
Abstract
Despite promising declines in new HIV diagnoses, Latinas continue to experience elevated rates of HIV in the United States. Their increased risk of HIV infection is influenced by socio-cultural factors that hinder effective prevention efforts. The objective of this study was to elicit the perspectives of Latinas about the influence of socio-cultural factors on HIV prevention. A qualitative description method was conducted with 33 women who participated in focus groups in South Florida. A conventional content analysis was used, with coding categories derived directly from the participants’ narratives. Analysis yielded three categories related to socio-cultural factors that influence HIV transmission: (1) Marianismo, (2) Machismo, and (3) Familismo. The findings revealed power imbalances in Latinas’ intimate relationships, shaped by these three socio-cultural factors that continue to influence sexual health behaviors and increase HIV risk. The findings also revealed that while power imbalances exist, Latinas also exercise autonomy, support their families, or find alternative ways to access prevention resources. These behaviors reflect ongoing sociocultural influences that shape decision-making and health engagement. It is therefore critical to consider these evolving dynamics when developing HIV prevention interventions that are responsive to the unique socio-cultural contexts affecting Latinas.
Introduction
Latinas continue to be disproportionally affected by HIV in the United States (U.S.). Despite promising declines in new HIV diagnoses, Latinas account for 20% of new diagnoses among people assigned female sex at birth (HIV.gov, 2025). It is estimated that in 2022, Latinas were nearly three times more likely than non-Latina women to die from HIV infection and 19 times more likely to have AIDS (U.S. Department of Health and Human Services, Office of Minority Health, 2025). Among Latinas, it is estimated that 87% of new HIV diagnoses are attributed to heterosexual contact and 12%are attributed to injection drug use (Centers for Disease and Control and Prevention, 2024). In regard to location, the Southern states as defined by the U.S. Census Bureau, accounted for almost half (52%) of the new HIV infections (HIV.gov, 2025). This disproportionate impact underscores the urgent need for targeted public health interventions and culturally responsive strategies to address HIV prevention and care among Latinas in Southern communities.
Increased risk for HIV infection among Latina women is linked to socio-cultural factors that influence HIV prevention (Cianelli et al., 2024; Peragallo-Montano et al., 2019). These factors are associated with traditional gender roles, such as machismo and marianismo (Cianelli et al., 2024), as well as the significance of family, commonly referred to as familismo in the Latino culture (Mendoza-Grey et al., 2024; Ramírez-Ortiz et al., 2020). Machismo refers to the view of masculinity in the Latino culture and describes the idea of a strong man in control of his environment including women and promotes male dominance in the sexual relationship (Cianelli et al., 2015; Valdez et al., 2023). It also reinforces the traditional gender roles that assign men as the providers and protectors, while women are relegated to more subordinate and supportive roles (Valdez et al., 2023). Machismo is not just an individual attitude or behavior, but a systemic norm that is deeply embedded in the Latino society’s institutions and has been associated with patriarchy, sexism, and chauvinism (Valdez et al., 2023). Negative aspects of machismo have been associated with a lack of condom use, infidelity, multiple sexual partners, unprotected sex or lower condom use, drug use, alcohol consumption, and intimate partner violence (IPV) (Cianelli et al., 2013, 2015; Ferrer et al., 2016; Mancera et al., 2017; Peragallo-Montano et al., 2019).
Marianismo is the counterpart of machismo and denotes the traditional view of femininity in the Latino culture (Da Silva et al., 2021). This view emphasizes the ideal woman as submissive to men, pure, dependent, vulnerable, abstinent until marriage, innocent, silent, and self-sacrificing (Cano et al., 2020; Cianelli & Villegas, 2016). Women who endorse marianismo values are submissive to the demands of men and accept extreme sacrifices and suffering for the family to maintain harmony (Da Silva et al., 2021; Morales & Fernando Rojas, 2020). It has also been associated with greater family cohesion, respect for the family hierarchy, prevention of substance use among Latinas, and development of spirituality and religious education in the family (Cano et al., 2020; Sanchez et al., 2019). However, this cultural value has been associated with a lack of protection during intercourse, IPV, and lack of sexual communication and negotiation with their partners about preventive behaviors, which increase their chances of acquiring HIV (Da Silva et al., 2021; Sanchez et al., 2019).
Familism is a salient cultural value and reflects the importance of family (or family pride) (Mendoza-Grey et al., 2024; Ramírez-Ortiz et al., 2020). Latinas who endorse high levels of familism values engage less in risky behaviors so as not to compromise their family values and maintain close relationships (M. M. Hernández & Bámaca-Colbert, 2016). Familismo has also been associated with HIV prevention behaviors, especially HIV testing and condom use (Ma & Malcolm, 2016; Ramírez-Ortiz et al., 2020). HIV-prevention risks arise when Latinas often suppress their needs, thoughts, and opinions in relationships to avoid conflict and maintain harmony and family cohesion (Cianelli & Villegas, 2016; A. Hernandez et al., 2012; Villegas et al., 2013). Latinas also tend to prioritize daily survival and family responsibilities over concerns about HIV prevention (Cianelli & Villegas, 2016; A. Hernandez, et al., 2012; Villegas et al., 2013).
Although existing literature recognizes the role of sociocultural factors in HIV risk and prevention among Latinas, recent research examining their current and evolving influence, as well as Latinas’ own perceptions of these factors, remains limited. Research with Latino families shows that family dynamics and cultural influences are not fixed but rather evolve across developmental stages and in response to broader sociopolitical contexts (Roche et al., 2022). In the past decade, shifts in immigration and acculturation patterns, changes in gender norms expectations due to increases in Latinas’ educational attainment and labor force participation, and access to digital health information have likely reshaped how sociocultural norms influence HIV-related attitudes and behaviors among Latinas; yet these changes have not been recently explored and Latinas continue being one of the most at risk and understudied groups in the U.S. (Ertl & Fresquez, 2024; Pew Research Center, 2024; Ravelo et al., 2022; Victorson et al., 2014).
Among Latinas there is limited understanding of which dimensions of these factors, such as marianismo, familismo, or machismo, have become most relevant or influential in recent years. Moreover, these factors operate through distinct dynamics and manifest in multiple contexts, including the household, partnership relationships, and clinical encounters (Dillon et al., 2018; Molina et al., 2019). Most existing interventions have focused on individual-level behavior change and have not adequately incorporated sociocultural mechanisms identified by Latina women themselves (Cabral et al., 2023, Daniel-Ulloa, 2016). The lack of interventions built on the cultural context of Latinas has led to cultural norms that continue shaping risk behaviors and sustaining HIV vulnerability among Latinas, limiting the understanding of Latino community experiences and slowing the adaptation of evidence-based interventions (Castro et al., 2023; Daniel-Ulloa, 2016). Addressing this gap can be promising to improve the effectiveness of interventions for Latinas. Therefore, this study aimed to elicit the perspectives of Latinas about the influence of socio-cultural factors on HIV prevention, with the goal of using this information to create a culturally tailored HIV prevention intervention. By grounding this analysis in participants’ own narratives, this study offers culturally relevant insights needed to guide the design of tailored, community-driven HIV prevention interventions for Latinas in Florida and across the United States. Prior to this study, no recent literature provided context on how cultural factors shaped the experiences of Latinas in Florida or the broader United States in relation to HIV prevention and risk, nor how these factors manifested in their daily lives. This understanding was essential for developing culturally tailored storylines that authentically reflected participants’ realities (Villegas et al., 2023).
Methods
Design
A qualitative description method (Sandelowski, 2000) was used to examine Latinas’ perspectives regarding HIV and relevant socio-cultural factors. This method provides straightforward descriptions of participants’ experiences and perceptions, particularly in areas where little is known about the topic under investigation (Doyle et al., 2020; Sandelowski, 2010). This study is part of the first phase of a larger study aimed at developing a culturally tailored intervention called ‘Infección de Amor (Infectious love)’, a telenovela (soap opera) intervention with a storyline that incorporates modeling of HIV prevention behaviors in relationship contexts grounded in Latina socio-cultural factors (Villegas et al., 2023).
Sample and Setting
A total of 33 Spanish-speaking Latinas participated in this study. Participants were recruited using a purposive sampling approach to identify cases deemed information-rich for the purposes of the study (Creswell & Poth, 2018). Participants were recruited face-to-face using flyers in the cities of Homestead and Florida City within Miami Dade County, located in South Florida. These areas are considered Miami suburbs and major agricultural areas. Demographic information about participants in the study is presented in Table 1.
Demographic Characteristics of Participants in the Study.

Source. Latinas classified as having low-income under the guideline issued by the Health and Human Services Department (2025).
The study was conducted between 2018 and 2019 in collaboration with three community organizations located in a predominantly Latino, low-income areas of Florida, where agricultural work is a primary source of employment. These organizations are non-profit and provide different community services. One of them focused on advocacy, reduction of domestic and sexual abuse, and support services for families. The other two organizations are advocacy organizations focused on providing job training, placement, and services (e.g., education, food access) to farmworkers, rural, and other low-income communities in Florida. These community organizations recruited participants for the study and supported the study-related activities. Potential participants were approached by a recruiter from the research team or community center staff at popular gathering places for Latinas, such as churches, libraries, and grocery stores. Additionally, recruitment was conducted through face-to-face interactions and flyers distributed at community agencies. All three locations had private rooms where research activities (e.g., screening, data collection) were conducted. Inclusion criteria were: (a) self-identified as a Latina, (b) worked in agriculture or related activities in South Florida, (c) were between 18 and 35 years old, (d) reported sexual activity with a man in the last 6 months, (e) able to speak Spanish, and (f) able to provide informed consent in Spanish.
Data Collection
Data were collected through four focus groups involving a total of 33 participants (7–10 women per group as suggested on qualitative research standards and prior experience). A primary facilitator led each session while a co-facilitator took notes. The discussions took place in familiar community organization settings, which helped create a comfortable and inclusive environment. To support participation, food was provided, and childcare was available during the sessions. Overall, participants engaged actively in the conversations, contributing diverse perspectives within a supportive group dynamic. The group size allowed sufficient interaction about sensitive topics and maintained a comfortable and safe environment that encouraged open discussion among Latina participants about culturally sensitive issues related to HIV prevention. Women interested in participating were screened by study personnel by phone or in person in a private location using an eligibility form created for the study. If potential participants met inclusion criteria, an appointment for the focus group was made. Before the focus group, women read the informed consent and after each participant’s questions were answered, those wanting to participate signed a written consent before participating in the focus group and received a copy of the consent form. Women were also informed of their rights to confidentiality and anonymity and could withdraw from the study if they wished to do so at any point. The consents were stored separately from the participant’s demographic information collected with a brief survey and focus group data. Only the first author had access to the list that allowed the identification of the participants. This was essential to protect the privacy and confidentiality of the participants. Before any data collection, The University of Miami Institutional Review Board approval (IRB ID: 20170690) was obtained. Upon completion of the focus group, participants received $40 in compensation for their time.
Members of the research team were trained in qualitative data collection, and focus groups were conducted by the PI of the study with previous experience with qualitative methods. Focus groups were conducted in Spanish, the participants’ preferred language, with an average duration of 60 min. Probes were used to stimulate discussion among participants. Focus groups were audio-recorded with two recorders and conducted in a private space in the community centers.
The research team developed a semi-structured interview guide to conduct the focus groups (Table 2). We used semi-structured questions because this format provides a balance between structure and flexibility, allowing the facilitator to guide the discussion while enabling participants to expand on issues that emerged as important to them (DeJonckheere & Vaughn, 2019). The team ensured consistency using the same interview guide for all participant interviews. The open-ended nature of the focus group questions allowed participants to share their experiences freely, without being constrained by predefined categories. While the categories identified in the analysis have been previously documented in the literature, they were not directly embedded in the interview guide. Instead, the questions were designed to explore how culture and interpersonal relationships influence HIV risk, and participants themselves introduced these topics organically when discussing behaviors that put women at risk. The analysis was guided by existing literature that acknowledges these cultural values, as well as by prior experience working with Latinas. It is important to note that the present analysis includes only the data related to sociocultural factors obtained from the focus groups using the semi-structured interview guide. Other findings from this study, which pertained to participants’ perceptions of and input on the telenovela content, were reported previously in a separate publication describing the development of the telenovela-based intervention (Villegas et al., 2023).
Semi-Structured Question Guide for the Focus Group Interviews.

Audio recordings were transcribed verbatim by a professional transcription service and stored in a locked office, with digital files saved on password-protected computers. Two members of the research team reviewed the transcripts to verify for accuracy and completeness.
The sample size for this study was determined to capture a diverse and meaningful range of experiences relevant to the study aim. In keeping with the qualitative descriptive methodology, our focus was on collecting data that provided sufficient detail, variation, and clarity to describe the phenomenon under study accurately. After conducting four focus groups, the research team agreed that the data offered a comprehensive portrayal of participants’ perspectives and that further data collection was unlikely to yield substantially new information. This decision was based on our commitment to developing a rich and accurate description of the phenomenon, grounded in participants’ voices and experiences and informed by our previous experience working with the population under study.
Data Analysis
A conventional content analysis in which coding categories were inductively developed from the textual data was used for this study (Hsieh & Shannon, 2005). Four research team members, who were not involved in data collection, manually and independently analyzed the transcripts of the four focus groups, reading them to establish familiarity, and conducted line‑by‑line coding, generating initial codes. After reading the transcripts, the four researchers noted that the emergent data naturally reflected patterns consistent with established Latino cultural values, as recognized in prior literature and in their previous experience working with Latinas. In this way, Latino cultural values helped contextualize participants’ narratives without imposing predefined categories or restricting the emergence of new themes from the data (Hsieh & Shannon, 2005).
These preliminary codes were discussed in a research team meeting, during which the overlapping concepts were consolidated and modified accordingly for analysis. Two additional research meetings were held to refine code definitions, merge or split overlapping codes, and finalize the codebook. This process involved reading and rereading the transcripts to ensure consistency and to generate coherent categories and subcategories (Hsieh & Shannon, 2005). The principal investigator (PI) of the study participated in this process to help reach a consensus, ensuring the rigor and quality of the data analysis. Exemplary quotes were chosen to illustrate and support the categories and subcategories.
The analysis was conducted in Spanish, and the results were translated into English by the bilingual team using the forward and backward translation approach. The research team acknowledges that their backgrounds, identities, and experiences shaped their engagement with the study. Comprising individuals from diverse backgrounds, including both Latino and non-Latino identities, the team brought a combination of insider and outsider perspectives that enriched the analysis of sociocultural factors influencing HIV prevention among Latinas.
To ensure rigor, the authors used Lincoln and Guba’s evaluative criteria to establish the study’s trustworthiness (Denzin & Lincoln, 2000). Dependability was supported by maintaining documentation of the analysis via an audit trail consisting of raw data such as direct quotes from the transcripts, drafts of the subcategories created during the analysis process, a codebook, and a code sheet. Additionally, credibility was supported through independent coding of the transcripts by four researchers with subsequent review by the PI, and further strengthened by the authors’ prolonged engagement with the data and the study topic. Assessment of transferability was enhanced by providing detailed descriptions of participant demographics and the study context, allowing consideration of applicability to other Latinas in different settings.
Results
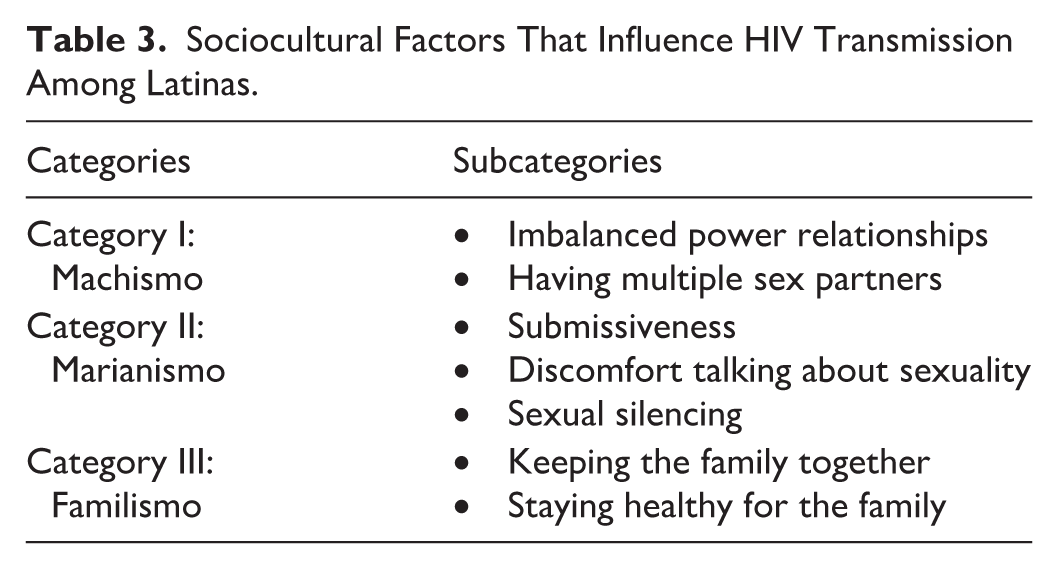
The analysis of the data yielded three categories related to socio-cultural factors that influence HIV transmission: Marianismo, Machismo, and Familismo. Each one of these cultural values had distinct subcategories (see Table 3). All the information presented in this section is based on women’s perspectives on the influence of sociocultural factors that influence HIV transmission among Latinas.
Sociocultural Factors That Influence HIV Transmission Among Latinas.
Machismo
Machismo, a deeply rooted cultural construct in Latino communities encompassing traditional male dominance and gendered expectations, was identified as a salient category in the analysis, shaping relationship dynamics and influencing participants’ HIV risk. This category encompasses two interrelated subcategories: Imbalanced Power Relationship and Having Multiple Sex Partners.
Imbalanced Power Relationship
Participants described issues regarding power imbalance in their romantic relationships. The presence of machismo which has been transmitted from generation to generation in the Latino culture has led to an imbalance of power in the relationship, with men being dominant, taking control over the relationship and decision-making. This affected the couple dynamics by decreasing partner communication and negotiation. One participant exemplified this experience with this statement: The thing is that many families are old-fashioned, like my dad. . . my dad told me that I have to do what my husband says.
This power imbalance has been so ingrained in the Latino culture that women mentioned that men often communicate this message to their children. This imbalance also influenced the idea that certain behaviors are acceptable for men and should be tolerated by women without hesitation. These behaviors are commonly risky and include multiple sexual partners, alcohol and drug use, intimate partner violence, and inconsistent condom use, among others. Fathers also tend to talk to their children in a language that minimizes their ‘daughters’ feelings and power in front of their sons-in-law. A participant described the following situation: My dad once went to drink with my former husband in Mexico and they arrived in the early morning, and I was incredibly angry, incredibly angry. And suddenly my dad told me to calm down, because he is a man, and he can arrive at any time he wants; ‘you can’t because you are a woman. I said ‘ha’, how ironic!
Latinas also emphasized that financial constraints put them in a situation of lower hierarchy with their partners, to the point of perceiving that they lost their autonomy. In some cases, women were not able to work much outside the home because they needed to take care of their children or their partners did not allow them to earn money or work outside the home since men preferred that women remain in a traditional gender role (i.e., housewife, mother). This view of the role of Latinas reinforced the idea of the man as the provider and the woman dedicated to the domestic space. While some Latinas view being a provider as a positive aspect of machismo, as it helped support the family, it can lead to stress and strain in their intimate relationships. Women often felt they lacked independence and were not treated fairly by their partners. In this regard, one participant mentioned: Sometimes, if a woman doesn’t work, a man can say: ‘I work, you have to do everything I say’ - that is, everything, everything. . .’ As if you were the servant of the house. . .You depend on them. . . yes, you become their property.
While power imbalances persisted in their narratives, it is important to recognize instances in which Latinas found ways to protect themselves by seeking alternative pathways to access prevention resources. Even in contexts where their agency was constrained, many participants demonstrated proactive efforts to protect themselves. Despite fear and significant challenges women tried to protect their health. One participant said: Well, when I go to the clinic almost every year, they run tests for everything—diabetes and all that [tests] as well. . . a few months ago, I went to get tested for all of that—for all the diseases, for chlamydia and everything [including HIV]. Because you never know, sometimes, you know. . . the husband might be there at home, and then you start thinking about getting all those tests done.
Having Multiple Sex Partners
A second subcategory derived from the analysis was related to Latina’s partners having multiple sexual partners. They recognized that this behavior has been taught since childhood in men in the Latino culture. It was normalized that if the man is monogamous, some people would question his masculinity and/or sexual orientation. In the Latino culture, it was mentioned the presence of discrimination and stigma against men and their masculinity if they identified as gay. For this reason, Latinas described that several Latino men also felt pressure to engage in having multiple partners to avoid negative comments regarding their masculinity. One participant said: When it comes to Latinos, it depends on how they are raised; Latinos are almost always taught by their parents. If you are macho and you have had a girlfriend since you were a child, the more women you have, the more macho you are. If you have only one, you are lazy [not very masculine], you’re not macho anymore.
Some participants recognized their husbands’ infidelity as a behavior that puts them at risk for HIV and attempted to negotiate condom use. Most of the time, Latinas felt it was difficult to have these conversations with their partners and negotiate safe sex because of the power imbalance in the relationship. Men usually reminded women that they had control and ownership over them. One participant mentioned: I knew he was hooking up with other women and I told him ‘Use a condom or one day you’ll give me something,’’ and he used to answer ‘no, you’re my wife, I don’t have to, I’ll protect myself with others but not with you.’
Marianismo
Marianismo, the cultural norm emphasizing women’s self-sacrifice, purity, and nurturing roles, was evident in focus group data as shaping women’s romantic relationships and HIV prevention behaviors. This theme encompasses three interrelated subcategories: Submissiveness, Discomfort Talking About Sexuality, and Sexual Silencing.
Submissiveness
Submissiveness was described by women as an attitude of adhering to the ‘partner’s decisions and wishes. As indicated in the previous category by women in the groups, Latino men had different behaviors towards women that reflect male dominance and control over them. In such situations, Latinas felt pressured to accept their partner’s decisions, even when they disagreed, to prioritize their partner’s preferences as much as possible. Within the concept of submissiveness, Latinas were often expected to satisfy their partner’s sexual needs and refrain from expressing any negative emotions about sexuality. Some participants feared confronting their partners due to the risk of violence and felt that being submissive could help reduce this risk. For example, one participant described: There are times when a woman submits to her husband. . . Oh no, it’s not that, it’s that he gets angry. . . -Oh, I have to go home now because I have to cook, because he’s going to come, and he is going to be angry- He seems more like a father than a husband now.
Discomfort Talking About Sexuality
Conversations about sexuality were challenging for Latinas due to social expectations that emphasize women’s chastity and purity. Open sexual conversations with parents or their partners were described by Latinas as inappropriate, a threat to the family’s reputation, and an indicator of sexual promiscuity. This cultural norm has been passed down from generation to generation and women usually felt guilty when they tried to talk about it. As a result, Latinas who inquired about sexuality were perceived as promiscuous, resulting in decreased communication about sexuality and the prevention of HIV and other sexually transmitted infections. One participant described her experience: And it’s important [to talk about sexual relationships] because I remember when I was a teenager, I grew up with my grandmother and for her, it was terrifying to talk about those things [sexuality/diseases]. So sometimes one has a bit of ignorance because schools don’t openly talk to you about sexuality or diseases.
Latinas often felt uncomfortable and embarrassed when they needed to talk with their families and romantic partners about sexuality. The lack of information further decreased their confidence in preventing HIV and STIs and reduced their partners’ willingness to discuss these issues. This affects the broader Latino community, as Latinas often raised their families without openly discussing sexuality. Many did not know how to talk about it or what questions to ask. Another participant provided her insight: Everyone feels embarrassed to talk about it [sexuality]. . . Because there is no [way] to speak openly, they haven’t received information to prevent a disease [HIV or STIs]. . .actually, it is necessary to be informed.
Sexual Silencing
Marianismo often led to silencing in regard to sexuality. Sexual silencing was described with different words by women that indicated that they felt it was prohibited to speak about activities connected with physical attraction and/or intimate physical contact (i.e., condom use). This prohibition led to a conscious suppression from Latinas to discuss these issues. Sexual silence was mostly related to fear of the ‘partner’s reaction rather than to feeling discomfort when talking about sexuality. This blocked any negotiation or discussion regarding critical categories such as sexual protection. For instance, participants explained: If you tell them [male partners] ‘Use a condom,’ they get angry and if they get angry, they don’t want to know anything. How long does their anger last? until they’re satisfied. There are some who have to do it without a condom because their husband got angry or not, it’s a topic that can’t be touched [discussed]. I have a friend who doesn’t speak it [sexual matters], for the same reason that her partner is macho, and she can’t speak [about it], she can’t say. Maybe you think or suspect that he is up to something and you ask him, then he says, “Oh, it’s you who’s doing it.” So, they turn it around on you, so it’s better to keep silence.
Sexual-silencing also influenced preventive HIV behaviors due to the fear of the ‘partner’s reaction. Another participant illustrated sexual silencing by describing her friend’s experience: She would tell me, -If I want to ask something about a disease or something, he would say, ‘Why do you want to know?. . .’- so she says, I’m afraid to ask or go to a clinic for that reason, - because he would forbid her.
In addition, one other participant narrated her experience with her husband. This case, reflects how women also abstained from communicating because they perceived that their partners were not in the mood or that communicating their needs to their partners because this was not perceived as a priority: Because you don’t know how to tell him. Well, at least I’ve been married for 21 years and sometimes I don’t talk about things that I want to discuss with him, because he doesn’t want to, because he doesn’t feel comfortable, because he’s tired, because he wants to watch TV. You can’t talk to him.
Familismo
Familismo, the cultural value emphasizing family unity, loyalty, and responsibility, played a central role in shaping participants’ decisions and behaviors related to HIV prevention. Two key subcategories are part of familismo: Keeping the Family Together and Staying Healthy for the Family.
Keeping the Family Together
Participants mentioned the importance of keeping the family together as a priority in the Latino culture. Keeping the family together and protecting their children’s needs were prioritized by women at all costs, even with mistreatment from their partners. Women described as the primary caregivers in the family. Further, financial stability was a key concern for these women, who often felt they needed to stay in the relationship to ensure their children’s basic needs were met. One participant illustrated this fear with the following statement: Sometimes they [women] let them [men] mistreat them [women] that way for fear of being left alone because [women think] ‘I will not be able to make ends meet, and that if I do this, he’s going to leave me, and if I report him, they [police] are going to take him, and I’m going to stay alone with the children.’
Staying Healthy for the Family
Some Latina women in this study expressed positive attitudes and willingness to engage in HIV and STI preventive behaviors when thinking about the well-being of their family, especially their children. They were driven by an intense sense of responsibility and commitment to their families. One participant suggested that she was willing to pay for health prevention, regardless of cost, to protect herself and consequently her family: There are low-income clinics that charge you 35-25 dollars, and you have a general checkup, I don’t know, some tests, it’s 20 dollars, 25 dollars for blood or urine. . . In other words, you really shouldn’t give up because you say, “oh, they charge me 300 dollars”, and if that were the case, you have to do it because your children also depend on you. So, imagine if you don’t get cured, then?
Latinas felt the need to have open conversations about sex and sexual preventive behaviors with younger family members. Despite the challenges of discussing sexual issues, new generations were increasingly willing to initiate these conversations. Topics of conversation included disease prevention and condom use, as one participant explained: I have brothers and sisters; I always, yes, I always speak clearly [about sexuality], more to my brothers. I speak clearly to them because that is – I tell them, “If you are going to mess with someone, or whatever, use a condom”; I speak clearly to them because I am already informed a little bit.
Another participant described how she spoke with her children about sexuality, even though doing so felt embarrassing and placed her in an uncomfortable position. Her willingness to engage in this conversation to prevent HIV and protect her children’s health reflected an act of care and guidance that underscores the family’s role as a key source of support and education.
I have a 17-year-old and a 12-year-old, and they watch La Rosa de Guadalupe [a popular soap opera in Latin America] a lot. . . they started to find out things [through the soap opera]. . . I always say [to myself] ‘Do not tell them everything directly because they are still young’. . . but I do talk to the older one. . . since my son already has a girlfriend, I told him, even though it was embarrassing, I said, ‘Look, I would rather you come to me and say: “Mom, give me money to buy condoms,” than for you to get infected or get someone pregnant right now, you need to focus on your studies.’ So, I came to him and gave him some [condoms], and he said, ‘What’s this?’ And I was like, ‘Don’t play dumb.
Discussion
This study makes a unique and timely contribution to the field of HIV prevention by capturing how Latinas interpret and navigate evolving sociocultural norms such as machismo, marianismo, and familismo. Building on evidence that family dynamics and cultural norms shift across developmental stages and in response to broader societal changes (Roche et al., 2022), this research explores how recent transformations among Latinas, such as increased educational attainment, labor force participation, and access to digital health information, have reshaped sociocultural influences on HIV prevention. The results showed continuity as well as change in behaviors and beliefs over time. Our findings highlight the complex role of these sociocultural factors, which can reinforce gendered power dynamics, limit open communication about sexuality, and constrain women’s autonomy in negotiating safer sex practices. At the same time, these cultural values can motivate Latinas to protect themselves by seeking information, prioritizing their families’ well-being, and asserting their right to health. Several of these protective behaviors were shaped by new forms of communication such as popular media like soap operas or by shifts in family communication dynamics, which opened space for more open and culturally grounded conversations about sexual health and HIV prevention.
In examining the category of marianismo, it becomes apparent that this concept significantly shapes power dynamics and communication within Latin relationships. Marianismo influences Latinas’ perceptions and experiences, shaping their decision-making and relationships. The literature consistently shows that submissiveness and challenges in discussing and learning about sexual health with one’s partner affect women’s ability to exercise agency and prioritize their sexual health and self-care, placing them at increased risk for HIV (Cianelli et al., 2015; Goodwyn et al., 2024; Ravelo et al., 2022).
Latinas often silence themselves—whether in response to requests for condom use or general conversations about sexual health—due to fear of their partner’s reactions, accusations of infidelity, or potential violent retaliation. This is concerning for two main reasons: first, women are deprived in taking control of their sexuality, even when aware of the risks associated with unsafe sexual encounters; second, the implicit and ever-present threat of violence that also shapes women’s choices. Baeza et al. (2024) described how the constant threat of violence increased Latina’s awareness of the power imbalance in relationships and reinforced the perception that they do not have a choice in sexual matters, eventually making them less likely to assert sexual boundaries with their partners. Goodwyn et al. (2024) and Ravelo et al. (2022) report that even when women may be aware of the sexual risk and have a strong HIV risk knowledge, they will not be able to use it due to their submissive position and fear of partners reaction. Latinas prioritize their partner’s preferences, even at the expense of their own needs and desires, and prefer to engage in self-silencing (Baeza, 2023). Consequently, this sexual silencing emerges as a formidable barrier, depriving many Latinas of the essential dialogue needed to negotiate sexual health and assert their desires.
Findings from the study support that machismo is a significant socio-cultural risk factor for HIV among Latinas. Traditionally, Latinas are seen as the homemakers and the men as the financial providers. Women have reported this financial imbalance forced them to remain in relationships where they had less power (Cianelli & Villegas, 2016). This power imbalance results in difficulties in negotiating condom use and feeling pressured into their partner’s sexual desires resulting in increased vulnerability to HIV (Teitelman et al., 2010). It has been shown that interventions that address machismo increase HIV knowledge and prevention, as well as improve sexual health communication between partners (Cianelli et al., 2024). This suggests a potential pathway for reducing gender-related health disparities in this population.
Traditional Latino masculinity often promotes attitudes that normalize infidelity as a demonstration of virility (Boyce et al., 2016). Similar to other studies, participants discussed that masculinity was often tied to the number of sexual partners men have (Villar-Loubet et al., 2011). This concept and perception of masculinity is ingrained from an early age in a man’s life and is accepted by Latinas. By addressing gender norms and power dynamics within relationships, interventions may help mitigate the cultural factors that contribute to health disparities among Latina women.
While familismo fosters strong family bonds and support networks, it can also contribute to Latina women remaining in dysfunctional or unhealthy relationships due to the prioritization of the family unity over personal well-being (Cianelli et al., 2015; M. M. Hernández & Bámaca-Colbert, 2016; Ramírez-Ortiz et al., 2020). Familismo can reinforce machismo and lead to women tolerating IPV and prioritizing family financial stability over their safety. However, consistent with our study findings, the deep sense of responsibility Latina women feel toward their family, particularly their children, often motivates them to seek preventive health measures, including HIV and STI testing (Ramírez-Ortiz et al., 2020).
Familism also creates opportunities for open communication about sexual health across generations despite cultural taboos (Da Silva et al., 2021). Studies have also shown that interventions among Latinas incorporating a strong family component—such as those that engage partners, children, or extended family members—tend to be more effective in addressing health disparities, including HIV prevention (Sanchez et al., 2019). Familism may also encourage Latina women to have open conversations about sex and sexual preventive behaviors with their partners as well as with younger members of their families. Familism can serve as a protective factor against risky sexual behaviors by fostering family cohesion, open communication, responsibility, emotional support, stigma reduction, and strong support systems (Cabral et al., 2023). In Latino families that embody familism, older family members are highly respected and serve as role models. Younger members are more likely to adopt health-conscious behaviors and pass these practices down through generations (Cabral et al., 2023). Therefore, familism can play a crucial role in shaping future interventions that promote safer sexual health practices within Latino communities.
The findings from this study underscore the importance of developing culturally tailored HIV prevention interventions that address the unique socio-cultural factors influencing Latinas. Nurses and healthcare providers can enhance interventions by incorporating culturally appropriate educational materials, such as innovative storytelling that reflects socio-cultural factors (Villegas et al., 2023). This approach might foster open discussions about sexuality, promoting greater engagement and understanding.
Furthermore, our findings advance culturally sensitive practice by supporting the integration of patient-centered communication into HIV prevention efforts. From a scholarly perspective, this study addresses a gap in qualitative research by centering the voices of Latinas, particularly in Florida, where recent demographic shifts and migration patterns have introduced new public health challenges. Our work contributes to science, education, and policy by providing culturally grounded evidence on how health care workers can tailor preventive care, foster trust, and enhance HIV prevention in culturally diverse communities.
Finally, although this qualitative descriptive study was not designed to develop or test theory, it is important to highlight that the findings of this study conceptually align with elements of the Socioecological Model (Bronfenbrenner, 1979) and Gender and Power Theory (Connell, 1987). The results illustrate how evolving cultural norms and gender dynamics shape HIV-related behaviors among Latinas, suggesting that future intervention research and studies using theoretical frameworks focused on individual behavioral change should also integrate these sociocultural dimensions into their design.
Limitations
This study has limitations including the use of self-reported data that may have introduced biases, as participants may have underreported or over reported their experiences due to social desirability (Latkin et al., 2017; Rao et al., 2017). This study focused on Latinas residing in South Florida, meaning the findings may not be fully transferable to Latinas in other parts of Florida or the U.S. South Florida’s cultural diversity and high HIV prevalence may uniquely shape Latinas’ perceptions and experiences with HIV. Another limitation is that participants were unfamiliar with PrEP, which may restrict their ability to reflect on how cultural values influence perceptions of HIV prevention.
While focus groups can present limitations, such as the potential for dominant voices to overshadow quieter participants or for individuals to withhold divergent views due to social pressure, they also offer unique advantages. In this study, the group setting fostered a sense of shared understanding and trust among women, which encouraged openness. This dynamic is especially meaningful within Latino culture, where communal dialogue and shared experiences often promote connection and validation. The group size was adequate to promote dialogue and enough interaction about sensitive topics. Many participants felt that their experiences were not isolated, and the possibility that others in the group might relate to their stories gave them confidence to speak candidly. This collective environment enriched the data by surfacing common categories and validating lived experiences, even as researchers remained mindful of the need to balance group consensus with individual nuance.
Conclusion
The findings highlighted power imbalances in Latinas’ intimate relationships, shaped by key socio-cultural factors that continue to influence their sexual health behaviors. While several views show that these factors affect prevention negatively, Latinas also demonstrate agency and resilience by finding ways to protect themselves whether through seeking information, prioritizing the health of their families, or negotiating safer sexual practices despite cultural and relational challenges. The findings highlight the dual role of cultural norms, as both obstacles and opportunities, in HIV prevention efforts and underscore the need for culturally tailored HIV prevention interventions that address the unique socio-cultural influences affecting Latinas.
These results have important implications for practice, policy, and future research. Practitioners and policymakers should consider the relational dynamics, gendered power imbalances, and cultural expectations that shape Latinas’ experiences, rather than focusing solely on individual-level behavior change strategies that overlook the broader cultural context. Future research and practice should prioritize culturally informed ethical safeguards and advocate for policies that recognize and address the structural and sociocultural determinants of HIV vulnerability among Latinas. Strategies should include integrating culturally relevant narratives into health education, promoting community-based dialogue that validates women lived experiences, and supporting interventions that foster empowerment and self-efficacy. Latinas. It is essential that future research includes Latinas and examines how they perceive the influence of cultural norms across contexts. This study contributes to that effort by demonstrating the value of participatory approaches that engage Latinas in the design and evaluation of prevention programs, ensuring interventions are both culturally responsive and community-driven.
Based on the knowledge acquired through this study, we were able to design a culturally tailored soap opera intervention that addressed HIV risk by incorporating Latina’s perspectives presented in this study reflected on character’s relationship dynamics, conflict, and power disbalances in an intimate relationship (Villegas et al., 2023). This narrative approach reflected the lived realities of Latinas and served as a powerful tool to empower and potentiate women’s agency in preventing HIV. By embedding prevention messages within familiar and emotionally resonant storytelling formats, such interventions can enhance engagement, promote critical reflection, and encourage behavior change. This model offers a promising strategy for future initiatives aiming to reduce HIV risk while honoring the cultural identities and strengths of Latina communities.
Footnotes
ORCID iDs
Author Contributions
The authors contributed to conceptualization, methodology, data curation, formal analysis, investigation, validation, writing (original draft, review and editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a CFAR pilot award. The Miami Center for AIDS Research (CFAR) at the University of Miami, Miller School of Medicine is funded by a grant (P30AI073961) from the National Institutes of Health (NIH), which is supported by the following NIH Co-Funding Participating Institutes and Centers: NIAID, NCI, NICHD, NHLBI, NIDA, NIMH, NIA, NIDDK, NIGMS, FIC, and OAR. Research reported was also supported by the National Institute on Drug Abuse (NIDA) of the National Institutes of Health under Award Number R34DA053887. The content is solely the responsibility of the authors and does not necessarily represent the official views of the School of Nursing, University of North Carolina at Chapel Hill and the School of Nursing and Health Studies at the University of Miami.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.