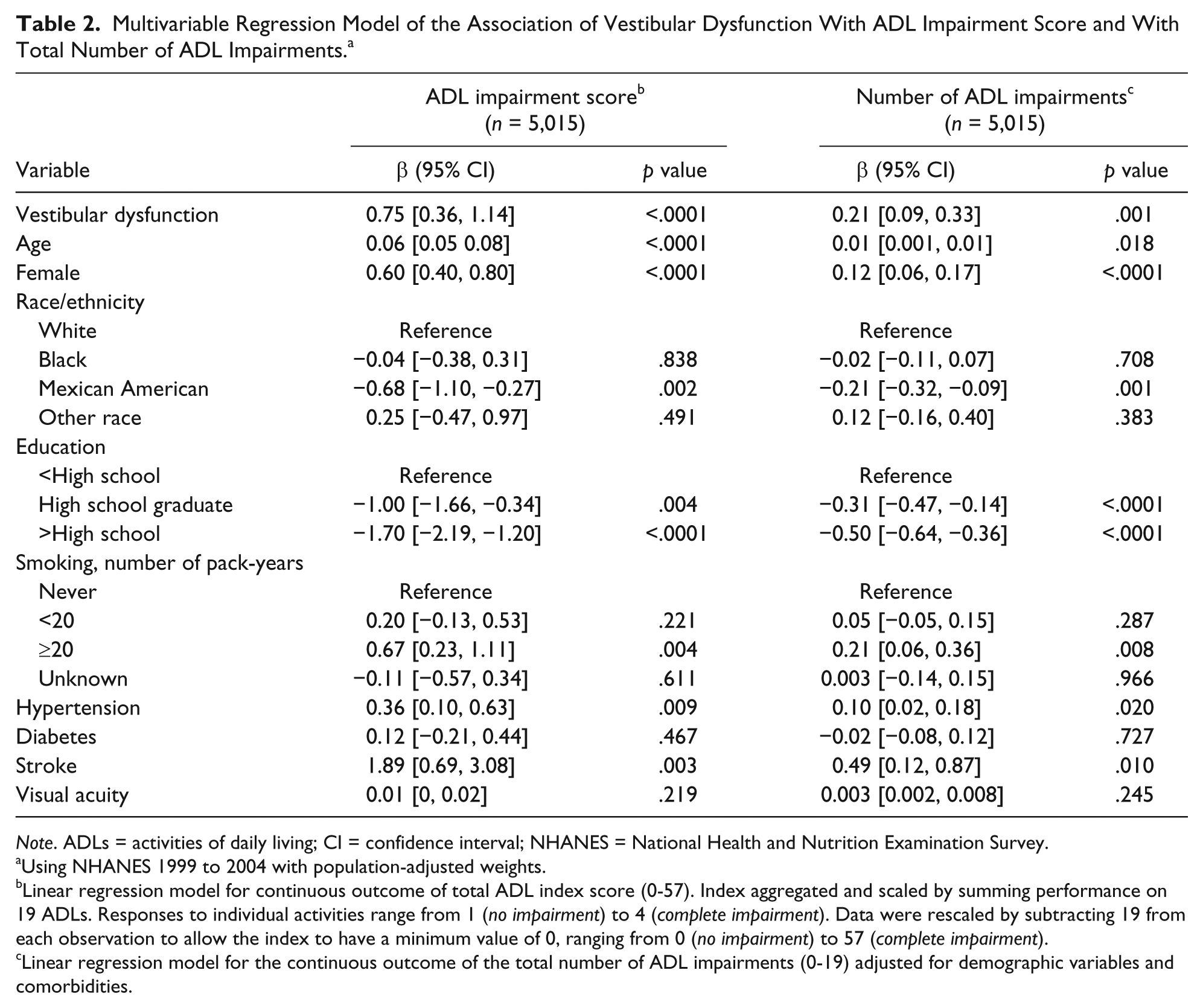
Note. ADLs = activities of daily living; CI = confidence interval; NHANES = National Health and Nutrition Examination Survey.
Using NHANES 1999 to 2004 with population-adjusted weights.
Linear regression model for continuous outcome of total ADL index score (0-57). Index aggregated and scaled by summing performance on 19 ADLs. Responses to individual activities range from 1 (no impairment) to 4 (complete impairment). Data were rescaled by subtracting 19 from each observation to allow the index to have a minimum value of 0, ranging from 0 (no impairment) to 57 (complete impairment).
Linear regression model for the continuous outcome of the total number of ADL impairments (0-19) adjusted for demographic variables and comorbidities.
We then determined the odds of ADL impairment associated with vestibular dysfunction for each of the 19 individual ADLs in adjusted analyses (Figure 1). We observed that vestibular dysfunction was associated with significantly higher odds of impairment for 9 of the 19 different ADLs. These included managing money (OR = 2.64, 95% CI = [1.18, 5.90]), getting in and out of bed (OR = 2.02, 95% CI = [1.18, 3.47]), standing up from an armless chair (OR = 1.80, 95% CI = [1.09, 2.95]), walking up to 10 steps (OR = 1.66, 95% CI = [1.06, 2.57]), standing for long periods of time (OR = 1.65, 95% CI = [1.29, 2.09]), walking for a quarter mile (OR = 1.63, 95% CI = [1.13, 2.34]), house chores (OR = 1.55, 95% CI = [1.12, 2.13]), stooping/crouching/kneeling (OR = 1.53, 95% CI = [1.19, 1.96]), and going out to movies/events (OR = 1.49, 95% CI = [1.05, 2.12]).

Odds of ADL impairment associated with vestibular dysfunction.
We developed structural equation models to explore the association between aging and ADL impairment score, and to evaluate for potential mediators of this association including vestibular function, visual function, and hearing (Figure 2). We observed that vestibular function mediated 21.7% of the association between aging and ADL score. Visual impairment and hearing loss mediated 0.8% and 8.9% of the association between age and ADL impairment, respectively.

Structural equation modeling and mediation analyses.
Discussion
We observed in this analysis of nationally representative data a significant association between vestibular dysfunction and ADL impairment. In this community-dwelling population, the overall level of ADL impairment was low and vestibular dysfunction only conferred an increase in the total number of ADL impairments of 0.2. Nevertheless, vestibular dysfunction was associated with a level of ADL impairment comparable with other significant health-related factors and comorbidities, such as a decade of age, heavy smoking, and hypertension. Moreover, we found that vestibular dysfunction appeared to account for nearly 22% of the association between age and ADL impairment.
This study confirms and extends prior work also reporting an association between vestibular dysfunction and ADL impairment. A population-based study in Germany observed that 40% of adults with self-reported vestibular vertigo had interruption of their daily activities, compared with 12% of adults with nonvestibular dizziness (Neuhauser et al., 2008). Another study of more than 2,000 patients presenting to a dizziness referral clinic for vestibular disease found that a majority of patients experienced a moderate-to-severe impairment in daily functioning (Ten Voorde, van der Zaag-Loonen, & van Leeuwen, 2012). Moreover, one study of individuals with peripheral vestibular disease reported that 1 month of vestibular rehabilitation resulted in improvement of self-perceived ability to perform ADLs (Cohen & Kimball, 2003), further supporting a link between vestibular dysfunction and ADL impairment. The need to measure disability in patients with vestibular disease has been previously recognized, resulting in the development of the Vestibular Disorders Activities of Daily Living Scale (Cohen, Kimball, & Adams, 2000). Our study adds to this literature due to the in-depth assessment of ADL impairment in NHANES, allowing us to determine the specific activities influenced by vestibular function. Moreover, we report from our structural equation models that vestibular loss may be one of the key mediators of the association between age and ADL impairment.
When we explored the association between vestibular dysfunction and specific ADLs, we observed the strongest association with the ability to manage money (i.e., balance a checkbook, pay bills). This result was somewhat surprising: We had expected vestibular loss to result in difficulty primarily in mobility-based activities. Indeed, the next strongest associations were observed with transferring from bed, standing from a chair, walking 10 steps, standing for long periods of time, and walking one-quarter mile. The association between vestibular dysfunction and money management may reflect the link between the vestibular system and cognitive domains such as visuospatial processing, which are just beginning to be recognized. A seminal study previously observed that individuals with bilateral vestibular loss had deficits in spatial memory and navigation, and had concomitant hippocampal atrophy on neuroimaging (Brandt et al., 2005). Subsequent studies have observed a link between horizontal body motion and processing of numbers in which leftward and rightward motion facilitated faster processing of smaller and larger numbers, respectively (Hartmann, Grabherr, & Mast, 2012; Loetscher, Schwarz, Schubiger, & Brugger, 2008). These findings suggest a link between vestibular input and numerical processing mediated by spatial cognition, and may explain our observation of a strong association between vestibular dysfunction and the inability to manage money.
We note several limitations of this study. The postural metric used in NHANES to estimate vestibular function is not a specific physiologic test of peripheral vestibular function and may also be affected by a participant’s strength and motor coordination. Moreover, this was a cross-sectional study and cannot support causal inferences, including in the structural equation models. These findings serve to generate hypotheses that can be substantiated in longitudinal data analyses. In addition, the NHANES survey was administered to community-dwelling individuals, and this study was restricted to individuals who were able to perform balance testing. Thus, our findings may not be applicable to individuals with greater levels of disability or who were institutionalized. This exclusion of more disabled individuals may explain why vision loss did not appear to mediate any of the associations between age and ADL impairment. Individuals with any significant degree of visual impairment may not have been able to perform balance testing and may be less likely to live independently in the community. Alternatively, the metric of vision loss measured in NHANES—visual acuity—may have less influence on ADL impairment relative to other dimensions of visual function such as visual fields or contrast sensitivity. Moreover, we could not evaluate whether anxiety or depression partially explained the association between vestibular dysfunction and ADL impairment, given that anxiety and depression and balance function were not assessed in the same NHANES cycles. Finally, the composite ADL impairment and total number of ADL impairment scores were not normally distributed even after log transformation of the variables. More disabled individuals living in institutional settings and individuals younger than 40 years were excluded from the study, which may have limited normality of the ADL score distribution.
This study suggests that vestibular dysfunction influences the ability to perform basic tasks that allow independent living. These findings provide a broader understanding of the potential individual- and societal-level impacts of vestibular loss in older individuals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.