
Abstract
Introduction
Self-rated health (SRH) denotes the perceived health of an individual and is a widely used concept in health research. In the literature, it is described by different terms interchangeably, such as perceived health and self-assessed health. Predictive factors of and associations with SRH have been investigated in numerous studies. Extensive research among various countries worldwide has shown that SRH is associated with mortality and morbidity (Idler & Benyamini, 1997; Jylhä, 2009; Mora, DiBonaventura, Idler, Leventhal, & Leventhal, 2008). Various aspects of objective health are important predictors of subjective health (Pinquart, 2001), for example, physical health, consisting of perceived symptoms and the number of medical conditions, is strongly related to SRH and is seen as a predictor of SRH (Mora et al., 2008). Poorer physical health is related to lower SRH (Eriksson, Unden, & Elofsson, 2001; French, Sargent-Cox, & Luszcz, 2012; Leinonena, Heikkinena, & Jylhä, 2001; Verropoulou, 2012). Nevertheless, aging people are often able to adapt to a decline in physical health, and therefore not always result in a decline in SRH (Leinonena et al., 2001). Older people redefine subjective good health; it is merely based on having fewer health problems than most age peers and a lack of severe complaints (Arnadottir, Gunnarsdottir, Stenlund, & Lundin-Olsson, 2011; Eriksson et al., 2001; French et al., 2012; Layes, Asada, & Kephart, 2011; Pinquart, 2001). Mental health, composed of subjective cognitive impairment, psychological well-being, and depression, is associated with SRH; a stronger association is found in people age 75 and older (Pinquart, 2001). Very old people seem to ascribe more value to their mental than to their physical health (French et al., 2012), and the lower someone evaluates perceived mental health, the more likely it is that s(he) will rate health more negatively (Jylhä, 2009; French et al., 2012). However, individuals do not always acknowledge mental disabilities as a part of their health.
Functional limitations, such as subjective individual limitations on daily activities, increase with age, and increased functional limitations are related to lower SRH. However, self-rating of health is dependent on adaptation to disabling conditions over time, and SRH can therefore increase over time (Hoeymans, Feskens, Kromhout, & Van Den Bos, 1997; Leinonena et al., 2001; Verropoulou, 2012).
Research on the influence of socioeconomic status (SES), in terms of income and education, on SRH, provides conflicting results (Eriksson et al., 2001; French et al., 2012; Jylhä, 2009; Olsen et al., 2007; Olsen & Dahl, 2007; Verropoulou, 2012). SRH is also based on culture and may be affected by the country of residence. In Europe, there are major variations in rating and perspectives of health among countries (Verropoulou, 2012). A more favorable or more negative rating of health is part of the character of individuals and the environment in which they live and depends on the aspects that an individual ascribes to her health (Brissette, Leventhal, & Leventhal, 2003; Jylhä, 2009). Environmental aspects, the physical and psychosocial setting in which individuals live, influence SRH (Arnadottir et al., 2011; Molarius et al., 2006). Studies show that social support, access to health care facilities (Lehning, Smith, & Dunkle, 2012), overall satisfaction with social relations (e.g., relatives and friends; Blazer, 2008; Melchior, Berkman, Niedhammer, Chea, & Goldberg, 2003) and a better quantitative and qualitative social network (Olsen et al., 2007) are associated with a higher SRH.
According to the Organisation for Economic Co-Operation and Development (OECD; 2012), life satisfaction consists of a personal evaluation of one’s health, education, income, personal fulfillment, and social conditions. Previous studies show that poorer SRH can be related to dissatisfaction with one’s life (Blazer, 2008). However, SRH was not statistically significantly correlated with life satisfaction among elderly Latvian women in a study involving samples from Latvia and Sweden (Horstman, Haak, Tomsone, Iwarsson, & Gräsbeck, 2012).
In 1998, it was stated that the average level of self-perceived health was generally worse in former Communist countries than in Western Europe among both men and women (Carlsson, 1998). There is still inequality in health between regions of Eastern and Western Europe, for example, countries such as Latvia and Sweden, the substantial differences are reflected in life expectancy and health indicators (World Health Organization [WHO], 2014). Latvia has a lower life expectancy at birth than most EU (European Union) countries (WHO, 2012). Latvian men have a life expectancy (69 years), below the worldwide average at birth; women are expected to live 79 years, and the average life expectancy for both sexes is 74 (WHO Regional Office for Europe, 2014a). In Sweden, life expectancy at birth is 80 years for men and 84 years for women, and the average for both sexes is 82 (WHO Regional Office for Europe, 2014c). In both countries, the population is aging: almost 19% of the population was 65 or older in Latvia in 2012, with an estimated increase to 23% in 2030 (World Bank, 2011; WHO Regional Office for Europe, 2010). In Sweden, 18.6% of the population was 65 or older in 2011 with an estimated increase to 30% by 2030 (Swedish Institute, 2012; WHO, 2012b).
Most Eastern European countries joined the EU in the process of enlargement during later years. However, there are still major differences between countries within the EU regarding living conditions, health, and SES. The aim of Health 2020, the policy framework and strategy of the WHO Regional Committee for Europe, is to “significantly improve the health and well-being of populations, reduce health inequalities, strengthen public health, and ensure people-centered health systems are universal, equitable, sustainable, and of high quality.” Thus, studying SRH in various European countries is highly relevant, given that this factor has the potential to inform such policies and strategies.
Sweden has one of the highest SRHs in Europe, whereas Latvia was ranked as one of the lowest in 2009 (European Commission, 2010). Compared with Sweden, there is limited knowledge in Latvia about perceived health among very old people, as well as factors contributing to it. The aim of this study was to explore variables associated with SRH and identify factors influencing SRH among very old people in Latvia and Sweden.
Method
Description of the Sample
This study was based on Latvian and Swedish data from the cross-national European project “Enabling Autonomy, Participation, and Well-Being in Old Age: The Home Environment as a Determinant for Healthy Ageing” (ENABLE-AGE, 2002-2004; Iwarsson et al., 2007) involving very old, single-living participants from five European countries, three Western (Sweden, United Kingdom, and Germany) and two Eastern European (Latvia and Hungary) countries. The main objective of the ENABLE-AGE project was to examine the home environment and its importance for major components of healthy aging. For each country, the target sample was 400 very old, single-living persons in urban areas, including both genders (stratified to include approximately 25% men). Furthermore, sampling was based on notion of “third” and “fourth” age (Iwarsson et al., 2004b).
The project design was explicitly explorative and did not aim for national representatives. In Sweden, the national sample was drawn randomly from the national population register of three municipalities in the southern part of the country (Helsingborg, Lund, and Halmstad). It was not possible to use official registers in Latvia. Latvian participants were recruited at social service centers and through older people’s voluntary organizations in Riga and Jūrmala, striving to apply principles of randomization as far as possible. The Latvian ENABLE-AGE baseline sample consisted of 75 to 84 year-old participants (n = 303), whereas the participants in the Swedish baseline sample were 80 to 89 years old (n = 397). In the Latvian sample, two participants had a missing value on SRH. Therefore, these two participants were excluded from the present study, leaving n = 301.
Procedures
During two home visits (lasting max. 2 hr), one out of the group of four to six trained interviewers (occupational therapists) collected interview and observation data by means of the ENABLE-AGE Survey Study Questionnaire in each country. During the ENABLE-AGE project, there were regularly workshops and meetings arranged to tackle any problems. For the present study, a subset of the comprehensive database was utilized. Project followed ethical principles for research according to the Helsinki Declaration. In each country involved, the project was subjected to ethical review, followed by formal consent according to national regulations.
Instruments
Based on literature reviewed, a framework was developed to select the data for this study that included demographics, physical and mental health aspects, functioning, environmental aspects, and life satisfaction (Figure 1). Only the instruments used for collecting these data are described below, further details on the instrumentation have been published elsewhere (Oswald, Wahl, & Schilling, 2007).
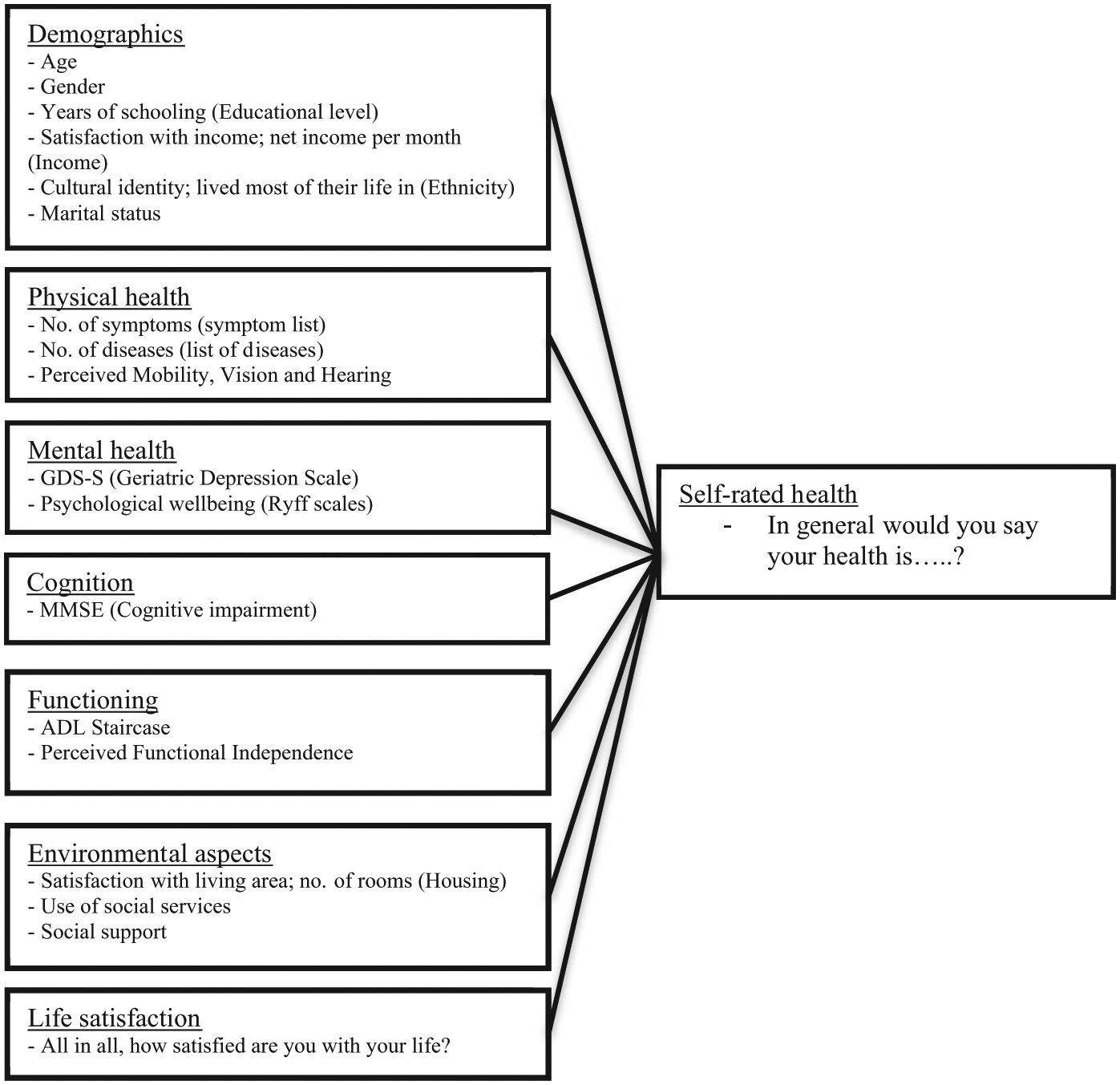
Framework for the exploration of SRH.
SRH
A single question was retrieved from the SF-36® (SF-36: 36-Item Short Form Health Survey) (Ware & Sherbourne, 1992): “In general would you say your health is?” Participants rated their health on a 5-point Likert-type scale with the response categories of excellent (1), very good (2), good (3), fair (4), and poor (5).
Demographic data included age (continuous variable), gender, educational level (years of schooling), and self-reported net income per month (continuous variable). Marital status was assessed on five categories (married; partner living somewhere else, for example, in nursing home; single living alone but having a close relationship with partner; divorced; widowed; or never married), and later on dichotomized into widowed and other. Satisfaction with income was assessed on a scale ranging from very dissatisfied (0) to very satisfied (10). Cultural identity was captured with two questions; “How do you define your cultural identity?” and “Where have you lived most of your life?”—subsequently dichotomized into Latvian or Swedish/other and Latvia or Sweden/other, respectively.
Physical health
The presence of disease was determined by using a list of 10 diseases retrieved from the International Classification of Diseases, version 10 (ICD-10); a score denoting the total number of self-reported diseases was used. Symptoms were self-reported by using the 30-item list from the Gothenburg Quality of Life instrument (Tibblin, Bengtsson, Furunes, & Lapidus, 1990); the total number of symptoms was used. Single questions retrieved from the SF-36® (Ware & Sherbourne, 1992) were used to rate perceived mobility (“How would you rate your physical mobility at the moment?”), vision (“How would you rate your vision at the moment?”), and hearing (“How would you rate your physical mobility at the moment?”) applying a 5-point Likert-type scale with the response categories of excellent (1), very good (2), good (3), fair (4), and poor (5).
Mental health
The Psychological Well-Being Questionnaire (Ryff, 1989) was used to assess purpose in life, autonomy, and environmental mastery. The variable generated by each Ryff scale was the mean of nine statements; a higher mean score represented greater psychological well-being. To examine the presence of depression symptoms, the short version of the Geriatric Depression Scale (GDS-S) was used; participants were asked to indicate their level of agreement with 15 statements. A total score was calculated, and the interpretation of the total scores was based on the instrument guidelines; total score < 5 indicated no depression, 5 to 9 indicated possible depression, and a score > 9 indicated depression (Greenberg, 2012; Yesavage, Brink, & Rose, 1982).
Cognition
Four tasks from the Mini Mental State Examination (Folstein, Folstein, & McHugh, 1975) were used to indicate cognitive impairment (Eccles, Clarke, Livingstone, Freemantle, & Mason, 1998); the proportion of correctly performed applicable tasks was used.
Functioning
Using the ADL Staircase (Hulter-Åsberg & Sonn, 1989; Sonn & Hulter-Åsberg, 1991), independence/dependence in nine Activities of Daily Living was assessed by a combination of interviews and observation Activities of Daily Living (ADL). On each item, the participant was rated as either dependent (0) or independent (1), and an individual score was summed up to a total score with 9 indicating full independence. In addition, the participants rated their perceived functional independence using a single item from the Neuropsychological Aging Inventory, ranging from 0 (completely dependent) to 10 (completely independent) (Oswald, 2005).
Life satisfaction was assessed by a single question “All in all, how satisfied are you with your life?”—rated on a scale ranging from 0 “very dissatisfied” to 10 “very satisfied.”
Environmental aspects
Participants rated satisfaction with their present living area on a scale ranging from very dissatisfied (0) to very satisfied (10). Because most participants were very satisfied, the responses were dichotomized into very satisfied (scores 9-10)/less satisfied (scores 0-8). Housing standard was represented by the number of rooms in the participant’s present dwelling. Consumption of various health care or social services during the last 12 months was captured with nine items (total score 0-9). In addition, existing social support was dichotomously (yes/no) assessed.
Data Analysis
The two samples were described with frequencies, means, standard deviations, medians, and quartiles, when appropriate. Differences between the Latvian and Swedish samples were tested by means of the Mann–Whitney’s U test or the t test for two independent samples for continuous variables and with the χ2 test for categorical variables. Moreover, Spearman’s correlations between perceived health and all variables included in theoretical framework (see Figure 1) were calculated.
Ordinal regression analysis was used to construct two “comparable models” to investigate the differences between the Latvian and Swedish samples. Prior to these comparable models, two country-specific models were constructed to determine which variables were significantly related to SRH in the two samples and therefore determine the factors that should be included in the Swedish and Latvian “comparable models.” If a variable appeared to be significant at the 0.1 level in at least one of the two country-specific models, the variable was included in both “comparable models” for each country separately to support the interpretation and understanding of the differences between the Latvian and Swedish samples. The probit link function was chosen based on the distribution of SRH. The relation of each explanatory factor with SRH was first investigated separately, using a p value < .25 as the criterion for inclusion in further analyses. A backward deletion procedure was performed to construct the models until the model consisting of variables with p values < .1 was achieved. Because of the coding, a lower SRH score meant better SRH. Consequently, negative regression coefficients indicated that with an increase in the value of that variable, better SRH was more likely, and a positive coefficient indicated that with an increase in the value of that variable, worse SRH was more likely. p values < .1 were set as the significance level. SPSS 19.0 was used for all calculations.
Results
The participants in the Latvian sample scored much worse SRHs than those of the Swedish sample: 86.8% of the Latvian sample rated their SRH as “fair” or “poor,” whereas most of the Swedish sample (72.0%) rated their health as at least “good” (see Figure 2). Comparing SRH in the Latvian and Swedish samples, a significant difference was found (p value < .0005).

SRH at baseline in the Swedish (n = 397) and Latvian (n = 301) samples.
Comparing the two samples, significant differences (p values < .0005) were found regarding almost all characteristics. That is, participants in the Swedish sample were older (because they were sampled so), the proportion of men was higher, and net income and satisfaction with income were higher (Table 1). Participants in the Latvian sample had more years of schooling, and the proportion of participants with a cultural background other than Latvian was higher. Regarding aspects of health and functioning, there were more symptoms, diseases, and higher depression scores in the Latvian sample. The participants in the Swedish sample rated their perceived mobility and visual ability slightly higher, but there were more ADL-dependent participants than in the Latvian sample.
Characteristics of Latvian (n = 301) and Swedish (n = 397) Samples.

Note. SD = standard deviation; IQR = interquartile range; GDS-S = Geriatric Depression Scale; MMSE = mini mental state examniation; ADL = activities of daily living.
Ranging from 0 (very dissatisfied) to 10 (very satisfied).
1 = excellent; 2 = very good; 3 = good; 4 = fair; 5 = poor.
Lower than 5: no indication of possible depression, 5-9: indicates possible depression, higher than 9: indication of depression.
Ranging from 0 to 5. Score of 5 means high/well-developed on psychological well-being scale.
Ranging from 0 (completely dependent) to 9 (completely independent) in Instrumental and Personal ADL.
Ranging from 0 (completely dependent) to 10 (completely independent).
As to significant correlations (p values < .1) between SRH and single variables, the overall pattern was similar for both national samples, showing differences regarding only demographic variables (Table 2). All physical and mental health variables had a moderate association with SRH; for both samples, the strongest association was between perceived mobility and SRH (rs = .54 in Latvia, rs = .60 in Sweden).
Associations With SRH in the Latvian (n = 301) and Swedish Sample (n = 397).

Note. Bold numbers show variables that were significantly associated with SRH based on p value ≤.1. SRH = self-rated health; GDS-S = Geriatric Depression Scale.
The two comparable models, for the Latvian and Swedish samples separately containing the same explanatory variables, are presented in Table 3. The Nagelkerke statistic showed that the explained variance for the final Latvian model was 0.542, and the corresponding statistic for the Swedish model was 0.548. The direction of the relations between SRH and the variables between the country-specific and comparable models did not differ. In both national samples and models, participants with worse perceived physical mobility and more symptoms were significantly more likely to have worse SRH.
Associations With SRH in the Latvian (n = 301) and Swedish Sample (n = 397).

Note. Bold numbers show variables that were significantly associated with SRH based on p value ≤.1. A positive coefficient indicates that with an increase in the value of a variable, worse SRH was more likely. A negative coefficient indicated that with an increase in the value of a variable, better SRH was more likely. SRH = self-rated health.
Men compared with women.
Those who identified their culture as Swedish or Latvian compared with others.
Complete independence was the reference category.
Very satisfied was the reference category, the first line is those who were very dissatisfied compared with very satisfied, second line is those who were moderately satisfied compared with very satisfied with the area they lived in.
In the Latvian sample, men, participants with higher education and a native cultural identity were significantly more likely to have better SRH. Turning to the Swedish sample, participants with worse visual ability and more dissatisfaction with the area they lived in were significantly more likely to have worse SRH. Swedish participants who were more satisfied with their life were significantly more likely to have better SRH. A higher age was in both samples not significantly associated with SRH.
The major difference between the Latvian and Swedish samples in the associations of the variables with SRH and their direction were seen for gender. That is, Latvian men were significantly more likely to have better SRH than women, whereas in Sweden, gender was not significantly associated with SRH.
Discussion
In this study, explanatory factors of SRH of very old people were examined and compared in a sample from Latvia, an Eastern European country with a low life expectancy, and a sample from Sweden, a Western European country with a high life expectancy. It was expected, according to the literature, that demographic factors, physical and mental health, functional limitations, environment, and life satisfaction were associated with SRH. Although all these factors were assessed and taken into account in the analysis, not all factors appeared to be significant in relation to SRH in the two national samples studied.
More negative rating of SRH was associated with poor perceived mobility and a higher number of symptoms among both Latvian and Swedish participants, which is in line with previous research (Eriksson et al., 2001; French et al., 2012; Leinonena et al., 2001). It was expected that a higher educational level would probably lead to higher scores on SRH (Olsen et al., 2007; Verropoulou, 2012); this study showed this association only among Latvian participants. According to the literature, men are more likely to score lower on SRH (Eriksson et al., 2001; French et al., 2012; Olsen et al., 2007; Verropoulou, 2012). In this study, Latvian men rated their health significantly better than Latvian women, whereas gender showed no significant association in the Swedish sample. A higher age was in both samples not significantly associated with SRH. Higher satisfaction with life was significantly associated with better SRH in the Swedish but not the Latvian sample. Given the history of Latvia, it is interesting that identification with the culture of the country they lived in was significantly associated with a better SRH among Latvian participants. No such association was found in the Swedish sample.
This study contributes to knowledge about health in very old people in Latvia. Furthermore, we were able to compare various aspects of health among samples of very old people in Latvia and Sweden. The findings showed that there are similarities in the factors that explain SRH, despite the large differences in historical background and economic status of the two countries. In both countries, perceived physical health and number of symptoms were significantly associated with SRH, but differences were seen regarding age, gender, and life satisfaction.
Several limitations of this study need to be emphasized. It should be noted that samples from the ENABLE-AGE Project were not nationally representative, considering the pronounced differences in life expectancy among the participating countries (Iwarsson, Wahl, & Nygren, 2004a), the sampling criteria were developed based on the notion of the “third” and “fourth” age (Baltes & Smith, 1999). It should be noted that sampling strategy differ among countries, for example, in Latvia in 2002, the population register was not available for researchers due to legislation on protection of personal data, and thus Latvian participants were recruited by means of convenient sampling at social service centers. Quite a number of potential participants declined taking part in the strenuous procedure of data collection due to health problems in both countries; 41% of the persons contacted accepted to participate in Sweden and 44% in Latvia. Therefore, it could be stated that those who were included in the study were more likely to have a better health status.
Moreover, it needs to be taken into account that the variables are interrelated; removing one variable from the model will therefore automatically change the model and its significant association with SRH. Although the variables are interrelated, many relevant variables were included to form a clear understanding of SRH and its associated variables. However, several aspects such as behavior, lifestyles, self-efficacy, coping and acceptance of disabilities and health or disease, as well as personal values with respect to SRH, are not taken into account and might have an impact on the findings.
The influence of cultural background and historical events was not taken into account; for example, Latvian participants had experienced many historical events—the first independent Republic of Latvia, World War II, Soviet regime, and changes after regaining independence. Not all changes brought improvement in the life of an individual, and very often participants in interviews mentioned expectations that did not come true. Data collection took place in 2002 to 2003, just before Latvia became a member of the EU, which was a period of ambivalence and uncertainty among Latvian inhabitants. Latvian participants seemed to score more negatively in general than Swedish participants; it might be hypothesized that Latvian participants scored more negatively overall because of their culture and background. No studies were found that compared SRH of Swedish and Latvian inhabitants, but Kaupuzs and Larins (2008) found that older people in Latvia scored lower on self-perceived health and physical activity than older people in Finland. In general, there are still limited and incomplete data on health conditions and determinants in the Latvian population, particularly older adults. To understand why people rated their health as they did, it is important to conduct qualitative research to gain insight into an individual’s value of SRH and each concept in relation to their rating of health. Timing of data collection is crucial; a participant who cannot cope with a new situation or major changes in life at the moment might rate their health differently than at another point in time.
SRH is an important health indicator and is associated with mortality and morbidity; as the EU is aiming for a healthier life and equality in health, it is important to understand factors influencing SRH. This study shows that there are differences among EU member countries in SRH and factors associated with SRH. More research is needed to explore SRH in Latvia in a representative sample of older persons to improve their health even more. It is important to state that variables associated with SRH, according to this study, are modifiable, such as physical mobility, visual ability, and satisfaction with the area people live in, contrary to fixed variables such as age, gender, and cultural identity. This is an important message for policymakers to invest in preventive measures that aim at keeping old people fit and healthy. The target group should be all adults to improve the long-term health of those who live into very old age to facilitate healthy aging and increase SRH in the future.
Conclusion
The results of this explorative study suggest that the number of perceived symptoms and perceived physical mobility are important aspects for SRH among very old people in Sweden and in Latvia. There were more diverse results regarding other factors in terms of opposite significance in relation to SRH when comparing both samples. This study makes it clear that, regardless of the different backgrounds of the participants, it is important to invest in physical health and mobility to promote healthy aging.
Footnotes
Acknowledgements
The authors would like to thank all consortium and national team members for their contribution.
Authors’ Note
This study was based on data from the EC-funded project Enabling Autonomy, Participation, and Well- Being in Old Age: The Home Environment as a Determinant for Healthy Ageing, ENABLE-AGE (QLRT-2001-00334). This study was performed in the context of the Centre of Ageing and Supportive Environments (CASE) at Lund University, funded by the Swedish Research Council for Health, Working Life, and Welfare. This study was supported by the Swedish Research Council, the Swedish Institute, the ScanBalt Bridge Award, and the Ribbingska Foundation in Lund, Sweden.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.