
Abstract
The rising prevalence of mental health disorders among children and adolescents presents a significant and ongoing challenge for healthcare and education systems. Child and adolescent mental health nurses are central to the early identification, ongoing monitoring, and provision of emotional support to young people and their families. Despite their essential contribution, research into their professional experience remains limited, particularly in regions where specialist services and qualified nursing professionals are scarce. This descriptive phenomenological study explored the role of nurses in addressing the mental health needs of children, adolescents, and their families in Castile and León (Spain), with the aim of identifying the principal challenges, needs, and strategies for delivering high-quality care. Seventeen nurses currently employed in these resource-constrained services participated in the study. Data were analyzed using Moustakas’s phenomenological method. Six themes were identified, highlighting the complexity and high level of specialization required in child and adolescent mental health nursing. Findings emphasize the need to strengthen interdisciplinary collaboration, expand workforce capacity and service infrastructure, and promote greater family involvement in therapeutic processes. This study deepens understanding of the experiences of Castilian-Leonese nurses in this field and offers valuable insights to guide future research and innovation in mental healthcare provision.
Background
Concerns regarding child and adolescent mental health have gained significant prominence, emerging as a priority for health and education systems given the high number of young people facing emotional difficulties and psychological disorders that directly affect their school life, social life, and general well-being, and because of the consequences in adulthood (European Commission, 2016; Patel et al., 2018; Radez et al., 2021). This reality is particularly complex owing to the interaction of numerous risk factors, compounded by adverse situations, creating a multifactorial and challenging landscape (WHO, 2025a, 2025b).
The prevalence of mental health conditions and subjective distress among young people has increased since the COVID-19 pandemic, accompanied by a notable decline in overall well-being (Blanchflower et al., 2025; Weber et al., 2024). Globally, among individuals under 25 years of age, women’s mental health demonstrates more significant challenges compared to men’s (Blanchflower et al., 2025). At the European level, it is estimated that 13% of the population under the age of 19 has experienced some mental health problem: higher rates are observed in males up to 14 years, with a more pronounced impact on females between 14 and 19 (Vázquez et al., 2024).
According to the latest National Health Survey conducted in Spain, health problems limiting daily activities in the general population are categorized as follows: 83.41% physical, 5.45% mental, and 11.14% involving both physical and mental origins. Age-specific analysis reveals distinct patterns: among children aged 5 to 14, purely mental problems account for 10.67%, with an additional 10.57% experiencing both mental and physical limitations. The 15 to 24 age group shows similar trends, with 10.70% and 11.66% respectively. Both cohorts represent the highest percentages of mental health-related activity limitations (Spanish Ministry of Health, Consumer Affairs and Social Welfare, 2019a). For children under 15, the survey identified that 13.16% of the population aged 4 to 14 is at risk of poor mental health, with a notably higher prevalence among boys (15.63%) compared to girls (10.53%; Suárez, 2022). Notably, Castile and León emerged with one of the highest percentages, at 16.21% of children at risk (Suárez, 2022). Nationwide, behavioral disorders (including hyperactivity) accounted for 1.78% and mental disorders, such as depression and anxiety, 0.60%. The Strengths and Difficulties Questionnaire (score ≥ 14) further confirms Castile and León’s position among regions with the highest proportion of at-risk children and adolescents. Furthermore, a significant correlation exists between lower socioeconomic status and increased incidence of these mental health problems, particularly among girls from lower social classes (Spanish Ministry of Health, Consumer Affairs and Social Welfare, 2019b).
Deterioration in self-perceived mental health is linked to physical health, increased suicide rates (especially among young people), school absenteeism, and learning difficulties. It is one of the main causes of increased hospital admissions among young people (Blanchflower et al., 2025). In Spain, the Multidisciplinary Working Group on Mental Health in Children and Adolescents, which includes other societies that oversee pediatric health, warned in 2022 of an increase of up to 47% in mental health disorders among minors, observed through an increase in the volume of care due to greater demand for mental health consultations (Spanish Association of Pediatrics, 2022). According to the 2023 Registration Program study by the Castile and León Health Sentinel Network (Spanish Health Department of the Regional Government of Castile and León, 2024a), in 2023 there were 190 referrals to specialist consultations for every 1,000 children under the age of 14 with a health card in this region. The most sought-after specialties were ophthalmology (22.9%) and otolaryngology (13.6%), although it should be noted that 9.6% of referrals were to mental health services. Additionally, 25.2% of pediatricians cited the lack of diagnostic resources for mental illness as a key factor in their decision to refer their patients.
These data reinforce the need to implement effective strategies to address and mitigate mental health challenges in the child and adolescent populations in Spain (Vázquez et al., 2024). However, in Spain, mental healthcare for children and adolescents is insufficient, characterized by a fragmented care structure that is dependent on systems designed for adults and varies according to each Spanish autonomous community (González López et al., 2019). Ensuring adequate mental healthcare during childhood and adolescence is essential for promoting the comprehensive development of individuals. Various studies emphasize the need to effectively ensure this right, guaranteeing access to the support and resources necessary to build a dignified life with a future (Anta et al., 2022; González López et al., 2019).
Psychological and psychiatric care for children and adolescents requires an interdisciplinary response, in which nursing plays an essential role (Hartley et al., 2022). Nurses, especially those working in primary care and child and adolescent mental health services, are strategically positioned to provide early detection, ongoing assessment, and emotional support for both minors and their families. Their ability to establish therapeutic relationships, conduct educational interventions, and collaborate with other health and social care professionals makes them key players in a comprehensive approach (Luz et al., 2023). Recent literature recognizes that nurses play an essential role in promoting child and adolescent mental health and providing comprehensive support to families, reinforcing the need to incorporate their perspectives into all phases of the care process (Govindan et al., 2024). In the Spanish context, this role is implemented through specific mental health nursing consultations and partial hospitalization facilities, such as child and adolescent day hospitals (Spanish Health Department of the Regional Government of Castile and León, 2024a).
Although the educational environment remains crucial for promoting mental health, its effectiveness increases with coordination between health services (European Commission, 2016; González López et al., 2019). Studies such as that by Green et al. (2013) demonstrate that health professionals with specialized mental health training facilitate minors’ access to specialized resources. Aligned with this approach, the World Health Organization’s Child and Adolescent Health Strategy advocates for creating and enabling protective environments that prioritize children’s and adolescents’ participation and emotional well-being (Weber et al., 2024). From a legal perspective, the Law on Comprehensive Protection of Children and Adolescents against Violence (Spanish Organic Law 8/2021) mandates the provision of safe institutional environments, including a holistic promotion of psychological well-being—an approach that nursing inherently supports through its professional training and practice.
Despite nursing’s recognized role in caring for minors with mental disorders, few studies have explored their professional experiences through a qualitative and contextually grounded approach. This gap in the literature hinders a comprehensive understanding of nurses’ role and the specific challenges they face in different care settings, particularly in community or emerging healthcare contexts (Luz et al., 2023). Therefore, this study aims to highlight the role of nurses in comprehensive child and adolescent mental health care, analyze current care practices, and provide evidence that can contribute to the development of more inclusive health policies aligned with professional reality. Through a qualitative approach, this study aimed to give a voice to nursing professionals, recognizing their contributions, difficulties, and training needs within a rapidly transforming health system.
This study explored the meaning of the professional experiences of mental health nurses in Castile and León (Spain) caring for children and young people with mental disorders, to better understand nursing’s role in this practice context. The study’s motivation emerged from the authors’ research experience in education for students with mental illness (MFH and JFPL) and in nursing and psychology (LAM and RSC). Following in-depth discussions of their professional concerns, the researchers committed to conducting systematic research on the main challenges, needs, strategies, and proposals of nursing staff in addressing child and adolescent mental health, which would enable the provision of quality care focused on the child and their family environment. The following research question guided the study: How do nurses describe their lived professional experiences in child and adolescent mental health services?
Method
Study Design
This study adopts a qualitative methodology of a descriptive phenomenological nature (Husserl, 1983) with an empirical approach (Giorgi, 2009), aiming to provide a detailed and systematic description of a phenomenon’s structure as reflected in the participants’ everyday experiences without imposing external interpretations (Giorgi, 2009; Reiners, 2012). This methodological approach was chosen for its ability to capture the meanings that mental health nurses attribute to their experiences of working with children and young people affected by mental disorders in complex and emotionally demanding clinical settings (Öhlén & Friberg, 2023).
Participants
A convenience sample of actively practicing nurses working in child and adolescent mental health care in Castile and León was recruited from several healthcare settings across the region, including: (1) Child and Adolescent Mental Health Day Hospitals, recently established centers that include therapeutic and educational classrooms enabling minors with mental health difficulties to continue their schooling; (2) outpatient clinics located in general health centers throughout the region, which provide mental health consultations following referrals from Pediatric Services; and (3) an acute care hospital ward (psychiatric and pediatric) that includes a hospital classroom to support students’ ongoing academic curriculum. Nurses in management roles or those without direct clinical contact were excluded.
Potential participants were contacted by telephone by the research team using institutional contact information. Contact information was provided by an institutional gatekeeper (author RSC)—the president of the Nursing Association—within the scope of their professional responsibilities, without intervening in participation decisions. Following initial interviews, some nurses voluntarily shared contact information for other colleagues. All participants received prior study information, after which they decided to participate and provided informed consent.
Seventeen nurses (15 women and 2 men) working in child and adolescent mental health consented to participate. Just under half of the participants (47.1%) held a specialization in mental health. The sample reflected diverse profiles in terms of age, overall professional experience, and years of practice in child and adolescent mental health (Table 1).
Specific Description of the Sample.
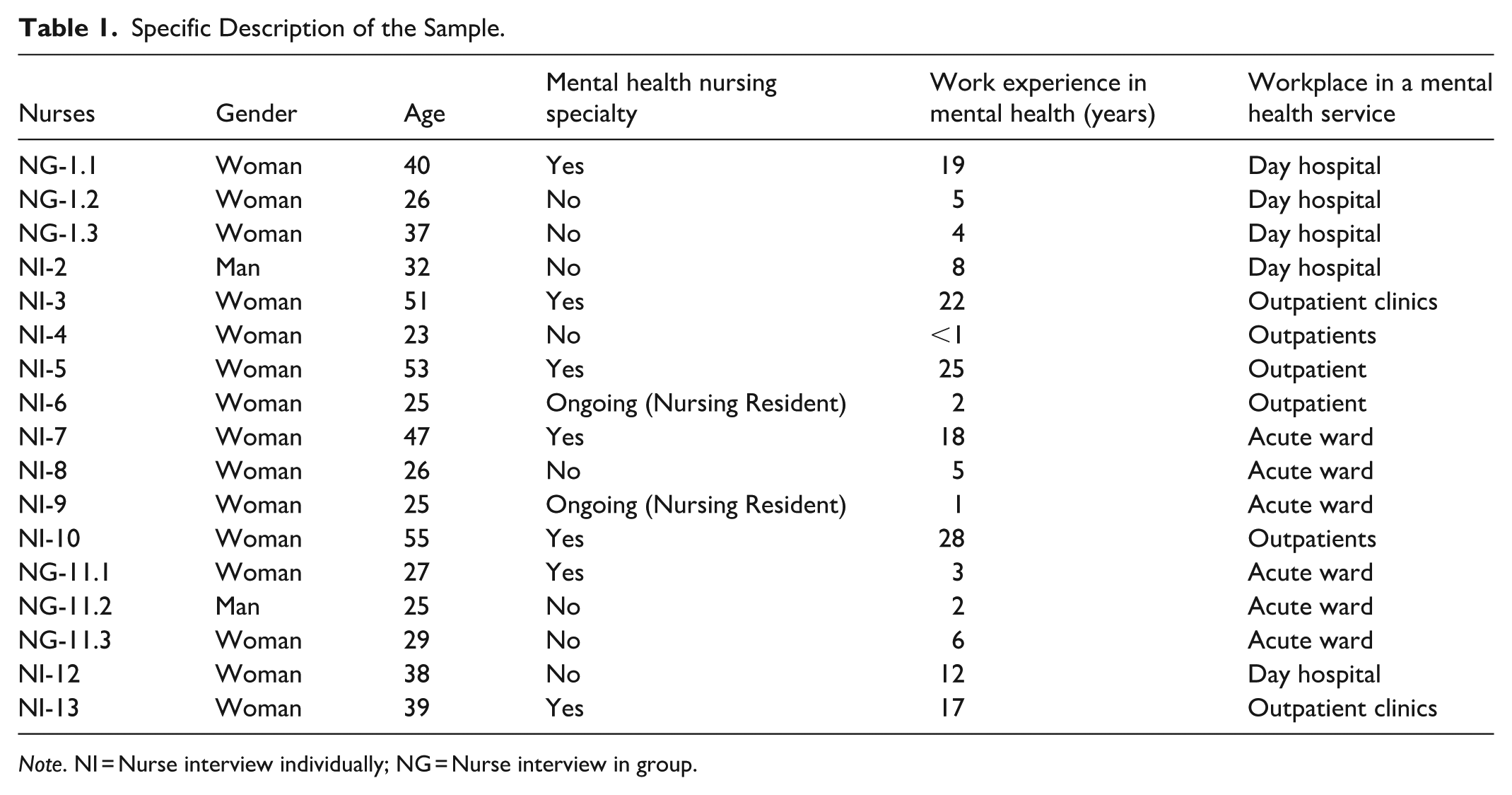
Note. NI = Nurse interview individually; NG = Nurse interview in group.
Data Sources
The data collection technique employed was phenomenological interviewing. The phenomenological interview constitutes an encounter with a phenomenon as it is experienced by a person who defines the characteristics of the phenomenon through their discourse, preventing the researcher from predetermining the phenomenon’s characteristics. Therefore, the interviewee is given the necessary space to bring the phenomenon to light and express it from their own consciousness (Guerrero-Castañeda et al., 2017). This format allowed us to explore personal and professional aspects while maintaining a consistent thematic framework.
A total of 17 interviews were performed for this research: 11 individual interviews and 2 group interviews with 3 participants per group. These group interviews were not focus groups, as no interaction or consensus was fostered among the participants; each participant responded independently. This methodological approach was adopted due to constraints in time and participant availability. The unit of analysis was individual: in the two sessions with three participants, each contribution was coded and analyzed separately, and subsequently all units were integrated into a common thematic synthesis.
The interviews were conducted during the first half of 2025 after participants signed the informed consent form and the research purpose was thoroughly explained. They were conducted individually (I) or in groups (G), with interview durations varying between 45 min to 2 hr, depending on the format. The interviews were audio-recorded with explicit participant consent and subsequently transcribed for analysis.
We decided to conclude data collection with 17 interviews, considering that the information obtained was sufficient to answer the research question. While traditional literature suggests that saturation can be reached between 12 and 16 interviews (Bartholomew et al., 2021; Guest et al., 2006), and in our case thematic reiteration was observed starting with the 12th interview, recent approaches question its usefulness. Given this, criteria such as “informational power” (Malterud et al., 2016), which prioritize the richness and relevance of the data rather than the number of interviews, were considered. Sample specificity, interview quality, and the clarity of the analytical aim supported our assessment of the sufficiency of the collected data.
The interview script sought to collect detailed information on multifaceted aspects of nurses’ professional practice in the field of child and adolescent mental health. It included questions aimed at understanding the sociodemographic, educational, and occupational profiles of the participants, as well as the roles they perform in different healthcare settings. The interview explored mental health needs among children, adolescents, and their families and their perception of how these needs evolve. They addressed the main clinical, family, and organizational challenges they face in their daily work and the strategies they use to deal with them. In addition, they explored the quality of coordination between the different members of the clinical team, identifying both strengths and potential areas for improvement. The interviewees shared their views on the impact they perceive of child and adolescent mental health resources on the therapeutic and academic process of children and adolescents. Finally, their proposals for improvement and innovation, both internally and across sectors, were collected to enhance the delivery of more effective, compassionate, and integrated care.
Data Analysis
Although the approach of this study aligned with Giorgi’s descriptive phenomenology (2009), the analysis process followed the steps described by Moustakas (1994), using them as a structured guide for analysis while maintaining a focus on the faithful description of the experience. Several detailed readings of the interviews were conducted, adopting a receptive attitude toward the nurses’ experience and their perceptions of the role of the nurse in child and adolescent mental health, setting aside our own assumptions (epoché or bracketing). Each statement or expression was treated as equally important and relevant, aiming to capture the meaning of the experience from the participants’ perspective. The researchers sought to understand, through their descriptions, the meanings inherent in their statements to discover common themes, identifying recurring elements and patterns to establish possible connections that would allow the creation of categories and subcategories, highlighting and listing the units of meaning (phenomenological reduction). This process was carried out using a manual qualitative analysis based on a phenomenological approach, which enabled capturing not only the descriptive aspects of their care practice, but also understanding the meanings professionals attribute to their role, their functions, the challenges they face and the improvements they propose (imaginative variation). Six themes were identified that structure the professional experiences of nurses in the different mental health facilities in the community as they are lived (synthesis of meanings): (1) Building a professional identity; (2) Addressing the situational vulnerability of minors; (3) Providing care through relationships; (4) Building care networks; (5) Providing care under resource constraints; and (6) Imagining possible futures. For a detailed overview of the analysis process, see Figure 1.

Diagram of the study analysis process.
Rigor
While acknowledging the diversity of our professional backgrounds, we employed the epoché strategy—characteristic of the phenomenological approach—by suspending our assumptions to prevent personal experiences from influencing data. This methodological process was further reinforced through collaborative analysis and researcher triangulation, thereby strengthening the study’s rigor and transparency. The research team’s collaborative engagement in both interview guide design and data analysis facilitated critical exploration and interpretive consensus, helping to ensure the study’s rigor and credibility (Lincoln & Guba, 1985).
Ethical Considerations
Ethical issues were carefully considered prior to conducting this study, which is part of a broader research project on students with childhood and adolescent mental illnesses. Following Ethics Committee approval (University Hospital of Burgos Ref. CEIm 2889), participant recruitment proceeded incrementally as nurses voluntarily agreed to join the study. The research strictly adhered to ethical principles of participant confidentiality (WMA, 2024) and secure data management (EU General Data Protection Regulation 2016/679; Spanish Organic Law 3/2018 on Personal Data Protection and Guarantee of Digital Rights).
Findings
The results are presented through interpretive themes, illuminated by direct quotations that articulate the meanings nurses attribute to their professional role and the experience of providing care in child and adolescent mental health. To promote transparency in the analysis, Table 2 lists the themes and subthemes. In addition, a description of the themes and sub-themes in Spanish, along with representative quotes, is included as a Supplemental File. We used the term “subthemes” to refer to internal variations of the phenomenon resulting from phenomenological reduction and the grouping of units of meaning (Giorgi, 2009; Moustakas, 1994).
Themes and Subthemes.

Theme 1: Building a Professional Identity: Vocation and Recognition in Child and Adolescent Mental Health
For the participating nurses, working in child and adolescent mental health transcends mere technical proficiency; it represents an ethical and emotional commitment that shapes their professional identity. Their sense of vocation emerges as a core value that legitimizes their presence in a complex clinical environment, where the genuine desire to engage—“wanting to be there”—is perceived as an essential prerequisite for meaningful care: I mean, I’d add that nursing is really a calling. . . you know? And when you step into mental health, it’s like there’s another layer of vocation on top of that. And if we’re talking child and adolescent mental health, that’s another step of vocation. So, yeah. . . to me, working in mental health with kids and teens is a place you really have to want to go to. You really need to look for people who genuinely want to be there. (NI-2)
The concept of “adding vocational steps” illuminates how the professional role is constructed through layers of personal commitment that transcend formal academic training. Professional identity is perceived as fragile and under-recognized, generating tension between the idealized vision of the role and the institutional realities: What does it mean to be a mental-health nurse? I don’t know. . . I’d have to think about it. I guess it’s being able to use skills you don’t always get to develop in general practice, and that you definitely don’t learn in nursing school. . . like, you know, real psychological skills. But it’s also frustrating sometimes, because you do see changes or progress, but they’re so small. . . while in general medicine you do something and right away you see it working. (NG-1.1)
Specialized training is mentioned not only as a technical requirement, but also as a means of preserving that professional identity and avoiding a sense of professional precariousness: It’s really important that the nurses running a child and adolescent clinic are actually mental-health specialists. Because, you know, when they bring in a nurse who doesn’t have the specialty, what usually happens is. . . well, like here in my clinic, they end up just taking blood pressures and not much else. So, yeah. . . having the proper training really matters. (NI-13)
In this regard, the absence of specific training programs is seen as a lack of institutional recognition of the complexities involved in care within this field: It’s true that the psychiatry specialty in mental health has come out, and they’re starting to create one for psychologists too. And, well, child and adolescent mental health is really different. It’s related, of course, to adult mental health, but it’s still different, and it’s so important to have nurses who are trained for it. . . nurses who have the specialty. And, you know, even within the specialty, we have to keep learning. I go to a lot of courses, and to a lot of conferences. . . (NI-10)
The meaning attributed to the professional role centers on vocation as a prerequisite for caregiving, training as a way to sustain professional identity, and institutional recognition as an unfulfilled obligation. Being a nurse in child and adolescent mental health involves navigating a constant tension between the desire to care and the lack of supportive structures. In short, the experience is shaped as a vocational practice that is intensified in this field, sustained by personal commitment, and strained by limited recognition and specialized training.
Theme 2: Addressing the Situational Vulnerability of Minors: Supporting Them With and Through the Family
Nurses are facing rising levels of self-harm, severe anxiety, and identity crises as these pressures disrupt the usual rhythm of caregiving, creating an urgent ethical and practical need for earlier and more effective support: Since September up to now, self-harm has gone up a lot. And self-harm along with suicidal thoughts. . . even suicide attempts, honestly. And during this school year, we’ve also seen the age dropping. Now, at the end of the year, almost all the kids hurting themselves are in the first grade of ESO [Compulsory Secondary Education]. . . around twelve years old. (NI-13)
This early increase is seen as an ethical warning that calls for a reorganization of the professional role, with a stronger focus on containment and prevention. However, this urgency runs up against the persistent difficulty of addressing the problem when the minor withdraws and rejects help, creating an experience of frustration and a feeling of limited professional agency: Yes, for me, the most frustrating thing is trying to help them and address the problem that is affecting them at that moment. And often they won’t let you. And they are so closed off that they don’t allow you to offer them the help you are offering. (NG-1.1)
These experiences come with the understanding that care cannot be delivered in isolation. The family emerges as essential to maintaining the continuity and sustainability of the child’s psycho-emotional well-being. In this context, involving families takes on a significance that goes beyond the technical aspects of care; it becomes a way to deepen care and prevent it from becoming fragmented: Prevention really starts with families (. . .) And honestly, a lot of the time the problem is in the family system itself. So if you’re not treating what’s going on inside the home, how are you supposed to fix it? (NI-6)
Experience shows that educating and supporting parents are not secondary tasks, but rather the bridge that translates clinical care into everyday practices, ensuring continuity between the clinic and the home. However, this possibility depends on the type of healthcare center. In day hospitals where specific programs (such as ADHD or eating disorders) have been implemented, the family actively participates in group sessions: We see the kids first for the initial appointment, and then we bring the parents in. . . sometimes we meet just with the parents, and other times with everyone together. (NG-1.2)
Meanwhile, in the acute inpatient ward, parental involvement is low, as reported by a nurse who works with these types of services: So, we don’t really get to do much family work with the parents, because they only come in for visits about two hours a day. And when the visit ends, that little moment afterward is when we talk with them and ask how things are going. (NI-7)
In outpatient clinics, parental involvement in sessions has been structured as part of the standard intervention protocol: So, we always see the child first, and then we see the child with the parents. . . no matter what, in every appointment. It’s not like we’re treating the parents, it’s more that we talk things through. . . you know, the things they need to reinforce with the kid, or whatever’s going on. They’re minors, so we keep the parents informed and tell them what they should be keeping an eye on at home, how to handle things. (NI-10)
Care is structured around three dimensions: the moral urgency to provide support in the face of early vulnerability, the family as an indispensable partner (co-agent), and the care system as a facilitator of continuity. At its core, this experience involves responding to the minor’s situational vulnerability within an ethical urgency that transcends the conventional timeframes of care, strained by the need for integration and the limitations of the system.
Theme 3: Providing Care Through Relationships: Roles That Go Beyond Technique
Nurses describe their roles in child and adolescent mental health as a woven fabric of clinical, educational, and emotional actions, where technical skills are intertwined with the therapeutic bond. Care is not limited to “performing procedures,” it is experienced as accompanying, supporting, and sustaining therapeutic continuity across different settings.
In outpatient clinics, clinical interventions such as monitoring vital signs and medication follow-up are understood as essential for ensuring safety and stability, but also as part of a broader process aimed at understanding each minor in their uniqueness.
We bring the patient in and take their vitals (. . .) We also do medication follow-ups, especially for kids with ADHD (. . .) and then we also do follow-ups for eating-disorder consultations. (NI-3)
This technical component is complemented by educational and preventive actions that nurses view as essential strategies for ensuring continuity of care beyond the healthcare setting. In day hospitals, psychoeducation on healthy habits, emotional management, and the use of technology becomes a space where minors can rebuild their abilities and strengthen their autonomy: We do a lot of work on basic activities of daily living (. . .) health education, things like nutrition, exercise, hygiene habits, sleep, substance use, technology. And, you know, emotional regulation, treatment adherence. . . all of that. (NG-1.3)
Alongside this, nurses take on crisis containment as a role that deeply engages their professional identity, where responding quickly and empathetically to self-harm or episodes of anxiety is not just a task but an ethical commitment to the minor’s vulnerability. This dimension also extends to organizational and follow-up responsibilities that sustain the structure of care over time.
Beyond the differences between outpatient clinics, day hospitals, and acute care units, the participants agree that the therapeutic relationship is at the core of all their roles. Providing care means creating a safe, nonjudgmental space where the minor can feel fully acknowledged and understood: We don’t really have “techniques,” you know? So the most important thing is the therapeutic relationship. The therapeutic relationship is absolutely essential in mental health (. . .) You have to show empathy, really listen (. . .) Just making sure they feel comfortable, not judged, that they feel like they’re coming here so we can help them however we can. (NI-8)
Professional practice is oriented toward clinical stability, the promotion of autonomy through education, and the maintenance of the therapeutic bond as the foundation of care. Care is conceived as a network in which technical procedures are subordinated to the therapeutic relationship, revealing the constant interaction between clinical techniques and humanity, where each intervention is experienced as an opportunity to restore continuity and meaning in the minor’s life.
Theme 4: Building Care Networks: Coordination as an Experience of Integration and Fragmentation
Nurses experience interdisciplinary coordination as essential for managing the complexity of care in child and adolescent mental health. When teamwork takes place in shared spaces, it is described as fluid and coherent. Each professional contributes a unique perspective to develop a comprehensive therapeutic plan: We have a really good multidisciplinary relationship. Every day we have a meeting with the social worker, the psychiatrists who see the kids, the psychologist, the nursing assistants, the occupational therapist, and us nurses. So every day we kind of go over how each child is doing. And I’d say yes, the communication is really good, and the work is definitely teamwork. (NI-9)
This sense of integration is felt most strongly in day hospitals and acute care wards, where the daily interactions allow for collaborative decision-making and comprehensive support. In contrast, in outpatient clinics, coordination is experienced as fragmented and still developing, creating a sense of professional isolation.
Coordination is experienced as oscillating between integration and fragmentation. When teamwork occurs in shared spaces, nurses perceive a sense of flow and coherence in care, enhancing their professional agency. In contrast, the segmentation of outpatient services creates feelings of isolation and limits continuity. Beyond the healthcare setting, collaboration with the educational system is seen as essential for the social reintegration of the minor, although its availability is not always guaranteed. Building networks is not merely a technical requirement; it represents the opportunity to provide care beyond healthcare alone, connecting health, education, and family.
Theme 5: Providing Care in Times of Scarcity: Experiencing Constraints as an Ethical and Practical Tension
Nurses perceive structural and organizational constraints as a condition that strains the very meaning of care. The lack of appropriate space forces nurses to improvise and reinvent routines, challenging their ability to preserve privacy and therapeutic quality: So the space is really limited, and there’s this one room that ends up being everything. . . the therapy room, the workshop room, the arts-and-crafts room, the playroom, and the dining area. And we try to move the folding tables around (. . .) We try to take them outside for walks (. . .) but yeah, with the space issues we have. . . (NI-2)
In day hospitals, staff shortages are perceived as a direct threat to the integrity of care, generating a sense of helplessness in the face of growing demand: For more than 24 [patients], no. And if the staff doesn’t increase, we just wouldn’t be able to do our job properly because we wouldn’t have the time. (NG-1.3)
In the acute inpatient unit, the shortage of beds is experienced as a structural limitation that fragments continuity of care, forcing rapid turnover and waiting lists that run counter to the need for longer admissions.
In outpatient clinics, the rigidity of the care model and the lack of time make it difficult to implement preventive and group-based interventions, leading to professional frustration at not being able to provide truly comprehensive care: The demand has grown so much that (. . .) I mean, if we had, imagine, two nurses, we could run more groups (. . .) Basically all our time is taken up by follow-ups (. . .) so there’s no time to run extra programs. . . (NI-13)
Providing care under conditions of scarcity is experienced as a practice caught between the ethical desire to offer comprehensive, holistic care and the structural impossibility of doing so. Material and organizational constraints are not merely technical barriers, they are lived experiences that challenge professional identity, generating a sense of powerlessness and threatening the very essence of care as a humanized and continuous act.
Theme 6: Imagining Possible Futures: Proposals Expressing a Desire for Continuity and Comprehensive Care
Nurses not only point out shortcomings; they also envision improvements that reveal the meaning they attribute to care. Their proposals are understood as ethical and strategic responses to sustain continuity of care and expand its preventive and community reach.
In the acute care unit, the idea of a transitional program between child–adolescent and adult services emerges as a way to prevent abrupt breaks that contradict the very logic of care: Actually, I’ve brought up the idea of a transition program, because it’s true that the child and adolescent teams are really protected (. . .) But the jump from child-adolescent to adult services is huge. And honestly, there’s no real difference between a kid who’s 17 years and 11 months and one who’s 18, but the kind of care they get is completely different. (NG-11.3)
The expansion of beds and physical spaces is described not only as a technical improvement, but also as a necessary condition for providing care without fragmentation. In day hospitals, having environments adapted for both group activities and private interventions is experienced as creating settings where care can unfold with dignity and safety.
Across outpatient clinics, day hospitals, and acute care units, nurses emphasize the need to strengthen their work with families, recognizing them as key partners in supporting the minor’s well-being: More intensive programs depending on what the families need (. . .) And when we’re talking about children, the families are the ones setting the routines at home. So I think it’s necessary for families to know what they need to change, or to have the support to actually make those changes. . . or even just to be able to cope with their child’s illness. (NI-5)
Imagining possible futures is understood as a practice that affirms an ethical desire to care beyond current limitations. These proposals are not merely technical improvements, but forward-looking visions that express the deeper meaning of care: ensuring continuity, expanding preventive reach, and sustaining family involvement. For nurses, planning changes means envisioning a comprehensive and humanized model in which care is never interrupted and can be delivered with dignity and consistency.
Discussion and Implications
This study enabled us to understand how mental health nursing professionals perceive their professional reality and experience working with children and young people with mental health conditions. The interview analysis revealed both the meanings nurses attribute to their professional role and the primary needs, challenges, strategies, and recommendations for improving care for minors.
The complexity of nurses’ roles in child and adolescent mental health services in Castile and León, as described by the interviewees, aligns with the qualitative study by Hartley et al. (2022), which highlights how the therapeutic relationship forms the core of nursing intervention in child and adolescent mental health. Through a phenomenological approach focused on nurses’ lived experiences, our study reveals that their intervention extends far beyond clinical or instrumental functions. Instead, it demands a holistic approach that integrates physical care, emotional support, and educational guidance. Specializing in child and adolescent mental health nursing requires continuous professional development, interpersonal sensitivity for building therapeutic relationships, and exceptional team collaboration skills.
Ravens-Sieberer et al. (2023) and Ibeziako et al. (2022) support these findings, highlighting that the shortage of specialized staff and intermediate resources significantly undermines care response capabilities, negatively impacting patients’ emotional stability and care continuity. The demand for youth mental health services has surged in recent years, as documented by the 2023 Registration Program of the Sanitary Sentinel Network of Castile and León (Spanish Health Department of the Regional Government of Castile and León, 2024b). The data reveals 190 specialized consultations per 1,000 children under 14 years old with health cards in the region.
The findings emphasize the critical need to enhance interdisciplinary coordination—not merely as a desirable approach, but as a fundamental strategy to ensure coherent, effective, and patient-centered care for young individuals. As the American Academy of Child and Adolescent Psychiatry (2023) highlights, effective coordination between professionals and services reduces relapses and improves treatment adherence in pediatric mental health contexts.
Likewise, the participants repeatedly emphasized the limited involvement of families in the therapeutic process. Active family inclusion not only optimizes clinical outcomes but also supports the sustainability of the emotional well-being in the child’s daily environment. While family involvement is widely recognized as an essential element of pediatric and mental health care (Committee on Hospital Care, 2012), our findings highlight the ways in which it is operationalized in specialized services. Nurses described developing strategies to engage families and coordinate care across multiple settings, signaling ongoing professional development and potential policy implications. These results align with Pine et al. (2024), who noted that active family inclusion not only improves clinical outcomes but also sustained emotional support within the family context. This perspective is consistent with the Committee on Hospital Care (2012), which advocates for a family-centered care model as a quality standard in pediatric practice. Addressing the challenges identified in our study may involve three key strategies: developing flexible, intensive family-centered programs that provide psychoeducation and support beyond routine clinical encounters; strengthening staffing and reorganizing clinical time to enable therapeutic groups, guidance sessions, and transition programs; and establishing continuity-of-care pathways to ensure families receive sustained support throughout critical stages of the treatment process (Pine et al., 2024).
The Committee on Hospital Care and the Institute for Patient and Family-Centered Care (2012) define patient- and family-centered care as an approach that recognizes the family as the child’s primary source of strength and support, advocating for respectful partnerships between families and healthcare professionals across all care dimensions—from information sharing and collaborative decision-making to service organization. Building on this foundation, Kuo et al. (2012) emphasize that engaging parents and caregivers is a fundamental quality standard, not an optional addition to individual treatment. Qualitative research has consistently demonstrated that family-centered care correlates with enhanced patient engagement, improved psychosocial outcomes, and increased satisfaction for both children and their caregivers (Shields et al., 2006). Family-centered pediatric care is grounded in key principles: respecting family values and preferences, mantaining open and collaborative communication, shared decision making, and delivering flexible care that responds sensitively to each family’s unique context (Pettoello-Mantovani et al., 2009).
In child and adolescent mental health services, meaningful family involvement significantly improves patient engagement, care continuity, and psychosocial outcomes (Hartley et al., 2022; Waid & Kelly, 2020). However, research reveals that limited structural and organizational support often results in fragmented and intermittent family participation (Luz et al., 2023; Sjolseth et al., 2026). Our findings extend this evidence to child and adolescent mental health nursing. Nurses describe concerted efforts to implement family-centered principles in daily practice—for instance, by intensifying preventive and supportive work directly with families in outpatient clinics and day hospitals. They actively assist caregivers in adapting daily routines and developing effective responses to a child’s illness. Simultaneously, nurses report that persistent challenges such as time constraints, complex family dynamics, and service fragmentation significantly restrict their ability to consistently engage families. These observations closely mirror tensions identified in previous qualitative and systematic review studies (Hartley et al., 2022; Luz et al., 2023; Waid & Kelly, 2020).
Another key dimension highlighted by nurses was the need to improve human resources and infrastructure to fully leverage all the preventive and community-based potential of their work. In this sense, the findings align with those described by McEnany et al. (2020), who warned of the unnecessary prolongation of hospital stays due to a lack of alternative resources—a critical barrier for effective care. Recent studies, such as Brynes et al. (2021), have documented the sustained increase in mental health-related visits to pediatric emergency services, which further strains available resources and underscores the need for intermediate and flexible care services.
In response to these deficiencies, nursing teams have identified innovative proposals advocating for more flexible care models focused on continuous patient monitoring. Studies such as Foster et al. (2025) emphasize the significance of home-based and longitudinal approaches, particularly for children and adolescents with high medical and social complexity. These approaches offer an effective and humanized alternative that enhances therapeutic adherence and reduces recurrent mental health crises. The findings of Batlle et al. (2023) further support this model, highlighting that flexible monitoring approaches—including home-based interventions—can significantly improve patient treatment compliance.
Advanced planning for transition processes, particularly the shift from child and adolescent mental health services to adult mental health systems, emerged as a critical challenge in the study. Aligning with Segura-Frontelo et al. (2020), participants emphasized the crucial importance of a structured transition between the child-adolescent and adult mental health systems to prevent potentially harmful interruptions in the therapeutic care. Collaborative teamwork and meticulous planning are essential to mitigate care discontinuities that could negatively impact clinical outcomes and social integration of young patients. Care models incorporating principles of continuity and anticipation, as documented by White et al. (2018), provide valuable guidance for navigating this complex transition in regional healthcare settings.
In summary, implementing organizational strategies—as those proposed by Winner et al. (2025)—could enhance care continuity and reduce patient readmissions while reinforcing nursing’s critical role in supporting therapeutic relationship. Benjenk and Chen (2018) substantiated these findings, demonstrating that targeted nursing interventions can significantly decrease patient recidivism in mental health services. Such interventions have proven to positively impact the sustainability and operational efficiency of healthcare delivery (Pugh et al., 2021). These proposals are not only operationally viable but also supported by empirical evidence across diverse clinical settings, thereby strengthening their potential for regional implementation.
Study Strengths and Limitations
This study offers a novel and significant contribution to the field of child and adolescent mental health by providing in-depth qualitative insights into the unique perspectives of nurses working in specialized care services across Castile and León. Through phenomenological interviews, researchers captured the lived experiences of these professionals, illuminating their role from both humanistic and transformative perspectives. The methodology facilitated a comprehensive understanding of nursing care, highlighting its pivotal role in establishing therapeutic relationships and bridging clinical, educational, and family domains. These findings provide a critical foundation for guiding future research, shaping policy interventions, and advancing the quality of care for children and adolescents with mental disorders and their families.
The study also presents several limitations. While the number of participants was sufficient for phenomenological analysis, the findings were confined to Castile and León, thereby limiting comparability with other autonomous communities or international contexts. Two group interviews were conducted with 3 participants each, alongside 11 individual interviews. Although these group interviews were not traditional focus groups and participants responded independently, this interview format may have potentially influenced the spontaneity and depth of responses, a factor that warrants careful consideration during findings interpretation.
Another recognized limitation is the gender imbalance among participants, which aligns with the predominantly female composition of the nursing profession (approximately 85% women in Spain and 90% worldwide). However, this imbalance is not considered a significant source of bias, as since the study focuses on understanding professional roles in mental health rather than sex-based differences. While acknowledging the lack of gender diversity, the interpretive quality of the findings remains robust, given that phenomenological methodology prioritizes the depth and richness of individual experiences over statistical representativeness.
Future research should comprehensively address multiple dimensions of child and adolescent mental health care. This includes employing standardized interview formats, analyzing individual and group data separately to mitigate potential bias, exploring the longitudinal impact of nursing interventions on family well-being, and conducting comparative studies on mental health service organization across Spanish regions. Researchers recommend developing mixed-method or evaluative studies to design evidence-based strategies, investigating nursing staff’s working conditions and emotional burden, and examining institutional support policies and professional burnout prevention mechanisms. Ultimately, family participation in therapeutic processes emerges as a critical aspect requiring more comprehensive research attention in mental health domains.
Conclusions
This phenomenological study provided profound insights into the role of nurses in child and adolescent mental health services. The research revealed that nursing interventions extend far beyond clinical boundaries, emerging as a critical mediating force between healthcare, educational, and family systems. Through an in-depth analysis of professional experiences, the findings highlighted several key imperatives: strengthening inter-institutional collaboration, expanding human and structural resources, and promoting family engagement in therapeutic processes.
The study distinctively recognizes child and adolescent mental health as a specialized domain, fundamentally different from adult mental health services. This field demands specialized training and is characterized by a profound vocational commitment. Critically, the research underscores that the quality of care cannot be comprehensively understood without acknowledging its relational dimensions, contextual adaptability, and the significant emotional complexity inherent in nursing practice within this challenging landscape.
The study’s implications call for the development of organizational environments that prioritize care continuity, collaborative networking, and institutional recognition of nursing care as the essential core of mental health services. These conclusions are not definitive but rather provocative, opening new avenues of scholarly inquiry. They invite researchers to explore, through diverse methodological lenses, the multifaceted factors that shape the sustainability, effectiveness, and human-centered nature of mental health care for young patients and their families.
Supplemental Material
sj-docx-1-gqn-10.1177_23333936261435393 – Supplemental material for Voices From the Frontline: A Phenomenological Study of Nurses’ Roles in Child and Adolescent Mental Health
Supplemental material, sj-docx-1-gqn-10.1177_23333936261435393 for Voices From the Frontline: A Phenomenological Study of Nurses’ Roles in Child and Adolescent Mental Health by María Fernández-Hawrylak, Laura Alonso-Martínez, Raúl Soto-Cámara and Juan F. Pérez-López in Global Qualitative Nursing Research
Footnotes
Acknowledgements
This study was made possible through the support of the Burgos Official Nurse Association and the Regional Health Management of Castilla and León (SACYL) of Spain, whose commitment to advancing healthcare knowledge and practice was essential to the development and execution of this project. We are deeply grateful to all the healthcare professionals who generously shared their time, experiences, and insights. Their contributions were invaluable and form the core of this research. We also wish to acknowledge the Best Practice Spotlight Organization (BPSO) program, part of the Registered Nurses’ Association of Ontario (RNAO) initiative and the National and International Association of School Nursing (AMECE), for their support and alignment with the values that guided this research.
Ethical Considerations
All procedures were performed according to the ethical standards of the Declaration of Helsinki and the National Research Committee. This study was approved by the Ethics Committee for Drug Research of the Burgos and Soria Health Area of the University Hospital of Burgos (ID: Ref. CEIm 2889) and the consent of the Burgos Healthcare Complex (CAUBU), Regional Health Management of Castilla and León (SACYL).
Consent to Participate
Informed consent was obtained from all participants prior to the research, guaranteeing their voluntary participation.
Author Contributions
Contributed equally as co-first authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Open access funding provided by University of Burgos. This study has been fully or partially funded by the call for research projects of the Spanish Association of Deans of Nursing Faculties (CNDE) to Dr Laura Alonso Martínez (grant number PINV_12CNDE23).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.