
Abstract
With the physical and mental impacts of caregiving being well-documented, there is an emphasis on creating interventions to support family carers and enhance their wellbeing. Many of these have been shifting toward accessible, web-based interventions. My Tools for Care (MT4C)-In Care is a self-administered, web-based intervention for carers of persons living with dementia residing in long-term care (LTC). The objectives of the current study were to understand the acceptability, usability, and usefulness of the MT4C-In Care toolkit. Using qualitative description, semi-structured interviews with family carers (n = 39) were completed across Canadian study sites in four provinces. Interviews were analyzed using deductive content analysis. Participants found the toolkit to be a suitable and adequate tool to support them as carers of persons living with dementia residing in LTC. They also perceived the online format easy to use, although there were barriers, outside of the intervention, to using the tool. The perceived usefulness was described by participants in three ways. The toolkit: (1) validated and normalized feelings, (2) provided permission for self-care and mental well-being, and (3) strengthened their caregiving knowledge. The MT4C-In Care interactive toolkit provided support that participants perceived as acceptable, easy to use, and meaningful.
There are approximately 55 million persons living with dementia worldwide, with the global prevalence projected to double by 2030 and nearly triple by 2050 (World Health Organization [WHO], 2023; World Health Organization & Alzheimer’s Disease International, 2012). Along with this rise, the demand for caregiving will increase. When a person becomes a caregiver, they begin a journey of highs and lows which impact their everyday life and well-being. In the context of caregiving, well-being encapsulates quality of life, in addition to intrinsic emotions, feelings, and beliefs, and extrinsic factors, such as beliefs about others’ emotions (Ford & Gross, 2018; Gibson et al., 2019). Family carers (hereafter referred to as carers) of persons living with dementia experience lower mental and physical health in comparison to individuals who do not have caregiving roles making them a vulnerable group (Rigby et al., 2009). Thus, many carers are at risk for caregiver burden, a global concern, as it profoundly affects carers of persons living with dementia (Fong et al., 2022; Gurayah, 2015; Ong et al., 2022; Smith et al., 2022; Torti et al., 2004).
Carer burden is a public health issue as it is linked to illness, depression, and decreased quality of life (Monteiro et al., 2024; Nasreen et al., 2024). Likewise, carer burden impacts well-being because it manifests from the carer’s perception of stressors and activities, which is impacted by “psychosocial factors such as kinship, context, and culture” (Etters et al., 2008, p. 424). This burden increases over time if carers are unable to access services, further underscoring the need to alleviate inequities related to the carers of persons living with dementia accessing resources early and for as long as possible (Connors et al., 2020; Gibson et al., 2019). Previous research acknowledges carers’ vulnerability and highlights a myriad of interventions, such as counseling in-person or via telephone, cognitive behavioral therapy, group therapy, being visited at home by a healthcare professional, or a combination of these (Elvish et al., 2013). Although interventions delivered in-person or by a professional, facilitator or other kind of interventionist are fruitful, barriers such as time, finances allocated away from caregiving, and requiring the carer to travel to support group locations perpetuates inequities to accessing support (O’Connor et al., 2014). It is imperative for inequities to be addressed to ameliorate the well-being of diverse carers of persons living with dementia.
Web-based interventions increase accessibility as they are cost effective and do not require commuting (Rottenberg & Williams, 2021). Carers have reported they would recommend web-based interventions to friends because they are comparable to in-person methods (Camateros & Vézina, 2016). Previous research demonstrates that web-based interventions reduce depression and anxiety among carers of persons living with dementia but are limited in facilitating enhanced coping and a reduction of emotional pain (Zhao et al., 2019). Similarly, more extensive literature reviews assert that technology-based interventions offer high flexibility and availability particularly to individuals in rural communities, which reduced feelings of caregiver burden (Deeken et al., 2019). Further, web-based interventions have been found to enhance self-efficacy (Bruinsma et al., 2021). Altogether, current research seeks to understand how the efficacy of web-based interventions can be optimized to enhance the scope of care for carers. To optimally respect the overarching goal of web-based interventions, which is to enhance the well-being of carers, it is essential to determine feasibility in addition to accessibility for alleviating inequities to services (Duggleby, Jovel Ruiz et al., 2018).
My Tools for Care-In Care
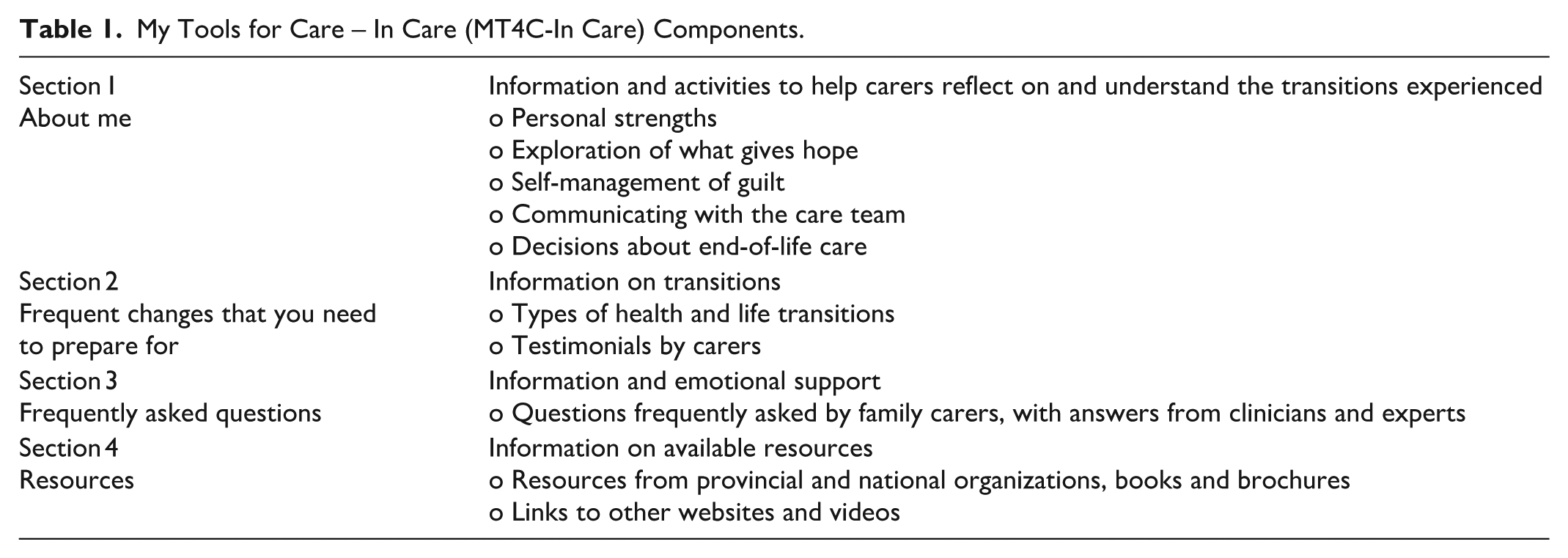
My Tools for Care (MT4C), a self-administered web-based psychoeducational intervention developed to support carers of community-living persons with dementia, was found to increase hope (Duggleby, Ploeg et al., 2018). Considering carers of persons living with dementia residing in long-term care (LTC) homes share common experiences with those carers of community-dwelling persons living with dementia, the MT4C online intervention was adapted for use with carers of persons living in LTC (Duggleby, Jovel Ruiz et al., 2018). This adapted interactive site, titled My Tools of Care-In Care (MT4C-In Care), includes: (a) a guided journaling section called “About Me,” (b) information on common changes to expect with dementia and care needs, (c) frequently asked questions, and (d) resources with contact information and links to other relevant websites. See Table 1 for a description of the various components of MT4C-In Care.
My Tools for Care – In Care (MT4C-In Care) Components.
Preliminary results demonstrated that MT4C-In Care was feasible, acceptable, and easy to use (Duggleby, Jovel Ruiz et al., 2018), and it has been found effective to promote social support as compared to an educational control in a randomized trial (O'Rourke et al., 2025). The purpose of this paper is to understand the acceptability, usability, and usefulness of the MT4C-In Care interactive toolkit through the perspectives of the participants in the intervention arm of a trial (Duggleby, O’Rourke et al., 2020; Duggleby, Peacock et al., 2020). For our analysis we used the following definitions: (1) acceptability is the receptiveness of the consumer to utilize the intervention for what it is intended to achieve (Dillon & Morris, 1996) and is comprised of the individuals’ feelings toward the intervention, and the perceived effort required (Sekhon et al., 2017); (2) usability refers to the ease of use (Boceta et al., 2019); and (3) usefulness is defined by the consumers’ belief using the tool will increase some performance or function (Dillon & Morris, 1996).
Methodology
This qualitative study is part of a larger, pragmatic mixed methods randomized control trial. Following adaptation of the intervention to address social support and loneliness, the aim of the larger study was to evaluate the effectiveness of the MT4C-In Care online intervention and is described in the original protocol (Duggleby et al., 2017). The current study incorporates the findings from analyzing qualitative interviews with carers (n = 39) who used the MT4C-In Care online toolkit over 2 months during the pragmatic trial to better understand the usefulness and acceptability of the tool.
To guide the current study, we undertook a qualitative description approach (Sandelowski, 2000, 2010). Qualitative description is well-suited to mixed methods studies, provides a straightforward description of the phenomenon using the viewpoint of participants by staying close to the data. Using purposive sampling, interviews, and content analysis to glean an understanding of participants’ real-world contexts reflects the principles of qualitative description that we pragmatically employed. In the case of the current study, we endeavored to understand the acceptability, usability, and usefulness of the MT4C-In Care intervention to increase its benefits for carers. We strove to answer the questions:
How acceptable is the MT4C-In Care intervention for family carers of a relative with dementia living in a LTC home? Is it a suitable and adequate tool to support them?
How usable is the MT4C-In Care intervention for family carers of a relative with dementia living in a LTC home? Is it easy to use?
How useful is the MT4C-In Care intervention for family carers of a relative with dementia living in a LTC home? Does it add value to the user?
Setting and Sample
The participants for the larger study were recruited in a variety of ways, including partnering with local Alzheimer Societies, older adult LTC homes, and advertising in newspapers; this is described in detail elsewhere (Duggleby et al., 2017). Participants for the qualitative interviews were selected purposefully from the intervention group based on demographic characteristics to ensure the sample had theoretical sufficiency (Tight, 2024). Recognizing the different population sizes in each province, we aimed to interview 15 participants in each of Ontario and Alberta, and five participants in each of Manitoba and Saskatchewan, for a total of 40 interviews. Participants were selected from the intervention group as they needed to have access to the toolkit and had used it prior to responding to the interview questions. Initially, the goal of recruitment was to seek variation according to carer gender, carer age, carer ethnicity, relationship, and the stage of dementia of the resident, but recruitment challenges during the COVID-19 pandemic, participant withdrawals, and not always using the toolkit created a need to be less selective to reach our target sample size. Additionally, difficulty with recruiting participants from several provinces, and several withdrawals from the intervention group, created a need to over-sample from Ontario to reach the intended target. Our final sample size included 39 participants.
Data Collection
The identified participants were asked to complete a qualitative interview using a semi-structured interview guide during their 2-month follow-up audio-recorded phone call by trained research assistants. The interview questions were developed by the research team reflect the research aims, and piloted by research assistants within each province during research assistant training, prior to their use with participants in the study. For purposes of the current study, we focus on the questions related to the usefulness of MT4C-In Care. This included questions about what participants were thinking when they used the tool, if they felt the toolkit supported them in the ways they dealt with changes and loneliness, or if the toolkit promoted social support, hope, self-efficacy or quality of life and in what ways. We also considered the parts of the toolkit participants was helpful and if not, how we could best adapt it to make it more so.
As part of the larger study, research assistants at each of the pan-Canadian study sites completed data collection (baseline, 2 months, and 4 months) with the participants which included the collection of quantitative measures: quality of life, self-efficacy, hope, loneliness, grief, and perceived social supports. Qualitative interviews occurred following the 2-month data collection phone calls and consisted of open-ended questions regarding their experience with the tool. The interviews lasted approximately 20 min. Audio-recordings were uploaded to a secure site and transcribed by an experienced transcriptionist who signed a confidentiality agreement.
Data Analysis
The interview questions (related to the usefulness of the tool) provided structure to deductively analyze the transcripts using content analysis (Hsieh & Shannon, 2005). Directed content analysis supported the description which sought to understand the acceptability, useability, and usefulness of the MT4C-In Care tool. After research assistants cleaned the transcripts, the first step of analysis involved reading and rereading the transcripts to get a sense of the participants’ experiences when using the tool. Operational definitions of key terms—useability, acceptability, and usefulness—were developed to support the initial coding. Using three transcripts, four research team members (two experienced qualitative researchers and two novice research assistants) independently highlighted any text that represented the predetermined key terms, this text was then coded. Text that did not fit one of the predetermined key terms was retained and labeled separately (to be considered later). The team then came together to compare initial coding and develop a codebook. Subsequent coding was undertaken by the two research assistants who each coded half the transcripts, with any questions or concerns brought to the team for discussion. The resulting codes were then subsumed under the appropriate category. Frequent team discussions and consensus building was done throughout the analysis process to ensure analytic rigor. Data management was done with an Excel spreadsheet to capture the codes and categories.
Trustworthiness
The current study adhered to standards to ensure rigor and trustworthiness. For instance, across the research sites, the same semi-structured interview guide was utilized; the same research assistant(s) contacted and interviewed the participants at each site for consistency in data collection. Data collection and analysis occurred simultaneously to ensure data being collected reflected the intent of the study. Research team meetings occurred monthly, and concerns were discussed among members to support the research assistants. These meetings were vital to shared communication and facilitated data analysis in order to support the project’s integrity.
Reflexivity: Disclosures of positionality and incorporating the ongoing practice of reflexivity for the academics and researchers on our team were employed to bring humanity and greater awareness within our research. In making our cultural assumptions explicit by acknowledging Eurocentric academic traditions, paternalistic healthcare practices, ageism, sexism, and ableism, we are taking steps toward actively challenging unconscious biases camouflaged in otherwise well-intentioned research.
Ethical Considerations
Prior to initiating the study, ethical approval was obtained from Research Ethics Boards in each province (University of Alberta Health Research Ethics Board (#Pro00090771); University of Saskatchewan Research Ethics Board (#1385); University of Manitoba Education/Nursing Research Ethics (E2019:127), and the Hamilton Integrated Research Ethics Board (#7659)). In the current study, verbal consent was obtained prior to each interview and interviews were conducted at a time that was convenient to the participants.
Findings
To understand participants’ views on the MT4C-In Care toolkit, data were analyzed to assess their perceptions of its acceptability, usability, and usefulness. The majority of participants were female (84.6%), married (69.2%), and living in an urban setting (59.0%), with a majority (51.3%) reporting annual income of $70,000 per year or more (and 12.8% who did not report their annual income). The sample was not ethnically diverse, with the majority being White (89.7%); the remaining participants in the sample included individuals who identified as having Chinese (n = 1), Middle Eastern (n = 1), and Indigenous/ Métis ethnicity (n = 2). The most common relationships toward the care-recipient were an adult child of a person living with dementia (64.1%) or a spouse (28.2%). The majority of carers (61.5%) were living with one or more chronic conditions, and well over half had previously used online resources (69.2%). The care-recipients of this population were mainly female (66.7%). The most common stages of dementia were late stage (48.7%) or middle stage (30.8%). The following is a presentation of the findings according to these categories, with supporting verbatim quotes from the participants that reflected the tool’s acceptability, usability, and usefulness. See Table 2 for more details of the participants. Our findings related to the three main categories of acceptability, usability, and usefulness are described below.
Demographics of Qualitative Interview Participants (N = 39).

Acceptability
The participants used MT4C-In Care as it was designed to be used—a key component of acceptability (Bowen et al., 2009; Dillon & Morris, 1996). To understand acceptability, perceptions of the MT4C-In Care Toolkit as a suitable and adequate tool to support carers of persons living with dementia who reside in LTC were assessed. A key goal of the MT4C-In Care intervention is to increase carers’ hope, social support, and general self-efficacy, decrease their grief and loneliness, and to improve their mental health and quality of life. In this way, participants identified that, for those who may have experienced challenges in this regard, MT4C-In Care would be of great benefit: Someone who has a lot of issues in their life or has a hard time coping with all of the stressors that they’re having to take over in their life - they might find this more comforting to read through some of this stuff and be comforted by it [23]
In particular, participants commented that MT4C-In Care would be highly acceptable for those carers who have just had their family member living with dementia move into the LTC facility; a transition that is fraught with emotions: “people who have just had someone admitted to a nursing home I think would be – I think it would be a wonderful tool for them. And I guess that would be my main focus” [238].
Part of this acceptability came from the provision of resources and stories that captured carers’ experiences. However, many participants commented that even more resources could be added to the toolkit to provide further support, particularly for those who had been carers for a long time: “I would say the part I like best is that, again, the prompts of like, what to think about and the resources that were available. . .I think that there’s more resources that can be added to it [277].” Moreover: It’s kind of superficial and again, it’s only for [a] beginner. There’s other more advanced resources or questions for advanced caregiver. Those who have been there for a long time. Such as life after death, palliative but grief, you know, I don’t think there’s an area on that, right? [244].
While many participants’ comments reflected the acceptability of the online nature of MT4C-In Care, it is notable that for some, it did not replace face-to-face connections: I understand that there’s this thing online. But that doesn’t translate into there actually being something at the assisted livings or long-term cares or wherever to help the people adjust, right, or to help families at all. And so, yeah, doing the stuff online sort of is – better than nothing. . . But it – it doesn’t translate into actual action that seems helpful [08].
Usability
In assessing perceptions of usability, data were examined for participants’ descriptions of their ease in using MT4C-In Care. The online format of the toolkit was seen as easy to use with most participants commenting that “It’s simple. It’s easy to navigate” [35], “the fact that it was online made it really, really convenient” [206]. The toolkit was identified by many as being user friendly: “It was user friendly. I really like things that are user friendly, like you don’t have to click a million places. And it saved my answers. So that was good. And I could go back [518].” However, while the online nature of the toolkit both contributed to its usability by being conveniently accessible and easy to navigate, it could also be a drawback for those who preferred to complete the writing exercises in a paper and pencil format: Sometimes I would prefer to work on paper as opposed to on the computer and I did try to run it off but I found that it only gave me one page at a time or that it was too time consuming for me to run it all off so I just didn’t bother [238].
Being online allowed participants to access the program anytime, however, for some, being in front of a computer was not how they wanted to spend their time: It’s extra time I would say. Because you know, I work from nine to five and I went through the kit in the weekend but in weekend I would rather not be spending my time on this toolkit online. I would rather do some other relaxing activities, you know. So, this is – this toolkit is pretty intensive and need a lot of time, sitting and doing paperwork, which I would not prefer to do [244].
For others, an online toolkit felt limited in its usability due to the personal nature of the content, and the motivation it required to complete. One participant commented that: “not everybody can put their feelings, you know, on a computer. . . it’s too personal” [222], while another summed it up by stating: “time, energy, and motivation. . . I think what I felt that I was – I had, given my permission or okay to be part of this survey and then it seemed like there was one more thing that I had to do [513].” Usability, in particular, seemed to have a gendered component with males noting that the writing and reflection activities may not have resonated with them as much: The other is just a personality thing. . . a lot of things were. . . I’d say like more personal in nature and touchy feely. . . I found that a lot of the exercises and things that were going there didn’t match that sort of personality [18].
Usefulness
Participants provided many descriptions of their perceived usefulness of MT4C-In Care; that is their belief that using the tool would increase their performance in some regard or their ability to function (Dillon & Morris, 1996). Overwhelmingly, the usefulness of the tool was seen first, to validate and normalize carers’ feelings, second, to help give them permission to focus on their own self-care and mental well-being, and finally in helping to strengthen their caregiving knowledge.
Validation and Normalization of Feelings
For many carers, caregiving was described as a lonely experience and one that left them feeling uncertain about whether what they are experiencing is normal. Participants expressed, when using MT4C-In Care, it helped to validate that they were not alone in their journey: “I liked the confirmation of feelings and problems. . . That you don’t feel alone or that you’re experiencing things differently than what you should [229].” Participants indicated that the direct quotes from carers contained within the tool helped them to not feel alone, they could identify with the quotes and note others (e.g., those who aided in developing the tool) experienced similar circumstances.
In many instances, the toolkit helped to normalize their experiences and the questions they had about what the person living with dementia was experiencing and their reactions to it. By using MT4C-In Care, carers felt supported. For example, one participant indicated: “I think some of the questions, the answers to the questions—I mean, a lot of the questions I have are exactly the same questions other people have” [519] Another participant stated: “[it’s] nice to know you’re not going through different things alone like you know you’re not the only one experiencing difficulties my wife’s having or I’m having [238].
These feelings of support and validation also extended to the decisions carers had made and the coexisting emotions that had gone with those choices. As one participant aptly stated: “I think it reinforced some of the decisions. It just validated a lot of my thoughts and concerns that, you know, I’m not the only whack job in the world that, you know, some of these things are normal [515].”
Permission for Self-Care and Mental Well-Being
MT4C-In Care was useful in helping participants realize their own well-being was important, something that can be a challenge for carers. Too often, carers felt they could not give themselves permission to take time for themselves as they always need to do things for the person living with dementia. As one participant stated: I think that’s where the hope is. What I’m doing is enough. I don’t have to keep doing more and more and more and more at the expense of myself. You know, there are, I think, the right to set boundaries. I think that’s sort of reinforced in there, too [35].
In this way, the usefulness of MT4C-In Care was seen as supporting and giving carers permission to think about and act on their own well-being: “the other section I actually really liked was ‘what am I doing for myself today?’. . .it’s really good to see it in writing from another source. Because as a caregiver, you often feel guilty about doing that stuff [06].”
By providing an opportunity for participants to think about their role in caregiving and the importance of their well-being, insight and reflections on their own emotions and feelings often occurred. MT4C-In Care showcased the significant role and impact carers have on the caregiving experience: I think what I liked about it, that one section ‘About Me’. . .You have an opportunity to kind of go through that and go, hey, wait a minute. I’m not insignificant in all of this. It’s meaningful that I understand what I’m all about. . . What are my strengths, my values, what do I bring to the table? It changes your whole perspective in terms of how your next steps should be [218].
In some cases, by providing a forum for reflection, participants realized they needed more support; For one participant, this positively translated into them reaching out for further support; something they had never done in the past: “So, I actually called the social worker twice in the last month. And that was—I would have never done that. So, the toolkit certainly supported me in making sure that I look after myself too [270].” Even as an online tool, the acknowledgment of this need for support is invaluable; since caring is complex, so too will the supports be that aid carers.
Strengthening Caregiving Knowledge
While MT4C-In Care validated that carers were doing the best they could and that they have a significant wealth of knowledge, the usefulness of the toolkit was also seen as providing additional tips around how to provide further care to the person living with dementia in the context of LTC. In some instances, this helped carers understand the changing nature of dementia and some of the coexisting behaviors that may occur: “It’s helped me to understand, like, what her situation is, and why she reacts the way she does sometimes. And it’s also taught me to try and look for. . .try to avoid triggers [276].”
In others, MT4C-In Care provided information on how to further engage with their family member: “I found the tips for visits good because I have my little thing that I’ve built up but I’m always open for more. It’s difficult to talk to somebody like that for a long period of time [07].” Overall, participants noted that the usefulness of MT4C-In Care would enable them to be better carers as summed up by the following participant: I think I was thinking about how—how best to use these tools to take care of myself so that I can be a caregiver to my mom. Like how to, you know, to use them effectively and efficiently, and to just be really honest and reflective, so that by doing them, that I could gain more insight into myself so that I could be a better caregiver for my mom [53].
Discussion
This study fills a significant gap in our understanding of carer’s views on the acceptability, useability and usefulness of a web-based psychoeducational intervention. There is a paucity of psychoeducational interventions, delivered in-person or web-based, aimed at carers supporting people living with dementia in LTC and this study provides important preliminary evidence of the value of a web-based intervention. Given the lack of web-based psychoeducational interventions for family carers within LTC, it is difficult to draw comparisons to support our study findings. However, the few studies that have been found confirm that carers of people living with dementia can experience benefits from web-based interventions (Hopwood et al., 2018) including their ability to address loneliness in carers (Davies et al., 2020). Still, we must be cautious in focusing solely on the developing of on-line resources given the risk of creating disparities in who can access these resources based on their economic capacities.
Acceptability
Acceptability of the MT4C-In Care tool related to its aim of supporting carers with the transitions they face when their relative with dementia lives in LTC. Hirschman and Hodgson’s (2018) review emphasizes the importance of additional research regarding the transitions that carers of people living with dementia experience; however, little research has been done on web-based interventions, including specific to the LTC setting. This was confirmed in a recent scoping review by Groenvynck et al. (2022) in which none of the interventions reviewed to improve the transition into LTC were web-based. Effective interventions are those that include the person living with dementia and the carer in decisions of goals for care and provision of education about what to expect (Hirschman & Hodgson, 2018). The MT4C-In Care intervention attempts to address these outcomes by providing supports in the form of real-world stories, writing prompts and resources to achieve this goal. Ultimately, the inclusion of resources (and prompts to use them) is a strength of MT4C-In Care though some participants wished for more resources to be added while others were overwhelmed by their number.
The access to resources in an accessible, timely manner is a strength of MT4C-In Care and other web-based interventions and tools. Indeed, the current study aligns with Hopwood et al.’s (2018) systematic review of web-based interventions which acknowledges the positive response carers have to web-based interventions. This access proved invaluable given the lack of support available during the COVID-19 pandemic but may have contributed to the feelings of some carers not wanting to go on-line more frequently with the shift to remote work. Further research is warranted to determine if these feelings remain in times when work is not fully on-line.
Building on telephone and internet-based interventions to support carers of those living with dementia (Marziali & Garcia, 2011), it is acknowledged that often, contact with health care professionals and/or other carers can be a desirable component of web-based models (Davies et al., 2020; Hopwood et al., 2018). In the current study, several participants acknowledged that a web-based platform alone was not ideal to meet their needs to interact with health care professionals or peers, however, given the national scope of MT4C-In Care, chat functions or video conferencing features have not been integrated. Instead, links are provided for carers to join existing chat groups. Future research may explore the feasibility of integrating these other kinds of options into MT4C-In Care.
Useability
The ease of using and navigating a web-based tool is essential to its success; this was borne out in the findings from our participants in the present study. In a web-based intervention by Lewis et al. (2010) for community-dwelling carers of people living with dementia they found that their participants suggested the need to make navigating their tool easier; a finding not reflected by our current participants. The difference in our finding is likely due to the design of our respective interventions and not sample characteristics.
The motivation to engage with the tool was brought forward by some of our participants, a noted challenge in other studies addressing web-based interventions (Stjernswärd & Hansson, 2017). This may be reflective of the COVID-19 pandemic’s effect on moving much work to an on-line environment. However, in their study of an on-line mindfulness intervention, Stjernswärd and Hansson (2020) noted that participants indicated their participation as more or less timely depending on their life circumstances and caregiver situation at the time of the intervention period.
In our study, participants identified that an option for a paper or hard copy of some parts of the MT4C-In Care tool would be beneficial, and to decrease time spent on a computer. This observation was similar to Lewis et al.’s (2010) web-based tool where participants suggested an accompanying workbook would improve the tool. Printing off information as an option is important to our study and Lewis et al. (2010) as this provides options for carers to tailor how they engage with a (web-based) intervention. Yet, it is important to bear in mind that not all aspects of the intervention (e.g., outside resources) have the option to be in a print-based format, and that asking participants to print off information uses their own time and resources, which may contribute to inequities in who can access this information based on economic or other factors.
Some participants appreciated and valued the sections of MT4C-In Care that offered support for reflection—but not all participants desired to use this aspect of the tool. MT4C-In Care is self-administered, and carers are encouraged to engage with the aspects that they find most helpful. This finding emphasizes the need for interventions that are tailored to different carers (Hopwood et al., 2018), including gender-based differences. This is borne out in research that indicates positive results are most often obtained with psychoeducational interventions that are tailored to the needs of their users (Williams et al., 2019; Zhao et al., 2019).
Usefulness
In our study many participants appreciated the direct quotes used in the tool as this was a means for them to feel validated that others had similar experiences. As a result of this, we have developed short films to additionally support the connection carers may feel when using MT4C-In Care. Similarly, Lewis et al.’s (2010) participants also valued being able to relate to what other carers had experienced and that their supporting videos were recognized as beneficial for participants. Being validated was also reported by Scott et al. (2022) as an important outcome of their e-learning intervention.
Engaging in self-care is a complex, yet challenging activity for carers of people living with dementia, yet is necessary to their well-being (Waligora et al., 2019). The benefits of self-care for carers of people living with dementia is highlighted in Oliveira et al.’s (2019) scoping review, including within web-based interventions. Participants using the MT4C-In Care toolkit emphasized the benefits of being prompted to care for themselves; something that too often carers fail to give themselves the space or time to do (Wolverson et al., 2022). Being engulfed by the caregiving role and losing a sense of self has been previously described (Skaff & Pearlin, 1992) and can be detrimental to a carer’s well-being (Sörensen & Conwell, 2011). Giving permission to carers to take time for themselves is vital to ensuring their on-going health and further research is warranted to find ways to support carers in this regard.
Having a better understanding of dementia and how to provide care in LTC as a family member was supported by users of MT4C-In Care. Similar studies examining online psychoeducational interventions for community-based carers noted similar effects to the current study with reports of higher feelings of mastery over caregiving and a better understanding of the disease process (Boots et al., 2014; Hepburn et al., 2022). However, given the lack of online interventions targeted at carers within LTC, future research is warranted.
Limitations
This study has limitations that require consideration. First there was a lack of diversity in our sample both in terms of sex and ethnicity. We interviewed 6/39 male carers (15%). While women overall account for the majority of caregiving (Stewart et al., 2016), carers over the age of 85 tend to be men (Anderson et al., 2021). Research has indicated that men have different needs and perspectives regarding caregiving and support needs (Stewart et al., 2016; Xiong et al., 2020) and therefore, the inclusion of additional men in the study may have added alternative perspectives on the toolkit. Exploring this in future research is an important area of study.
Secondly, our sample also lacked ethnic diversity, with 89.7% of participants being White. Caregiving is a cultured experience (Kenning et al., 2017; Yang et al., 2021) with differences being reported within different populations. Having a diversity of cultural perspectives would enhance the toolkit and widen the scope of support it can offer.
Thirdly, we recognize that level of education, which is often a proxy for income, and age of participants may influence their comfort with technology, access to, and the use of on-line resources. The digital divide still does exist, and this may limit those with lower incomes using on-line resources (Vogels, 2021). Barriers for older adults to use technology have been identified, yet we need to acknowledge that older adults are increasingly adopting the use of technology in their daily lives, and this is reflected in the current study (International Telecommunication Union, 2021).
Fourthly, participants whose family member died prior to the collection of the qualitative data (2-month mark) were withdrawn from the study. However, these participants did have a chance to use the tool and their perceptions may have been valuable, especially considering the tool has a section to help cope with loss. In addition, caregivers who chose not to be interviewed or who withdrew from the study for other reasons, including not seeing value in the toolkit, likely have perspectives that differ from the analyzed sample. While a fulsome analysis of withdrawal reasons, and impacts of withdrawals upon outcome achievement, is previously reported (O'Rourke et al., 2025), future research to capture perspective of those who tried and chose not to use the intervention is needed to revise this, and other, psychoeducational interventions.
Finally, the current study found challenges with recruitment during the COVID-19 pandemic which was evident across all sites, but especially in the less-populated provinces. In addition to recruitment struggles, there was the reality that carers were essentially locked out of LTC sites during the height of the pandemic contributing to a sense of distress in many caregivers (Parmar et al., 2021); this unique context likely does not reflect the perspectives of carers who have access to their relative.
Conclusion
Web-based interventions such as MT4C-In Care, provide an important tool in the toolbox of the limited supports and resources that health care providers can offer carers of people living with dementia in LTC. Tools such as MT4C-In Care are critical pieces in assisting to bolster social support (O'Rourke et al., 2025) and the self-efficacy, well-being, and quality of life of carers (Brooks et al., 2018) and may play an important role in reducing the detrimental effect loneliness has on carer health (Victor et al., 2021). Yet, more remains to be researched to explore and address the benefits of online interventions for carers of people living with dementia.
Footnotes
Acknowledgements
The authors wish to thank all the participants for graciously giving their time to this study.
Ethical Considerations
We received ethics approval from the University of Alberta Health Research Ethics Board (#Pro00090771); University of Saskatchewan Research Ethics Board (#1385); University of Manitoba Education/Nursing Research Ethics (E2019:127), and the Hamilton Integrated Research Ethics Board (#7659).
Consent to Participate
All participants provided oral informed consent prior to enrollment in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Public Health Agency of Canada Dementia Community Investment (Grant 1920-HQ-000021).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Our ethics approval, consent forms state that participant data can only be made available to the research team.