
Abstract
The goal of this research was to investigate the effectiveness of the 10-week, University of Missouri (MU) Extension strength training program Advanced Stay Strong, Stay Healthy (ASSSH). It was hypothesized that the program can improve strength, balance, agility, and flexibility—all physical measures of falling among seniors. Matched pair t tests were used to compare differences in five physical measures of health, body composition, and percent body fat (%BF). Two-way ANOVA was conducted to examine the age effects on changes in physical health from the start and finish of the exercise program. Following programming, participants significantly improved strength, flexibility, and balance, and significantly reduced %BF (p < .05). Our data indicate that ASSSH can improve the physical health of senior citizens and can successfully be translated into community practice by MU Extension professionals.
Introduction
Unexpected falls are a frequent and serious problem facing adults aged 65 and older (Tinetti & Williams, 1997). Injuries resulting from falls represent a significant health burden because approximately 30% of those aged 65 years and older experience at least one fall each year (Campbell, Borrie, & Spears, 1989; Tinetti, Speechley, & Ginter, 1988). Despite randomized control trials and clinical guidelines showing that fall-prevention interventions can be successful, falls and fall-related injuries continue to rise along with associated health care costs (Child et al., 2012). A systematic review estimating the economic burden of falls of older adults living in the community was shown to be US$23.3 billion in the United States alone (Davis et al., 2010).
One of the hallmark features of the aging process and significant risk factors for falls is sarcopenia—the age-related loss of skeletal muscle mass and strength (Rosenberg, 1997)—defined as a value of lean body mass two standard deviations below the average value calculated in healthy, young men and women. The declining muscle mass of sarcopenia occurs at an alarming rate of 4% to 5% per decade (Short, Vittone, Bigelow, Proctor, & Nair, 2004) and results in impaired quality of skeletal muscle, leading to increased muscle weakness (Visser & Schaap, 2011). Such weakness is a strong predictor of falls in the elderly, a significant contributor to decreased quality of life, and associated with an increased morbidity and mortality in this population (Moreland, Richardson, Goldsmith, & Clase, 2004).
Research over several decades has shown compelling evidence supporting the benefits of targeted physical activity programs for older adults to increase muscle strength and reduce fall risk (Chakravarthy, Joyner, & Booth, 2002; Roubenoff & Hughes, 2000). Among those, strength training is considered a promising intervention for reversing the loss of muscle function and the deterioration of muscle structure that is associated with advanced age. This reversal is thought to result in improvements in functional abilities and health status in the elderly by increasing muscle mass, strength, and power (Hurley & Roth, 2000). Strength training exercises also improves bone density and helps minimize osteoporosis.
Despite strong evidence on the benefits of strength training for increasing muscle mass and bone density, follow-up research on falls and falls prevention can often be challenging and problematic. A consistent lack of follow-up makes it difficult to identify the effects the interventions have on actual rates of falling, making it difficult to evaluate this translational research. An example of an evidence-based program that has been implemented by University of Missouri (MU) Extension professionals in community-based settings is Stay Strong Stay Healthy (SSSH), a targeted strength training program geared for older adults with higher fall risk. The SSSH program content was modeled after the StrongWoman program developed at Tufts University (Nelson et al., 1994). Each class of approximately 20 participants consists of group strength training, balance, and flexibility exercises 1 to 2 times a week for 10 weeks. Ball et al. (2013) studied the effects of participation in the SSSH program on fall risk. The results, published in the Journal of Aging and Health, showed that following programming, participants demonstrated statistically significant improvements in strength, balance, coordination, and flexibility.
Following the success of SSSH, the Advanced Stay Strong, Stay Healthy (ASSSH) program was developed in 2009 by a team of MU Extension Specialists who wanted to meet the increasing need for a follow-up program to the 10-week SSSH program. The ASSSH program was designed to challenge participants who have completed the SSSH program in new and different ways, to help avoid staleness and plateaus, and to improve activities of daily living. The neuromuscular system quickly adapts to stressors and loads, and must be challenged for gains in strength, flexibility, and balance to continue. The primary aim of this research was to investigate the effectiveness of the MU Extension program ASSSH.
Method
All exercise training sessions and pre- and post-assessment of strength, flexibility, and balance measures were conducted by trained exercise personnel. The exercise intervention consisted of group strength training, balance, and flexibility exercise 2 times a week for 10 weeks. Sessions began with a 5-min warm-up period, followed by two sets of 10 repetitions of 8 to 10 various strength exercises including (but not limited to) wide leg squat, standing leg curl, lunge, biceps curl, overhead press, wall push-ups, bent forward fly, rear raise, one arm row, chest press and chest fly. Classes finished with a cool-down period including light stretching and balance exercises. Each exercise session lasted approximately 1 hour. Procedures in this research study were conducted in accordance with the University of Missouri Health Sciences Institutional Review Board. A detailed description of the ASSSH program including number and pacing of exercises can be seen in the appendix.
Participants
Participants were recruited via flyers, online newsletters, and word of mouth. Participants were screened for any medical problems that might affect their ability to complete the study using the Physical Activity Readiness Questionnaire (or PAR-Q) and provided physical authorization to participate. Data were analyzed from participants who completed at least 60% of the workout sessions (n = 23). The average age of the sample was 60.5 years (SD = 7.6; range = 50-76); 40.2% (n = 6) were over 60 years of age and 91% (n = 21) were females.
Measures
Body composition was assessed by Dual Absorptiometry X-Ray (DXA; QDR 4500A, Hologic, Inc., Bedford, MA, USA) using fan beam technology. Each participant completed a whole-body DXA scan pre- and post-intervention. Bone mineral density, fat mass, and lean mass were represented in pounds (lbs). Percent body fat (%BF) was calculated by the software and represented as fat mass (g) / total mass (g) × 100.
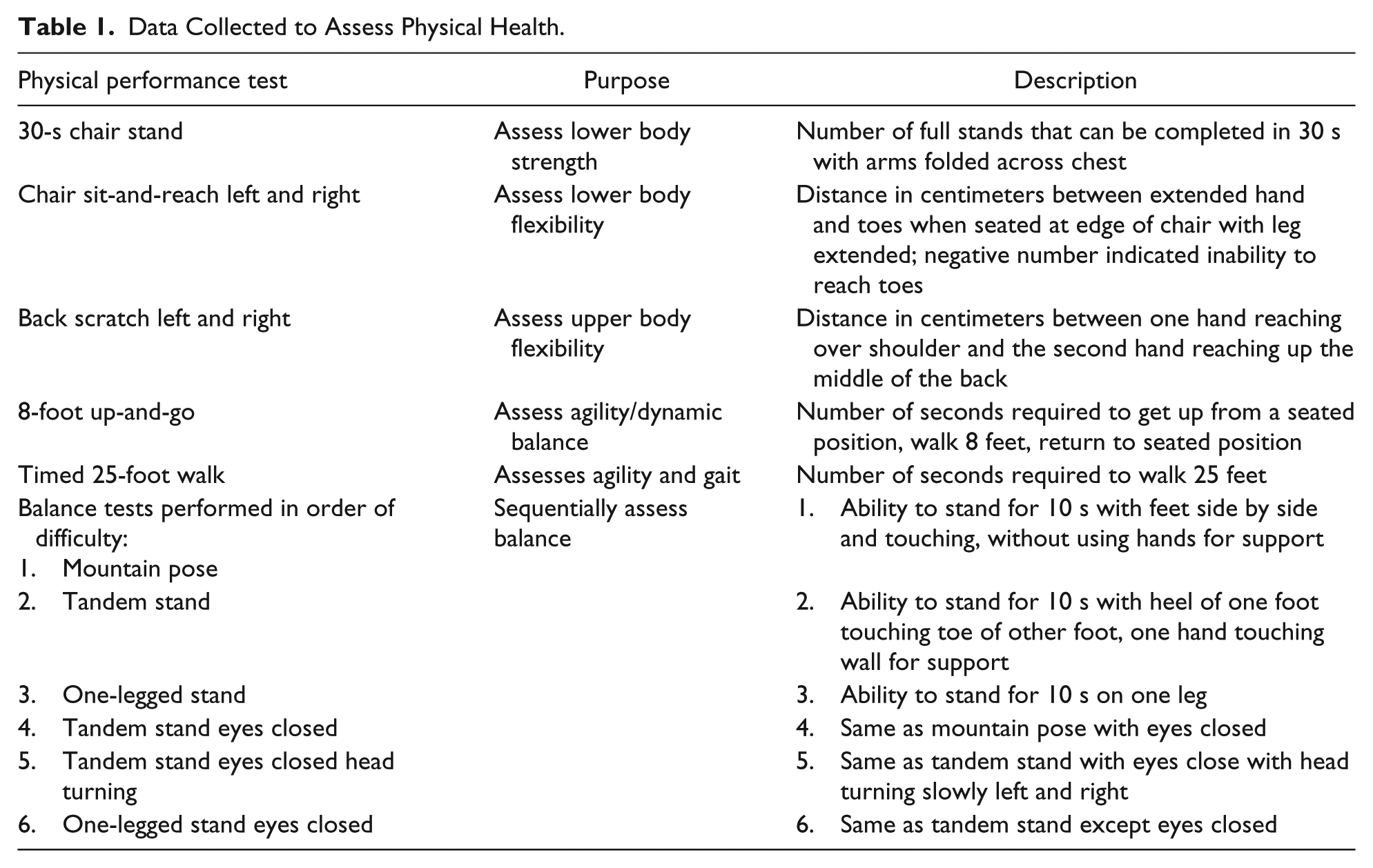
In addition to demographic and body composition data, participants were evaluated using fitness measures from the Senior Fitness Test before and after 10 weeks of strength training. The fitness measures included the “chair stand test” assessing lower body strength and muscular endurance, the “8-foot up-and-go” assessing balance and coordination while moving, the “chair sit and reach” assessing lower body flexibility, and the “back scratch” assessing upper body flexibility. Balance was assessed using a graded balance test (Baker et al., 2001). Detailed descriptions of each test are outlined in Table 1.
Data Collected to Assess Physical Health.
Descriptive statistics including age, height, and weight were produced, and matched pair t tests using an alpha level of .05 and 95% confidence interval (CI) were used to compare differences in measurement of physical indicators of strength, flexibility, and balance. Two-way ANOVA was conducted to examine the age effects of exercise on strength, balance, and flexibility before and after the exercise intervention.
A follow-up survey was mailed to participants 3 months following the completion of the exercise program. The participants did not schedule a visit to complete this form. They were asked to voluntarily complete the survey and return anonymously by email or via mail in the preaddressed envelope.
Results
Participants showed statistically significant improvement from the pre- to post-assessment test in each of the physical markers used to assess strength and flexibility (Table 2). Participants with greater attendance to the exercise protocol (n = 6; attendance = 100%) showed statistically significant improvements in the sit-and-reach test (p = .03 vs. .06) and balance test (p = .004 vs. .01), whereas those in the lower quartile for attendance (n = 6; attendance = 81%) did not show significant improvement in those tests.
Pre- and Post Differences in Group Means From Physical Fitness Test.

Participants also showed statistically significant improvement - in %BF (Table 3). Furthermore, participants with greater adherence to the exercise program had significant reductions in fat mass (p = .09 vs. .30) and total body mass (p = .05 vs. .39) compared with participants in the lower quartile for class attendance who did not statistically improve in those categories.
Pre- and Post Differences in Group Means for Body Composition.

Note. %BF = percent body fat; BMD = body bone mineral.
Three months following the completion of the program, participants were mailed a follow-up survey. The survey had a 78% response rate. Of those who returned the follow-up survey, 94% of participants continued to lift weights at home, in a group, or at a gym; 61% agreed or strongly agreed that their ability to do everyday tasks had improved (i.e., carrying groceries, taking out the trash, walking up stairs, doing light housework, etc.); and 78% described their health as either “somewhat improved” or “a lot more” improved after completing the program.
Discussion
The results of this study display that the ASSSH program significantly improved several parameters of physical fitness, including lower body strength. This was demonstrated by the improvement in the chair stand test, in which participants were able to perform 5.43 more stands in 30 seconds after 10 weeks of programming. Participants also significantly improved the time to complete the 8-foot up-and-go test (−0.83 s), which demonstrates an improvement in balance and coordination while moving. The 0.83s improvement was not only statistically significant, but also functionally relevant and meaningful in this population. Poor balance is strongly coordinated with an increased risk of falls for older adults (Lord, Ward, Williams, & Anstey, 1994), and although balance training was not a major component of the intervention, balance and coordination improved as a result of the strength training. In addition, improvements in balance performance have been shown to be attributable to increases in strength. Participants improved their balance test score by 47.7%. These findings are consistent with previous research demonstrating that strength training can improve balance in older adults (Orr, Raymond, & Singh, 2008).
Participants also significantly improved upper and lower body flexibility as shown in the chair sit and reach and the back scratch tests. Participants improved their chair sit and reach measures by 2.0 inches (in.) on the right side and 2.1 in. on the left. Participants also improved their upper body mobility shown by an increase in the back scratch test by 1.5 in. on the right side and 1.2 in. on the left side. Although strength training was the primary focus on the intervention, stretching was incorporated daily into the training sessions, so an improvement in flexibility (upper and lower body) was expected.
In addition, participants lost 1.2 lbs of fat mass overall and gained 1.0 lbs of lean body mass, equaling a weight loss of only 0.2 lbs, demonstrating that although some participants gained weight, the weight gained was likely to be lean mass and not fat mass. This statistic highlights just one of the benefits of strength training, to improve overall body composition not decreasing total body weight per se.
The 3-month follow-up survey revealed that participants’ ability to perform everyday tasks was not significantly improved. This could be due to the fact that participants were already particularly fit for their age, so their ability to improve upon everyday tasks was limited.
Study Strengths
It is worth mentioning that the physical fitness of the female participants in this study was much higher than the national average for this age population. The national range of scores for men in chair stands is 12 to 19 stands for adult men aged 60 and older. By comparison, the range of chair stands completed by the men (range = 63-69 years) at baseline was 15.5 (range = 11-20 stands), roughly average for their age group. However, the women in this study performed above the national average. The range of scores for women in chair stands is 10 to 17 stands for adult women aged 60 to 74 years. By comparison, the chair stands completed by the women in this study (range = 50-76 years) at baseline was 18.8 (range = 8-35 stands), which is considered above average for the 60 years and older age group. The fact that significant improvements in fitness were observed with this relatively “fit” group illustrates the real-life effectiveness and ability to translate this program into the community.
Another strength to this study was overall exercise adherence. Compliance to the aforementioned protocols was excellent (average attendance = 89.1%). Participants did occasionally miss class due to illness, scheduling conflicts, and so on. Those who missed the face-to-face class sessions were sent a list of specific exercises to complete at home. At the next training session, participants self-reported if they completed the at-home exercises or not. Of the six participants who missed training sessions, four completed the routine at home, increasing the overall adherence rate to 90.5% for all strength sessions completed (M = 18.1 out of 20 total sessions). Six of the 23 participants attended 100% of the exercise sessions.
Collectively, participants’ body fat decreased by an average of 1.24 lbs, and lean mass increased by an average of 1.0 lb. It has been found that human muscle can exert a force of 6 kg/cm2 of cross-sectional area, which is equivalent to 85 lbs/in.2. Given that muscle mass and strength are significant indicators of fall risk, the increase in lean mass in these participants is likely to be biologically significant, if not statistically significant, in this relatively small cohort.
Apart from the contributions of muscle weakness and deficits in balance, low bone mass is also a risk factor for fracture (Cummings, Black, & Nevitt, 1990; Hui, Slemenda, & Johnston, 1989). This particular strength training intervention did not show significant improvements in total body bone mineral (BMD) or regional BMD. Yearlong studies of high-intensity resistance training have shown an increase or maintenance of BMD in postmenopausal women (Villareal et al., 2011). However, given the time course of bone remodeling (Kronhed & Moller, 1998), it was unlikely that a detectable change in BMD would occur following this 10-week training period.
Although there was a lack of sedentary control group in this study, it is likely that this exercise intervention avoided BMD attenuation, and without exercise, BMD would have likely decreased in these participants as a result. Research by Shah et al. (2011) supports this concept in their study examining the independent and combined effects of weight loss and resistance training on bone metabolism in relation to changes in BMD in obese older adults. The results showed that bone loss at the total hip was relatively less in the diet-exercise group (−1.1%) than in the diet group (−2.6%), whereas BMD increased in the exercise group (+1.5%). These data demonstrated that exercise training combined with diet-induced weight loss not only reduces frailty but can also attenuate the weight loss–induced reduction in BMD and lean body mass, suggesting that a combination of weight loss and exercise training may be an important prescription for obese older adults.
Study Limitations
The majority of the limitations in this study stemmed from the community-based design. Community-based exercise programs such as ASSSH do not follow suit with traditional methods and ideal research design, environment, and methods. The best approach to this type of study is to randomize participants after recruitment and baseline testing to a control group and intervention groups. This, unfortunately, was not feasible. The lack of control group in our current study limits the level of evidence our data can provide. Had we recruited a purely non-exercise control group, between-group differences might have been more marked. Second, we relied on field measures of strength, balance, and flexibility to assess fall risk, which may be limiting by ceiling effects rather than laboratory-based objective measures, which would require inaccessible, expensive equipment such as a force-plate, perturbation platform, or sway meter (Cyarto, Brown, Marshall, & Trost, 2008). The lack of a test to assess aerobic capacity could also be viewed as a limitation of this study.
Finally, although the ASSSH program significantly improved flexibility, balance, and strength of participants, it is also worth mentioning that improving a fall risk factor does not guarantee a fall reduction. There is a need for a larger study of this design to evaluate the effect that is powered to detect a treatment effect on falls, and ideally injurious falls and fractures (Khan, Liu-Ambrose, Donaldson, & McKay, 2001).
Conclusions and Future Directions
The purpose of this study was to determine the effectiveness of the MU Extension program ASSSH on reducing fall risk. Older adults are the fastest growing segment of American society. Those who maintain good muscular strength, flexibility, and balance by exercise participation have a lower risk of falls, enjoy a better quality of life, and generally live longer than their inactive counterparts. Unfortunately, there are few community-based exercise programs targeted at older adults. ASSSH is a viable option for seniors to improve their health and demonstrates that appropriately supervised community-based exercise classes can be safe for older adults prone to osteoporosis, osteopenia, and risk of falling.
Despite the compelling evidence, older adults have the lowest rates of participation in formal exercise programs among all age groups (Sims, Hill, Davidson, Gunn, & Huang, 2007). Long-term weight loss is a difficult task, and most individuals who start with good intentions and commit to change their behaviors fail to continue. However, long-term adherence to physical activity is essential for the maintenance of health benefits. MU Extension professionals can use behavior change strategies to enhance participants’ motivation and adherence to regular physical activity and a healthy diet, rather than only focusing on weight changes. In addition, flexibility programs may be useful as an alternative exercise program for older adults with physical limitations who do not find resistance training manageable or appealing. The benefits of including flexibility programs on alternate days with resistance training is an interesting potential area for future research and warrants further investigation.
There is an increasing demand for research studies that clearly define the dimensions of exercise needed to improve overall health. Decades of experimental research have shown that exercise appears to play an important role in preventing falls among older adults. However, there is a limited availability of low-cost, exercise-intervention programs to help increase strength, flexibility, and balance in older adults prone to falls. The demand for this type of organized community program will increase as the number of aging adults continues to grow older over the next several decades. ASSSH has shown significant and meaningful improvements in strength, balance, and flexibility and is a functional option for older adults looking to keep their independence and improve their quality of life for years to come.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.