
Abstract
Healthcare providers employ various strategies to ensure continuous care for patients taking pre-exposure prophylaxis (PrEP) for HIV prevention. However, sustained engagement in care remains challenging, especially among populations at a higher risk of acquiring HIV, such as individuals who engage in high-risk alcohol use or have alcohol dependence. Understanding the provider-level factors—markers of quality care—that positively influence patient engagement remains underexplored. Through a descriptive qualitative approach and thematic analysis of 38 interviews with 14 participants who use PrEP and who screened positive for hazardous or harmful alcohol consumption (AUDIT scores >7), six major themes were constructed that characterize PrEP quality care: (1) Access to Care and Continuity of Treatment, (2) Positive Patient-Provider Relationships, (3) Educational Engagement, (4) Psychosocial Support and Motivation, (5) Financial Accessibility, and (6) Peer Support. Overall, quality care in the context of PrEP is multifaceted, encompassing efficient service provision, positive patient-provider interactions, accessible and well-defined health education, psychosocial reinforcement, affordability, and peer-based support systems. These findings underscore the need for holistic approaches to PrEP care that address logistical, relational, educational, and financial factors to enhance patient experiences and outcomes.
Introduction
Pre-exposure prophylaxis (PrEP) is a highly effective, prescription-based medication that significantly reduces the risk of acquiring Human Immunodeficiency Virus (HIV). While often marketed to populations considered at disproportionate risk for HIV acquisition, particularly Gay, Bisexual, and Other Sexual Minoritized Men (GBSMM), PrEP is an effective prevention strategy for any HIV-negative individual at risk of exposure. According to the Centers for Disease Control and Prevention (CDC) guidelines, all sexually active individuals, regardless of gender, should be screened and informed about PrEP use (Centers for Disease Control and Prevention, 2021).
PrEP is available in two forms: a daily oral pill and a long-acting injectable administered bimonthly or biannually (U.S. Food & Drug Administration, 2021, Gilead Sciences, 2025b). Although long-acting injectable PrEP has demonstrated greater efficacy, uptake remains low due to multiple barriers, including limited awareness, insurance and access issues, fragmented healthcare workflows, and patient mistrust of injectable formulations (Keddem et al., 2024). Therefore, improving oral PrEP adherence and sustained care engagement remains a critical public health priority.
The PrEP care continuum consists of three essential phases: awareness, uptake, and adherence/retention (Nunn et al., 2017). While PrEP usage increased by 17% from 2022 to 2023 in the U.S., (AIDSVu, 2024) adherence remains a significant challenge. Consistent oral PrEP use reduces the risk of HIV transmission by approximately 99% from sexual contact and by at least 74% from injection drug use (Centers for Disease Control and Prevention, 2021). However, its effectiveness is contingent on continued adherence. Regions with higher PrEP usage consistently report lower HIV incidence rates (Sullivan et al., 2024).
Despite its proven efficacy, low adherence and poor retention threaten the success of PrEP programs (Calabrese, 2020). Persistence tends to be short-lived—many users discontinue PrEP within 6 to 12 months (Zhang et al., 2022), with even shorter durations among those most vulnerable to HIV (Laborde et al., 2020). Individuals who misuse alcohol face particular challenges in maintaining PrEP adherence (Watson et al., 2022).
Multiple studies demonstrate that an increase in hazardous alcohol use may lead to a decrease in PrEP adherence (Grov et al., 2019; Okafor et al., 2020; Shuper et al., 2020; Storholm et al., 2017; Strong et al., 2024), thus exacerbating HIV concerns given the high prevalence of alcohol use among PrEP users (Shuper et al., 2020). Alcohol use also correlates with sexual practices that increase the likelihood of HIV exposure, simultaneously increasing the need for PrEP while reducing adherence (Hojilla et al., 2020). Thus, strategies to improve oral PrEP adherence must account for the specific needs of those engaging in hazardous alcohol use. To promote PrEP retention, healthcare providers employ various strategies, including routine follow-up, adherence support, patient tracking, flexible scheduling, and referrals to supportive services (Haberer et al., 2023). These examples, while not universally applied, positively impact PrEP persistence. Regular provider visits facilitate laboratory monitoring, allow for patient engagement, and create opportunities to screen for alcohol or substance use (Arnold et al., 2012; Luehring-Jones et al., 2019). These screenings help identify barriers and bolster motivation for continued PrEP use. Supportive tools, such as adherence counseling, reminders, and educational materials, further help patients stay on track (Marcus et al., 2014). Patient registries and tracking dashboards help identify lapsed users and those who may benefit from PrEP re-initiation (Mayer & Krakower, 2015). Flexible scheduling and streamlined testing enhance care continuity (Centers for Disease Control and Prevention, 2021). Other critical supports include referrals to housing, behavioral health, or substance use services (Centers for Disease Control and Prevention, 2024). Collaborative efforts among health departments, community-based organizations, and clinics are crucial in providing holistic PrEP care (Norton et al., 2013). These partnerships address broader social needs that affect adherence, such as housing insecurity and mental health (Eaton et al., 2015; Mayer et al., 2018).
Underpinning these interventions is a patient-centered approach (Sewell et al., 2021). High-quality PrEP care goes beyond biomedical effectiveness and encompasses respectful, accessible, and affirming environments. Patients benefit from care that aligns with their preferences, including flexible options that reduce the burden of daily adherence (Aaron et al., 2018; Calabrese et al., 2022; Hosek et al., 2017; Sullivan et al., 2019). These strategies, consistent with CDC guidelines, help dismantle barriers to PrEP care (Mayer et al., 2020).
While multiple interventions have demonstrated effectiveness in supporting PrEP uptake and adherence, these are not universally applied across care settings. Moreover, gaps remain in understanding how interventions can be tailored to meet the needs of individuals with intersecting challenges, such as hazardous alcohol use.
Addressing Gaps in Care
Despite robust implementation strategies, gaps remain in adherence and sustained engagement, particularly among individuals facing compounded vulnerabilities, such as stigma, substance use, and systemic barriers (Calabrese, 2020; Edgman-Levitan & Schoenbaum, 2021). PrEP providers are well-positioned to incorporate alcohol screening and intervention into routine care.
Exploring PrEP users’ definitions of quality care and experiences can help uncover patient-prioritized markers of effective service delivery. These insights may diverge from provider-defined metrics and can inform strategies to improve adherence and engagement. Furthermore, alcohol use remains an under-addressed barrier in PrEP care, particularly for those engaging in hazardous drinking (Harris et al., 2025).
This study is situated in Kentucky, a state within the Southern United States, a region accounting for 50% to 53% of new HIV diagnoses but only 39% of PrEP users (AIDSVu, 2024; Siegler et al., 2018). The South has the lowest PrEP-to-Need Ratio (PnR), at 10.0. The delayed adoption of PrEP, limited provider training, limited public health messaging, and systemic barriers such as stigma within healthcare settings, limited Medicaid coverage, shortages of HIV-specialized providers, and transportation challenges common across rural areas of the South shape Kentucky’s low PnR (9.5; AIDSVu, 2024; Sargent et al., 2024; Siegler et al., 2018). Despite Medicaid expansion, coverage gaps, challenged system coordination, and structural factors like poverty and uninsurance continue to hinder PrEP uptake. While the U.S. Preventive Services Task Force (2023) has issued a Grade A recommendation for PrEP, requiring most private insurers to cover it without cost-sharing, implementation gaps and varying Medicaid policies may limit its impact on populations most affected by HIV.
Additionally, Kentucky experiences high rates of alcohol-related harm. Between 2015 and 2019, excessive alcohol-related deaths rose by over 40.2%. About 15.8% of adults report monthly binge drinking (National Center for Drug Abuse Statistics, 2023). In 2010 alone, excessive alcohol use cost Kentucky $3.2 billion (Sacks et al., 2015). Multilevel interventions are urgently needed to bridge these intersecting disparities (Hargreaves et al., 2016).
Lastly, although PrEP is recommended for all sexually active adults at risk for HIV, GBSMM remains the heavily impacted population in the United States (Centers for Disease Control and Prevention, 2021). This population also demonstrates a higher rate of alcohol use (Grov et al., 2019). Therefore, the GBSMM population is well positioned to navigate PrEP care while engaging in hazardous alcohol use, and more information is needed to understand the markers that have retained them in care despite challenges associated with alcohol and PrEP adherence.
Theoretical Sensitizing Concepts and Research Questions
Sensitizing concepts are flexible, background ideas that guide qualitative inquiry by offering a starting point for analysis and interpretation rather than fixed definitions (Blumer, 1969; Bowen, 2020; Padgett, 2016). Originating from Blumer’s Symbolic Interactionism, they emphasize the dynamic and interpretive nature of social life, encouraging researchers to explore how meaning is constructed through interaction, rather than prescribing rigid frameworks, sensitizing concepts direct attention to relevant phenomena, allowing theories to evolve and align with empirical evidence discovered in the field.
Three theoretical frameworks sensitize the design of this qualitative study, informing the development of the research questions. The Health Belief Model conceptualizes PrEP adherence and alcohol misuse as health behaviors influenced by perceived barriers, benefits, and self-efficacy (Rosenstock, 1974). The Patient-Centered Care Model emphasizes quality care grounded in communication, emotional support, and respect for patient preferences (Picker Institute, 2025). The PrEP Care Continuum offers a structural lens through which to examine PrEP-related experiences across awareness, uptake, adherence, and retention (Nunn et al., 2017).
Together, the frameworks offer a holistic and nuanced understanding of engagement in PrEP care, one that is greater than the sum of its parts. The theories highlight distinct but interrelated aspects of the participants’ experiences, including trust, stigma, vulnerability, provider relational dynamics, the navigation of healthcare systems, and PrEP decision making. When synthesized, they illuminate how individuals’ beliefs, interpersonal relationships, and structural factors intersect to shape PrEP engagement. This theoretical synthesis is essential to understanding the lived experiences of our study population and for capturing the complexity of PrEP use in the real world.
A qualitative approach allows exploration of care facilitators and barriers, offering a nuanced understanding of what patients consider high-quality care. These insights are vital for designing inclusive and effective PrEP programs that promote long-term engagement and health equity. Therefore, this study aims to respond to the following research questions:
How do PrEP users who engage in high-risk alcohol use describe markers of quality care and identify factors that enhance adherence and sustained engagement in PrEP services?
How do participants describe the intersection between their awareness of high-risk alcohol use, PrEP use, and experiences with quality care?
Methods
Study Setting and Design
Our research team conducted a descriptive qualitative study (Sandelowski, 2010), which emphasized an in-depth understanding of the “what,” “who,” “where,” and “how” of participants’ experiences of PrEP, alcohol use, and quality care, without imposing strong theoretical interpretation. Qualitative description is not deeply interpretive; rather than framing events within abstract theoretical or philosophical constructs, it presents the facts of a case in clear, everyday language.
This study was conducted as part of a larger randomized controlled trial focused on reducing the risk of alcohol consumption and its associated pathogenic effects on the gut-liver axis in individuals using PrEP. The research was based at three clinics in Louisville, Kentucky, which provide PrEP services: two infectious disease clinics and one internal medicine practice. All procedures were approved by the University of Louisville Institutional Review Board (#22.0606), with written informed consent obtained from all participants.
Study Population
A subset of 38 interview transcripts was analyzed from 14 patients engaged in PrEP care and identified as engaging in hazardous or harmful alcohol use (AUDIT score >7) or possible alcohol dependence (AUDIT score >15) as per the Alcohol Use Disorders Identification Test (AUDIT; Saunders et al., 1993). Other inclusion criteria were aged 18 to 85 years, English or Spanish-speaking, cognitively able to consent, confirmation within electronic medical records of seronegative HIV, Hep B, Hep C status, and actively receiving PrEP care at one of the participating clinics.
Study Procedures
Eligible participants completed a survey and an in-depth qualitative interview (see Supplemental Appendix A for the interview guide), focusing on how alcohol use impacts progression through the PrEP continuum. Interviews took place at the Clinical Trials Unit office between September 2023 and February 2025. Upon screening and confirming eligibility, participants received written study information and had the opportunity to ask questions. Participants chose pseudonyms to maintain confidentiality.
As data collection and analysis continued, follow-up interviews were conducted with all 14 participants to gain a deeper understanding of the markers of quality care for PrEP users. Upon completion of each interview, participants were compensated with a $75 prepaid gift card, and transportation assistance was available through a concierge service.
Quantitative Data Collection
Participant demographics, including age, sex, gender identity, relationship status, education level, race, employment status, household income, and insurance status, were collected. Alcohol use was assessed using the AUDIT, a World Health Organization (WHO)-developed tool to measure alcohol consumption, dependence, and related harm (Saunders et al., 1993). PrEP adherence was evaluated through self-reported questionnaires and confirmed by checking electronic medical records, including providers’ and pharmacy orders. A single-item PrEP adherence question “Thinking about the past 4 weeks, what percent of the time were you able to take all your PrEP medications? Responses should fall between 0% and 100%” (Blumenthal et al, 2019), and a rapid tenofovir Test (SureQuick) was also used to verify adherence.
Qualitative Data Collection
Qualitative data were collected through in-depth interviews focused on experiences with PrEP and alcohol use (Supplemental Appendix A). The interviews were recorded, transcribed, and verified for accuracy. Of the 14 participants, all completed second interview, and 10 completed a third interview. Follow-up interviews focused on clarifying earlier responses, deepening exploration of emergent themes, and member-checking the research team’s preliminary interpretations.
Data Analysis
Descriptive statistics were used to characterize the sample. Following Braun and Clarke’s methodology, thematic analysis was used to analyze the interviews (Braun & Clarke, 2021). This systematic approach identifies and examines themes within qualitative data. The thematic analysis involved six steps: (1) familiarization with the data, (2) initial coding, (3) theme searching, (4) theme revision, (5) theme definition and naming, and (6) report production.
The coding team, comprised of four qualitative researchers (LMH, BDS, NN, and JM), began with (1) familiarization with the data, meaning that each team member read the transcripts in their entirety, listened to all interview recordings, and took notes on markers of quality care. The analytic goal of this step was to become highly familiar with the participants’ stories, content, patterns, and key points. Next, independently, the team (2) generated initial codes, by each research team member, took half of the interview transcripts, and line by line coded sentences, phrases, or ideas with short descriptive codes that described their meaning. This process organized and labeled these data into manageable chunks related to markers of quality care. After generating all the initial codes, the research team held an all-day retreat to (3) construct themes. During this process, the team collectively grouped the initial codes into broader themes, identifying overarching patterns that represented key ideas or repeated meanings related to quality care. At this time, we also engaged in diagramming, demonstrating that each theme encompassed several related codes under a single conceptual umbrella. Next, a smaller team (LMH and BDS) engaged in (4) reviewing themes, a process in which they checked each theme against the data to ensure it accurately reflected the participants’ narratives. Some themes were refined and combined at this stage to provide clarity and coherence. Then the larger team came back together, and engaged in (5) defining and naming each theme, giving a specific meaning, grounded in data and direct quotes from participants, to develop a thematic codebook to move onto Dedoose software for computer-assisted qualitative data analysis (SocioCultural Research Consultants, 2024) for thematic coding of the entire data set. All of the transcripts were then coded using this codebook, with flexibility to adapt and refine codes as needed. Four analysts coded transcripts independently in pairs, followed by team meetings to compare interpretations, resolve discrepancies, and iteratively refine themes. The team wrote memos and met weekly to document the relationships between codes and emerging themes (Charmaz, 2014). Lastly, our research team (6) produced the report, engaging in the process of collectively writing up the study findings, by grounding them in illustrative quotes from participants.
The PrEP Care Continuum was used to interpret the impact of providers in fostering a safe space for patients to navigate, including nuanced situations in which additional barriers may arise. A Patient-Centered Model was used to understand the traits and behaviors of providers that cultivate quality care for PrEP patients. Furthermore, our team worked to identify the factors contributing to negative experiences in PrEP care. The Health Belief Model was employed to understand how providers facilitate patients’ framing of their HIV prevention needs. The final analysis presented themes related to PrEP patients’ perspectives on markers of quality care, identifying factors that enhance adherence and sustained engagement in PrEP services.
Reflexivity and Positionality
Our interdisciplinary research team is composed of social workers, public health professionals, psychologists, physician-scientists, and biomedical researchers united by a shared commitment to health equity, HIV prevention, and community-engaged scholarship. Collectively, our positionalities reflect a spectrum of lived, professional, and academic experiences that shaped how we engaged with and analyzed the data in this study.
As a team, we recognize that our work exists within a global and historical context marked by structural inequities, colonial legacies, and systemic racism that continue to influence HIV prevention and care. We approached the research process with intentional reflexivity, acknowledging our varied identities across race, gender, nationality, and professional roles, and how these shape our assumptions, interpretations, and relationships with communities most impacted by HIV. Our collaboration was guided by principles of humility, reciprocity, and shared learning. We consistently sought to interrogate our own power and privilege within research partnerships, particularly when working across cultural and community boundaries.
Members of our team brought diverse forms of proximity to HIV prevention work and to communities disproportionately affected by HIV. Some members have worked directly in HIV care and prevention programs in the United States, Canada, South Africa, India, Brazil, Peru, Honduras, Vietnam, and Tanzania; others have partnered with community-based organizations, providers, and people with lived experience of PrEP use and HIV. For others, engagement came through long-standing research collaborations or professional practice in adjacent fields such as substance use, behavioral health, or biomedical research in the Southern United States. Together, these experiences grounded our understanding of HIV prevention not merely as a biomedical challenge, but as a deeply social, cultural, and structural issue.
Our team’s methodological training spans constructivist grounded theory, thematic analysis, and community-based participatory research. Senior members of the team, trained in Straussian and constructivist grounded theory under scholars such as Kathy Charmaz and Adele Clarke, guided the analytic process and mentored emerging researchers in qualitative rigor and reflexivity. Junior researchers brought experiential knowledge from direct service, clinical work, and lived community engagement, which enriched our interpretive lens. We collaboratively coded data and engaged in iterative discussions to ensure transparency, trustworthiness, and alignment with participants’ voices and contexts.
The convergence of personal and professional identities shaped our analytic process. Those with clinical and social work backgrounds emphasized relational sensitivity, stigma, and resilience in participants’ narratives; biomedical scientists contributed perspectives on physiological and systemic mechanisms; and public health researchers highlighted structural determinants and inequities. International and cross-cultural team members, bringing experiences from across the globe, brought critical insights into how culture, colonialism, and global power dynamics inform PrEP use and HIV prevention. Multiple team meetings per week created space to discuss and surface our biases, ensuring that our interpretations reflected participants’ lived realities rather than our professional assumptions.
Throughout the study, we viewed reflexivity not as a static declaration but as an ongoing, relational practice inspired by thought leaders such as Charmaz and Clarke. We maintained a dialogic approach to analysis, foregrounding questions such as: Who benefits from this work? Whose voices are amplified or silenced? How do our positionalities shape what we see and what we may overlook? This collective reflexivity deepened our interpretation of the data and strengthened the integrity of our findings.
Ultimately, our positionality as a diverse, reflexive, and equity-driven team informed not only how we analyzed these data but also how we understand our responsibility as researchers to conduct work accountable to the communities most impacted by HIV and to contribute to social change grounded in justice, humility, and care.
Trustworthiness and Rigor
Trustworthiness and rigor were established through methodological transparency, reflexivity, and iterative engagement with the data. The research team pursued a sample that provided a sufficiently diverse range of experiences to address the aims (Braun & Clarke, 2021; Thorne, 2025), and information redundancy was pursued to ensure thematic completeness (Braun & Clarke, 2021; Rahimi, 2024). These aims were supported through situational analysis, positional mapping, and diagramming techniques that deepened understanding of relationships among concepts and contexts (Braun & Clarke, 2021; Charmaz, 2014).
Following the initial 14 interviews, 24 follow-up interviews were conducted to address data gaps and obtain participant feedback on emerging interpretations (Birt et al., 2016). To enhance credibility and confirmability (Lincoln & Guba, 1985), the study triangulated data sources, the team engaged in peer debriefing, and expert review (Lincoln & Guba, 1985). This multi-layered approach integrated participant interviews, peer feedback, and expert validation from providers in PrEP care to strengthen the consistency and dependability of the findings.
Participant feedback during follow-up interviews was particularly valuable for refining both the thematic interpretations and the language used to represent participant experiences. These processes collectively provided multiple perspectives on the data, reinforced the analytic rigor, and ensured that the findings authentically reflected participants’ voices and contexts.
Results
The study sample consisted of 14 male participants with a mean age of 38.1 years. The majority identified as White (71.4%), followed by Black (21.4%), and multiracial or other (7.1%). Most identified as Gay (64.3%), followed by Bisexual (21.4%), Heterosexual (7.1%), and Queer (7.1%). In terms of ethnicity, most participants identified as non-Hispanic (93.3%), with one participant identifying as Hispanic (6.7%). Self-reported PrEP adherence over the past 4 weeks was relatively high, with a mean adherence score of 78.4% (SD = 32.5), and tenofovir was detected in all participants (100%). AUDIT scores indicated that nearly two-thirds (64.3%) of participants may meet criteria for alcohol dependence and roughly one-third (35.7%) have hazardous or harmful alcohol use (35.7%). Demographic descriptors (age, sex, race or ethnicity, sexual orientation) are provided with each quotation to contextualize the speaker (Table 1).
Participants’ Sociodemographic and Behavioral Characteristics (N = 14).

Note. The SureQuick rapid tenofovir adherence test is a lateral flow immunoassay that detects tenofovir (TFV) levels in urine. The test can determine if a patient has taken TFV within the past 48 h. The test results are reported as either detectable or undetectable TFV. A negative test line indicates detectable TFV, whereas a positive test line indicates undetectable TFV. AUDIT = Alcohol Use Disorders Identification Test; PrEP = preexposure prophylaxis.
When discussing markers of PrEP quality care, participants primarily focused on PrEP care, viewing it as their primary healthcare need and often the impetus for their engagement in healthcare services. As displayed in Figure 1, this care was coordinated by multiple providers, including primary healthcare providers, pharmacists, public health practitioners, and infectious disease physicians, and emphasized factors that enhanced adherence and sustained engagement. The analysis results indicate six major themes embedded within participants’ descriptions of quality PrEP care, including (1). Access to Care and Continuity of Treatment, (2). Positive Patient-Provider Relationships, (3). Educational Engagement, (4). Psychosocial Support and Motivation, (5). Financial Accessibility, and (6). Peer Support.

PrEP markers of quality care coordinated by multiple providers.
Continuity of care, financial accessibility, and peer support were identified as particularly crucial in maintaining adherence and addressing alcohol-related concerns. In each of the six major themes, markers of quality care were described by contrasting them with negative experiences with non-PrEP care providers. Overall, participants valued and desired a holistic, stigma-free healthcare experience that integrated PrEP with broader health needs, including alcohol use.
As noted, each of the 14 respondents scored in the moderate to high-risk alcohol use category (AUDIT scores >7), although participants described various patterns of alcohol use and fluctuating consumption. Participants’ narratives often referenced their alcohol use, often specifically how it intersected with their PrEP care and broader health considerations. Like their PrEP use, participants described alcohol consumption as a social norm, frequently playing a central role in social interactions and sexual encounters. In turn, it influenced how they navigated their healthcare needs and experiences, with alcohol functioning as an undercurrent to the themes identified above. Despite their hazardous drinking patterns, participants generally reported that alcohol use was not meaningfully addressed by their providers. However, their narratives indicated their high awareness of the health risks associated with their alcohol consumption, both in the short and long term.
Access to Care and Continuity of Treatment
Many participants highlighted the ease of accessing PrEP services and expressed satisfaction with the continuity of care. They described seamless transitions in care, including smooth insurance handling, timely access to medication, and strong relationships with healthcare providers and pharmacies. For example, patients expressed satisfaction with regular follow-ups, their pharmacies’ efficiency, and their healthcare providers’ proactive engagement, ensuring they did not miss doses. Al (33, Male, Black, Gay) reflected on his PrEP care experiences: “I’m getting medication on time. I’m adhering to it, literally 99.8% of the time on time and daily. My questions are answered. I don’t feel judged or anything going into an appointment.” PrEP users valued their relationships with PrEP providers and acknowledged that their positive experiences were not uniform across all healthcare providers. For instance, Alexander (60, Male, White, Gay) shared, “Well, I was off of it for almost a month. My surgeon took me off it because he didn’t know what it was, which kind of surprised me.”
Thus, patients expressed concerns about the lack of PrEP awareness among healthcare providers, contributing to decreased continuity of care. Additionally, participants noted that having their PrEP inquiries addressed by providers helped to build trust and create a safe space for them as patients.
Patients voiced that some providers were attentive and provided continued care to PrEP users, accounting for other health concerns, such as exposure to other sexually transmitted infections and alcohol dependency. For example, Mark (27, Male, White, Gay) shared, “The pharmacist that I saw for my last appointment did mention going on doxy PEP, so I’m on that now, which is nice.”
Manuel (56, Male, Hispanic, Heterosexual) shared his experience of gradually reducing alcohol due to a discussion with his healthcare provider. He stated, “The doctor that took care of me, he did try to send me to a program, but I told him I didn’t have time. So he just said if I feel bad to just go to him urgently.” Although Manuel was unable to link to treatment at that specific time, the introduction to treatment facilitated by his PrEP provider eventually led to a reduction in alcohol use, thus representing a critical milestone in this healthcare journey.
Positive Patient-Provider Relationships
Consistent positive relationships with healthcare providers were a significant marker of quality care. Many participants emphasized the importance of trust, clear communication, and feeling supported by their providers through measures that promoted safety and destigmatization. Participants spoke about how their primary care provider introduced them to PrEP and continued to guide them through the process, creating a sense of accountability and consistency. For example, Spider (30, Male, Black, Gay) reflected on the ongoing relationship he has with his provider: I think he [provider] is the one that was actually telling me about PrEP initially when I first started when I was dating my last partner who was HIV undetectable. . .I’ve just kind of been taking it, as in then, even my new partner that I’ve been with for almost a year now, having a conversation with him [provider] about why I still take it.
Additionally, patients with long-term relationships with providers noted that positive patient-provider relationships contributed to their adherence to PrEP and overall satisfaction with their care. Malachi (29, Male, Black, Gay) reflected on his relationship with the pharmacy: Luckily, my pharmacy knows who I am because I come a lot of course for a lot of different things. So they’re pretty on top of it whenever they do see me and know which medicines that I need at that time and which medicines I don’t.
Long-term relationships also facilitated easier communication and greater comfort between patients and providers. Spider shared, “Yeah, I’ve been with my PCP for four years, so we talk often, even just on MyChart [patient portal] if I ever have a question or something like that. And so it’s a really good relationship.” Additionally, participants noted that their providers communicated with them in a non-judgmental and stigma-free manner, which contributed to a sense of affirmation and safety, particularly for those accessing PrEP in more public or community-based settings. For example, Eric (32, Male, White, Queer) shared: “I’ve never felt judged. I mean, they’re pharmacists, they’re medical professionals. I am not the scariest thing that they’re going to see. I’ve never felt any judgment or anything.”
Patient-provider relationships were a marker of quality care for PrEP users. They helped foster long-term care and comfort when discussing new medication, leading to PrEP initiation for some patients and promoting long-term adherence. Participants reported consistent communication, reinforcing trust between patients and providers. Eric noted that his PrEP provider is “the longest healthcare provider that I’ve been with,” which fostered support and linkage to care for other ongoing health needs.
Educational Engagement
Another prominent theme was patients’ level of awareness of PrEP, which many attributed primarily to the information and guidance they received from their healthcare providers. Many noted having their health-related questions answered in ways that increased their knowledge and confidence in making PrEP-related decisions. For example, Al (33, Male, Black, Gay) shared: At one point, I switched from Truvada to Descovy and had a bunch of questions answered, and decided to switch back to Truvada. I’ve understood so much more about this level of health and what this drug does. I’ve learned so much more, and everyone’s been able to answer questions.
Nicholas (21, Male, Black, Queer) also shared how provider guidance shaped his understanding of PrEP adherence “I did start to come around to their side because having a clear, strong message and taking it daily is better than the risk that you take on if you are doing prep 2-1-1.”
These examples illustrate how provider education helped participants make informed decisions and fostered confidence in their treatment, whether related to different medications (e.g., Truvada vs. Descovy) or adherence strategies (e.g., daily adherence vs. on-demand PrEP). Access to clear information helped patients become more actively engaged in their healthcare and gain deeper understanding of PrEP.
Psychosocial Support and Motivation
Participants also expressed that the frequent, 3-month medical visits required to be on PrEP provided psychological support and motivation to remain adherent. For example, Chris (33, Male, White, Gay) shared: They’re just amazing. They call me, and I never have to worry about it. I never have to give a second thought about it. I just know that when it’s time, my phone will ring, and they will call me. It works perfectly.
Consistent communication and reminders about PrEP refills motivated participants to adhere to their medication. Several participants described the importance of follow-up visits to maintain accountability for their health. They noted that ongoing check-ins with healthcare providers fostered a routine that promoted physical and mental well-being, and some stated that these visits helped them overcome previous hesitations about engaging with the healthcare system. For example, Al (33, Male, Black, Gay) said, “The safety in knowing that that medication is there to help and the fact that I am having to go follow up with doctors every three months, I feel like it’s a good roadway, road map.” Participants often shared that although the ongoing PrEP appointments were challenging to manage due to their busy schedules, these appointments motivated them to discuss other health-related needs and provided psychosocial support to help them stay adherent.
Financial Accessibility
Patients noted that financial barriers to PrEP and the reliance on providers to overcome clinical barriers to PrEP access were crucial to quality care and to establishing strategies and resources to minimize care disengagement. Some participants faced minor issues related to inadequate insurance or financial barriers. However, they quickly pointed out that their clinics and pharmacies provided workarounds, such as grants and extra short-term supplies, enabling them to maintain adherence to PrEP and ensuring that financial obstacles did not disrupt their treatment. Al (33, Male, Black, Gay) reflected on his experience receiving the grant funds to help with his medical bill: I think the only time I’ve had some issues in paying anything were the doctor visits, sometimes the annual visit. I do know that I got a bill that was a little bit more than what I could pay at that time in 2018, working where I was working, but the clinic was very good in having grant funding to be able to pay for that.
Mark (27, Male, White, Gay) explained a sliding-scale approach used by a non-profit PrEP provider to assist uninsured users: “If you have medical coverage, they take those profits from people who have medical coverage and use it for people who are uninsured.”
Some participants highlighted the provider’s preparedness to address PrEP adherence barriers related to insurance lapse as a marker of quality care. For example, Chris (33, Male, White, Gay) shared that his pharmacy promptly updated his insurance on file. Additionally, some providers prescribed an extra month of supply for their patients to ensure PrEP adherence. Chris shared, When I did have no insurance, that did not stop me from missing any. The little pharmacy I use, they are really good about, they call me every, I don’t know, I guess literally whatever day I can refill, they call me that day. So I always usually have at least about a month ahead. So even when I didn’t have insurance, I’ve never had, I’m sure I still would have been able to get it, it’s free or whatever, but I never was worried that ‘oh my God, I’m going to miss this.
The provider’s preparedness to navigate insurance complications and offer solutions on the spot helped bridge any foreseeable gaps in PrEP care, ensuring adherence and providing hope that care would be uninterrupted. In addition to financial and logistical assistance, participants also described receiving informal encouragement and practical help from peers and friends who shared similar experiences. These informal support systems, though not part of formal PrEP services, played an important role in helping participants remain adherent and engaged in care.
Peer Support
Peer-to-peer interactions and support were also considered important to participants who primarily described informal peer support from friends and community members. For example, participants highlighted that being informed by their social circle or healthcare peers helped them make informed decisions about PrEP use. Some participants shared that peer-to-peer support, characterized by an equal relationship devoid of power dynamics between the patient and provider, may be less intimidating for some PrEP patients. Patients reported that these relationships could also be more desirable due to shared values around using PrEP, such as sex positivity, harm reduction, and destigmatization. Several participants expressed a strong desire for formal peer support models integrated within clinical PrEP services, highlighting an opportunity for implementation.
Joe (48, Male, White, Gay) described peer support for adherence as: It feels more like there would be stigma for not being on PrEP. . .if somebody hears that I’m doing 2-1-1, they’re like, ‘What are you doing? You should be taking this daily.’ It’s kind of the opposite thing where I feel like there’s a positive pressure.
At times, participants described stigma in the community against event-based (2-1-1) dosing, likely due to its lack of U.S. Food and Drug Administration (FDA) approval, despite its evidence-based nature. As a result, prescribing 2-1-1 dosing is considered off-label. It is only recommended in accordance with clinical guidelines for individuals who meet specific criteria: they request non-daily dosing, have sex infrequently (e.g., less often than once a week, and can anticipate sex (or delay sex) to permit the doses at least 2 h prior to sex. To support this evidence-based option for men who have sex with men who prefer it, provider education and community-level destigmatization strategies may be necessary.
Beyond PrEP Adherence, peer support models of care also played a significant role in participants’ efforts to reduce alcohol use. Several participants identified reduced drinking as an important health goal, emphasizing how social dynamics could either support or hinder these efforts. For example, Mateo (37, Male, White, Gay) described how the support of a friend who was also limiting drinking made it easier to make healthier choices: “My friend that I was with was not drinking very much either, and it was easy just to be like, we will have a soda.” Others, such as Eric (32, Male, White, Queer), who had been in and out of treatment for alcohol dependence, emphasized the importance of peer support within treatment experiences. When asked about positive alcohol misuse treatment experiences, he described how peer relationships were the most meaningful and helpful, rather than programs that emphasized top-down models. He explained, “I think that having more peer-to-peer is more helpful than having a manager or sort of lord.” In discussing substance use programs, Eric’s account underscored the intersection of substance use and PrEP care. This theme, though less common, highlights the potential to integrate HIV prevention and substance use services more intentionally, thereby enhancing engagement and overall care experiences in both domains. Additionally, it broadens the concept beyond PrEP adherence alone, illustrating how peer relationships support broader health behavior change.
Lastly, our analysis highlighted an intersection among participants’ awareness of risk, alcohol use, PrEP use, and experiences with quality care, which led to the social processes depicted in Figure 2. Participants described (1) an awareness that their alcohol use contributed to their engagement in high-risk sexual behavior, which increased the risk of HIV exposure. This HIV-risk awareness was an important factor in their motivation to engage in PrEP care. Subsequently, (2) their experiences with quality PrEP care increased their engagement in healthcare more broadly. Participants also shared that (3) their health-risk awareness related to their alcohol use contributed to their broader health concerns, yet remains a largely unassessed health factor, engaged indirectly, if at all, despite strong relationships with PrEP providers.
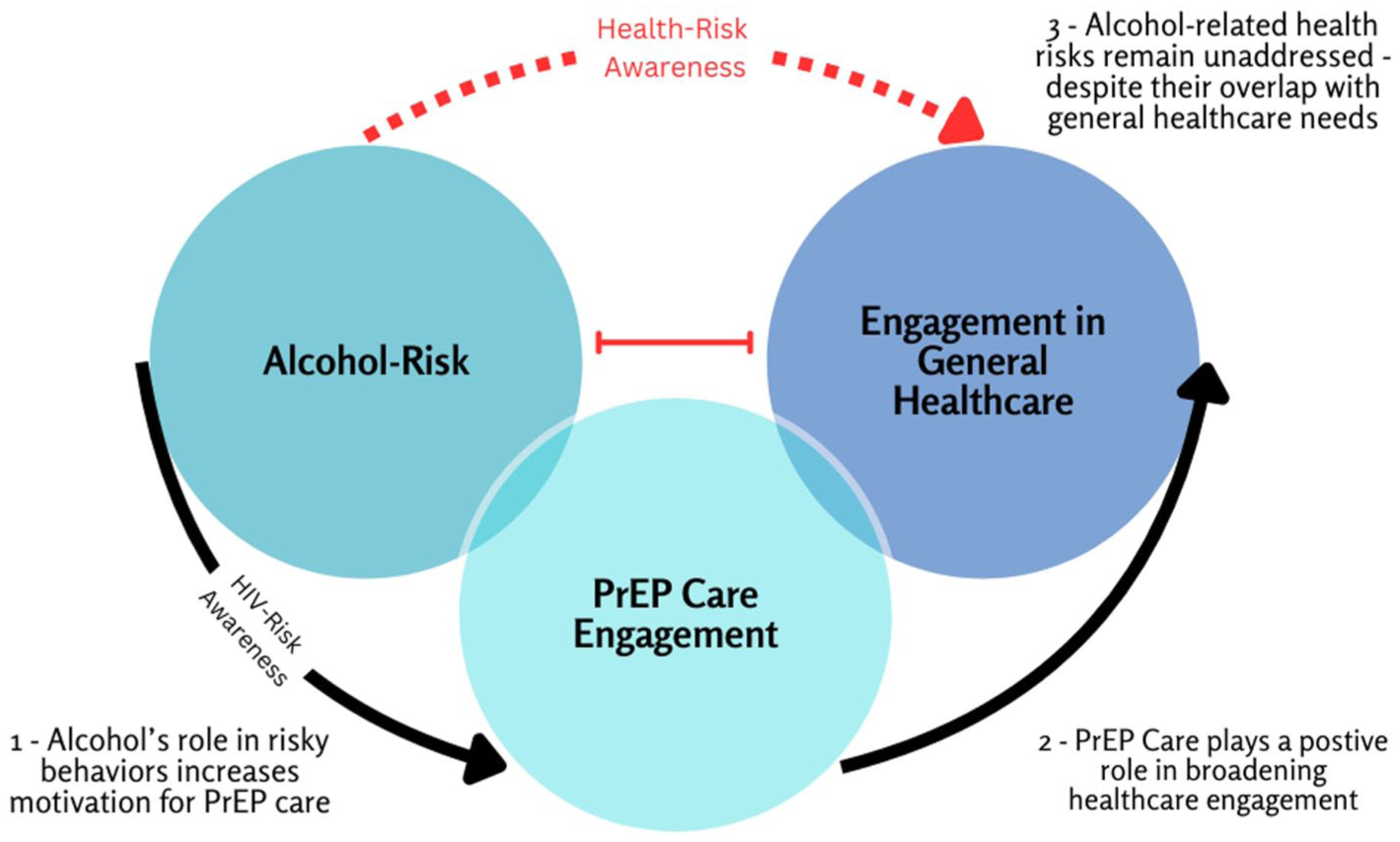
The intersection of awareness of high-risk alcohol use, PrEP use, and experiences with quality care.
Overall, participants conceptualized quality care in the context of PrEP and high-risk alcohol use as including not only efficient and accessible healthcare services but also positive patient-provider relationships, ongoing support, clear communication, and systems that mitigate financial and logistical barriers. The presence of a single provider who provided quality care, such as seamless, transparent, and well-informed care, made a critical difference.
Discussion
This study aimed to understand markers of quality of care for individuals who use PrEP while engaging in alcohol misuse, highlighting the intersection between participants’ awareness of risk, alcohol use, PrEP use, and experiences with quality care. Our findings indicate that participants overwhelmingly reflected on quality care with the PrEP care continuum and conceptualized PrEP quality care as multidimensional, including (a) efficient service provision, (b) affirming patient-provider interactions, (c) accessible and clear health education, (d) psychosocial reinforcement, (e) affordability, and (f) peer-based support systems.
Our findings suggest that providers play a pivotal role in helping PrEP users navigate their engagement in the PrEP care continuum. Research shows that adherence and continued PrEP care are challenging (Calabrese, 2020). However, providers have successfully implemented strategies to retain their patients in care. These strategies include follow-up visits, medication reminders, and timely medication delivery. These strategies support the current literature on PrEP care (Haberer et al., 2023).
Frequent communication between patients and healthcare providers was one of the key factors in delivering quality care. Frequent communication plays a crucial role in PrEP adherence and retention (Laborde et al., 2020). This communication occurs via various platforms, addressing questions and providing additional channels for patients to submit questions (e.g., MyChart). Regular communication and check-ins, whether through appointments, phone calls, or messages, help keep patients accountable and motivated to stay on PrEP. These follow-ups also serve as medication refills and adherence reminders, encouraging patients to remain consistent (Wang et al., 2025). Furthermore, our findings on frequent communication align with recommendations to engage patients in ongoing conversations about PrEP, including its benefits, potential side effects, and adherence strategies (Laborde et al., 2020). By ensuring patients understand how PrEP works and addressing their concerns or misconceptions, providers empower them to make informed decisions and remain committed to their medication regimen.
Additionally, financial support was a key quality marker of care. These findings support financial barriers as one of the most cited factors that impact PrEP adherence and retention (Srikanth et al., 2022). Providers proactively navigated insurance issues and financial obstacles to ensure uninterrupted access to PrEP. This included assisting patients with grant applications, providing temporary supplies when insurance coverage lapses, and managing co-payments and prescription coverage (Buchbinder & Liu, 2019; Sullivan et al., 2019). For providers to assist patients in navigating financial barriers, they may link patients to resources and cost-sharing PrEP programs, such as the Gilead Advancing Access program (Gilead Sciences, 2025a). The financial resources provided by healthcare providers enhance the value of the patient-centered model of care, which emphasizes addressing patients’ needs and promoting continued access to care (Picker Institute, 2025).
Our results indicate that patients value and desire holistic care that addresses mental health. Patients desired providers to offer psychosocial support by helping them overcome adherence-related emotional or mental health barriers. Studies on effective interventions have shown that counseling, encouragement, and support for developing daily routines or habits to integrate PrEP into one’s life improve adherence and engagement in clinical care (Marcus et al., 2014). Psychosocial reinforcement is closely tied to motivation-enhancing interventions and to the support healthcare providers provide.
Our findings indicate that PrEP care retention is more effective in coordinated care, a core principle of patient-centered care. Participants reported relying on primary care providers and pharmacists to access their medication. These findings can potentially address the purview paradox—the conflicting beliefs in healthcare on which providers should screen and prescribe PrEP (Jackson et al., 2024; Pleuhs et al., 2020). Participants identified primary care, infectious disease clinics, specialty STI clinics, and pharmacies as their focal points for PrEP providers and care. These findings underscore the importance of providers facilitating ongoing engagement, as participants valued seamless service delivery from multiple providers.
As shown in our results, when providers are uninformed about PrEP, patients are uncomfortable and disappointed during provider education, and these encounters risk weakening patient-provider trust. Additionally, the impact of coordinated care emphasizes the importance of community-based pharmacies in PrEP delivery. Therefore, future efforts should continue to advocate for more states to pass legislation that permits pharmacists to use PrEP supplies, such as the California State Senate Bill 159 (Jackson et al., 2024). Authorizing pharmacists to furnish PrEP and PEP (post-exposure prophylaxis), while removing insurance preauthorization requirements that make accessing the medication more cumbersome for patients seeking to receive it. Ultimately, participants value all settings that facilitate engagement in care.
Strong patient-provider relationships facilitated continued engagement in care. These results are reinforced by the existing literature, which describes providers’ supportive, nonjudgmental approach as helpful in reducing stigma and fostering trust, making patients more comfortable in openly discussing adherence barriers or challenges. This transparency allows providers to address concerns more effectively (Calabrese, 2020; Dubov et al., 2018). More broadly, the results demonstrated that these positive relationships had a cascading effect on participants’ overall healthcare. The strength of their personal relationships with providers played a vital role in supporting PrEP adherence and persistence, reducing barriers to access, fostering trust in healthcare services, and facilitating referrals to a wide range of other medical services.
Our findings demonstrate that providers play an instrumental role in helping patients advance through the PrEP care continuum. Providers are essential to patients’ awareness of PrEP; they introduced the medication and created safe learning spaces. In terms of uptake, communication was the central factor that facilitated engagement in this phase, including the decision-making regarding PrEP type. The adherence and retention phase is influenced by the provider’s awareness and ability to anticipate barriers to care engagement and to offer alternatives (e.g., PrEP on demand, linking patients to financial support resources). These attributes also aligned with the patient-centered model, which is grounded in respect, prioritizing patients’ needs, and communication. The recommendations and education on 2-1-1 PrEP demonstrate providers’ flexibility and willingness to adjust PrEP adherence conversations based on patients’ needs. Lastly, respect was critical for creating long-term relationships and dismantling power hierarchies between patients and providers, thereby enhancing safety and openness on both sides.
Our findings also explain how PrEP providers help to enhance patients’ ability to assess their risk of HIV and PrEP decision-making (e.g., switching from Truvada to Descovy or self-perceived risks). Following the Health Belief Model, communication, education, and psychological support allowed providers to offer support that enabled patients’ critical assessment of their perceived risks to HIV and the benefits of PrEP adherence. In addition, providers minimized barriers to PrEP adherence, ultimately empowering patients to engage in PrEP care.
Given the strong, trust-based relationships that many PrEP providers have already established with their patients, there is a clear opportunity to intentionally leverage these bonds to improve care for PrEP users, such as addressing alcohol misuse among patients. For example, one participant mentioned that his provider recommended that he reduce the number of drinks he was consuming weekly and referred him to a treatment program. Through addressing alcohol misuse, providers can disseminate substance misuse screening, engagement, and support. Our study indicates that PrEP providers are uniquely positioned to offer critical care to PrEP users who engage in alcohol misuse.
Building on the existing trust, providers can directly engage patients on their alcohol misuse by offering harm reduction interventions such as Screening, Brief Intervention, Referral to Treatment (SBIRT), and Motivational Interviewing (MI; Pérula-Jiménez et al., 2024). These strategies provide a starting point to address alcohol misuse in a way that patients will respond to, highlighting their preference for close provider relationships, holistic and ongoing support, clear communication, and nonjudgmental, destigmatized care.
By design, the brief intervention (BI) phase of SBIRT leverages existing health risks, providing a context for providers to address health concerns more holistically and inviting patients to connect the dots between other health concerns and alcohol use (Babor et al., 2007). While some PrEP providers may worry about jeopardizing the nonjudgmental, destigmatized approach that is central to care, research supports that these strong relationships and patient-centered care are essential for effective substance misuse support. Furthermore, these findings underscore the value of interventions like SBIRT, which is designed to screen for substance misuse universally, provide brief interventions for those with risky behavior, and offer referrals to treatment when needed.
SBIRT’s methods, rooted in MI, align with the nonjudgmental, patient-centered approach that is crucial to PrEP care. This model provides PrEP providers with a structured approach to address an unmet need—adequate substance misuse screening and intervention—while maintaining the positive, supportive relationships that are key to quality PrEP care (Barata et al., 2017).
We recommend developing policies and practices acknowledging PrEP providers’ unique position to enhance patient-centered care. This would ensure that PrEP users receive not only HIV prevention services but also support in other areas of their healthcare needs. By capitalizing on this potential, PrEP providers can play a more proactive role in addressing broader health issues, ultimately strengthening the overall impact of PrEP care and improving health outcomes for users.
To foster ongoing care, providers should incorporate a more formalized peer support model into the PrEP care continuum. Peer navigator programs have garnered attention in PrEP care and can lead to increased engagement in care (Pichon et al., 2022). Peers should receive training in PrEP care, demonstrate a high level of knowledge about PrEP, and refrain from spreading misinformation (Garett & Young, 2022). When referring patients within a minoritized population like GBSMM, peers must be well-integrated into the LGBTQ+ community to increase credibility and trustworthiness (Jaramillo et al., 2025). Therefore, providers can connect patients with peer navigators, PrEP support groups, or community resources to enhance motivation and adherence when appropriate. Peer experiences often provide a relatable source of encouragement and practical tips for managing daily adherence (Dolezal et al., 2015; Dombrowski et al., 2015).
Patients also noted a distinction between what they considered quality care among various providers within the PrEP Care Continuum. For example, patients valued timely medication delivery from their pharmacist and their PCP’s holistic engagement in addressing their health. These findings underscore the need for and value of provider care coordination. Each provider role contributed to the patients’ overall experience. Noting that PrEP care providers, regardless of role, seemed to align with them in ways other providers do not. Future research should work with individuals who experience marginalization or stigmatization in developing person-centered approaches among healthcare providers, particularly when providers conceptualize healthcare needs as a human rights issue. Examining the influence of providers’ personal values or beliefs, identities, or encounters with others’ experiences of discrimination could yield valuable insights. These factors may create an inclination for providers to align themselves with patient needs, adopting compassionate, patient-centered care strategies.
Limitations and Future Research
The use of follow-up interviews with most participants enabled the research team to revisit topics of patient markers of quality care concerning PrEP and alcohol use multiple times. However, this approach has several limitations. First, while all participants engaged in two or three interviews, the relatively short intervals between data collection may have constrained the ability to document longer-term patterns or effects related to PrEP adherence and alcohol use. Future longitudinal research could address this gap by examining whether changes in alcohol use behaviors and patient markers of quality care change over extended follow-up periods, potentially offering richer insights into their impact on sustained PrEP adherence.
Although this study focused on the PrEP users who engaged in hazardous or harmful alcohol use, participants reported relatively high PrEP adherence. This limits the extent to which the finding reflects the broader and more diverse PrEP users for whom the alcohol use may pose challenges to adherence. In the meantime, education and destigmatization of 2-1-1 PrEP remains critical among providers to share with GBSMM patients who have adherence challenges. This strategy will allow providers to promote engagement in HIV prevention with respect to complex PrEP needs and fluidity of adherence barriers among patients.
Another limitation to consider is that the sample was predominantly White. The study sample included only a small number of Black participants and one Hispanic participant, resulting in limited racial and ethnic diversity. Future research should include more perspectives from Black and Latino men to confirm and expand these findings, particularly given the well-documented racial disparities in HIV outcomes. Additionally, all participants were males and reported positive perceptions of PrEP, which may not represent the full diversity of experiences among PrEP users. Patients may be more likely to perceive their care as high quality if they remained in care throughout our study period. This limitation may influence the interpretation of patient markers of quality care, as the study did not represent individuals with negative perceptions or lower adherence rates. Future studies should aim to incorporate a broader range of participants, including those with negative experiences or lower adherence, to better understand the complexities of markers of quality care and alcohol use across varying levels of PrEP engagement.
Conclusion
Our findings indicate that healthcare providers are instrumental in helping patients navigate their PrEP care use and should remain attuned and attentive to windows of potential needed care for alcohol misuse. Some providers may benefit from continued PrEP education to ensure patients do not discontinue PrEP use while engaging in high-risk alcohol use. By embracing patient-identified markers of quality PrEP care, providers can address various adherence challenges, including alcohol misuse, financial constraints, stigma, and emotional or mental health obstacles, to support patients in maintaining consistent PrEP use. The quality care markers embedded within the PrEP care continuum suggest that PrEP providers are uniquely positioned to foster improved, destigmatized relationships between PrEP users and the broader healthcare system, thus being well-positioned to address hazardous alcohol use. Trusted connections facilitate greater access to healthcare and establish links to a wide range of additional services, including treatment for alcohol use disorders.
Furthermore, the study underscores the potential for PrEP providers to adopt a more integrated approach to patient care. By incorporating routine screening and focused interventions, such as standardized protocols for addressing alcohol misuse, providers can further enhance their role in promoting overall health. Emphasizing coordinated care that includes non-PrEP providers and formalized peer support mechanisms may also strengthen patient engagement, retention, and self-efficacy.
We conclude that future PrEP educational efforts should highlight the positive role of providers in PrEP care to foster morale. Future research should explore how integrated care models affect PrEP adherence and overall health outcomes over time, especially in communities with high HIV incidence. Examining provider-level barriers and facilitators, including the adoption of digital health tools and telemedicine, will be critical for informing policy and clinical practices. Ultimately, a more holistic and coordinated approach to care can help keep patients engaged in the PrEP continuum and reduce alcohol misuse, thus improving treatment outcomes.
Supplemental Material
sj-pdf-1-gqn-10.1177_23333936261429417 – Supplemental material for Markers of Quality Care in PrEP Services: Qualitatively Exploring Dimensions of Support Among Persons Who Engage in High-Risk Alcohol Use
Supplemental material, sj-pdf-1-gqn-10.1177_23333936261429417 for Markers of Quality Care in PrEP Services: Qualitatively Exploring Dimensions of Support Among Persons Who Engage in High-Risk Alcohol Use by Nqobile Nzama, Lesley M. Harris, Blake D. Skidmore, Juma S. Mwenda, Jelani C. Kerr, Martin T. Hall, Sadaf Sedaghatshoar, Andrea Reyes-Vega, Harideep Samanapally, Anupama Raghuram, Smita Ghare and Shirish Barve in Global Qualitative Nursing Research
Footnotes
Ethical Considerations
This study was approved by the University of Louisville Institutional Review Board (#22.0606). Each participant provided written consent.
Author Contributions
Medical Journal Editors (ICMJE); all authors have contributed to the conception and design of the study, drafted or have been involved in reviewing this manuscript, reviewed the final version of this manuscript before submission, and agree to be accountable for all aspects of the work. Specifically, using the CRediT taxonomy, the contributions of each author are as follows: Conceptualization and Methodology: L. M. Harris, J. C. Kerr, M. T. Hall, S. Ghare, S. Barve; Formal Analysis: N. Nzama, L.M. Harris, B. D. Skidmore, and J. S. Mwenda; Funding acquisition: L.M. Harris, J.C. Kerr, M.T. Hall, S. Ghare, S. Barve, Project administration: L. M. Harris, J. C. Kerr, S. Barve, A. Reyes-Vega, R. Anupama; Supervision: L. M. Harris, J. C. Kerr, A. Reyes-Vega, H. Samanapally, S. Barve, R. Anupama; Validation: L. M. Harris, A. Reyes-Vega, Samanapally, R. Anupama, S. Barve. Writing—original draft: N. Nzama, L. M. Harris, B. D. Skidmore, J. C. Kerr, M. T. Hall, J.S. Mwenda, S. Sedaghatshoar. Writing/Revising: N. Nzama, B. D. Skidmore, L. M. Harris, J. C. Kerr, M. T. Hall, S. Ghare, R. Anupama.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the National Institute on Alcohol Abuse and Alcoholism (NIAAA), 1R01AA030485.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.