
Abstract
At least 10% of fathers experience depressive symptoms during the postpartum period, yet they are often overlooked and under-supported. It is critical to understand paternal postpartum depression as it has been linked to serious consequences, such as increased suicide risk among fathers. Further, paternal postpartum depression influences the entire family unit as it has been associated with maternal mental health issues and negative father-infant interactions. Through a qualitative descriptive design, we aimed to (1) identify the factors that fathers report as contributors to their postpartum depression symptoms, and (2) examine the reported postpartum depression symptoms among fathers and the associated impacts on their lives. Using thematic analysis, we analyzed 63 anonymous Reddit posts by fathers about their paternal postpartum depression experiences. Contributors included: (1) altered role adjustment, (2) resource-demand imbalance, (3) challenging maternal and infant circumstances, and (4) disparate yet concurrent realities. Symptoms included: (1) cognitive-emotional, (2) somatic, and (3) masked. Impacts included: (1) fractured social connections, (2) diminished career satisfaction and performance, and (3) positive outcomes on the other side. Fathers experienced various contributors, symptoms, and impacts of paternal postpartum depression. There is a critical need to increase awareness of and support for paternal postpartum depression to increase overall postpartum family well-being.
Introduction
Fathers’ mental health during the perinatal period is largely overlooked but highly impactful for men and their families (Scarff, 2019; Walsh & Garfield, 2024). About 10% of men experience paternal postpartum depression (PPD), characterized by depressive symptoms occurring in fathers during the first year after the birth of a child (Rao et al., 2020). This is likely an underestimate given that there are not screening guidelines in place for fathers (Fisher, 2017) and men are less likely than women to seek help for emotional concerns (Sagar-Ouriaghli et al., 2019). Risk factors for paternal PPD include maternal perinatal depression, relationship dissatisfaction, unemployment, low socioeconomic status, and lack of social support (Chavis, 2022; Tarsuslu et al., 2020). Paternal PPD has received much less attention compared to maternal PPD, but it is important to address this condition as it has been linked to serious consequences, such as increased suicide risk among fathers (Quevedo et al., 2011).
Beyond individual consequences, paternal PPD influences the entire family unit as it has been linked to maternal mental health issues and negative father-infant interactions (Davenport et al., 2022). Contemporary fathers engage with their children significantly more than in the past due to factors such as women working outside of the home and shifts in gender-based role norms (Livingston & Parker, 2019; Petts et al., 2018). However, experiencing adverse mental health symptoms can hinder fathers’ abilities to effectively engage with their children, potentially resulting in negative child outcomes including mental health and behavioral problems (Fisher, 2017; Fisher et al., 2021). Further, fathers are often major sources of support for mothers during the postpartum period; however, their own experience of depressive symptoms may impact their ability to provide emotional support for their partner and practical support for their family (e.g., infant caregiving responsibilities), potentially also negatively impacting maternal mental health. Thus, there is a need to understand fathers’ experiences with paternal PPD to inform future interventions designed to support the mental well-being of fathers in the postpartum period, thereby influencing overall family health.
A recent systematic review examining fathers’ lived experiences of paternal PPD identified that fathers often hide their postpartum depressive symptoms and avoid seeking help due to fears of judgement or lack of support (Davenport et al., 2022). Anonymous social media platforms offer an innovative and promising avenue for exploring accounts of paternal PPD experiences because participants are relieved of concerns about disclosure and subsequent judgement related to stigmatizing subjects (Choudhury & De, 2014). Fathers in Ammari and Schoenebeck’s (2015) study reported using anonymous forums like Reddit to document their parenting journey, learn fathering skills, and seek support when real-name platforms felt too public or judgmental. Ammari et al. (2018) further demonstrated that fathers rely on anonymous platforms like Reddit as outlets for overcoming societal judgement when sharing sensitive experiences such as mental health challenges and paternal caregiving burdens. Together, these studies show that Reddit functions as an active, socially dynamic space where fathers express concerns and receive support.
This growing body of research underscores how Reddit serves not only as a support network but also as a rich data source for understanding the lived experiences of fathers. For example, previous studies have successfully used Reddit to explore stigmatizing concepts among fathers of infants such as unintended fatherhood (Smith et al., 2022) and prenatal anxiety (Pilkington & Rominov, 2017). Additionally, researchers have used Reddit to examine fathers and expectant fathers’ use of the platform for support (Cameron et al., 2023; Cameron, Simpson, et al., 2025; Teague & Shatte, 2021) and to explore parenting expectations between mothers and fathers (Feldman, 2021). Each of these studies contributes to the body of knowledge related to new fathers’ mental health and support needs. To build on this knowledge, our study highlights fathers’ emotionally candid experiences with paternal postpartum depression specifically and contextualizes the concept, including its contributors, symptoms, and life impacts, as described by fathers who self-identify as experiencing it.
Notably, Eddy et al. (2019) used blogs, websites, and online forums, including Reddit, to understand fathers’ experiences with paternal PPD among 27 fathers. Despite this important work, an update to understanding this phenomenon is warranted. Social media use has increased substantially over the last 5 years. In 2019, Reddit had an estimated 430 million monthly active users, compared to 1.2 billion in 2024 (Statista, 2024). Furthermore, conversations related to paternal PPD have increased substantially within the media (Kindelan, 2024; Ruggeri, 2022; Ruggieri, 2023) and scientific communities (Fisher et al., 2021; Watkins et al., 2024). Although awareness is growing, paternal PPD is not formally classified as a distinct psychiatric disorder in the DSM-5-TR; thus, it is not routinely screened for or diagnosed worldwide (Bruno et al., 2020). Gaining a deeper understanding of how PPD presents in fathers is essential for improving detection and treatment.
Study Aim and Research Questions
This study updates and expands on our understanding of fathers’ experiences with paternal PPD through the following research questions:
(1) What factors do fathers report as contributors to their postpartum depressive symptoms?
(2) What are fathers’ reported postpartum depressive symptoms and the associated impacts on their lives?
Gaining a deeper understanding of the unique contributors, symptoms, and life impacts of paternal postpartum depression will help to inform more tailored screening, support, and intervention strategies for fathers during the postpartum period.
Methods
Study Design and Data Collection
We used a qualitative descriptive approach (Sandelowski, 2000) and collected data from the anonymous, open-forum, social media platform, Reddit. We selected Reddit due to its anonymity, topic-specific virtual communities (“subreddits”), and in-depth user narratives, which provided rich data for addressing our research questions (Choudhury & De, 2014). Further, it is an ideal data source for reaching fathers of infants because most (58%) users are between 18 and 34 years old and identify as male (57%; Proferes et al., 2021). We identified relevant subreddits including r/daddit, r/postpartum_depression, r/MensLib, and r/Parenting; subreddits are individual communities within the Reddit platform focused on specific content or interests where users can engage in discussions. We then used Pushshift application programming interface (API) using Python scripts in Jupyter Notebook (Baumgarterner et al., 2019) to scrape posts using the following subreddit and keyword combinations: r/daddit + postpartum depression, r/postpartum_depression + paternal, r/MensLib + postpartum, r/Parenting + postpartum depression. In addition, we searched all of Reddit, outside of these particular subreddits, for posts that included the key phrase “paternal postpartum depression.” The data were scraped on May 15, 2023.
We included only posts that were written from the self-identified father’s point of view in first person and were related to personal experiences with paternal PPD. To be included, posts had to include a clear indication that it was about a paternal postpartum depression experience by including the direct phrase “paternal postpartum depression” or similar (i.e., male postpartum depression) in the title or post thread and written by the father himself such as stating phrases like “I am a dad.” We identified 181 original posts with 28 meeting inclusion criteria. We then screened the comments on each of included original posts (total of 283) for additional relevant posts. After screening a total of 464 posts, we extracted 63 meeting inclusion criteria and combined them into one Microsoft Excel document. Original posts were posted between March 2015 and April 2023, with 76% occurring since 2019. Based on the data retrieved we were able to capture a reasonable range of experiences to address the research questions (Thorne, 2020).
Data Analysis
We imported each post as an individual case within NVivo 12 (Lumivero – Denver, CO) and engaged in inductive thematic qualitative analysis (Braun & Clarke, 2006). Initially, all authors independently engaged in “repeated reading” to familiarize ourselves with the data and get a sense of the whole. Next, we inductively generated initial codes related to contributors, symptoms, and impacts and systematically coded features of the data across the dataset. We met as a team at regular intervals over a 6-month period to discuss coding discrepancies. Symptom codes were then organized in alignment with DSM-5-TR diagnostic criteria where relevant, and a “masked symptoms” category was added based on a concept analysis of paternal postpartum depression (American Psychiatric Association, 2022; Chen et al., 2023). T.N.R and M.D.G. collated the codes into potential categories to answer each part of the research question. The team then, through iterative review, examined patterns across categories to develop themes and selected exemplar quotes. Finally, we reviewed, defined, and named the themes and presented the findings.
To enhance rigor and trustworthiness of our findings, we documented our process with a detailed audit trail and supplemented it with reflective memos post-coding sessions to foster reflexivity and discern data patterns (Tracy, 2010). All authors are registered nurses with professional experience in women’s and children’s health. During the data analysis phase, two authors were mothers (M.D.G. and C.C.) with one actively navigating the postpartum period (M.D.G.). All authors have experience caring for individuals experiencing postpartum depression and working in healthcare systems charged with meeting the needs of the entire family during the childbearing experience. These shared personal and professional experiences informed our sensitivity to postpartum issues and shaped our interpretation of paternal narratives, while also requiring us to remain critically reflective to minimize bias in analyzing fathers’ experiences. We engaged in investigator triangulation through a collaborative analysis approach (Carter et al., 2014) and upheld multivocality to ensure diverse participant perspectives were represented (Tracy, 2010). Although the data are publicly available and anonymized, we paraphrased quotes to protect the privacy of individuals posting in Reddit forums and to avoid discouraging others from engaging in this form of discourse (Proferes et al., 2021). Given the nature of the publicly available data, the study was deemed exempt by the University of North Carolina at Chapel Hill Institutional Review Board (ID 396174) and informed consent was not required.
Findings
Narrative excerpts from 63 fathers were included in this study. Given the excerpts were obtained from an anonymous online platform, we do not have demographic data for each father. However, some fathers voluntarily included information such as infant age, infant sex, number of children, etc. in their posts. Abstractable demographic data can be found in the Supplementary Material case table. The following findings outline contributors, symptoms, and impacts of paternal PPD as described by fathers who reported experiencing paternal PPD themselves. A visual representation of the themes is included in Figure 1.
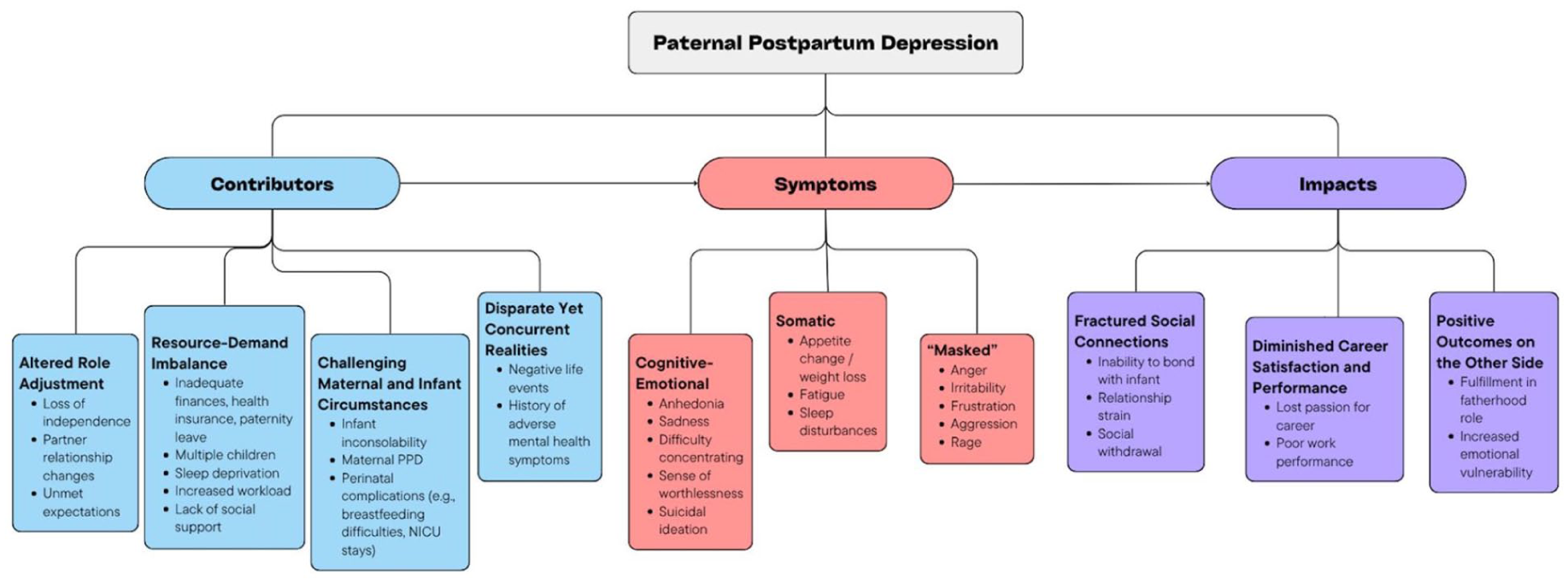
Examples of contributors, symptoms, and impacts within each theme.
Contributors
Contributors to experiencing paternal depressive symptoms were categorized into the following themes: (1) altered role adjustment, (2) resource-demand imbalance, (3) challenging maternal-infant circumstances, and (4) disparate yet concurrent realities.
Altered Role Adjustment
This theme encompassed fathers’ challenges with adjusting to the lifestyle changes that occurred as a result of having a new infant. Many fathers discussed their loss of independence, change in routine, and struggles with perceived identity shifts: After my daughter was born, I experienced some depression related to the major life transition—struggles in my relationship with my wife, financial pressures of raising a child, and the overall shift in lifestyle that comes with becoming a parent. (D22)
Another father similarly expressed: I’m doing my best to manage the depression, but it often feels overwhelming. I sometimes question whether I was meant to be a parent, feeling trapped in a cycle of grieving the loss of my personal freedom and sense of self. (D25)
Fathers also described difficulties in adjusting to changes in their relationships with their partners: I really miss feeling connected to my wife, both emotionally and physically. Even though I know things will improve over time, it doesn’t make the present any less difficult. (D36)
Many fathers discussed that the life change of having a new infant was not what they expected: Watching my friends bond so effortlessly with their children made me feel inadequate. I expected to feel the same joy and excitement with my own child but didn’t, which left me feeling upset and confused. (D51)
Resource-Demand Imbalance
This theme encompassed difficulties with perceived lack of resources, such as finances, health insurance, adequate paternity leave, and support, that were necessary to meet the demands of fatherhood. One father stated: Without access to paternity leave or vacation time, trying to keep up with work on top of everything else has been completely overwhelming and emotionally draining (D37). Another father similarly expressed: Paternal leave just isn’t taken seriously in today’s work culture. I had to work full time during the first two months after my baby was born. When I shared that with a female colleague, she dismissed it, saying I didn’t need leave since I wasn’t the one who gave birth. (D45)
One father described that his healthcare provider proved to be an inadequate resource for managing paternal PPD symptoms: When I went to the doctor about my depression, it confirmed my fears about the lack of support. Although he initially seemed concerned, once I mentioned I had a newborn, he brushed it off, saying what I was feeling was “normal” and that I just needed to toughen up. It felt dismissive and unhelpful. (D26)
Several fathers mentioned that having more than one child contributed to their depressive symptoms: I’m not sure if it was the constant sleep deprivation, caring for a baby and a toddler, or both, but everything spiraled downhill very quickly (D01). Fathers also mentioned their sleep deprivation during the infancy period contributed to their depressive symptoms – their infants demanded care while their bodies demanded sleep: Sleep deprivation, combined with a history of undiagnosed depression, left me mentally foggy. I struggled to think clearly, felt disconnected from reality, and questioned whether I even mattered. (D27)
Many fathers described the increased workload that came with having an infant and difficulties with maintaining it: It feels like I’m parenting alone. With my wife still recovering from a C-section, I’ve taken on nearly all the household responsibilities and most of the baby care. Although I’m not the one breastfeeding, I’m even needed for that piece of baby care, to burp the baby, clean up, or assist my wife while she’s unable to move freely. Even small tasks aren’t really off my plate. (D37)
Many fathers discussed feeling isolated and having a lack of social support, a resource known to be protective of mental health during the postpartum period (Cho et al., 2022; Feinberg et al., 2022): If there’s a support group for dads going through something similar, or even just a space to vent and feel less alone, I’d love to know. Right now, I feel like I’m barely staying afloat. (D19)
Another father stated: I’m sharing this here on Reddit because I don’t know where else to turn. My partner is incredibly supportive, but as the first one in my friend group to become a father, I feel isolated. I’m hoping to connect with others who understand what I’m going through. (D26)
Challenging Maternal and Infant Circumstances
This theme encompassed challenges fathers encountered related to infant temperament and perinatal complications. Many fathers described difficulties with handling negative infant temperament, including crying and inconsolability: When my baby cries, especially when she’s upset, the sound is so intense it triggers a sense of panic in me. I feel completely trapped and overwhelmed. (D25)
Another father stated: When I’m caring for our baby, I’m consumed by feelings of anger and resentment. I had hoped those feelings would fade over time and that I’d begin to bond with him, but instead they’ve only intensified. I find myself deeply disturbed by his constant crying and neediness. (D53)
Several fathers described the challenges with dealing with their partner experiencing postpartum depression: My wife is going through severe postpartum depression and is actively trying to heal. I feel like I can’t be honest with how I’m really feeling because I don’t want to add to her emotional burden. Instead, I suppress my emotions and operate on autopilot just to get through each day. (D36)
Some fathers also described challenges with navigating other perinatal complications including traumatic birth, unplanned pregnancy, infant loss, neonatal intensive care unit stays, and breastfeeding difficulties: My partner was unable to breastfeed, and although it wasn’t her fault, it caused her significant emotional distress. She felt like she was failing our son, and it often left her in tears. I supported her as best I could during my leave, but I only had two weeks of paternity leave and one week of vacation. It was incredibly difficult to watch someone I love suffer like that. (D26)
Disparate Yet Concurrent Realities
This theme encompassed fathers’ descriptions of situations that were not directly related to the perinatal experience but that exacerbated depressive symptoms for fathers during the postpartum period. Some fathers mentioned they experienced negative life events, unrelated to pregnancy or postpartum, occur during the perinatal period, which contributed to their PPD symptoms: My mother had a stroke just a month before our baby was born, and the emotional toll of that experience contributed to the onset of my own postpartum depression. (DR45)
Many fathers also described having a history of experiencing adverse mental health symptoms: I was diagnosed with depression 4 years ago, though I had been struggling even before then. I know what depression feels like (numbness, hopelessness, isolation), but what I’m experiencing now feels even more intense and debilitating than before. (D26)
Symptoms
We categorized symptoms fathers described according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) symptoms included in the diagnostic criteria for Major Depressive Disorder (MDD; American Psychiatric Association, 2022). We further categorized these symptoms into cognitive-emotional symptoms (anhedonia, depressed mood, difficulty concentrating, sense of worthlessness, and suicidal ideation) and somatic symptoms (appetite change, fatigue, and sleep disturbances). Lastly, we derived a category of “masked” symptoms, which are not included in the DSM-5-TR for MDD but encompass experiences of anger, irritability, frustration, aggression, and rage that have been documented among men experiencing depression (Chen et al., 2023).
Cognitive-Emotional Symptoms
Several fathers described experiencing anhedonia, including a loss of pleasure, interest, or enjoyment: I no longer find joy in anything. For over a year, life has felt flat and colorless. Food has lost its flavor, music is just irritating, and even the idea of watching a movie feels exhausting. I can’t even tolerate my dog’s energy and enthusiasm. It’s all too much. (D23)
Most fathers reported experiencing depressed mood including feeling sad, low, nothingness, or emptiness: Since my son was born, I’ve felt like I’m sinking into a deep, joyless sadness. Everything feels dull and lifeless (D23). Some fathers described difficulty concentrating, thinking, or making decisions: My wife noticed right away how disconnected I had become. I would often stare off into space while she was talking, completely disengaged from the moment (D51). Many fathers described experiencing a sense of worthlessness or inappropriate guilt: Lately, I’ve been crying uncontrollably and feeling incredibly useless. Even though my fiancée reassures me that I’m doing well, I can’t shake the fear that I’m not cut out to be a good father (D58). About 11% of fathers in our study expressed experiencing thoughts of suicide or self-harm: I’m having disturbing thoughts about harming myself and my baby, and it’s terrifying. I know something is seriously wrong, and I don’t know how to cope (D53). Another father stated:
There were times when I was so sleep-deprived and overwhelmed by work and parenting that, while driving home, I would imagine veering into trees just to make everything stop (D54).
Somatic Symptoms
Few fathers reported experiencing appetite changes or unintentional significant weight loss or gain: I’ve unintentionally lost 20 to 30 pounds in just a month, likely because I honestly can’t remember the last time I ate a real meal (D20). Some fathers described experiencing fatigue or exhaustion: I’m constantly exhausted, no matter how much I sleep. Before having a baby, I could wake up early and work out with energy and enthusiasm, but now, just getting out of bed feels impossible (D05). Some fathers also described sleep disturbances, aside from waking for infant care responsibilities, including experiences of hypersomnia or insomnia: Even though my child sleeps through the night, I haven’t gotten more than 4 or 5 hours of sleep in nearly a year. I wake up at 4 a.m. automatically, like it’s a stress response. I lie in bed with anxiety attacks, dreading the day ahead, worried about how overwhelming and exhausting it will be. I hate feeling this way about my life. (D25)
Masked Symptoms
Many fathers provided reflections about experiencing episodes of anger, irritability, frustration, aggression, and rage oftentimes toward the infant: Even the smallest noise from my kids instantly puts me on edge. I’m overwhelmed by intense anger that feels irrational and frightening. I know they’re just babies who can’t help how they express themselves, but that doesn’t stop the constant waves of rage and frustration that feel like they’re wearing down my sanity. (D19)
Another father stated: I understand that paternal depression is real, but right now it feels like I don’t matter. On top of everything, I can’t even step away to decompress. I’m stuck, trying to manage this growing anger, and even borderline hatred, toward my baby, and I don’t know how to deal with it. (D29)
Impacts
Fathers described how their depressive symptoms impacted their lives. We categorized these impacts into the following themes: (1) fractured social connections, (2) diminished career satisfaction and performance, and (3) positive outcomes on the other side.
Fractured Social Connections
This theme encompassed fathers’ descriptions of how their experiences with symptoms of paternal PPD impeded their abilities to foster relationships with their children, partners, families, and friends. Many fathers described their inability to bond with their infant: At first, I really struggled to connect with my baby. I didn’t want to hold or show affection toward him, and it made me feel abnormal. Deep down, I was terrified that if I did form a bond and something happened to him, the pain would completely destroy me. (D51)
Several fathers mentioned that their experience with paternal PPD symptoms caused strain on their relationships: Since my son was born nearly a year ago, I’ve felt constantly overwhelmed. That stress took a serious toll, and it ended up destroying my marriage (D46). Some fathers also described experiencing social withdrawal as a result of experiencing depressive symptoms: Male postpartum depression is absolutely real. I’m experiencing it myself, and it’s caused me to pull away from both friends and family (D14).
Diminished Career Satisfaction and Performance
This theme encompassed fathers’ descriptions of how their experiences with symptoms of paternal PPD negatively affected their career satisfaction or work performance. One father stated: I’ve completely lost interest in my career and abandoned the hobbies and goals that used to matter to me. Now, I just go through the motions of going to work, putting in my time, and coming home (D23). Another father stated: I’m struggling at work because I never get a chance to recharge or feel mentally stable. There’s no time in the day to come back to myself (D53).
Positive Outcomes on the Other Side
This theme encompassed fathers’ descriptions of their experiences with eventual positive outcomes and feeling fulfilled in their fatherhood roles after experiencing paternal PPD symptoms. One father stated: After months of intense paternal postpartum depression, therapy, and trying a new antidepressant, I’ve finally come out the other side, and I feel genuinely good. My daughter is now 18-months-old, and I’ve embraced being a stay-at-home dad. I’ve really grown into and accepted this role. (D33)
Another father stated: Going through this experience has made me more emotionally open with my friends and family. I promised my wife that once I recovered, I’d try to help others by speaking out. Paternal postpartum depression is real, and no one should feel they have to suffer in silence. (D51)
Another father stated: I believe that experience really enhanced my emotional intelligence, and as a result, I’m now better equipped to be a supportive husband and father (D04). Additional paraphrased narratives are included in the Table 1.
Additional Paraphrased Narratives Illustrating Themes.

Discussion
Our findings highlight contributors, symptoms, and impacts of paternal PPD experienced by fathers as evidenced by anonymous posts on Reddit. Notably, over three-quarters of the posts in our sample were published after 2019, potentially reflecting multiple factors such as an increased prevalence of paternal depression, a heightened need for support, and greater awareness and recognition of men’s mental health, including paternal postpartum depression, since the COVID-19 pandemic (Cameron, Joyce, et al., 2025; Ellison et al., 2021; Gottert et al., 2022).
Many of the identified contributors to paternal PPD related to the burden within fathers’ roles to provide for their family financially, support their partner, and participate in infant caregiving. This finding aligns with previous qualitative studies in which fathers have highlighted the pressures of being the family supporter by assuming multiple roles including emotional supporter, “breadwinner” and caregiver (Griffith et al., 2025; Murray Cunningham et al., 2024). Other contributors were structural, such as lack of support for fathers in the perinatal period culturally and within healthcare systems, including but not limited to, lack of trained mental health providers in issues specific to fathers, no recommended follow-up or screening for fathers in the postpartum period, and policies that hinder smooth transition to parenthood and inequitably affect fathers.
The paternal PPD symptoms fathers described in our study align with those that have been reported in previous studies including cognitive-emotional (e.g., low mood), somatic (e.g., exhaustion), and “masked” symptoms (e.g., irritability; Chen et al., 2023; Davenport et al., 2022; Davenport & Swami, 2023b; Macdonald et al., 2020). Regarding “masked” symptoms, due to masculine norms, men experiencing depression tend to “mask” their symptoms, which may manifest as risk-taking behaviors (e.g., substance use) or aggression and irritability (Chen et al., 2023). While fathers in our sample did not commonly report engaging in behaviors such as substance use as has been previously documented (Chen et al., 2023; Recto & Champion, 2020; Recto & Lesser, 2021), many described experiencing anger, frustration, and violent thoughts that were often directed toward the infant. While infant resentment has been described in previous studies in the context of paternal PPD (Chen et al., 2023; Davenport et al., 2022; Eddy et al., 2019), analyzing anonymous reflections of fathers’ experiences, beyond the work conducted by Eddy et al. (2019), provided a unique opportunity to uncover the severity of these feelings. Additionally, we were able to understand the potential impact of paternal PPD symptoms including infant harm given it is plausible fathers may not share these thoughts without anonymity for fear of judgement or potential consequences. It is also important to note that about 11% of fathers in our study reported experiencing suicidal ideations. A previous study found that men who experienced paternal PPD had a 45% increased suicide risk compared to men not experiencing mood disorders (Quevedo et al., 2011). These realities highlight the importance of increasing awareness and supporting fathers’ mental health to mitigate potential negative outcomes for fathers and their families.
Fathers in our study described that Reddit was their “only place to turn” or their “only hope,” identifying the lack of awareness and support for paternal PPD. This lack of awareness and support creates a barrier to fathers seeking help for their symptoms (Reay et al., 2023); untreated paternal postpartum depression can negatively influence the well-being of the father and his family (Mahmoud et al., 2024). Additionally, there is a lack of training for mental health providers related to caring for fathers experiencing paternal mental health issues (Fisher et al., 2021). Developing and testing curricula for training health professionals is necessary so that fathers may equitably benefit from evidence-based care during a vulnerable time in their lives when they and their families are at risk for harmful consequences. Further, psychoeducational interventions delivered by nurses have been shown to improve paternal mental health (Park et al., 2020). Nurses are well-positioned to begin educating families during the prenatal period about paternal PPD and share resources to increase awareness and provide support for fathers (Davenport & Swami, 2023a; Melrose, 2010). For example, settings where fathers are often present, such as prenatal ultrasound appointments or postpartum recovery units, offer ideal opportunities for educating families about paternal PPD (Walsh et al., 2017). In cases where this falls outside the scope of a nurse’s expertise, they should collaborate with other professionals to ensure that fathers’ mental health needs are properly assessed and addressed (Davenport & Swami, 2023a).
Assessing and addressing fathers’ mental health needs begins with screening. It is critical to increase screening efforts for paternal PPD to identify fathers at risk and connect them with appropriate resources and professional support. Additionally, given that the estimated 10% of fathers experiencing depressive symptoms in the postpartum period is likely an underestimate (Fisher, 2017; Rao et al., 2020), increasing screening efforts would allow us to obtain more accurate estimates of the paternal PPD prevalence. The Edinburgh Postnatal Depression Scale (EPDS), for example, has been validated in fathers (Matthey et al., 2001; Shafian et al., 2022), and the Edinburgh Postnatal Depression Scale-Partner (EPDS-P) was created to detect paternal depression through maternal report (Fisher et al., 2012). While useful, these tools do not capture men’s experiences of depression, which often manifest as anger, aggressiveness, or engaging in risk-taking behaviors (National Institute of Mental Health, 2017; Philpott, 2023). They can be supplemented with other measures that assess such behaviors such as the Masculine Depression Scale and Male Depression Risk Scale (Fisher & Garfield, 2016), but ultimately, there is a need to create validated tools that are specific to fathers’ experiences with paternal PPD.
In addition to exploring contributors to and symptoms of paternal postpartum depression, we also examined the perceived impacts of paternal PPD on fathers’ lives. While we focused on how fathers described impacts as circumstances that occurred due to experiencing symptoms of paternal PPD, in some cases it was difficult to determine whether a given experience (e.g., inability to bond, relationship strain) was a contributor, symptom, or impact. In other words, while certainly part of the father’s experience, sometimes it was difficult to decipher in what sequence the experiences happened. Nonetheless, paternal PPD has been shown to have lasting negative effects on fathers, infants, and families beyond the first year postpartum (Fisher et al., 2021; Scarff, 2019). Thus, it is critical to employ a more holistic approach to postpartum care by considering fathers’ mental health as imperative in supporting the development of healthy families, not only in clinical settings but also through health policy efforts that recognize and address paternal mental health needs.
While gender role norms are shifting and infant engagement is becoming more common for contemporary fathers, many national and workplace policies limit fathers’ abilities to fully embrace new parenthood (Petts & Knoester, 2019). Fathers in our study expressed that parental leave was not valued in society, a notion that is confirmed by family leave policies in many countries. For example, the United States has no federal policy for paid leave for new parents (Boston College Center for Work and Family, 2019), and only 13 states and Washington D.C. have paid family leave programs (Glynn, 2023). Further, just 27% of all U.S. workers have paid family leave benefits provided by their employers, while only 13% of private sector workers have access to paid paternity leave (Fathers Need Paid Family and Medical Leave, 2025), revealing that policies, albeit limited in support for all parents, provide even less support for new fathers.
There are many reasons why paternity leave can be beneficial for fathers and families. While on leave, fathers have more time to bond with their infants, learn parenting skills, and develop strong co-parenting relationships with their partners (Boston College Center for Work and Family, 2019; Petts & Knoester, 2019). Additionally, while on leave, fathers can share the increased workload of infant caregiving within the home to decrease the burden on the mother. Division of household labor during the postpartum period has been associated with lower levels of adverse mental health symptoms (Pilkington et al., 2015). Ultimately, longer paternal leave has been associated with increased mental well-being for both parents (Philpott et al., 2022). Our findings underscore the importance of advocating for inclusive parental leave policies that support both mothers and fathers, promoting healthier family systems.
Limitations
While our study has several strengths, most notably the richness of anonymous data, there are some limitations to note. First, we acknowledge that the use of Reddit as a data source may exclude fathers with limited digital access, English proficiency, or literacy skills, which could influence the representativeness of the perspectives captured. Second, given the anonymous nature of the data source, participant demographics were unknown unless voluntarily included in the narrative. Thus, we could not analyze how demographic characteristics might relate to participant experiences. Not being privy to demographic information compelled us to remain close to participant voices and refrain from extensive interpretation, consistent with the study design (Sandelowski, 2000). However, this limits our ability to explore how intersecting identities, such as race, income, nationality, and gender identity may shape the mental health experiences of fathers. Future research should incorporate targeted data collection that enables more nuanced examination of how these demographic factors intersect and contribute to diverse paternal experiences. It is also important to note that we referenced United States culture and policies in this paper. However, we recognize the narratives posted on Reddit could come from fathers across the globe though demographics were largely unknown. Additionally, our search was limited to posts that populated from using search terms such as “paternal” and “paternal depression” for the purposes of not mis-representing the concept. However, it is likely that we did not capture all posts on Reddit describing fathers’ first-hand experiences with paternal postpartum depression. Finally, many symptoms attributed to paternal PPD may overlap with other mental health conditions (Falah-Hassani et al., 2017) meaning the findings may reflect broader paternal perinatal mood disorders rather than postpartum depression specifically.
Conclusion
Many fathers experience depressive symptoms during the postpartum period due to altered role adjustment, resource-demand imbalances, challenging maternal and infant circumstances, and disparate yet concurrent realities. Symptoms of paternal PPD can include cognitive-emotional and somatic symptoms, but often manifest as “masked” symptoms, such as irritability, anger, and aggression. When paternal PPD is left untreated, there can be serious consequences for the entire family. Yet, fathers are often under-supported during this sensitive period of adjustment. There is a critical need to increase awareness of and support for paternal PPD to promote healthy fathers and families.
Supplemental Material
sj-pdf-1-gqn-10.1177_23333936251374618 – Supplemental material for “Whispered on Only the Darkest Corners of the Internet:”: A Qualitative Descriptive Study Exploring Fathers’ Experiences with Paternal Postpartum Depression on Reddit
Supplemental material, sj-pdf-1-gqn-10.1177_23333936251374618 for “Whispered on Only the Darkest Corners of the Internet:”: A Qualitative Descriptive Study Exploring Fathers’ Experiences with Paternal Postpartum Depression on Reddit by Taylor N. Richardson, Michelle D. Graf, Lauren Hicks and Courtney Caiola in Global Qualitative Nursing Research
Footnotes
Acknowledgements
The authors thank Dr. Dan Hiaeshutter-Rice for his assistance with scraping the data.
Author Contributions
T.N.R.: Conceptualization, Methodology, Software, Formal Analysis, Investigation, Data Curation, Writing – Original Draft, Writing – Review & Editing, Visualization, Project Administration, Funding Acquisition; M.D.G.: Software, Formal Analysis, Investigation, Writing – Review & Editing, Visualization, Funding Acquisition; L.H.: Software, Formal Analysis, Investigation, Writing – Review & Editing, Funding Acquisition; C.C.: Software, Formal Analysis, Investigation, Writing – Review & Editing, Visualization, Supervision
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work of Drs. Taylor N. Richardson, Michelle D. Graf, and Lauren Hicks on this project was supported by the National Institute of Nursing Research under award number T32NR007091. This content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used ChatGPT to tweak some of the theme names to improve readability and to paraphrase direct quotes. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.