
Abstract
Group Antenatal Care (GANC) provides a person-centred approach to prenatal care, integrating health care delivery with health promotion, while empowering participants and building a sense of community. GANC has proven to be effective and positively experienced by both participants and care providers and is also feasible to implement. However, introducing such innovative care models in a metropolitan city like Brussels involves navigating both challenges and opportunities. This study explores how GANC facilitators implement sessions in Brussels, the extent to which the core components are incorporated, and the rationale behind the chosen approaches. We used a descriptive multiple case study design grounded in constructivism and conducted reflexive thematic analysis. We collected data from four settings offering GANC, including 21 observations of four series of sessions and four in-depth interviews with GANC-facilitators. The findings indicate that settings shape the format of the sessions through the creation of a supportive atmosphere, the structure of content, and the integration of health assessments, which creates the format of the sessions. Furthermore, two key dynamics were identified: participant engagement and interaction, and facilitator responsiveness. Our study demonstrates that the settings can uphold the foundational principles of GANC, while addressing the opportunities and challenges within Brussels’ complex urban environment.
Introduction
Antenatal care offers a unique opportunity to promote health and well-being of both mother and child. It is a starting point for monitoring, health advice, psychological, and social support and, if needed, life-saving interventions. Antenatal care has the potential to give children the best possible start in life. For some, it can break the vicious cycle of health disadvantage, such as mental health disorders or unhealthy behaviours, passed down from one generation to the next (Aizer & Currie, 2014). In Belgium, people are free to choose the type of care provider and health care setting for the follow up during pregnancy and birth (Benahmed et al., 2019). Most pregnant people opt for an obstetrician in a hospital setting as their primary care provider, over a midwife or general practitioner in primary care. Care during pregnancy encompasses preventing pathology through clinical interventions and preferably includes psychosocial support and education classes.
However, health services are dispersed, and regular care primarily focuses on screening for pathologies (Benahmed et al., 2019). Both public and private actors offer health education, but they mainly organise it alongside the medical follow-up, not as a part of it. The significant additional time commitment from pregnant people (and partners), combined with other challenges such as financial, language and cultural barriers, may contribute to lower uptake of these services by those in vulnerable situations (Schönborn et al., 2024). The WHO advocates for antenatal care that integrates and gives equal importance to health care and health promotion (World Health Organization, 2018). It recognises Group Antenatal Care (GANC) as a health system intervention to improve the uptake and quality of antenatal Care (World Health Organization, 2016).
GANC is a healthcare model that integrates these different aspects of antenatal care in one session with the same care providers, rather than dispersed over different time slots, settings, and care providers. It builds on the CenteringPregnancy model, originally developed in the United States to transform the existing antenatal care into a more effective, qualitative and women-centred care (Rising et al., 2004). To achieve this objective, it integrates three core components: (1) health care, (2) interactive learning, and (3) community building. GANC is provided to a cohort of 8 to 12 participants in a series of 9 GANC sessions over the course of the pregnancy and one postnatal session. During these 2-hr GANC sessions, an interactive discussion on topics relevant for the duration of the pregnancy follows the individual medical check-up and self-assessment. Two same and trained facilitators guide the GANC sessions, of which at least one is legally authorised to provide the medical check-up. Table 1 includes the definers of GANC, which form the foundation of the model.
Definers of GANC, Based on the Centering Pregnancy model®.

Compared with traditional one-to-one care, GANC results in comparable or better maternal and neonatal outcomes (Carter et al., 2017; Schellinger et al., 2017; Tubay et al., 2019). More apparent, participants who received GANC are more satisfied (Sadiku et al., 2023) and are “getting more than they realised they needed” (McNeil et al., 2012).
In Brussels metropolitan region, the capital of Belgium, currently four public organisations offer GANC, two in primary care and two in a hospital setting. High diversity in nationality and sociocultural heterogeneity characterises Brussels (Centre d’Épidémiologie Périnatale, 2024), which manifests in inequalities within perinatal health (Sow et al., 2018) and health care utilisation. The characteristics of a context make it unique, and therefore implementers should take the specific needs and conditions of this context into account (Durlak & DuPre, 2008; Grimshaw et al., 2012). By doing so, they increase the likelihood of acceptability and feasibility, which in turn leads to sustainability of the intervention.
However, when translating a proven effective intervention, such as GANC, to a new context, it is crucial to retain the core components (Carroll et al., 2007). Fidelity to its core components may ensure that the positive outcomes of GANC are achieved (Chambers et al., 2013; Novick et al., 2013; Wiltsey Stirman et al., 2012). Previous research has predominantly examined fidelity from a quantitative perspective, focusing on whether specific elements of the GANC model are present or absent, without focusing on underlying rationale for adaptations. Other studies tend to concentrate on the broader implementation process, highlighting high-level challenges, such as stakeholder engagement, recruitment strategies, scheduling logistics, and resource limitations. However, few studies offer an in situ exploration of how GANC sessions actually unfold. Understanding the shaping of GANC in this metropolitan city is an important objective in the translation towards other similar contexts. Our aim is to explore how settings in the Brussels metropolitan region shape GANC sessions, whether they incorporate the core components of GANC and the rationale behind their approach.
Methodology
Design
We employed a descriptive multiple case study to understand how GANC was shaped across four settings, drawing on qualitative data from observations of GANC sessions and interviews with GANC facilitators. The study was theoretically grounded in constructivism (Guba & Lincoln, 1982). This paradigm acknowledges that lived experience, culture, and other factors form our perceptions and understanding of reality. In line with this paradigm, the researcher’s subjectivity is seen as a resource for research and data-coding and –interpretation as an inherently and inevitably subjective practice (Gough & Madill, 2012). From a constructivist perspective, incorporating multiple cases has the advantage of generating context-specific insights that deepen understanding of the phenomenon, rather than achieving generalisability (Stake, 2013).
Context
We conducted this study in the Brussels metropolitan region, the capital of Belgium. We approached the four settings currently offering GANC, which, to our knowledge, are the only settings offering GANC in Brussels. They varied in terms of location, structure, organisation of (prenatal) care, and patient population (Table 2). All facilitators in the selected settings were women and midwives with prior experience in providing prenatal care. Their experience with GANC varied, ranging from 3 months to 3 years. All had completed GANC training and were therefore familiar with the core principles of the model. In the Belgian context, facilitators are typically midwives who lead the group sessions, during which the health assessment also takes place. Obstetricians carry out the ultrasounds separately. In some cases, additional individual medical or psychosocial follow-up is required or preferred alongside the group sessions. Facilitator or other healthcare professionals provide these follow-up encounters.
Overview of the Case Characteristics.

Participant Recruitment
We used purposive sampling to recruit participants, including GANC facilitators of the participating settings. The targeted facilitators of the four settings received verbal information regarding the research, including its aims and objectives. We informed them that the study did not serve as an evaluation of their performance but aimed to understand how GANC sessions were shaped in practice, with the possibility, though not the intention, to inform implementation improvements for their setting. In line with the ethical code, we did not provide this information to supervisors or management. Throughout the observation period, the researcher regularly checked in with facilitators to ensure that her presence was comfortable and did not interfere with their practice. All eight facilitators gave verbal consent (not audio recorded) for observation of the GANC sessions and an interview following the observations. The lead author (FT) was in close contact with the participating settings and facilitators through collaboration related to the project. This ensured that facilitators felt comfortable in the presence of the observer.
Ethical Considerations
The Medical Ethics Committee of the University Hospital Brussels (Approval number 2019-365) granted ethical approval on 20 November 2019 (approval number 2019-365). All participating settings provided formal approval for their involvement in the study. Observations of GANC sessions and interviews with facilitators required consent of participants. The researcher introduced herself and the study to the participants in each setting, after which they gave consent for the observations. The participants did not receive incentives for participation. The de-identified recordings, transcripts and coded data were stored on a password-protected and encrypted computer.
Data Collection
We conducted observations of GANC-sessions, followed by semi-structured interviews with each facilitator-duo. The advantage of combining both methods lies in the ability to study the implementation of GANC, as it is conducted (through observation), not only as it is disclosed verbally (e.g., through interviews) (Mulhall, 2003; Walshe et al., 2012). The data retrieved from the observations was used as a basis for the interview script.
Data collection was carried out between February 2021 and October 2022. The Covid-19 pandemic was active during this period and affected group size. One setting deliberately limited the number of participants and, according to three settings, pregnant people were reluctant to participate due to the COVID pandemic (reported during off-the-record meeting). No additional security measures had to be taken. The lead author (FT) conducted all observations and interviews. The data collection tools, comprising the observation checklist and interview guide, were developed by the lead author (FT) and iteratively refined by the research team (FT, AVD, KB).
Observations
The lead author (FT) conducted 21 structured and unstructured observations of four GANC groups in four settings. We chose to start the observations from the second GANC session in order for the participants to feel sufficiently comfortable attending GANC. Starting from the second GANC session, the researcher observed each session of one GANC group per setting to gain an authentic impression of GANC and avoid disturbing group dynamics. This is also in line with one of the essential elements of GANC, recommending a consistent group (see Table 1). We opted for participatory observation (Gold, 1958), as we judged that not participating would disrupt the dynamics. In practice, this meant taking part in the group as discreetly as possible—for example, sitting in the circle with participants rather than apart, and participating during activities, such as holding up an agree/do not agree card, without steering the discussion.
The researcher used an observation guide to capture fidelity of organising GANC according to the key components, namely medical follow-up (including self-assessment), interactive discussion and community building. The guide also intended to enhance reflexivity by acknowledging and hence minimising the influence of own assumptions and beliefs based on previous knowledge and experiences. As the observations of a group progressed, less attention was paid to the format, given this remained constant across GANC sessions, and more attention went to irregularities, interactions and behaviours.
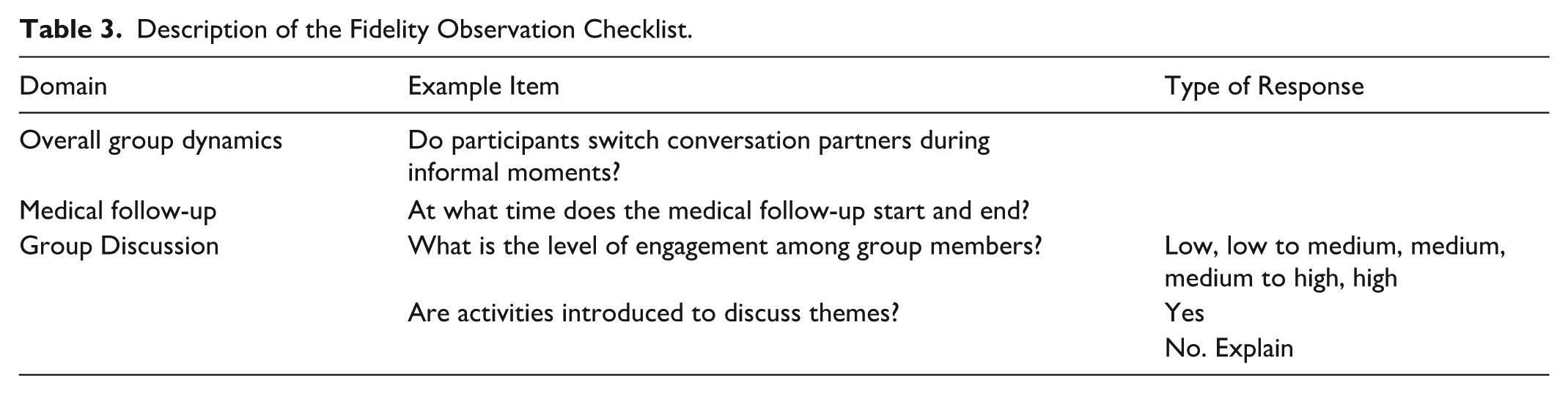
The observation guide was based on the implementation guides of Group Care Global (Group Care Global, 2022a) and CenteringZorg (CenteringZorg, 2023), and was adapted to the Belgian context. Sample items from this guide can be found in Table 3 for illustration. In addition, the researcher observed and made detailed notes on the flow of the GANC session, including behaviours of pregnant people and facilitators (verbal and non-verbal), interactions, impressions and reflections, and background information, such as attendance and availability of space and equipment. Examples of questions to guide the observations can be found in Table 4.
Description of the Fidelity Observation Checklist.
Examples of Questions and Directions for Field Notes.

The researcher was present in the group space. To minimise the impact of her presence, she did not take the lead and only interacted if a participant or facilitator approached her first. This was discussed with the facilitators prior to the first observation. The individual medical check-up was not observed to preserve confidentiality. Information about the individual medical check-up was obtained during interviews.
Interviews with Facilitators
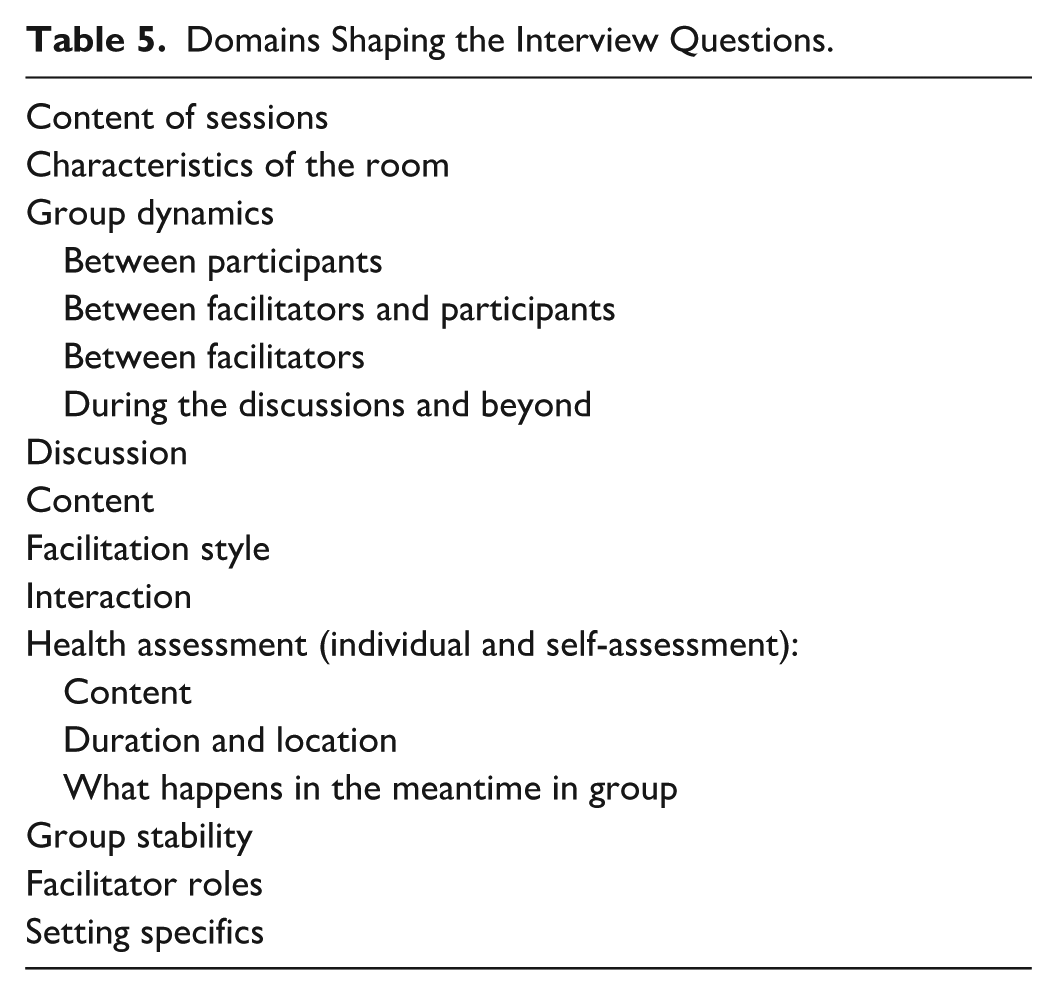
Following the final GANC session of the observed group, the lead author (FT) conducted four interviews with the facilitator duo of the respective group (duration 55–70 min each). The paired interviews provide a complete picture of the practice (Wilson et al., 2016). Interviewees could confirm, clarify and complete each other’s responses. Following an initial analysis of the observations, recurring issues were identified across the four settings. These domains shaped the interview questions and are presented in Table 5. During the interview, the researcher posed open-ended questions to clarify ambiguities from the observations and explore the motivations behind observed actions. The interviews were audio-recorded.
Domains Shaping the Interview Questions.
Analysis
We used reflexive thematic analysis, which aligns with a constructivist view that acknowledges subjectivity and interpretation in the research processes (Braun & Clarke, 2006, 2019). The researcher is an active participant in knowledge generation. A reflexive position throughout the analysis ensures the generation of quality and rigorous study findings (Braun & Clarke, 2022, 2023). We primarily opted for an inductive coding approach, where themes were developed directly from the data content, and a semantic approach, focusing on what was explicitly said and observed without interpreting underlying meanings or assumptions, for the data from both observations and interviews. However, to assess whether settings implemented GANC with fidelity to the original model, we also analysed the data deductively, focusing on the core components. The remaining analysis was guided by the research question: How do organisations in the Brussels metropolitan region shape GANC sessions, and what is the rationale behind their approach? Identifying patterns, similarities and differences across the different settings and through an iterative process allowed to refine and regroup themes.
The analytical process was both repetitive and iterative, with insights building progressively through multiple rounds of analysis. Initial analysis began during data-collection, as the observations and interviews conducted across the four settings overlapped, providing insights and guided subsequent data collection. The lead author (FT) followed the six phases for reflexive thematic analysis (Braun et al., 2015; Braun & Clarke, 2006), of which the first is to familiarise with the data by transcribing interviews and subsequently reading the transcripts and observation-notes multiple times. The dataset was coded, after which the codes were clustered into potential themes and subthemes. These themes were then reviewed against the coded extracts, refined, described, and named. Finally, the themes were presented in the report, supported by data extracts. The results are presented jointly, rather than separately by setting, to serve the research purpose and ensure the protection of participant identities. NVivo software was used to assist in managing and organising the data throughout the analysis process.
Reflexivity
The research team (FT, AVD, KB) held regular critical team-based discussions to support reflexivity (Braun & Clarke, 2024). In addition, meetings and written feedback from the co-authors (HB, MR) offered further perspectives and enhanced reflexivity. This occurred throughout the entire research process, from study outset to analysis and writing. The aim of this collaborative process was to achieve richer interpretation rather than consensus on meaning (Byrne, 2022). The researchers and the choices made aimed to be sensitive and accountable to the needs of the participants and participating settings. Finally, the use of both observations and interviews with facilitators was a final strategy to ensure the researchers’ interpretation aligned with the facilitators’ perspective. The narratives and reflections shared by the GANC facilitators in turn influenced the researchers’ evolving interpretations. This inter-subjective process challenged initial analyses and revealed the rationale behind adaptations. In line with Byrne’s notion of “knowing-with,” our interpretation was co-constructed through a dialogic engagement with participants’ insights, rather than from a detached analytical stance.
The observer (FT) adopted a reflexive stance by giving thought on how her background, assumptions, and dual role as both a researcher and practitioner influenced the research process. Her insider role as a midwife, sociologist, and public health professional with experience in GANC and its implementation, that is, attended the GANC training and guided six settings in the implementation of GANC, including those involved in the study, provided her with valuable knowledge and an understanding regarding the shaping of GANC. She also reflected on her outsider perspective as an academic trained in qualitative research. Her shared demographic characteristics with GANC participants—such as being a woman of similar age—helped facilitate rapport. At the same time, she acknowledged and openly communicated her differing characteristics, including her role as a researcher and her background.
Results
Within the observed groups, the group sizes ranged from 3 to 7 participants. The series comprised 6 to 9 GANC sessions. Each group GANC session lasted between 120 and 175 min. Each group was facilitated by its own consistent pair of midwives across all sessions. The spoken language during discussions was French, while a facilitator translated into English or Dutch if necessary. The age range of participating individuals was 22 to 39 years. All groups were highly diverse in terms of ethnicity and parity, except for one group, which consisted exclusively of primiparous participants.
Based on the data, we describe how GANC is shaped in the 4 Brussels settings in terms of session format and the dynamics that occur. The way settings shape the format of GANC sessions is described under three themes: the atmosphere, the structure of the GANC-sessions, and the integration of health assessments. In addition, two key dynamics, participant engagement and interaction, and facilitator responsiveness , are reflected in the final two themes. As shown in Table 6, each theme includes sub-themes that are integrated into the presentation of the findings. In the description bellow, we explicitly state when findings stem from interviews or are based on observational data.
Themes and Subthemes.

Theme 1: Atmosphere
A key finding highlights the efforts made by settings to create a pleasant, relaxed, and welcoming environment. This theme is supported by three sub-themes: the physical transformation of the space, the role of facilitators’ behaviour in setting the mood, and the perceived impact of the atmosphere on participants. Small interventions, such as arranging cushions or chairs in a circle, playing music, or offering drinks and food, physically transform the space. As noted in one facilitator duo interview, the combination of these elements significantly alters the typically clinical setting of the rooms:
Facilitator #1: “The space is really different.”
Facilitator #2: “It's not a cozy room, but it feels cozy.”
However, observations suggest that it is primarily the facilitators’ behaviour that sets the mood. Their approach to welcoming participants is personal and warm, putting participants visibly at ease. This is echoed in participants’ comments, such as “happy to be here”, “feeling relaxed,” and “looking forward to the GANC sessions.”
The impact of the atmosphere is evident across various aspects of the sessions. Observations show that this atmosphere enhances conversations among group members during informal contacts and group discussions. Facilitators explained during interviews that a relaxed atmosphere creates a safe environment for open discussion. Conversely, when facilitators appeared tense or stressed, it negatively affected the mood and group dynamics. The facilitators in question confirm that they feel insecure and rushed to provide the health assessment within the reserved time, that is, 30 min for all participants, and to address all planned topics during the interactive discussion. Integrating health assessment into the GANC session seems to be challenging to some but not all settings (cf. theme 3) and having a flexible plan and being responsive to the needs of the group go hand in hand (cf. theme 5).
Theme 2: Structure of the GANC-Session
A second theme concerns the structure of the GANC session, which was expressed in four subthemes: the use of the core components as a framework, the tailored sequencing of these components, and variability in the structure of group discussions. All settings structure the GANC sessions around the model’s core components, that is, health assessment, time for community building and group discussions, as confirmed by observations. These core components serve as a framework to guide the sessions. Time and space are allocated to each, demonstrating fidelity to the model, even if the specific implementation differs.
Differences were observed in the sequencing of the core components across settings, tailored to each context. Most settings (three out of four) organise the health assessment before the discussion. This allows participants to arrive gradually, unwind while waiting for their turn, interact with others, and complete the self-assessment. For practical reasons one setting starts with the discussion and conducts the medical assessments during the break: “There is no time to do it another time. During the break, they’re eating anyway. We can use that moment better.” (Facilitator #1). An additional reason is punctuality: “It ensures they have no excuse to come late.” (Facilitator #2). Observations confirmed that, compared to the other settings, participants did arrive more punctually. Facilitators also explained that starting with the discussion stimulates interaction during the break: “They’ve already had an exchange, so it’s easier to be social (during discussions).” (Facilitator #2). To enhance community building, most settings (three out of four) provide time for informal contact, during breaks, upon arrival, and at the end of the session. Facilitators explained that a gentle start and close to the session, encourages participants to engage with each other. All settings devoted a major portion of the session to interactive discussion.
Finally, variability was observed in the way interactive discussions are structured, adding a second organisational layer beyond the overall session format. Some settings (two out of four) consistently include an opener, a break, and a wrap-up, while one omits these elements due to time constraints. Another does not follow a fixed structure, claiming to adapt based on the situation or participants’ needs. The absence of a break often led to declining interaction in the second half of the discussion.
Theme 3: Integration of the Individual Health Assessments
A third theme concerns the integration of individual health assessments within the GANC session. Three subthemes were generated: the location and time allocated to health assessments, the balance between individual and group needs, and the strategies employed by facilitators to manage this balance.
In all settings, the health assessment is incorporated into the GANC session and includes standard medical follow-up such as assessment of foetal heartbeat, movements, growth and position, checking for pregnancy-related complaints (e.g., pain, bleeding, or contractions), reviewing laboratory results, and providing prescriptions and referrals.
Differences in location and allocated time influence whether the health assessment is perceived as integrated into the overall session. Based on this, we observed two distinct approaches: in two settings, the health assessment is interwoven with the session, while in the other two, it is conducted as a separate activity. In the first case, the health assessment was brief, taking approximately 30 min in total for all participants and typically took place in a screened corner of the same room where the discussion occurred. This aligns with the original GANC model, which suggests that “Risk assessment takes place within the group space.” This integration allowed for minimal disruption to the flow of the GANC session and group dynamic. Nonetheless, one facilitator expressed concern about the quality of care due to the limited time: “I think it has to go fast. Much faster than I prefer. (. . .) We have the feeling we’re forgetting things.” (Facilitator #3). Interestingly, this concern appeared to be more a perception than a reflection of actual omissions. In the other two settings, health assessments is treated as separate from the GANC sessions. These take place in a separate room and require more time, creating a clear delineation with the group session.
Conducting health assessments separately introduces tension between individual needs and group needs. First, it disrupts group dynamics, as the second facilitator and remaining participants have to wait for the assessments to be completed: “It’s difficult for me to keep the conversations going and they (the participants) didn't really start chatting either.” (Facilitator #4). Second, allocating more time to the individual health assessment, reduces the time available for group activities. Facilitators explained that this additional time is necessary given the presence of high-risk pregnancies and psychosocial vulnerabilities requiring extra monitoring, support, and administrative coordination. As two facilitators explained in one duo interview:
Facilitator #5: “I do find it difficult to also pay attention to extra things with this (vulnerable) group - like appointments with the social assistant. It is difficult.”
Facilitator #6: “Group Care within our organisation comes with a lot. They have medical issues, and not all of them speak the language.”
Facilitators working with these populations also noted that considerable time is spent addressing participants’ questions. This is particularly the case when facilitators act as case managers and coordinate participants’ care. One explained: “There are always questions that come up, complaints or specific questions about diabetes. (. . .) And then also the following appointments, giving the prescriptions for ultrasounds, the blood draws, explaining why the blood sampling has to be done. So that takes time during the individual consultation.” (Facilitator #6).
To maximise group time and strengthen integration, facilitators employ various strategies. Above all, they emphasise thorough preparation, such as having an overview of necessary examinations and prescriptions ready. Where appropriate, facilitators refer common topics to the group discussion: “We can tell them that those (individual) moments are used to discuss really specific and sensitive issues. And everything else in terms of ultrasound or blood sampling will be discussed in the group.” (Facilitator #7). Others suggested introducing information earlier in the programme to pre-empt recurring questions: “We reflected on the idea of providing all explanations about the care process, including which examinations will take place each trimester, at the start of the sessions.” (Facilitator #7)
Facilitators also used informal contacts during the sessions to address personal questions of participants and provide psychosocial or administrative support. For instance, we observed that during the informal contacts, the second facilitator was checking in on participants’ mental well-being and offering help with postnatal midwife applications. Nonetheless, one facilitator emphasised that participants should still have the opportunity to discuss sensitive matters privately: “There are always going to be questions they don't want to ask in the group.” (Facilitator #8).
Theme 4: Participant Engagement and Interaction
A fourth theme concerns participant engagement and interaction within GANC sessions. Four subthemes were identified: the sense of connexion created among participants, the influence of participant characteristics, the impact of group size and time, and the role of facilitators’ behaviour in shaping dynamics.
GANC aims to create opportunities for socialisation to enhance community building. In this regard, a sense of connexion emerged among participants across all observed GANC sessions. Interestingly, interviews revealed that this bond was mostly temporary and limited to the purpose of the sessions. Facilitators did not observe deep or lasting relationships: “They are happy to see each other for now and are willing to share, but truly connecting on a deeper level. . . it never really becomes amicable.” (Facilitator #2).
Participant engagement during discussions was moderate within the observed groups. In particular, the disclosure of personal information was limited. Facilitators confirmed this: “I think putting feelings into words is very difficult (for this target group).” (Facilitator #8). However, facilitators also indicated that bonding and interaction varied between groups: “In our other group, more interaction and questions came up. With this group, if you didn't supply it, there'd be nothing. . .” (Facilitator #6)
This highlights a complex interplay between elements and behaviours of group members, including the GANC facilitators. Regarding participant characteristics, observations revealed that shared aspects such as language and culture or health care issues such as gestational diabetes resulted in group members to reach out to one another. These interactions led to the emergence of smaller subgroups during both discussions and informal moments. Participants supported each other, for example by translating for those who did not speak French or Dutch. However, these subgroup conversations sometimes disrupted the larger group dynamic. Facilitators also mentioned that personality traits, such as being introverted or extroverted, influence interaction. Some participants naturally assumed a leadership role, helping to bind the group together. “She (group leader) acted as a liaison.” (Facilitator #6). Observations further showed that multiparous participants, whether spontaneously or encouraged by facilitators, often shared their experiences. These contributions tended to elicit responses from others, which enhanced interaction within the group.
Facilitators noted that a sufficient large group size is crucial for interaction, as it creates more diversity as two facilitators explained in one duo interview:
Facilitator #1: “Because of the small group, you need assertive (participants). If 2 out of 3 are quiet, it's hard to find balance. Or if there are language problems, it's difficult to have smooth interaction.”
Facilitator #2: “Or it’s hard to temper assertive mums and let others have their say.”
Time played a role in building connections. Observations suggested that participant engagement and relationships deepened over time, which facilitators echoed: “It takes time to get to know each other, for both them and us. (. . .) We were just starting to find each other. And then it ended.” (Facilitator #7)
Facilitators influenced group dynamics not only during discussions but also in informal moments. According to interviews, their role in informal settings focussed on creating conditions that encourage interaction. However, they were cautious not to impose it: “But I don't know if that's our role. We create the space for it, and if they want to do it, they do it. It's a little patronizing otherwise.” (Facilitator #6). The original GANC model emphasises the importance of interactive discussion, guided by a facilitative leadership that honours each member’s contribution. Observations demonstrated that facilitators used various strategies during discussions, usually intentionally, to support rather than control engagement and interaction.
The materials and activities facilitators employ encouraged participation during discussions. Observations indicate that simple methods were often the most effective, which one facilitator confirms: “It (material) is more of a means to an end. And most people don't see it as childish because of that” (Facilitator #2). Opening and closing activities created space for emotional expression, either verbally using the “emotion dice” or physically through music and dance. Notably, in the absence of such activities, participant openness remained superficial. Observations also showed that facilitators’ self-disclosure enhances group engagement. According to facilitators, this strategy was deliberate and aimed at creating a sense of equality: “It is not sharing for the sake of sharing, but sharing in function of the group, what’s helpful. Sense of: we are all in this together.” (Facilitator #2).
The depth of topic discussion affected group dynamics. Excessive elaboration or an overload of information overwhelmed participants and limited interaction, as confirmed in interviews: “Sometimes we go too far in describing (the process). They don't have to fully understand why something happens.” (Facilitator #5). In contrast, when discussions were limited to 15 to 30 min per topic and remained concise and focussed, engagement levels increased. Discussion techniques also shaped interaction. Observations show that most facilitators encouraged all members to contribute, aiming for equal participation. However, some facilitators answered questions too quickly rather than using the recommended “acknowledge, refer, and return” technique as advised in GANC. This was confirmed during interviews: “And we may be a little dominant in the group process (laughs).” (Facilitator #2). According to the same facilitator this is partly due to time constraints and partly because participants do not possess the information: “For some matters, I think we can definitely ask more questions. (. . .) Of course, we give the opportunity for it to come out of the group, but if it's really not in there.” (Facilitator #2).
Theme 5: Facilitators’ Responsiveness
A fifth theme concerns facilitators’ responsiveness in conducting GANC sessions. Three subthemes were created: the balance between proactive and reactive approaches, responding to group needs, and flexibility in facilitator roles. We observed that facilitators conducted GANC sessions using both proactive and reactive approaches, where the former is planned and structured and the latter is responsive. Both approaches are necessary to establish group dynamics and interaction. This aligns with the original GANC model, which recommends having an overall plan for each session, that covers core content while also allowing variation in emphasis. Observations reveal that all facilitators prepared content and structure, discussion topics, and associated methods and materials. However, the timing and thoroughness of this preparation varied. In some settings, preparation was meticulous, with structured activities and materials. In others, topics and methods were chosen shortly before the session.
Facilitator flexibility proved crucial for responding to group needs. A highly flexible approach is necessary in one setting where participants typically enter care later in pregnancy. As a result, GANC sessions start at around 25 weeks of gestation and consist of fewer sessions. Facilitators explained that they adapted the content entirely to participants’ requests: “These weren’t topics we had planned, but themes that came out (of the group), so we adapted.” (Facilitator #6). This approach was considered appropriate for this context: “I understand if your group only comes (together for) 3 times, you have to prioritize. So I do think it's a good approach to look at what’s actually going on (in the group).” (Facilitator #8). In contrast, when facilitators adhered too rigidly to their plans with little room for flexibility, they found it difficult to respond to what was happening in the group or to meet participants’ emerging needs: “Maybe we don't have enough time to do that (respond to needs), because we want to give way too much information. (. . .) When someone has a question, we think we have to answer it quickly, because there’s still so much left to cover.” (Facilitator #5). Observations revealed that focusing on key messages during discussions was an effective strategy to deliver core content while remaining responsive. The following facilitator also made this reflection: “We run out of time every time. (. . .) To give people time, we have to try to make our messages more concise.” (Facilitator #5). Responsive facilitators adapted not only the content, by incorporating themes that resonated in the group, but also the structure (e.g., inserting a break or energiser when engagement faded) and the method (e.g., choosing a more suitable activity). For instance, we observed that the topic “Ramadan during pregnancy” was introduced during one group discussion in addition to the planned content.
Responsiveness also involved flexibility in facilitator roles. Depending on the group needs, facilitators translated or clarified information, monitored and adjusted group dynamics, or offered additional support. They also complemented one another dynamically. For instance, observations showed one facilitator taking the lead in a discussion when the co-facilitator mentioned “not having a good day.” However, responsiveness was sometimes lacking when facilitators are inattentive or overly dominant.
Discussion
GANC is applied in diverse contexts and among varied target populations (Group Care Global, 2022b). Adaptations to the model are necessary to align with the context where it is implemented. Similarly, the Brussels settings studied have shaped GANC to suit their particular context. Based on our findings, we describe this shaping in four key points.
A first key finding is that all participating settings implement GANC with fidelity to the model, adhering to its three core components: that is, health assessment, an interactive discussion, and enhanced community building. Facilitators use these as a framework to organise the GANC sessions (cf. Theme 2), although implementation differs by setting. For instance, some settings fully integrate the health assessment into the group setting, while others conduct it separately due to contextual limitations (cf. Theme 3). Likewise, some group discussions are highly interactive and responsive, while others follow a structured plan with less flexibility (cf. Theme 5).
A second key factor influencing GANC delivery is the role of the facilitators. One way this influence becomes visible is through the use of a predetermined structure and prepared content, which most settings apply when setting up their GANC sessions. For instance, facilitators develop materials and activities to enhance interactivity, physically transform the room, create the atmosphere and include breaks to promote social support. The structure and preparations provide guidance and boost confidence for facilitators, particularly for less experienced facilitators. Prior research confirms that experienced facilitators rely more on their facilitating skills and tailor sessions to participants’ needs (Martens et al., 2024; Teate et al., 2013).
Our findings suggest that these facilitation skills, particularly their responsiveness, affects participant interaction. Facilitators strive to balance a planned, fixed structure with the flexibility needed to meet participants’ specific needs. For example, an overly rigid plan during discussions may leave little room for emerging concerns or questions. In such cases, the facilitator’s agenda tends to dominate, and facilitators lead the discussions (Wright et al., 2018), which contradicts GANC’s philosophy of prioritising woman-centred care.
At the same time, a degree of structure and preparation makes GANC sessions more efficient and allows space to be responsive, such as addressing questions, needs or unplanned topics. Well-developed interactive material also boost group interaction and highlight key messages. This aligns with a core GANC principle: each session has a plan, but emphasis may vary (Rising & Quimby, 2016).
A third key factor shaping GANC delivery is group related. In our study, facilitators noted that even when applying the same methods and formats, group dynamics varied significantly. Certain group characteristics can support or hinder interactive discussions and community building—for instance, the presence of leaders can foster engagement, while language differences may create barriers.
Facilitators must develop skills to effectively manage group dynamics (Bastiaens et al., 2016; Craig et al., 2021), while also centring participants’ needs and questions (Andersson et al., 2014). Strengthening referral and recruitment processes can help settings increase enrolment (Talrich, Van Damme, Bastiaens, Rijnders, et al., 2023; Talrich, Van Damme, Bastiaens, Bergs, et al., 2023) and strategically compose groups—for example, balancing language or parity. This intentional composition can enhance group cohesion and interaction during GANC sessions.
GANC facilitators take on multiple roles to shape sessions (Gresh et al., 2022). They shift between providing medical follow-up, offering psychosocial support, facilitating discussions, and improving cohesion. Implementing GANC, requires a new set of pedagogical skills. Learning these competencies, roles and responsibilities takes time and requires training (Ahldén et al., 2008; Bastiaens et al., 2016; Gresh et al., 2022) along with strong mentoring and ongoing fidelity checks (Grenier et al., 2022).
The final key finding is the strong influence of the context on the shaping of GANC and the adaptations made. The Brussels patient population, marked by psychosocial vulnerability, linguistic and cultural diversity, and a high prevalence of medical risk, plays a central role in the shaping of GANC. The group setting appears to be advantageous during discussions, as participants can translate for one another. Additionally, the facilitative approach and available time further supports communication and understanding. A study conducted in the United Kingdom involving participants with limited English proficiency similarly highlighted the importance of the sense of community created within GANC, which was essential for both a positive experience and learning (Wiseman et al., 2024). The study also noted that although simultaneous interpreting altered the flow of sessions for some facilitators, it was more effective compared to peer translation. Due to practical and financial constraints, hiring a professional translator is not always feasible. In such cases, translation by peers or the facilitator can serve as a suitable alternative.
Integration of the health assessment proved more challenging in this context. Two out of four settings in our study struggled to limit the time of the individual health assessment and conduct it in a separate space. Limiting the assessment to 5 min per participant and conducting it in the group space helps normalise pregnancy, increases care efficiency (Rising et al., 2004) and creates more time for group discussion and informal interaction. The allocated time is sufficient to perform the regular assessment (namely to measure the fundus, and to listen to the foetal heart tones) and to share concerns (Rising, 1998). However, according to our respondents, more individual time is needed due to the high prevalence of pathological pregnancies and psychosocial needs among their patient population.
While complex cases challenge GANC implementation, these participants may benefit equally or even more from the support and information GANC provides (Wiseman et al., 2022). GANC has the potential to harmonise and integrate prenatal care, with the facilitator acting as care coordinator. An individual follow-up consultation may be recommended for issues requiring more privacy or time (Rising, 1998), but should be considered after exploring other available options. As several settings in our study demonstrated, thorough preparation, including prescriptions and an overview of requested tests and consultations per participant, ensures more efficient operation. In addition, in order to limit the time during the individual health assessment the co-facilitator might address some of the personal or sensitive questions during informal moments. A combination of medical and non-medical care providers, such as a social worker or psychologist, acting as group facilitators could enhance the ability to provide psychosocial support, especially with the complex psychosocial needs related to the characteristics of the Brussels metropolitan population. Another option is to strengthen the group’s ability to offer support by forming sufficiently large (8–12 participants) and diverse groups.
While these strategies offer practical ways to optimise time, they must be accompanied by a shift in mindset. Reducing time in one-on-one consultation contrasts with prevailing models that prioritise medical monitoring over prevention, empowerment, and health behaviour change. Some providers inexperienced with GANC, express discomfort discussing sensitive topics in a group and fear missing psychological or social issues (Ahldén et al., 2008). This contrasts with our observations and other research into participants’ experiences (Lazar et al., 2021). It is possible that these assumptions stem from insecurity among facilitators (Lazar et al., 2021).
Partner involvement is another factor that may influence group dynamics. Although partner participation was not explicitly studied, its presence or absence likely plays a role in shaping GANC sessions. Facilitators reported difficulties in engaging partners: a challenge that has also been noted in other studies (Hunter et al., 2018; Hunter et al., 2019). Facilitators shared after data collection that steps had been taken in new groups to promote partner involvement, such as organising a separate session for participants and their partners or significant others.
Recommendations
The findings suggest that when implementing GANC in Brussels and similar contexts, fidelity to the core components is feasible. Facilitation training combined with regular reflection on practices and peer review, supports implementation and fidelity by guiding facilitators in adopting various roles and skills. Organisations should prepare during the pre-implementation phase by establishing a format and structure to guide facilitators, especially those with less experience, during sessions. Implementation efforts, such as recruitment and referral processes, should be explored to enhance enrolment and thereby increase diversity and interaction. Sessions should also be tailored to diverse and vulnerable populations, using tools such as visual materials. Above all, the central goals of GANC—patient empowerment and placing patients at the heart of care—should guide every aspect of its design and delivery. Further research is needed to explore participants’ perspectives in these contexts and how GANC can be adapted to better meet their needs and preferences.
Strengths and Limitations
This multiple case study included four settings with varying levels of experience. The settings reflect the diversity in a metropolitan region. Additional strengths include the combination of observations of GANC sessions and interviews with facilitators, allowing richer data from multiple perspectives. Moreover, the qualitative and constructivist approach allowed exploration of the topic that has largely been studied through a quantitative or positivist lens. A limitation is that the perspectives of individuals participating in the GANC sessions were not included. Future research should explore their experiences. Observations were limited to one group per setting, but this was mitigated by interviews with facilitators, which provided insights into other group dynamics.
Conclusion
This multiple case study demonstrates that it is feasible to implement GANC in a complex urban setting, such as Brussels. While integrating its core elements and uphold its foundational principles, it is necessary to take into account the specific context in which GANC is implemented, considering its challenges, and opportunities. When shaping GANC sessions, the format, including the atmosphere, structure, and integration of health assessments play a pivotal role. Equally important are the underlying dynamics, not only in terms of participant engagement and interaction, but also the responsiveness of facilitators
Our results show that the rationale behind adaptations operates at multiple levels—such as logistical constraints, time pressure, or prevailing norms. Organisations should reflect the rationale behind their actions, especially when adaptations conflict with fidelity. Through this reflective approach, they will gain a deeper understanding of not just what is or should be done when implementing GANC, but also how it is achieved and why particular decisions are made. Central to this process is a commitment to the philosophy of GANC, which places woman-centred care at its core. Participants needs, questions, and experiences should above all guide the implementation and shaping of GANC.
Footnotes
Acknowledgements
We would like to thank all health care providers who participated in this study to make time and to share their experiences for this study. We are grateful to the advisory committee for their guidance and advice throughout the process, with a particular gratitude to Saskia Van Besauw, Katelijne De Koster and Prof. Jochen Bergs.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was obtained from the Belgium National Institute for Health and Disability Insurance (NIHDI) as part of the Federal Public Service Finance. However, the funders had no role in the study design, data collection, data analysis, interpretation of data or writing of this article and this work was supported by the National Institute for Health and Disability (CGV 2018/363).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not publicly available due to privacy or ethical restrictions.