
Abstract
Mental health and substance use (MHSU) disorders are the primary contributors to disability among children and youth, often with an early age of onset. Rural communities face added challenges in accessing care. Nurses may be a key professional support for rural children and youth needing MHSU care, but there is a gap in the literature about nurses’ roles in this practice area. This interpretive descriptive study explored the insights of rural nurses regarding MHSU care for children and youth in community practice settings in British Columbia, Canada. Semi-structured interviews were conducted with eleven rural nurses who were either MHSU specialists or generalists with MHSU as part of their practice. Reflexive thematic analysis and interpretive description were used to analyse the data. Three key themes were constructed: (1) children and youth’s mental health was tethered to the rural and remote context; (2) MHSU care was more than just MHSU treatment; and (3) the essential components of rural child and youth MHSU nursing practice. Early intervention and rural-centric approaches may support rural children and youth. By supporting rural nurses, MHSU care for children and youth can be enhanced.
Introduction
Worldwide, mental health and substance use (MHSU) disorders are the primary contributors to disability among children and youth (Erskine et al., 2015) and typically have an early age of onset: 34.6% of youth with a mental health challenge experience it by age 14, 48.4% by age 18, and 62.5% by age 25 (Solmi et al., 2022). Moreover, children and youth with MHSU challenges are at an increased risk of suicide (Ackerman & Horowitz, 2022), chronic MHSU conditions (Malla et al., 2018; Wiens et al., 2020), homelessness, incarceration, and exploitation (Miller, 2009). Compounding these high rates, early onset, and adverse outcomes of MHSU challenges, children and youth living in rural areas face multiple barriers, such as long waitlists, stigma (Centre for Addiction and Mental Health, 2019), financial insecurity, fragmented care (Moroz et al., 2020), extensive travel (Sinclair, 2020), and a lack of youth-friendly MHSU services (Hawke et al., 2019) or a lack of services in general (Canadian Institute for Health Information, 2019). Rural and remote communities are defined here as geographically isolated, poorly resourced, and/or with smaller populations (Canadian Association for Rural and Remote Nursing [CARRN], 2020). Globally, rural communities often lack adequate MHSU supports and services (Thomas et al., 2024), including harm reduction resources. This is especially concerning given that people living in the rural contexts who use substances may face higher rates of toxic drug poisonings (i.e., drug overdoses) (Dunn et al., 2016) or death from toxic drug poisonings (Hu et al., 2022) – the leading cause of death in young people aged 10 to 18 years in British Columbia, Canada (British Columbia Coroners Service, 2023).
Comprehensive and timely support may prevent adverse outcomes related to untreated MHSU challenges in children and youth (McGorry & Mei, 2018). To address the inequitable barriers to care in rural regions, community health nurses (CHNs) may play a role in supporting child and youth MHSU care (McAllister, 2019). CHNs provide care in diverse community-based practice settings, supporting the health of individuals and communities across the continuum of health promotion to illness prevention and palliation (Community Health Nurses of Canada [CHNC], 2019). Given their trusted position and integration within the community, rural CHNs (hereto referred to as rural nurses) may play a crucial role in providing healthcare to children and youth. However, there is limited understanding of their provision of MHSU care in community settings; the research identified focuses on school nursing and does not include other settings such as primary care clinics or outpost nursing stations (Burch & Stoeckel, 2021; Pattison-Sharp et al., 2017; Ratter, 2023). This gap limits understanding of the contextual realities of rural nursing practice and constrains the development of targeted supports, policies, and services that reflect the needs of rural children and youth.
Research Aim
The purpose of this study was to better understand the practice of rural nurses’ child and youth MHSU care in community settings by describing rural nurses’ perspectives related to delivering child and youth MHSU care, with particular attention to how rural context, community resources, and systemic factors influence their practice. Thus, this research project aimed to answer the question: What are nurses’ perspectives about how rural context, community resources, and systemic factors influence their practice when delivering child and youth MHSU care in community settings?
Methods
Theoretical Framework
The CHNC Standards (CHNC, 2019) (i.e., the Standards) and the Knowing the Rural Community: A Framework for Nursing Practice in Rural and Remote Canada (CARRN, 2020; Pavloff et al., 2022) (i.e., the Framework) comprised the guiding theoretical framework for this study, rooted in the nursing practice principles of accessibility, client participation, health promotion, appropriate skills and technology, and intersectoral cooperation. Both advocate for equitable, holistic, and person-centred care nested within the community context, with an emphasis on the health of all people (CARRN, 2020; CHNC, 2019). The Standards uniquely contribute harm reduction considerations and a focus on community practice settings (CHNC, 2019), while the Framework extends to all nursing practice settings with a specific focus on the rural context (CARRN, 2020). Together, they provided a comprehensive scaffold for understanding rural community health nursing regarding child and youth MHSU care. Moreover, this composite theoretical framework aligned well with this study’s interpretive description methodology (Thorne, 2016), emphasizing context, collaboration, person-centred, pragmatic, and socially just care, all developed from and for the nursing profession, informed by nursing theory and knowledge (CARRN, 2020; CHNC, 2019; Thorne, 2016).
Interpretive Description Methodology
This study used an interpretive description methodology, an applied qualitative research design meant to address practice-specific knowledge gaps or queries (Thorne, 2016; Thorne et al., 2004). Interpretive description was originally developed from naturalistic inquiry, ethnography, grounded theory, and phenomenology, while adapting these traditions to the applied purposes of nursing. In this study, we drew from phenomenology to elicit how nurses’ lived experiences could be applied to the practice-oriented aims of the nursing discipline. This theoretically flexible and context-attuned methodology (Thorne, 2016) was optimal to answer the research question; by exploring what can be learned from the qualitative experiences of rural nurses regarding child and youth MHSU community care, their practice insights could be transformed into practical, clinically relevant knowledge for the rural practice setting.
Reflexivity and Positionality
This study was conducted by a team of four researchers whose diverse professional and personal backgrounds informed the research process. ST led the data collection and analysis, bringing perspectives drawn from their experiences as a child and youth, and later as a community health nurse, in rural communities, as well as their identity as a queer, gender-diverse, white settler. EK supervised all aspects of the study; her contributions were shaped by her professional nursing experiences in an urban setting as a community health nurse who worked with children and families in well-child clinics and schools. EK’s identity as a cisgender white mother also informed her assumptions and perspectives about child and youth MHSU community care. NDO provided input at all stages of the study, particularly in analysis and interpretation. NDO identifies as a cisgender woman, as a nurse, and academic with expertise and experience in rural and remote health. DJ, a white cisgender man, has 25 years of experience within a health authority serving a large rural population. He works as a nurse in mental health and relational practice, and his ongoing efforts to build relationships with local Indigenous nations to improve culturally safe care further shaped his contributions. Collectively, the research team’s positionalities influenced assumptions about the importance of understanding and supporting community health nurses who provide MHSU care to children and youth in rural contexts, while reflexive practice helped ensure that interpretations remained grounded in participants’ accounts.
Participants and Procedures
Participants and Recruitment
The study was conducted virtually, with participants located in British Columbia, Canada. Individuals were eligible to participate if they were a regulated or licensed nurse (i.e., Licensed Practical Nurses (LPNs), Nurse Practitioners (NPs), Registered Nurses (RNs), and Registered Psychiatric Nurses (RPNs)) and worked in rural British Columbia with children and youth in community settings. Given the absence of a universally accepted definition of ‘rural’, we did not impose strict inclusion criteria. Instead, nurses were able to self-identify whether they worked in rural or remote contexts. This approach ensured that the study captured nurses’ own understandings and experiences of rural practice, which were then situated within the study context. To capture a range of care experiences, the study sought to include all nurse types (LPNs, NPs, RNs, and RPNs) and nurses providing both specialized and generalist MHSU care. Demographic information such as age, sex, or gender identity was not collected as part of this study, and therefore the sample cannot be characterized in these terms. Three participants were known as previous professional acquaintances during ST’s prior clinical experience in rural health; however, there were no ongoing, supervisory, or dependent relationships between participants and researchers. Participants were recruited using purposive and snowball sampling. Recruitment materials were distributed via professional networks, social media channels, email distribution lists, and nursing groups. Potential participants completed a Qualtrics survey assessing eligibility and provided online consent, which included details on the researcher’s identities, study’s purpose and rationale, use of study data as ST’s Master’s thesis, protocol, and participant rights. Eligible participants were contact by ST, and verbal consent was confirmed prior to the interview. Participants were informed of a $40 e-gift card honorarium both in the recruitment poster and at the end of the interviews, and participants who consented to receive the honorarium were emailed the gift card shortly after the interview was completed. While honoraria may influence participation or responses, we framed this incentive solely as recognition for time, rather than as a motivator for particular responses. Following the interview, participants were invited to refer others in their network who might be interested in the study. If they agreed, they received an email with recruitment information as part of a snowball sampling approach.
Sample Size
In interpretive descriptive studies, sample sizes typically range from 5 to 30 participants, contingent upon the research focus and rationale provided by the researchers (Thorne, 2016). For under-studied topics like rural child and youth MHSU nursing in community practice settings, a smaller sample size of approximately 10 to 15 participants was anticipated to yield meaningful, practice-useful data. Although this smaller sample size would not capture the full variation and inherent complexity (Thorne, 2013) of rural child and youth MHSU nursing, this limitation was accounted for using the concept of information power (Malterud et al., 2016). Information power specifies that a smaller sample size can be used when there is adequately rich data relevant to the study’s purpose, and considers factors such as study aim, sample specificity, theory use, dialogue quality, and analysis strategy (Malterud et al., 2016). The specific aim and sample of this study allowed for a narrow focus, while the use of a composite theoretical background (i.e., the Standards (CHNC, 2019) and the Framework (CARRN, 2020)) grounded this study in rural community health nursing. Efforts to promote high-quality dialogue and analyse the data in depth (i.e., by using reflexive thematic analysis (Braun & Clarke, 2020) and interpretive description (Thorne, 2016)) further supported the adequacy of the sample size, ensuring sufficient depth and richness of data to reach information power (Malterud et al., 2016).
Data Collection and Analysis
Data collection and analysis occurred concurrently so that both processes were iteratively enriched by the other (Thorne, 2016). Data were collected through a single semi-structured interview with each participant, ranging from 23 to 91 min, with an average duration of 55 min. Interviews were conducted virtually using the University of British Columbia’s (UBC) approved videoconference platform (Zoom) and were audio-recorded to capture participants’ narratives comprehensively. No pilot interview was conducted; however, the semi-structured interview guide (Supplemental File 1) was reviewed by NDO, EK, DJ, and a Canadian nurse leader in rural health for clarity and relevance prior to use. The interview guide, developed from the Framework (Pavloff et al., 2022) and the Standards (CHNC, 2019), prompted participants to provide descriptive accounts of their experiences supporting child and youth MHSU care in rural community settings. These descriptive accounts were used as an entry point to explore how community, rural context, and broader societal factors shaped their nursing practice. ST conducted and transcribed the interviews and wrote field notes during and after the interviews. Only the participant and researcher were present. NVivo 14 was used to code and organize the data.
Coding and theme development were collaborative. ST led the initial coding, which was iteratively reviewed and refined with EK, and further discussed with other senior research team members (NDO, DJ). This process enhanced analytic credibility by ensuring that themes reflected shared interpretation rather than individual bias. Consistent with interpretive description, participants were not asked to review themes or findings, as the analytic responsibility rests with the researchers to develop contextually relevant interpretations (Thorne, 2016).
We used reflexive thematic analysis from a constructionist philosophy (Braun & Clarke, 2021) to analyse interview data, exploring what can be learned from CHN experiences of providing MHSU care to children and youth. The six phases of reflexive thematic analysis guided the analysis, with the understanding that these phases are meant to support the process rather than be rigidly followed. These phases included (a) data familiarisation; (b) systematic data coding; (c) constructing initial themes; (d) developing and reviewing themes; (e) refining, defining, and naming themes; and (f) writing the report/manuscript (Braun & Clarke, 2020). In addition to the six reflexive thematic analysis phases, themes were reviewed for clinical applicability, asking ‘so what?’ when thinking about the data in relation to rural clinical nursing practice (Thorne, 2016).
Reflexive thematic analysis (Braun & Clarke, 2020) and interpretive description (Thorne, 2016) both supported data analysis. Reflexive thematic analysis offered specific guidance on analysis methods while interpretive description provided the overall analytical aim of clinical applicability. The philosophies of reflexive thematic analysis and interpretive description are compatible. Both approaches emphasize researcher positionality, theoretical flexibility, the importance of context, and the use of theory. Further, both highlight the importance of data familiarization (Braun & Clarke, 2019; Thorne et al., 2004). While the interviews began with descriptive questions, interpretive description acknowledges that rich description is often the foundation from which higher-level interpretation is constructed (Thorne, 2016). Accordingly, our analysis moved beyond surface description toward identifying patterns, relationships, and implications for rural nursing practice.
Quality and Rigour
Thorne’s (2016) measures of quality were used to promote study quality and rigor. Epistemological integrity was maintained by aligning the study’s design with a constructivist approach, ensuring that the research methodology was in harmony with this philosophical foundation. Representative credibility was achieved through maximal variation by interviewing nurses who provided specific MHSU care and generalist care. Moreover, this study strove for analytic logic through the research report and audit trail, enhancing the trustworthiness of the findings. Further, interpretive authority involved transparent reflexivity, facilitated by using memos and field notes by ST, and subsequent discussion with the senior research team of interpreting the findings. In addition, this study also accounted for the elements of applied researcher accountability, including attention to moral defensibility, disciplinary relevance, pragmatic obligation, contextual awareness, and probable truth (Thorne, 2016). The researchers understood the potential impact of research findings on practice and situated the findings in the nursing discipline and the contemporary context of specific rural Canadian communities. By adhering to Thorne’s (2016) principles throughout the research process, ethical considerations were thoroughly integrated at every stage of the process. Ethical approval was granted by the UBC’s Behavioural Research Ethics Board (ID # H23-00823). To protect participant confidentiality, we removed all identifying details or replaced them with generic terms in transcripts, assigned pseudonyms, and carefully screened all quotations to ensure participants or communities could not be recognized.
Results
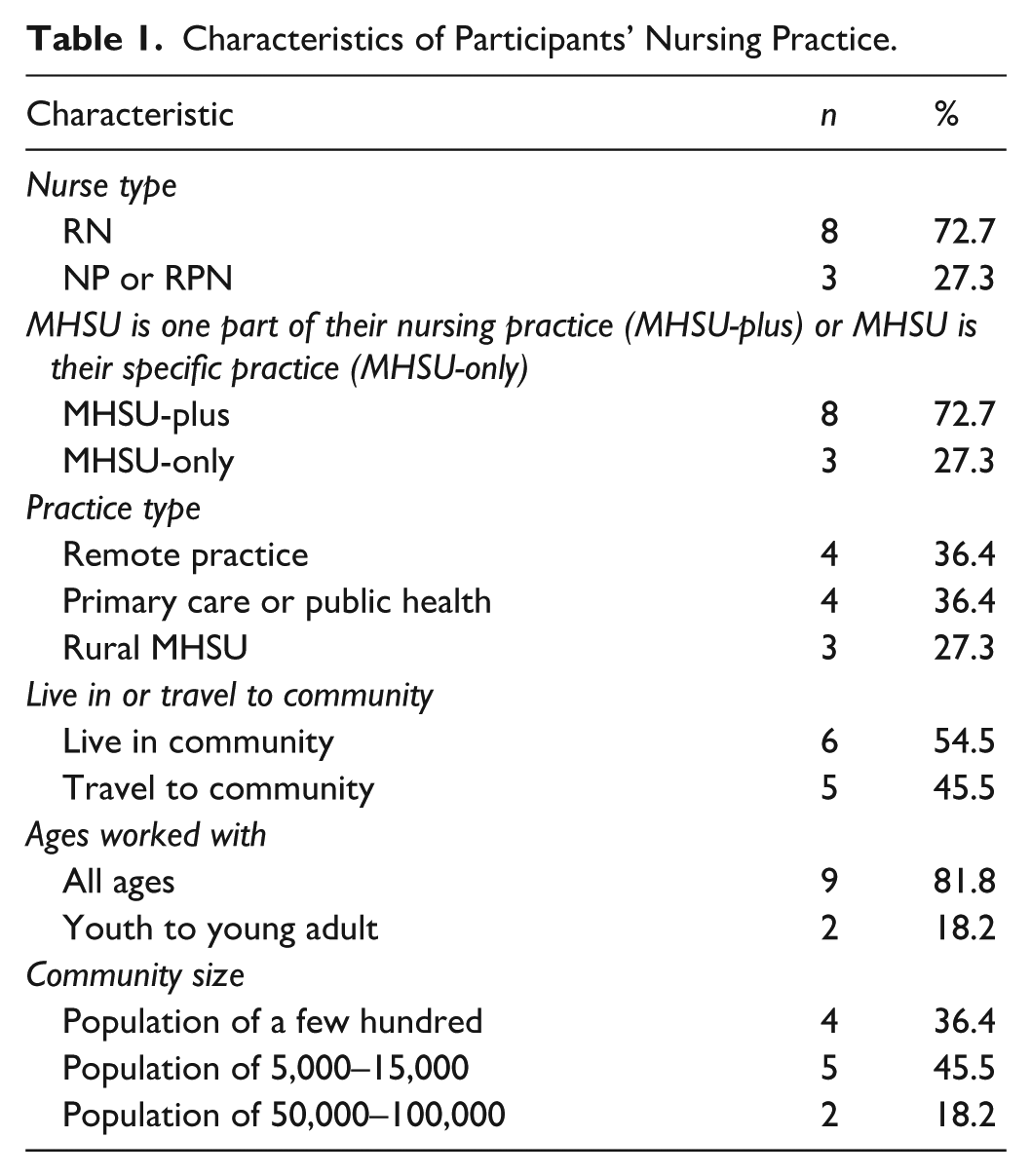
Eleven participants were interviewed, including RNs (n = 8) and NPs or RPNs (n = 3) (Table 1). No participants dropped out of the study; three additional potential participants had initially expressed interest in participating but did not respond to scheduling requests. Nurses worked in settings with a range of population sizes, including larger centres that served wide geographical catchment areas. Even when based in larger communities, these nurses provided care to surrounding rural and remote populations. All settings included core rural features such as resource deficits, transportation challenges, and geographical distance from major centres (CARRN, 2020).
Characteristics of Participants’ Nursing Practice.
Three themes were developed based on the researchers’ interpretation of the descriptive data, which reflected the nurses’ perspectives and practice experiences: (1) children and youth’s mental health was tethered to the rural and remote context; (2) MHSU care was more than just MHSU treatment; and (3) the essential components of rural child and youth MHSU nursing practice.
Theme 1: Children and Youth’s Mental Health Was Tethered to the Rural and Remote Context
Participants described how rural and remote contexts were important to the wellbeing of all rural people. However, since children and youth tend to have less agency than adults, this decreased autonomy uniquely tethered the youth’s mental health to the rural community. Rural children and youth can be particularly affected by (a) everybody knowing everyone; (b) peer, family, and community norms or standards; (c) navigating the (un)available resources; and (d) the need to leave the community to grow. Together, these sub-themes illustrate the complex dynamics within rural contexts – between connection and stigma, opportunity and limitation – that shaped children and youths’ experiences of MHSU.
Sub-Theme 1a: Everybody Knowing Everyone
Rural nurses repeatedly talked about how everybody knows everyone and is affected by whatever happens in the community, especially in smaller or more remote communities. Familiarity among community members could pose particular challenges for children and youth seeking privacy in their healthcare. There may be fewer confidential places that youth can go for MHSU support, more limits around confidentiality, and a greater chance that they (or their families) are related or connected to the providers they have access to. While this sense of community can cultivate feelings of belonging, it can also compound difficulties for youth if there is MHSU stigma. Such stigma can exacerbate the challenges of accessing MHSU care, potentially making it even more difficult for youth to access the MHSU care that they need from the limited available services.
One of the hard things is that everybody’s your cousin, everybody’s your aunt, and everybody’s your uncle, so who do you talk to that’s gonna keep it just to you and not talk to everybody about it? – Participant 4 I think there’s so much stigma . . . you have no anonymity there. You have to make an appointment and then there’s . . . not even a room, there’s just a kiosk. . . And so . . . there’s no anonymity, . . . your mom probably knows the people who are working behind the desk. – Participant 9
Sub-Theme 1b: Peer, Family, and Community Norms or Standards
The participants spoke about how children and youth may be more highly influenced by their peer groups, families, and communities due to fewer social influences than if they lived in urban or more highly populated places. If the youth was surrounded by peers, family, or community members who hold low standards for what is possible, the youth may internalize these standards and maintain a shared sense of hopelessness or normalized mental ill health. Conversely, if the community was tight-knit or had a strong cultural identity, this may support the youth’s sense of belonging and mental wellbeing. The influence of these standards or norms may be heightened in more remote or less populated communities.
Because there’s such a small group of kids in each age group, . . . you can’t really choose your friends. . . . Certain kids who maybe seem like they [want to] go to university or strive to do well in school, . . . it almost seems like they kinda hold themselves back because. . . a lot of their peers don’t really care. So then . . . the standard is not super high. . . . And when your . . . peers are maybe into . . . substance use, . . . I think it’s easier to slide into that, because those are who you’re surrounded by all the time and looking . . . to fit in. – Participant 6 I do see a lot of kids who are in [foster] care, and I can’t think of one child who’s in care who doesn’t have a co-morbid mental health concern, . . . rooted in like vicarious trauma from witnessing, often their parents struggled with mental health and addiction. And so yeah, there’s a lot of kids that I see who have struggles at a very early age, with attachment, anxiety, depression, behavioral difficulties, . . . ADHD, oppositional defiance disorder, things like that that kind of go hand in that with household stress, and perinatal stress. . . . I can’t think of many children that I see that don’t have some form [of] mental health struggles, and as a result of the family disruption. – Participant 1 It’s so isolated and like everybody’s related, so anything that happens here ripples to everybody else. So . . . there was . . . a series of bad events like starting with quite a bad death, and some traumas . . . and so adult, youth, everybody’s mental health suffered. And then, of course, like you get adults who are then more tense and less available for the youth, and then you get youth acting out in some ways, trying to get attention, or just not getting the care and love that they need. And so then you start to see an increase in youth self-harm and things like that. So yeah, it’s so small. And everyone’s related, so everyone feels everything. And there’s no way for someone not to be impacted. – Participant 3 I think the fact that it is such a tight-knit community is very helpful for children to feel like they belong, and that they’re not alone. – Participant 4
Sub-Theme 1c: Navigating the (Un)available Resources
Several participants highlighted how there were limited opportunities for children and youth in their communities, and that transportation posed a significant barrier to access the available resources. Compared to urban communities, some rural communities had fewer recreational or MHSU resources that support youth wellbeing such as swimming lessons or psychological assessments. Transportation barriers exacerbated these resource limits; youth may have lacked access to a vehicle, a driver’s license, or a ride. Some of the nurses noted that even when public transportation was available, it was inadequate due to insufficient operating hours or failing to reach outlying areas where some youth lived. To overcome these challenges, some organizations offered transportation support, such as financial coverage, or virtual MHSU support to attend healthcare appointments. This reinforced the adaptability of rural systems but also underscored how child and youth wellbeing was tied to structural availability of services.
There’s no real bus service, so, for example, if somebody wants to stay after school, then how are they gonna get home? They’ll either hitchhike . . . , which is less safe now, especially in the wintertime when it gets dark pretty quick, after a bus goes. But . . . the buses . . . don’t serve the [community] in the way that if you were in . . . an urban centre you could go off, and. . . go to swimming practice, or you could go meet your friends downtown, or you could go do other things. And there’s . . . more opportunity for sure. I think . . . that the loneliness and isolation is hugely due to transportation. They don’t have their own cars. Cars are too expensive. And most live way off in [geographically distant area] or way off somewhere else. – Participant 9
Sub-Theme 1d: Leaving to Grow
Participants shared that some rural youth needed to leave their home community to pursue further education, find a career, or access appropriate MHSU support. However, this departure disconnected youth from their familiar support networks and cultural norms. This challenge was particularly acute for youth in remote communities as some youth needed to move away permanently to access MHSU care. Nurses reflected that this tension between staying in one’s home community and leaving to access opportunities was a recurring challenge for rural youth, shaping their experiences of both loss and possibility.
I think, with mental health, a lot of the youth that are having issues or have had issues, they get transported . . . out of the community, and then they tend to stay with family out of the community because they need more resources. – Participant 4 And so there’s definitely challenges . . . with kids who are growing up in these remote, small places. . . . Growing up in the community can be great when things are good in the family, and when they’re young, but teens and early young adults, . . . can have . . . a harder time of where do I fit in life, and where do I go? ‘Cause there’s a struggle of ‘this is home, and this is where my family is’ . . . but when they are wanting to seek higher education, different jobs, ‘how do I fit in in a big city’, but wanting to go home, but those jobs aren’t there? So in that teen, young adult age, trying to figure out where to be in life, I think, is harder. . . . Say you want to seek higher education, but you have to travel a long way for that, . . . that’s a lot more culture shock than somebody who’s in [larger city] going to Vancouver . . . and it’s further distance, too. – Participant 7
The participants pointed out how facets of the rural environment such as community connectedness, culture and norms, available resources, and transportation played a crucial role in shaping child and youth mental health, underscoring the ways rural context both supported and constrained child and youth wellbeing.
Theme 2: MHSU Care Was More Than Just MHSU Treatment
Participants described encountering a range of common youth mental health challenges, including depression, anxiety, suicidal ideation, self-harm, anorexia, bulimia, paranoia, and psychosis. All rural nurses were aware of or worked with youth who used substances, primarily alcohol, cannabis, and nicotine, and less often, stimulants, opioids, and psychedelics. The nurses described a broad range of MHSU nursing care for children and youth, primarily youth, including MHSU crisis intervention, assessment, counselling, treatment, harm reduction, case management, and referral to a higher level of care. Their versatile nursing approaches also extended beyond what is formally thought of as MHSU care to include strategies aimed at promoting safety within the healthcare system and navigating its complexities. Underlying these efforts was the prevailing mistrust in the health system among some rural youth and families that nurses work with.
Intergenerational trauma secondary to the . . . residential schools is like [the] definition of determinants of health at play. One thing that . . . I’ve noticed . . . is that because of like fear and the experiences that people have had with . . . their traumas, they often fear our systems. – Participant 1
Recognizing this challenge, rural nurses employed strategies aimed at (a) developing trust and safety between rural youth and the healthcare system, (b) facilitating continuity of care, and (c) advocating for equitable access to resources. This emphasis on trust-building and navigating the healthcare system underscored the vital role of rural nurses in ensuring effective care for children and youth, particularly in regions with limited resources and support services.
Sub-Theme 2a: Developing Trust and Safety Between Rural Youth and the Healthcare System
Participants emphasized aspects of relational care as central for establishing trust and safety with youth, recognizing that the need for relational approaches was intensified in some of the more remote or resource-deficient settings. Since nurses were the first point of contact with the healthcare system for some youth and one of few formal supports in their rural communities, cultivating trust became even more crucial; there were few or no alternative options for youth to seek MHSU care.
There’s a lack of . . . resources . . . and supports in rural [communities], so you really have to get creative and you have to build solid relationships so that your clients connect with you and come to your appointments and the injections and things like that, so a lot of relationship building. – Participant 10
Multiple nurses underscored that creating a safe, confidential space within their work setting (i.e., outpost nursing station, primary care clinic room, public health office, in a vehicle during outreach) for youth was an essential way to support trust and open communication.
Kids want to be seen in person, . . . there’s a real safety when they’re in a room that . . . they’re not gonna get walked in on. . . You learn so much just in that like hangout period, where they’re playing with something or they’re drawing on something, . . . and then they like drop you those little nuggets about . . . what they’re actually feeling. They need the space and time to do that. – Participant 3
Additionally, two nurses highlighted the importance of supporting youth to lead their care decisions, recognizing the challenges they faced in trusting external resources, such as a suicide hotline.
I normally talk about what what’s going on for them? . . . What have they tried before? What resources have worked for them? Do they know about Foundry? [provincial youth primary care, including MHSU, centres] . . . What do they want most? . . . What would their step one be? And then trying to facilitate that, whether it’s . . . connecting them with . . . a counsellor [at] Foundry . . . or . . . trying to pave the way calling with them sometimes, because it’s always scary to call a suicide hotline or any kind of outside number, like it’s . . . really hard to trust, especially when you’re a teenager, to admit that you need some help. . . . I’m really letting them drive what they need . . . and being open to them not being ready for it ‘cause . . . it’s really up to them. But just knowing that . . . here’s all the things, and sometimes all the things can be overwhelming. So . . . what’s one thing you wanna do? . . . How can we make that happen? – Participant 9
Moreover, four nurses described strategies to instill hope and possibilities in youth, such as encouraging career exploration and validating youth’s reactions to traumatic experiences.
[In] our positions, we had to have . . . lived experience to be able to take this role, and I use that to be able to support the youth, to . . . normalize it for them, and . . . to see that there is hope on the other side. You can achieve things even when you’ve gone through, . . . some severe whatever, and you’ve had your own challenges. There is hope. You can continue, like you can do the work. – Participant 11
Community programs and initiatives, like a human rights protest, were described as potential avenues to visibly demonstrate healthcare providers’ safety for youth.
And so there’s . . . visible support, . . . like we as the providers go, and we wear the T-shirts and show our faces, and let the people take pictures of us and say who we are, . . . and then that, in hopes, will trickle to the patients, especially the young folks, to know that their providers are safe. – Participant 1 I started a program where the . . . daycare kids like as young as 3 to 6, I have a day where I’ve had them come in and sort of take away the fear that they have of nurses, doctors in the hospital, like showing them how certain things are done, . . . like vitals, machines, or a cast, or an X-ray or drawing blood, just to sort of make that different for them, because they’re overhearing historically how the treatment was for their [Indigenous] culture, and so a lot of them are quite afraid of what’s going on. And then also the fear around, oh, so and so was here, and they got shipped off. That’s very scary for kids. They don’t wanna be shipped off. They wanna be where their family is. So just sort of explaining that to them a little better in the . . . child lens. – Participant 4
By prioritizing relationship building, rural nurses not only cultivated trust but helped youth to empower themselves in their healthcare journeys, potentially improving their future interactions with the healthcare system.
Sub-Theme 2b: Facilitating Continuity of Care
To ensure continuity of MHSU care in rural communities with limited resources, rural nurses adopted multifaceted approaches. Some nurses described how they integrated care by offering support that addressed the physical and mental health care needs during interactions with youth.
Teenagers are coming into immunizations, and so talking about HPV [human papillomavirus] and . . . how important that is, and then . . . what else is going on for them in their lives, and kind of one-stop shopping it . . . and knowing that our door is always open, they can come in whenever. – Participant 9
Leveraging their familiarity with the community, rural nurses provided tailored care that was responsive to the specific needs of youth, sometimes stepping beyond their usual roles to provide comprehensive support. Additionally, they collaborated with various health and social service providers to bridge gaps in service.
Like all rural nurses, [rural MHSU nurses] have to kind of fill every gap. – Participant 8
By proactively sharing relevant background information about youth between care providers who may be unfamiliar with the community and extending their reach to support rural clients admitted to urban hospitals, nurses enhanced the quality of MHSU care and minimized the risk of rural youth slipping through the cracks or receiving inadequate care.
We do daily meetings with acute care for anyone who’s [admitted] for their mental health and substance use issues so that we can make that connection and eliminate some of the gaps of them maybe going to the hospital, [and] us in rural communities not knowing. So now we all know, because we have a . . . daily meeting. So we hope the person consents, and then you can form a relationship. Sometimes . . . I’m supported to go meet them in the hospital, make a connection in person. . . . I could speak to a youth . . . or young adult who is really high risk . . . in a hospital setting, make that connection so that I can support them when they’re back rural. – Participant 10
Sub-Theme 2c: Advocating for Equitable Access to MHSU Resources
Participants actively engaged in advocating for resources and services to address systemic barriers. They participated in regional committees, communicated the realities of their rural communities’ needs, and pushed for fair allocation of resources.
For the treatment beds, there’s a regional bed committee that I was never a part of, and then somebody sent me a link, and then I was able to go to a zoom call and tell them, ‘hey, guys . . . this is the reality of my folks here’. . . . That communication . . . really . . . does improve the knowledge and the understanding . . . and it helps our clients be able to access care in a fair sort of way . . . when people in urban settings have a better idea of what they’re facing. – Participant 8
Their advocacy efforts extended to ensuring timely access to care for youth, such as nurses in high schools to provide non-judgmental support and information.
I found that hardly anybody has a doctor, and so . . . my big push lately has been to try and provide timely access . . . for teens. . . . I’m advocating for public health nurse presence, or some kind of presence in the . . . high school, so that that kids can come and they have access to say, birth control, or . . . if they’ve got STIs, or if they’ve got other challenges. . . . I would love to be able to provide more opportunities for kids to be able to ask questions with no judgment and health advice . . . and have . . . a constructive and a good relationship with people in the healthcare system, because when you have good interactions, it paves the way to be able to have better interactions later, and to be able to ask for help later when you need it. – Participant 9
Rural nurses also facilitated transitions from acute care to substance use treatment by advocating for seamless transfers between care levels and providing logistical support, thereby increasing the likelihood of successful outcomes for youth.
If [youth] are hospitalized with anything related to their substance use, and they want treatment, we can really push . . . the acute care end to say . . . ‘They really want to go. We’ve worked with them. This is their opportunity. And . . . let us help’ and as soon as we say we can help, the acute care . . . doctors, will sign anything, psychiatrists will sign anything if you’re offering to . . . take the bulk of that referral . . . and complete it. So often we’ll do that when our clients are in hospital like ‘let us do the work’ and let’s get them in so that they can go from the hospital to treatment and have a good . . . chance of success. – Participant 10
All nurses identified social determinants of health that underlie or influence rural youth MHSU, including gender, sexuality, historical and ongoing trauma, culture, racism, education, social support, housing, income and financial insecurity. The COVID-19 pandemic, the ongoing toxic drug crisis, and rural community isolation were also noted to contribute to MHSU challenges among youth.
Looking at the social determinants of health . . . I’ve like recognized it kind of everywhere in everybody’s care and so applying that to youth: most often . . . the youth in my practice I see are affected on multiple levels, on like lacking in social determinants of health. So access to. . .safe housing, having. . .those strong family units, . . . lack of access to social supports and education, so a few of them aren’t attending school, . . . lack of access to longitudinal primary care. – Participant 2
Rural nurses highlighted that advocacy work addressing the social determinants of health was part of the nursing scope of practice and was MHSU care. Through these advocacy efforts, nurses worked to bridge the gap between available services and the diverse needs of rural youth, ultimately enhancing the overall MHSU care landscape and health of rural communities.
The biggest challenge . . . I see is that there’s no emergency housing for youth here whatsoever. . . . If they’re in an unsafe position, there’s nowhere to go. . . . [So] learning how to advocate for these changes . . . has been super beneficial for me. . . . I’ve tried to . . . find the . . . channels to advocate for change within [health authority] and basically it’s ‘go to your manager, . . . make the suggestion, and then the manager will take it to . . . the steps above them’. And then . . . what gets lost in the process? What gets lost in translation, you know? And so that’s . . . another reason why I found connecting with BCNU [British Columbia Nurses Union] and learning how these advocacy pieces work [necessary], and . . . connecting with MLAs [Member of Legislative Assembly] and being able to say . . . “this is what we really need here”. . . . I do believe it is . . . part of MHSU work. – Participant 11
Theme 3: The Essential Components of Rural Child and Youth MHSU Nursing Practice
To support rural child and youth MHSU care, participants described a continuum of factors that made this work possible, ranging from nurse qualities to system supports. They emphasized that effective care was facilitated by several key aspects: (a) embracing rural nurse qualities, (b) having enough time to care, (c) access to practice support, (d) knowing the community, (e) being part of a cohesive and supportive team, and (f) effective communication and collaboration across health systems.
Sub-Theme 3a: Embracing Rural Nurse Qualities and Ways of Being
Participants described core qualities and ways of being that helped them to navigate, support, or carry out child and youth MHSU care. These qualities are more about how nurses provided care rather than what care was provided. They approached their work with authenticity and relatability, establishing connections with youth.
I just try to be authentic and try to support them with as much as I know how to do. – Participant 4
Nearly all of the participants described how their own lived experiences related to MHSU deepened their empathy and understanding, enhanced rapport building, or guided effective care strategies for children, youth, and families.
I’ve had lived experience . . . with mental health and addictions as a youth. So I think . . . having lived experience has helped me a lot, just to understand better . . . what needs to be addressed . . . with the patients . . . . It just gives you a different . . . understanding of the situations that people are coming from. – Participant 1
Further, some of the nurses noted the importance of a harm reduction approach or philosophy of practice, of holding a nonjudgmental attitude and meeting youth where they’re at, to help create a safe and supportive environment. This approach was particularly important in rural and remote communities that had limited confidential spaces.
I meet the youth where they’re at to kind of reduce any barriers that way. A lot of the youth have trust issues, and so it’s hard to get them to come into facility . . . so oftentimes I will meet them at a local park or at a local restaurant. A lot of the meetings happen in my vehicle so that they have a safe place where they know people aren’t gonna overhear them, but yet it doesn’t have the stigma of accessing mental health supports. – Participant 11
In addition, two rural nurses described how a strengths-based perspective supported MHSU care.
I think that the important part is, I don’t have to have all their answers. I have to let go of fixing it, I just have to convince them that they matter. They matter to me, and they matter . . . in the world, and . . . there’s lots of people . . . who think that they matter as well. And it’s hard for some kids who don’t have a lot of people who care about them . . . to think that anybody else thinks that they do. – Participant 9
Some of the rural nurses shared that flexibility, resourcefulness, and creativity were important qualities for navigating the constraints of rural healthcare systems.
[It’s] hard to find the resources to support somebody when they’re not living in urban centers with access to more things to do with . . . gender identity issues, sexual health clinics, things like that. So again, that’s another piece of us having to be creative is finding those resources, . . . being up with that stuff ourselves so we can support our youth because it’s . . . definitely an issue, and then that also contributes to them using substances and drinking alcohol and things to cope and manage the way that they’re feeling. – Participant 10
Overall, these qualities and ways of being enabled rural nurses to deliver compassionate, holistic, and effective MHSU care that addressed the unique needs of children and youth in rural communities.
Sub-Theme 3b: Having Enough Time to Care
Time was highlighted as a key care facilitator when working with children and youth. Nearly half of the rural nurses talked about the importance of having enough time to provide MHSU care. Three nurses noted that having time for care was one strength of their remote communities.
I think, for a lot of the relationships as you can probably appreciate, it takes time for youth to really open up to know that you’re a safe person that they can share [about their substance use] and won’t be judged. – Participant 2 The advantage of working in this really small community, and compared to where I’ve worked in busy, bigger emergency departments, is . . . we have more time. And so . . . I’m not getting pulled to look after other people so much, so I could sit and listen, and I’ll just say, . . . tell me more about that, and that feels good, right? ‘Cause I think . . . people wanna be heard and have somebody to just talk to and feel like they’re getting heard. . . . I can have the time to do that, and that feels good to be able to have that time. – Participant 7
Some of the nurses commented on how a lack of time hindered their ability to access education or collaborate with local support.
I would love to have . . . more education in the child and youth stuff and . . . if I take time to figure out what I should take, . . . then I can probably pitch it, and . . . it will probably be supported. But that’s like off the side of my desk while I’m also the only person [in this role]. – Participant 8
Sub-Theme 3c: Access to Practice Support
All of the participants shared a range of resources that supported MHSU care, including resources for children, youth, and their families, and resources to inform or guide nursing practice. The topics included immediate virtual support and MHSU information for children, youth, families, and care providers; and child and youth MHSU nursing practice support. All of these resources were free and accessible with an internet or phone connection.
Some of the participants talked about theories and approaches that supported their MHSU practice with children and youth, including cognitive behavioural therapy, harm reduction, motivational interviewing, polyvagal theory, and trauma-informed practice. In addition to these theories or approaches, nurses spoke about considering perspectives from a wide variety of sources on topics for their practice, like parenting, trauma, and mindfulness.
Sub-Theme 3d: Knowing the Community
Rural nurses shared that their MHSU work was facilitated by knowing the client, family, and community. Although having a dual role may have been challenging, it helped some nurses to understand the youth’s life context and humanized their care encounters.
And quite often the kids that are presenting, . . . if they’re coming in for alcohol abuse, . . . we know the community, and we know their family, and you know it’s like a generational thing like you just seen their [parent] the week before, for like abuse or detox, you know, stuff like that. So that’s kind of an interesting aspect, just the fact that . . . you know their family and kind of the history of their family in that as well. . . . It kind of opens your eyes up more to what they are facing, makes you a little bit more empathetic, . . . just with what they’re going through on their day-to-day. I think, when you’re in a bigger centre, and you see a kid come in for that, . . . you hear what they’re telling you there and now, but . . . when you’re [in the rural community] and . . . you see them day to day around the community, and you know what else they’re facing, it . . . makes you relate to them a little bit more on a deeper level. – Participant 6
Additionally, one rural nurse noted that knowing support persons from the community could have increased the likelihood of youth engaging with those supports if the nurse vouched for them.
Knowing like the drug and alcohol counselors for youth, or the school counselors, or . . . child and youth mental health, like knowing them, so when you’re referring them, you can say, ‘hey, . . . I know this guy, he’s so awesome, he’ll come to you and work with you at school’. So like knowing the roles of the people you’re referring them to, not just like blindly giving them a phone number, like get to know the people who are supporting the youth so you have a personal opinion when you’re selling the youth to accessing [them]. I really feel that that’s helpful. But that . . . comes with time and experience and getting to know the community and those other people supporting youth, because . . . then you hope that their chances of connecting . . . are higher. – Participant 10
Sub-Theme 3e: Being Part of a Cohesive, Supportive Team
Some participants described different facets of a supportive team: co-worker support, adequate and regular staffing, leadership support, counselling, and immediate consultation. Co-worker support included immediate critical incident debriefing, especially after challenging and emotionally demanding situations such as youth overdoses or assaults; regular team check-ins; a willingness to help colleagues; and support to think creatively through resource-limited situations.
Recently, [we had a critical incident] and the . . . follow up of that was quite a lot of like team support, and debriefing from that. We have a lot of kids that . . . repeatedly overdose or are victims of varying types of assault, and we tend to see them quite promptly after. So . . . we just make sure to always have someone [for debriefing], like we have [a] group chat. And so we do a lot of debriefing . . . right away. There’s no like, ‘let’s book a [critical incident stress debrief] next month’, . . . it’s like right now, anybody needs to call anytime like outside work, whatever, come over, or do you need dinner? . . . We have just kind of like a no holds bar policy, . . . if somebody needs something, . . . just call. – Participant 1
Almost half of the rural nurses underscored the challenges of working in isolation or the effects of an inconsistent team. A regular and adequately staffed team better facilitated continuity of care, co-worker support, and safety.
More regular staffing makes a difference. When we’re all travel nurses, there is no team. Sometimes you’ll meet other travel nurses, and . . . right away, you have each other’s backs, but it’s not the same as an actual regular team. – Participant 3 If there’s someone that’s in a mental health crisis and they need to go to higher level of care, we’re waiting for a plane to come, and it can take a day or 2 or 3. And so with the staffing that we have, I could be awake for 48 hours watching this patient by myself, and then leaving the community without a nurse. – Participant 4
One rural nurse linked insufficient staffing with the potential to negatively impact continuity of care and subsequently, the development of trust between nurses and youth.
It’s really nice when . . . there’s . . . continuity of care up here. . . but that is a staffing issue. But you know, when there is like the same staff, and you can build that trust with them over a series of years in that community, and they know, okay, you’re a person I can talk to, and that’s safe. But when there’s always new staff like travel nurses coming in, or travel doctors, . . . each time they have their guards up a bit, . . . and you have to slowly break those down again. So yeah, that’s a big struggle in the rural communities, just having that continuity of care to kind of build that trust with teenagers. – Participant 6
In addition to the necessity of adequate staffing, nurses shared how valuable it was to be supported by responsive, communicative leadership that advocated for nurses’ well-being and supported Indigenous culture in the workplace.
It’s a lovely place and very well supported like . . . management and administration is just amazing for us there. . . . [Health authority] recognizes the Indigenous culture and supports it. . . . The administrator will check in with us like every 2 hours to make sure that we’re not burning out, our mental health is not being affected, and that we have the supports that are needed. And [they] will either . . . drive [themself] in or fly in the next day, if we need it. [They’ll] make the doctors get involved as well where the doctors are gonna have to do a 4-hour shift of staying up all night . . . if we’re . . . hitting a wall. Yeah, so I feel very supported that way. – Participant 4
One example of more formal support was having an organization set up counselling that the healthcare team could access in the workplace. In contrast, another nurse noted that there was private counselling available through extended benefits, but it may have been insufficient.
We actually have . . . a day set aside for . . . counsellors coming in . . . to provide individual counselling to all of us, . . . because we get vicarious trauma working with clients in this [work]. – Participant 5
Rural nurses identified immediate consultation for child and youth MHSU care as another feature of a supportive team. Few of the nurses had access to immediate consultation, and the ones who did were from larger rural centres. One nurse identified the lack of immediate consultation as a barrier to care when supporting youth in crisis.
Now I have a really experienced, dedicated team of nurse practitioners for immediate consultation, so that has been a wonderful change. When I first started with this organization . . . I only had access to virtual consults for physicians that were not immediately available. So that’s been great, just having more immediate support. – Participant 5 But it’s been challenging because the team leads, they’re busy, . . . and the on-site team leads don’t have specific knowledge, and so then they have to dig to somebody else, right? There’s that hierarchy of like who I can access. And then our main knowledge coordinators are out of [city], so then it means sending an email or asking for a meeting, and meanwhile you’re trying to support these youth in crisis. – Participant 11
Sub-Theme 3f: Effective Communication and Collaboration Across Health Systems
All of the nurses spoke about the lack of rural MHSU resources for all rural people broadly and for children and youth specifically. When the appropriate resources existed, nurses described siloed services and fragmented communication, highlighting the need for effective communication and collaboration across all health system levels.
There are programs and services that we know nothing about. We don’t hear anything about it. Or we maybe get like an email, and . . . other people get presentations and things like that which we don’t get here. And so that, I think is a bit problematic. – Participant 8
Effective communication improved awareness of, access to, and collaboration with resources that supported rural child and youth MHSU.
This morning I was connecting with [a nurse] up at the hospital . . . to look at wound care, because a lot of our clients who come in for their [harm reduction supplies], . . . they’re like, well, I need antibiotic cream because look at my hands or look at [my] trench foot, or whatever. . . . So I connected with [specific nurse] to say, hey, if you provide . . . these items, we can make up the kits and then put them out . . . when we’re doing harm reduction and walkarounds. And when . . . we’re giving people what they need, . . . they’re gonna trust us more, and . . . if we can give them something so they don’t have to go to the hospital, we save $700 every time, right? So [another nurse]’s gonna connect with [local service] cause they’ve got better stuff, and then hopefully, . . . they can give us the stuff, and it’s not a big deal, and then we’re working, not in silos. – Participant 9
Further, understanding and supporting the rural reality was an important facet of health system communication between urban and rural settings.
I’m not sure that [urban intake clinician] understands the reality of [rural] clients. . . . Like what does it mean when you’re living in a trailer with no electricity, and you don’t have cell phone coverage? . . . So when I’m interacting with services and they’re telling me that my clients need to engage in lower-level services before they can access like treatment programs, . . . I’m like, what lower-level services are you talking about? They’re talking to me, like that’s it. . . . So I think the rural reality is hard to understand unless you are part of that experience. – Participant 8
These rural nurses offered valuable insights about child and youth MHSU care, drawing on their deep understanding of the unique challenges, strengths, and realities of their rural and remote communities. They weaved insights that helped to better understand their nursing practice, including the embeddedness of child and youth mental health in their rural context, the expanded role nurses had within MHSU care, and a deep awareness of what supported their practice. From the individual nurse to the broader health systems level, these nurses worked hard to care, connect, and advocate toward better MHSU care for rural children and youth.
Discussion
Rural healthcare delivery is shaped by intersecting factors such as geographical isolation, resource limitations, and the social determinants of health, all of which influence how children, youth, and their family’s access MHSU services (Thomas et al., 2024). Literature on rural nursing emphasizes the broad scope, adaptability, and strong relational focus that characterize nursing practice in these contexts (MacLeod et al., 2017; Thomas et al., 2024). Rural youth face unique challenges compared to their urban peers, including reduced service availability (Canadian Institute for Health Information, 2019), longer distances from MHSU services (Jones & Quinn, 2021), and the potential for heightened stigma in smaller, closely connected communities (Graves et al., 2024). These systemic factors are compounded by broader inequities in rural healthcare systems, where fewer providers, inconsistent funding, and limited integration of services can hinder MHSU care (Thomas et al., 2024).
Within this broader body of knowledge, we used rural nurses’ descriptions of child and youth MHSU care in community practice settings in BC to develop themes showing what can be learned from their approaches to providing care and the contextual factors that shape their practices. Their accounts reinforce and expand on existing understandings of rural health and nursing practice, particularly as they relate to the delivery of MHSU care in resource-constrained and geographically isolated environments. These findings not only align with literature on rural health equity and system-level barriers (Leimbigler et al., 2022) but also highlight the ways nurses adapt their roles to address gaps in care (Barrett et al., 2016), leveraging trust-based relationships, local knowledge, and advocacy to support children and youth’s mental health and wellbeing. Additionally, these findings strengthen the Standards (CHNC, 2019), particularly their emphasis on equity, health promotion, and community partnerships, and the Framework’s (CARRN, 2020) recognition of the multilayered, rural contextual realities shaping rural nursing practice. This study delineates the importance of the rural nurse-client (i.e., child, youth, and family) relationship for building trust in the health system and facilitating access to care, especially when nurses are adequately supported and resourced. Two key points are discussed further: the role of rural nurses in early intervention and in supporting rural-centric approaches to MHSU care.
Rural nurses can play a pivotal role in early intervention, the early identification and treatment of MHSU challenges (McGorry & Mei, 2018) among children, youth, and families in rural communities. Since rural nurses may serve as the first professional point of contact (MacLeod et al., 2022), this provides a unique opportunity for relationship and trust-building from the outset in children and youth’s healthcare interactions. This early engagement is crucial, as research underscores the early onset of MHSU challenges in youth (Solmi et al., 2022). Early psychosis intervention studies indicate that recognizing and addressing MHSU challenges in their beginning stages can lead to better outcomes and reduced long-term MHSU impacts compared to treatment-as-usual (Correll et al., 2018), and early intervention approaches also show promising results when extended to non-psychotic disorders such as depression (Davey & McGorry, 2019). As explored in Theme 1, that child and youth MHSU is bound to the rural context, the potential familiarity that rural nurses have with their clients and local communities could help them to assess the psychosocial context of children and youth and recognize early signs and symptoms of MHSU challenges. Their understanding may extend beyond clinical symptoms and a narrower understanding of MHSU care to include building trust between children, youth, and the health system, facilitating continuity of care, and advocating for MHSU resources, as described in Theme 2. This understanding could facilitate comprehensive individual and systems-level MHSU care (Mpheng et al., 2022). However, to intervene early, rural nurses need to be supported, as identified in Theme 3, by sufficient staffing levels, appropriate supports and resources, and adequate training (Mpheng et al., 2022). For example, Cusack et al. (2017) describe how comprehensive supports, such as access to proper training and education, are needed for nurses to provide comprehensive mental health care, including early intervention. In rural communities where there may be substantial staffing and resource inadequacies, this comprehensive support may need to include additional facets, such as virtual support and 24-hour helplines for MHSU care (Novak Lauscher et al., 2023).
Alongside early intervention, the findings underscore rural nurses’ role in supporting rural-centric approaches (Perkins et al., 2019) to MHSU care. Rural communities encounter distinct and complex challenges such as limited or absent services and geographical isolation (CARRN, 2020). Recognizing the necessity of properly supporting rural mental health care, Perkins et al. (2019) outline the importance of rural-centric approaches compared to adopting urban-centric approaches. Rural-centric approaches, grounded in the unique characteristics of rural communities, emphasize place-based, integrated, and community-engaged service development (Perkins et al., 2019). Rural nurses could have an important role in supporting rural-centric approaches to MHSU care for children and youth. Through their potential sensitivity to the psychosocial context of their clients and communities, as discussed in Theme 1, rural nurses are likely more aware of what MHSU supports and resources are needed, compared to resources developed by urban health services. Moreover, in alignment with Theme 2, rural nurses may need to advocate for their role to be adaptable and responsive to community needs (i.e., rural-centric), encompassing a broader scope of practice compared to their urban counterparts. This could include integrating counselling support within nursing practice (British Columbia College of Nurses and Midwives, 2023; MacLeod et al., 2022) in communities with few or no counselling supports, such as motivational interviewing to support client behaviour change (Gagneur, 2020) or cognitive behavioural therapy for depression (Van Lieshout et al., 2022). Collaborative efforts by nurses working across health promotion and illness prevention may offer greater benefits to rural children, youth, and families compared to a narrow scope of practice (Burch & Stoeckel, 2021). For example, Kulbok et al. (2012) described how public health nurses followed a community participatory health promotion model to partner with interdisciplinary researchers, youth, parents, and community members to develop a youth substance use prevention program. Furthermore, as discussed in Theme 3, supporting rural nurses in their practice is essential for implementing rural-centric MHSU services. Rural nurses may need the time to get to know their communities, especially if they are new to the community (Kulig et al., 2018); the team and community support to collaborate on service development or provision (Beks et al., 2018; Etter et al., 2019); and improved communication across local and non-local health systems (Sutherland et al., 2020) to leverage available resources to create and adapt services. These necessary supports can provide the foundation for nurses to advocate for and deliver context-sensitive MHSU care to children and youth in rural areas.
By illustrating both the systemic barriers and the unique opportunities that shape rural nurses’ roles in child and youth MHSU care, our findings have notable implications for practice and policy. For nursing practice, rural nurses require organizational support to protect time for therapeutic engagement (MacLeod et al., 2022), access to real-time consultation (e.g., virtual psychiatric support) (Cosgrave et al., 2018; Novak Lauscher et al., 2023), and opportunities for interprofessional and community partnerships (Ratter, 2023). Embedding routine MHSU screening and fostering early intervention can help identify concerns earlier and improve long-term outcomes (Correll et al., 2018). Reducing stigma through open dialogue with children, youth, and families, as well as through community education, are also important strategies (Childs et al., 2021; Radez et al., 2021). Continuing education that equips nurses with trauma-informed, culturally safe (Curtis et al., 2019), and community-centred approaches, as noted in both of our theoretical frameworks (CHNC, 2019; Pavloff et al., 2022), are necessary for strengthening care in rural contexts.
For policy, health agencies and governments must move beyond urban-centric models and design flexible, rural-centric approaches that account for geographic distances, technology challenges, and workforce shortages (Perkins et al., 2019). Policies that support care integration between rural and urban systems – such as streamlined referral pathways and shared health information and education systems – could reduce fragmentation and improve continuity of care (Sutherland et al., 2020). Importantly, creating opportunities for rural nurses to contribute to health policy development and advocacy is essential to ensure rural health perspectives are meaningfully included in system design (Kulig et al., 2004).
Limitations and Future Research
While this qualitative study offers valuable insights into the role of rural nurses in supporting MHSU care of rural children and youth, there were multiple limitations. First, the study sample consisted primarily of nurses from rural and remote regions of BC, Canada, potentially limiting the transferability of the study findings to other regions in Canada or worldwide. Additionally, the sample size was relatively small and homogenous, which may have restricted the breadth and depth of perspectives included in the study. Demographic information such as gender identity was not collected. This absence limits an in-depth consideration of how gender norms and roles may have shaped both nursing practice and the findings. While our study did not explicitly collect gender data, it is important to situate these findings within the broader context of nursing as a gendered profession. Predominantly comprised of women, nursing has historically been undervalued and under-resourced, and these gendered associations continue to shape how nurses’ contributions are valued and how power and resources are distributed within patriarchal health systems (International Council of Nurses, 2022). These inequities also intersect with other dimensions such as race, class, and gender diversity, shaping how different groups of nurses’ experience and resist structural disadvantage within healthcare (Candelaria et al., 2025). Finally, this study did not include the specific perspectives of rural children, youth, and families, although some of the rural nurses in the study were also community members with children and/or youth. Including their perspectives could have provided valuable firsthand insights about MHSU care in rural areas. Despite these limitations, this study contributes to the growing body of literature on rural child and youth MHSU nursing and provides a foundation for further research in this important area of healthcare. Future research should continue to expand our understanding of rural child and youth MHSU nursing care. Studies with more diverse samples are needed to ensure a broader representation of rural nurses, including men, gender-diverse individuals, and nurses from various geographic regions. Examining whether nurses from different backgrounds hold unique perspectives or employ distinct strategies in MHSU care delivery could inform the development of tailored MHSU supports and interventions. Additionally, understanding how nurses can actively engage in rural health policy development and advocacy efforts is essential, requiring exploration of barriers, facilitators, and strategies for nurse involvement in policy-making processes. By addressing these research gaps, we can enhance the capacity of rural nurses to support MHSU care and contribute to positive health outcomes for children and youth in rural areas.
Conclusion
The prevalence and early onset of MHSU disorders present significant challenges for children and youth globally (Erskine et al., 2015; Solmi et al., 2022), with rural communities facing additional barriers to accessing care (Moroz et al., 2020; Sinclair, 2020). This study aimed to learn from rural nurses about MHSU care for children and youth in community settings, describing the pivotal role rural nurses can play in providing comprehensive MHSU care and highlighting the support needed for their practice. Further research is needed to better understand MHSU care provision aimed at addressing the unique needs of rural communities. This study underscores the importance of supporting rural nurses, recognizing their invaluable expertise in understanding and improving MHSU care of children and youth, and highlights the need for rural-centric policy and practice supports that address inequities in rural healthcare.
Supplemental Material
sj-docx-1-gqn-10.1177_23333936251404917 – Supplemental material for An Interpretive Description of Nurses’ Perspectives on Rural Child and Youth Mental Health and Substance Use Care
Supplemental material, sj-docx-1-gqn-10.1177_23333936251404917 for An Interpretive Description of Nurses’ Perspectives on Rural Child and Youth Mental Health and Substance Use Care by Sage Thomas, Nelly D. Oelke, Dennis Jasper and Elizabeth Keys in Global Qualitative Nursing Research
Footnotes
Acknowledgements
We are deeply grateful to the rural nurses who generously shared their time and experiences for this study; their insights and reflections form the foundation for this work. We also thank Michelle Pavloff for her valuable contributions and insights related to Canadian rural and remote nursing, which helped strengthen the study design and framing.
We respectfully acknowledge that this research was conducted across the ancestral, traditional, and unceded territories of Indigenous peoples across what is colonially known as BC, Canada. We are thankful to these communities whose ongoing stewardship, leadership, and wisdom continue to shape rural health and nursing practice.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.