
Abstract
Introduction
The ability and efficiency of mastication is the first step in the digestion of food, and this ability declines with age (Locker, 2002; Morley, 2001; Takata et al., 2006). Masticatory ability is closely associated with maintaining adequate nutrition in older populations (de Morais et al., 2013; Kwon, Suzuki, Kumagai, Shinkai, & Yukawa, 2006; Walls, Steele, Sheiham, Marcenes, & Moynihan, 2000). Lower masticatory ability reduces the variety in a person’s diet, leading to malnutrition, weight loss, and a low body mass index (BMI) among the older adults (Nordenram, Ljunggren, & Cederholm, 2001; Tamura, Bell, Masaki, & Amella, 2013). It is also reported that impairment of mastication is associated with general health status (Miura et al., 1998; Miura, Araki, & Umenai, 1997; Miura, Kariyasu, Yamasaki, Arai, & Sumi, 2005; Sun et al., 2007), quality of life (QoL; Brennan, Spencer, & Roberts-Thomson, 2008; Kimura et al., 2009; Takata et al., 2006), and cognitive function (Elsig et al., 2015; Mummolo, Ortu, Necozione, Monaco, & Marzo, 2014; Teixeira et al., 2014). Active life expectancy also related chewing ability (Nasu & Saito, 2006). Impaired masticatory ability often leads to frailty and institutionalization. Maintenance or recovery of sufficient chewing ability for older adults is related to a longer active life expectancy.
This study investigated whether self-rated masticatory ability is associated with a self-reliant life with adequate subjective health conditions in a community-dwelling older population. The older population in Japan is expanding over time and accounts for more than 25% of the population (i.e., 32 million). The percentage of long-term care recipients above 65 years of age was 17.9% in May 2014. The gap between life expectancy and active life expectancy is 9.13 years in females and 12.68 years in males, respectively, and this is a pressing issue in Japan with increasing older populations, despite the fact that society has achieved the highest level of life expectancy. The extension of active life expectancy constitutes a pivotal issue for not only the well-being of the older population but also the demographics and socioeconomic of the society.
Method
Participants
This study population consists of participants in survey, which is a prospective and population-based study, and is designed to identify factors for self-reliant life in community-dwelling older adults in Japan (Kayama, Hironaka, & Tani, 2014). This study recruited 1,706 individuals who were 65 years and above, living in Kumamoto City, and obtained informed consent from 1,554 of those subjects. Those subjects had involvement with regional welfare commission volunteers and community comprehensive care center staffs. The study excluded subjects who died, moved, or were hospitalized during the study, and thus, 1,377 individuals participated (459 men and 910 women, mean age 79.8 ± 6.6 years). This structured questionnaire survey was conducted in conjunction with regional welfare commission volunteers and community comprehensive care center staffs.
Data Collection
The methods for data collection were described previously (Kayama et al., 2014).
Subjective health status was established by questionnaire with four levels of choice; queried items included “very healthy,” “moderately healthy,” “not very healthy,” and “not healthy.”
Instrumental activity of daily living (iADL) was evaluated using an eight-item questionnaire that included walking for 15 min with or without a cane; going out at least once a week, answering the telephone; and using home electronic appliances, daily shopping activity, taking trash out, managing money, and ventilating rooms.
Forgetfulness was queried by the question item: “Have you been horribly forgetful lately.”
Daily shopping activity was compared among those living with their family/caregiver and those who did not. Daily shopping activity was categorized as supermarket store, convenience store, home delivery, and no shopping.
Safe home management behaviors were categorized as organizing rooms and smoking in bed.
The level of social activity evaluation included attending culture lessons or pursuing a hobby and interacting with neighborhoods. The level of neighborly ties as social capital were evaluated using a questionnaire that asked whether subjects shared any gifts; had frequent conversations; usually exchanged greetings; and rarely interacted with their neighbors.
Family composition was characterized as living alone, living with spouses, living with family, and spending alone in the daytime.
Self-rated masticatory ability was measured on a 5-point scale from being able to eat whatever subjects wanted to eat, able to eat most foods except some hard ones, limited foods because of inadequate chewing, unable to eat few foods because of insufficient chewing, and a fluid diet. In this survey, a fluid diet was defined as a swallowable food without chewing.
This study was approved by the Ethical Committee of Kumamoto Health Science University, Kumamoto, Japan (No. 23-12 for epidemiology), and informed content was obtained from all participants.
Statistical Analysis
All data were reported as the mean ± standard deviation. Categorical variables were compared using the chi-square test. A logistic regression analysis was used to determine which categorical factors were independent predictors of having self-perceived health without requiring long-term care services. A multivariate logistic regression analysis was used to calculate the odds ratios (ORs) and 95% confidence intervals (CIs) after controlling simultaneously for potential confounders. Comparison between multiple groups was performed by using a multivariate ANOVA adjusted with covariates. All statistical analyses were performed using IBM SPSS Statics for Japan version 19.0 for Windows (IBM, Japan). A value of p < .05 was considered to be statistically significant.
Results
The initial evaluation of the participants (1,377 individuals) in the present study showed that 578 subjects could eat whatever they wanted to eat, 686 could eat most foods except a few that were difficult, 83 could eat a limited number of foods because of insufficient chewing ability, 6 could eat few foods because most were too difficult to chew, and 3 were on a fluid diet. Participants who answered “unknown” (21 persons) were excluded from the current statistical analysis. The association between the subjects’ self-rated masticatory ability with having good self-perceived health without requiring long-term care as a self-reliant life among the older adults is shown in Table 1. The population that could chew whatever they wanted to eat included the highest proportion (68.6%) of those having good self-rated health without requiring long-term care (p < .001, χ2 test), and only 6.2% of those with poor self-rated health and requiring long-term care insurance were found in this population. In contrast, the population that could eat a limited number of foods because of insufficient chewing ability accounted for 56.6% of those with poor self-rated health and requiring long-term care.
Association of Self-Rated Masticatory Ability With Self-Reliant Life in Older Adults.
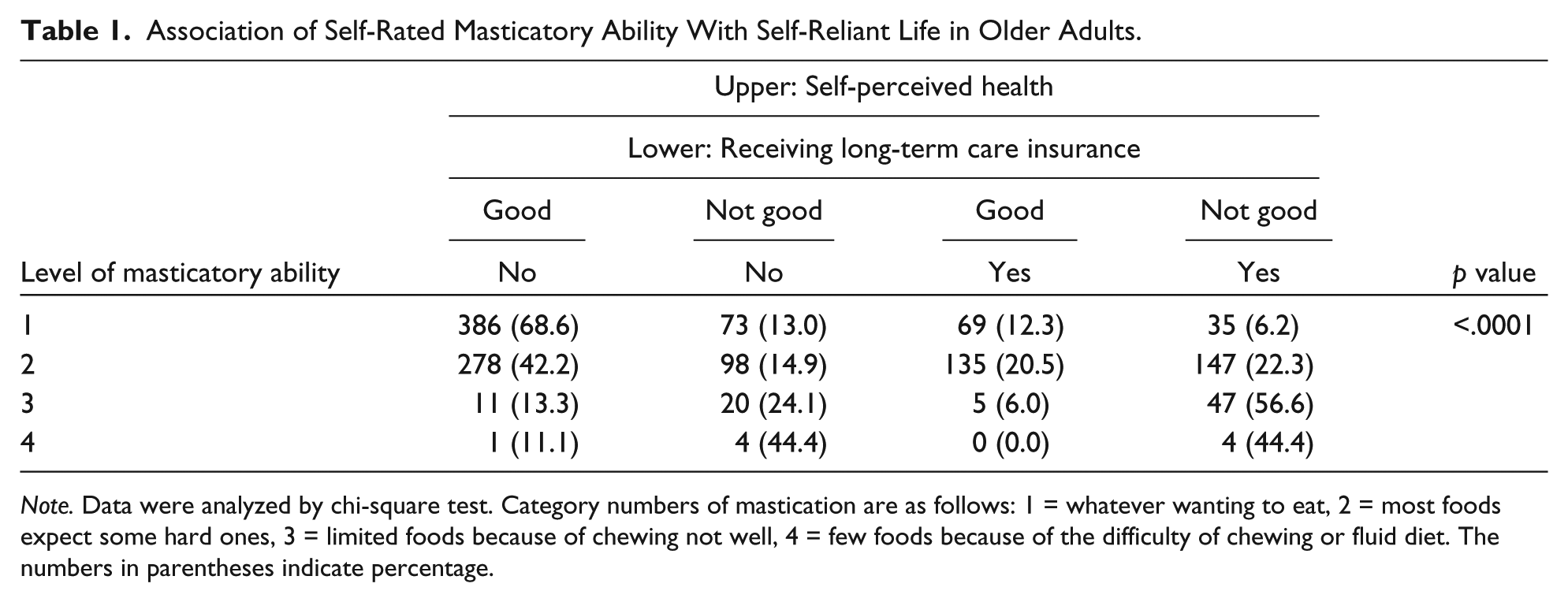
Note. Data were analyzed by chi-square test. Category numbers of mastication are as follows: 1 = whatever wanting to eat, 2 = most foods expect some hard ones, 3 = limited foods because of chewing not well, 4 = few foods because of the difficulty of chewing or fluid diet. The numbers in parentheses indicate percentage.
The association between self-rated masticatory ability with other characteristics of the participants is shown in Table 2. The group with adequate self-rated masticatory ability included a younger population (65-74, 53.2%) than the other groups (75-84, 43.0%; above 85, 32.7%). The gender of the participants was not associated with masticatory ability. The group having a BMI < 18.5 included a significantly lower proportion of those with good mastication. The characteristics associated with mastication were walking for 15 min; anxiety about falling; going out once or more per week; becoming forgetful; using the telephone availing electronic appliance; daily shopping; taking the trash out; managing money; having a hobby; interacting with neighbors; and sharing with neighbors. In addition, having good self-rated health and not requiring long-term care with good subjective health was also significantly associated with the subjects’ self-rated masticatory ability (p < .001, χ2 test).
Association Between Self-Rated Masticatory Ability With Demographic, Nutritional, Status, iADL Items, and Self-Reliant Life in Elderly.
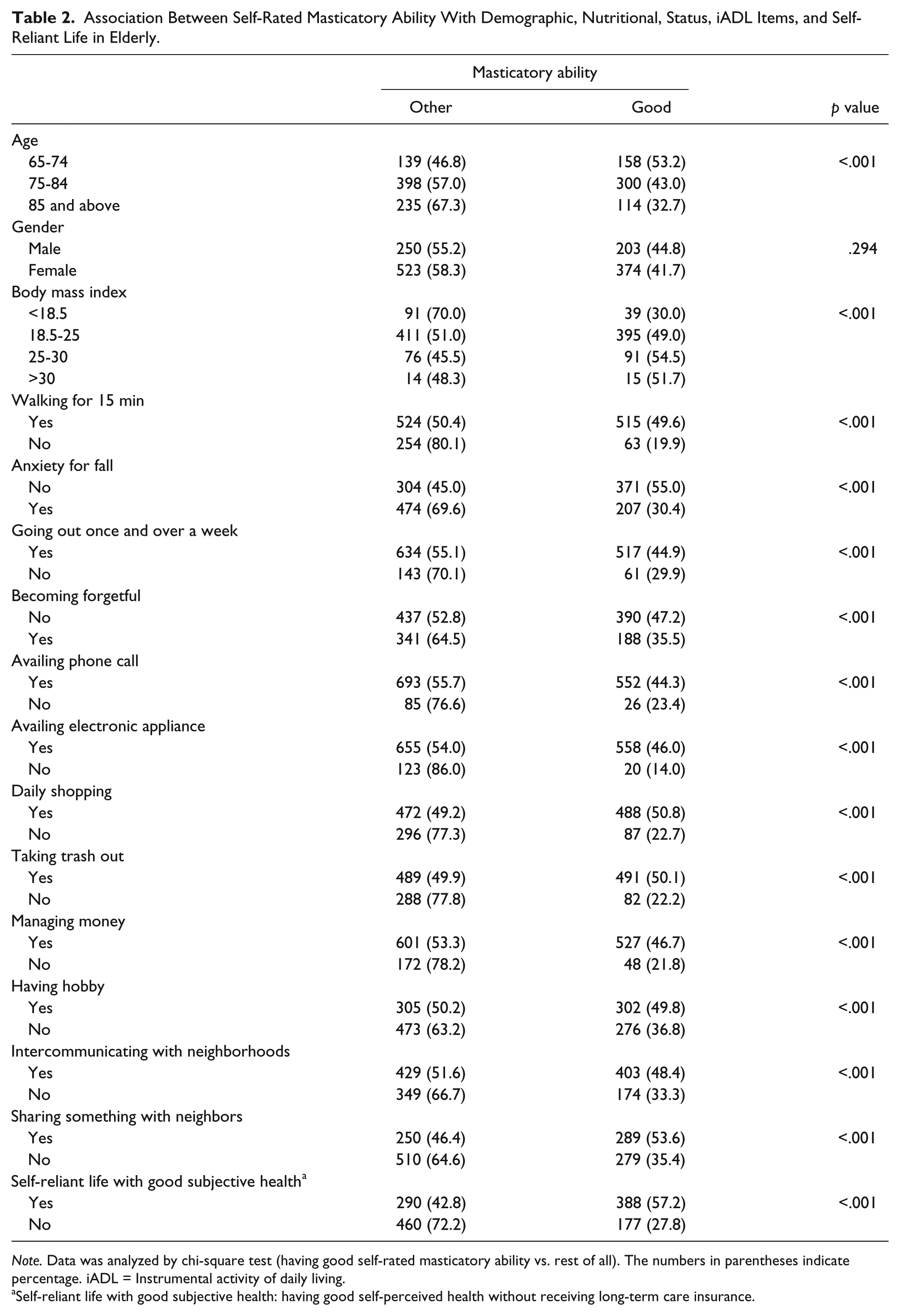
Note. Data was analyzed by chi-square test (having good self-rated masticatory ability vs. rest of all). The numbers in parentheses indicate percentage. iADL = Instrumental activity of daily living.
Self-reliant life with good subjective health: having good self-perceived health without receiving long-term care insurance.
The ORs and 95% CIs for having good self-rated health without receiving long-term care insurance were calculated using a logistic regression analysis adjusted for multiple confounding factors, such as demographics, iADL, social capital, cognitive function, and self-rated masticatory ability (Table 3). An unadjusted univariate analysis revealed that better mastication, younger age, better iADL (walking for 15 min, going out once and over a week, using the telephone, using home electronic appliances, going to shopping daily, taking the trash out, managing money, and ventilating rooms), good social capital (having a hobby, interaction with neighbors), and better cognitive function (not forgetful) were associated with good self-rated health without receiving long-term care. The crude OR for mastication was 3.47 (95% CI = [2.76, 4.38]). Model 1 adjusted for age and gender attenuated the OR for mastication but remained statistically significant (OR = 3.26, 95% CI = [2.58, 4.13]). Model 2, adjusted for iADL, social capital, and cognitive function, and the OR for mastication, was still statistically significant (OR = 2.16, 95% CI = [1.64, 2.83]).
Association of Self-Reliant Later Life With Self-Rated Masticatory Ability Determined by Multilevel Logistic Regression.
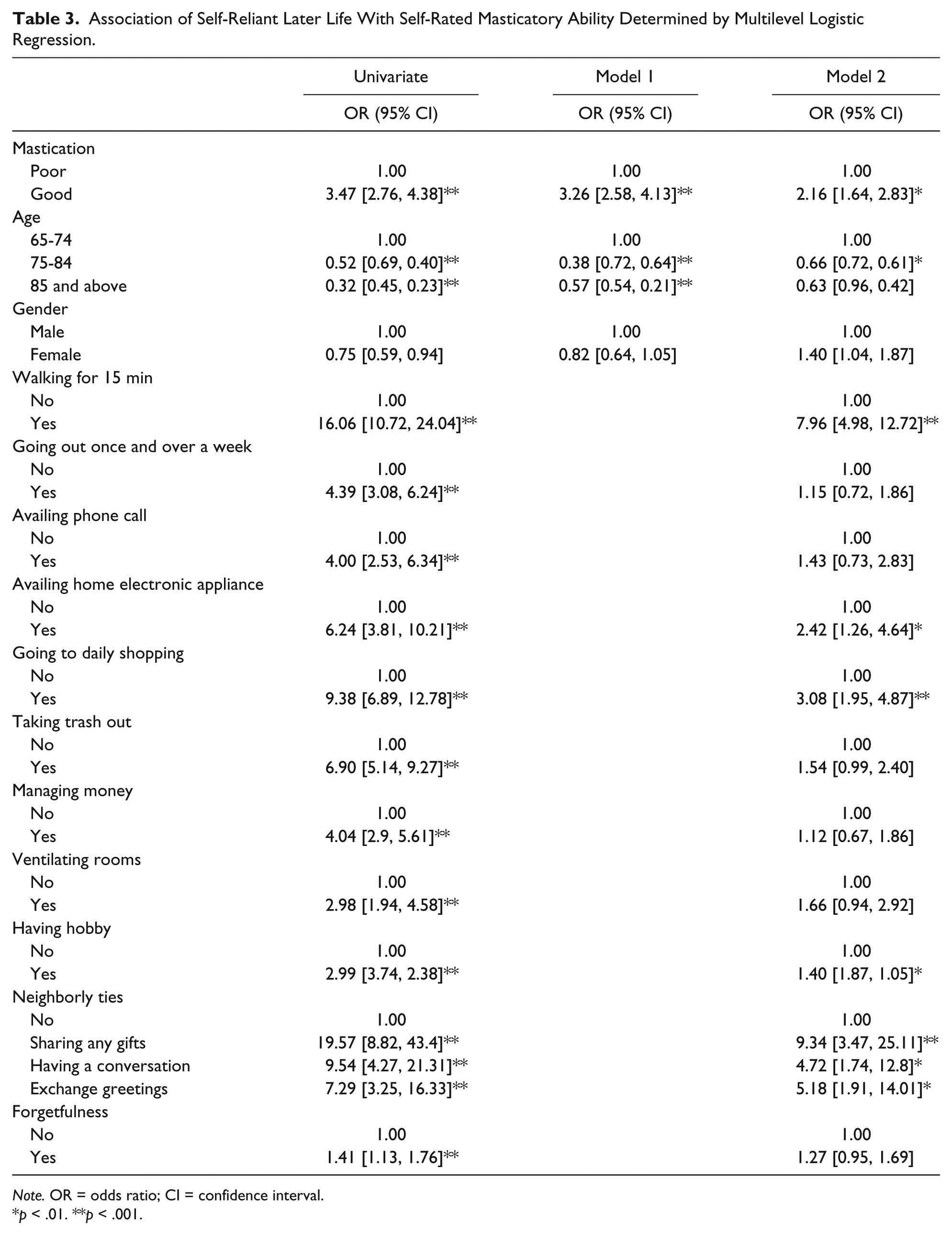
Note. OR = odds ratio; CI = confidence interval.
p < .01. **p < .001.
The participants were divided into four groups based on their self-rated masticatory ability and self-reliant life, and the number of iADL items (eight items maximum) in each group were analyzed (Figure 1). A multiple ANOVA adjusted for gender and age revealed that there were significantly more iADL items in individuals having good mastication (7.64 ± 0.84) than those without good mastication (7.32 ± 1.28) even among those with self-rated good health who were not receiving long-term care. Similarly, there were significantly more iADL items in the individuals having good mastication (6.55 ± 1.71) than in those who did not (5.44 ± 2.19), even in the group that did not have good self-rated health and were not receiving long-term care.
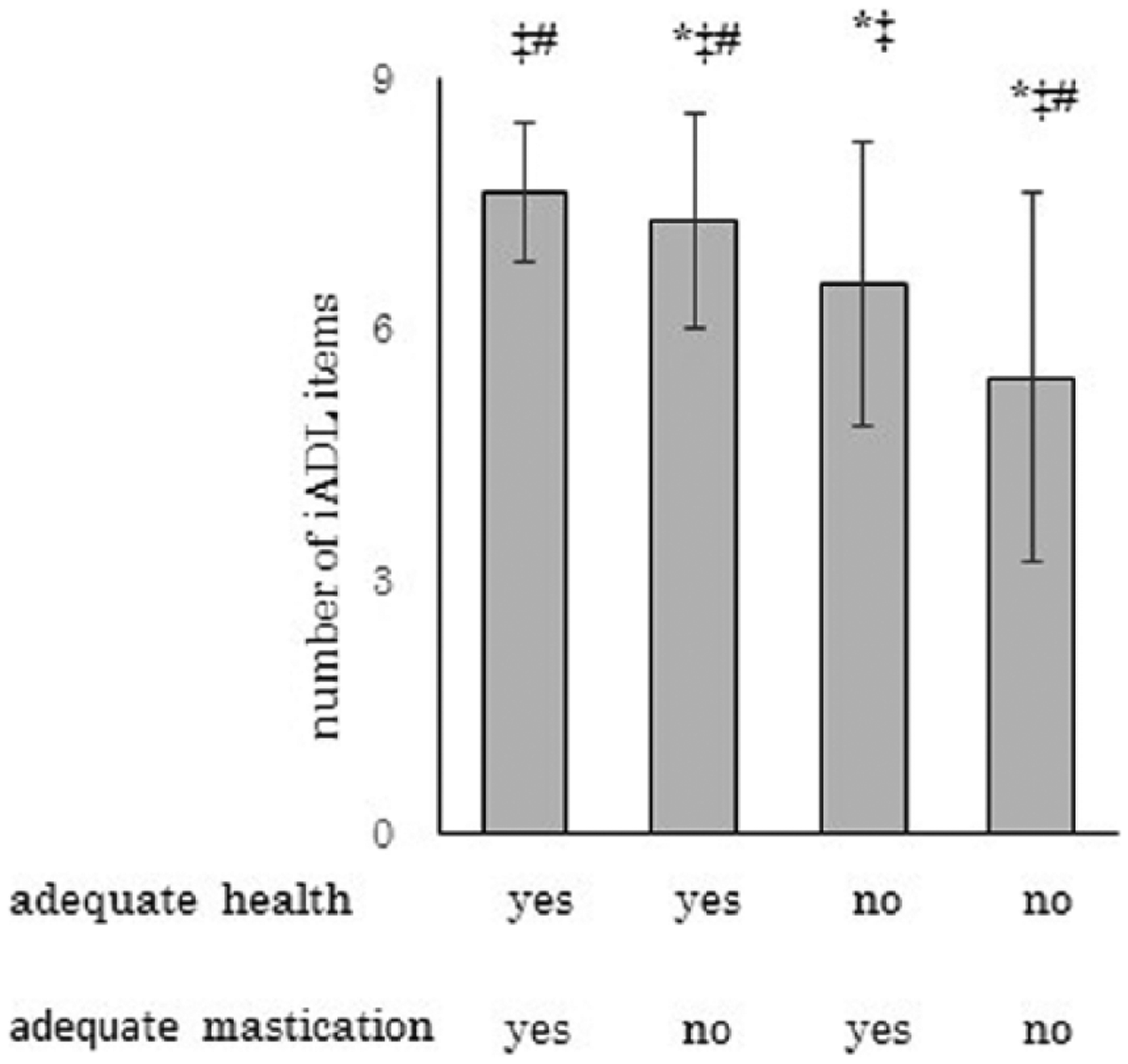
Comparison of number of iADL items for the four groups by self-perceived masticatory ability and health.
Discussion
The current study found that self-rated masticatory ability was significantly associated with the self-perceived good health in those not receiving long-term care insurance in community-dwelling age of 65 and above. The self-perceived good health in subjects who were not receiving long-term care insurance defined those with a self-reliant later life. The present study is the first report on the relationship between a self-reliant later life with positive self-perceived health and self-rated masticatory ability. The significant association between the subjects’ self-rated masticatory ability and their self-perceived good health without receiving long-term care insurance indicated that satisfactory masticatory ability could be an independent predictor of a self-reliant later life.
Rising a rate of long-term institutionalization of older adults damages both the sustainability of social security and the aged own QoL. Health, Labour, and Welfare Ministry in Japan estimated a reduction in health care cost would be 8.9 billion dollar per year in 2020, if increase in active life expectancy would exceed increase in total life expectancy. To maintain their active life and to live in their familiar environment until the end of the life without institutionalization or hospitalization, it is critical to expand active life expectancy. In addition, multiple lines of evidences demonstrated that life expectancy crucially related with the self-perceived health (Kaplan & Camacho, 1983; LaRue, Bank, Jarvik, & Hetland, 1979; Rakowski, Mor, & Hiris, 1994). Taken together, we defined the aged self-reliant status as self-perceived adequate health without long-term care-required certification.
The current findings are consistent with those of previous studies reporting the relationship between patients’ QoL and their masticatory ability. A previous study found that poor chewing ability based on the number of chewable foods was significantly associated with poor QoL status in 80-year-old subjects (Takata et al., 2006). Miura et al. (2000) reported that satisfactory chewing status is correlated with QoL evaluated by the total score of the Philadelphia Geriatric Center (PCG) morale. A report on older Brazilians showed that those satisfied with their ability to chew food was closely correlated with the score of each domain (physical, psychological, environment, and social relations) on the World Health Organization Quality of Life Questionnaire-Brief Version (Hugo, Hilgert, de Sousa Mda, & Cury, 2009). Another recent study reported a relationship between certification of long-term care insurance and self-rated chewing ability. The result of the Kaplan–Meier analysis for individuals aged 65 to 79 years clearly demonstrated that the proportion of individuals not certified for long-term care insurance significantly declines in those with self-rated fair or poor masticatory ability compared with those having good mastication (Moriya, Notani, Murata, Inoue, & Miura, 2014). A Cox proportional hazard analysis also shows that the certification for long-term care insurance was 1.87-fold (CI = [1.07, 3.27]) higher in the individuals with fair or poor masticatory ability in comparison with those with adequate ability (Moriya et al., 2014). A 6-year follow-up study on rural community–dwelling older adults in Japan by Shinkai et al. (2003) demonstrated that depression of basic activity of daily living (ADL) and iADL were 1.88-fold (CI = [1.26, 2.82]) and 2.22-fold (CI = [1.50, 3.27]), respectively, higher in individuals with poor chewing ability in comparison with those with better ability. Taken together, maintaining the chewing ability in later life would advantage self-reliant life through keeping well both mentally and physically. These evidences suggest that masticatory ability should be the concern in gerontological research.
To ensure sustainability of social security system, it is important to close the gap between life expectancy and active life expectancy. Moriya et al. (2011) conducted a study of 882 individuals aged 65 and above, and a multivariate logistic regression demonstrated that severely impaired masticatory ability is significantly related to higher hospitalization costs. Kimura et al. (2013) assessed masticatory efficiency using color-changing chewing gum in 269 community-dwelling Japanese older adults above the age of 75, and concluded that lower masticatory efficiency is significantly associated with lower ADL, lower cognitive function, and depression. The result of panel interview surveys for age of 65 and above in Japan indicated that active life expectancy of individuals who could chew relatively hard foods was 2 to 3 years longer than people who could chew only relatively soft foods in daily diet (Nasu & Saito, 2006). These evidences, including our findings, strongly suggested that maintenance of adequate chewing ability in older adults is closely related to expansion of the active life expectancy, leading to the sustainability of social security system.
The participants of the current study were armed with a regional welfare commission volunteer or community comprehensive care center. Therefore, the proportion of participants receiving long-term care insurance in the present study was 33.8%, higher than the average proportion in Japan (17.9% in aged 65 and above). The proportion of participants whose health was perceived to be well was 67.2%, slightly lower than a population based on a recent survey on health consciousness by the Ministry of Health, Labour, and Welfare in Japan (77.9% in aged 65 years and above in 2014). This study conducted a structured-questionnaire interview-based investigation in conjunction with the regional commission volunteers or public nurses on the staffs of community comprehensive care center, closely interacting with community-dwelling older adults through regular home visits. Therefore, the volunteers or the public nurses commissioned this investigation had built a good rapport with the participants in the study, allowing them to collect true-to-life data.
The self-rated masticatory ability was closely correlated with neighborhood social capital, such as interacting with neighbors and sharing something with neighbors, as shown in Table 2. Results from a prospective cohort study based on the Aichi Gerontological Evaluation Study indicated that both community and individual levels of horizontal social capital (such as volunteer group, sports clubs, and hobby clubs) are significantly associated with retaining 20 or more teeth in individuals aged 65 and above (Aida et al., 2009). Aida et al. conducted another study based on a survey in Ohsaki city and demonstrated that neighborhood social capital, accomplished by four kinds of networks (civic, sports and hobby, volunteer, and friendship networks), is closely correlated with dentate status in older adults (Aida et al., 2011). In contrast, social capital is not correlated with the use of oral prosthesis, such as a denture or dental bridge (Yamamoto et al., 2014). There were few questionnaire items to measure social capital in the current study; thus, conclusions based on the relationship between social capital and masticatory ability were limited. Further study on the association between social capital and masticatory ability is needed.
Study Limitations
Several limitations of this study should be considered. First, self-rated masticatory ability has not correlated with any objective masticatory function such as bite force. This may weaken our argument, although there are multiple evidences on good correlation between subjective and objective chewing ability. Second, participants of this study were selected by regional welfare commission volunteers and community comprehensive care center staffs, suggesting to have bias. Further study is needed to assess the community-dwelling elderly people who have no relation with regional welfare commission volunteers or community comprehensive care center staffs. Third, we did not have any socioeconomic status, such as income and length of educations, of participants. Although society in Kumamoto area narrowed the gap between the rich and the poor in older adults, subjective masticatory ability may be related with socioeconomic status in Japanese older adults. Fourth, there is a geographic limitation, as the participants were all from one city. Fifth, only a self-reported information was examined in this study. Some clinical data, such as serum albumin level for nutrition condition or blood pressure for general condition, might strengthen our findings. Sixth, to ensure this mechanism, effect of clinical intervention on masticatory ability, such as denture wearing, dental implant, and muscle training, would be a considerable research task.
In conclusion, there was a significant association between self-rated masticatory ability and having self-perceived good health in older adults who were not receiving long-term care insurance, suggesting that a satisfactory level of chewing could be an independent predictor for self-reliant living in the community-dwelling older population. The result of our study demonstrated that asking the self-rated masticatory ability could be an easier and a useful tool for non-healthcare professionals to assess the health status of regional older adults.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.