
Abstract
Communication difficulties experienced by people with aphasia (PWA) cause disconnects between meaningful conversations and care received. The purpose of this study was to identify concepts PWA define as (1) the most critical facilitators to transitional care and communicative access success, and (2) transitional care and communicative barriers. A qualitative descriptive study design was utilized. Semi-structured interviews were conducted with six PWA and two communication partners and analyzed using directed content analysis, guided by the theory of Human Scale Development. Findings revealed that barriers and facilitators centered on three Needs: (1) Participation: Participation in life events was directly related to public understanding of aphasia; (2) Protection: Healthcare services failed to provide necessary care, and participants relied on themselves to gain access to healthcare; and (3) Understanding: Healthcare conversations were described as one-sided, with successful healthcare interactions being mediated by empathic responses. Results identified how successful navigation of stroke care for PWA are complex and multifaceted processes. Findings affirm the importance of effective communication in healthcare. Participants call to action the need for healthcare professionals to be better educated on accessible communicative strategies.
The profound impact of language loss is often felt by individuals with chronic post-stroke aphasia. Stroke affects roughly 795,000 Americans every year (Martin et al., 2023), and aphasia is present in approximately one-third of those individuals (Flowers et al., 2013). Post-stroke aphasia occurs when damage in language centers in the brain causes comprehension and expression language deficits. Aphasia can interfere with an individual’s capacity to understand and communicate spoken or written language while other cognitive and social skills may still be preserved (Loft et al., 2022; O’Halloran et al., 2012). Diagnosis of aphasia is associated with increased lengths of stays in acute care, increased in-hospital mortality, and a higher risk for complications while hospitalized (Flowers et al., 2013; Lazar & Boehme, 2017; Wu et al., 2020). Providing care for people with aphasia (PWA) is challenging for healthcare professionals for various reasons (Carragher et al., 2021; Hur & Kang, 2022; Loft et al., 2017, 2022). Aphasia is heterogenic in presentation and, therefore, may require utilization of different communication methods (e.g., gestures, written language, verbal) to facilitate accessible and effective conversation. Thus, difficulties can arise in rapid-paced healthcare settings where the amount of time healthcare workers can spend with individuals is limited.
The term “healthcare professionals/workers” is employed throughout the manuscript. This broader terminology provides insight into the diverse roles and contributions of all professionals involved in patient care. However, it is crucial to acknowledge the pivotal role that nurses play in creating an inclusive healthcare environment for PWA. Nurses commonly serve as communication partners for PWA across various healthcare settings, as they have more frequent daily interactions with PWA (D’Souza et al., 2021). Interprofessional collaboration is essential for achieving optimal patient outcomes, and the distinct contributions of nurses are indispensable within this collaborative framework. While the responsibility of ensuring communicative access is shared among all healthcare professionals, the consistent presence of nurses in the healthcare process provides invaluable opportunities for facilitating effective communication and creating an inclusive healthcare environment for PWA.
Several recent studies have highlighted the difficulties PWA face in healthcare settings and demonstrate the inadequacies and inaccessibility of healthcare services for both PWA and their care partners (Carragher et al., 2021, 2024; Hersh & Armstrong, 2021; Loft et al., 2022; Rose et al., 2019). Additionally, the evidence suggests that care partners and families of PWA are not provided with enough support or education to manage long-term stroke care for their loved ones (Grawburg et al., 2013; Hersh & Armstrong, 2021; Rose et al., 2019). Transitional care interventions are sets of actions created to address gaps in healthcare and ensure coordination and continuity of care as individuals transfer between different locations or levels of care
Failure to incorporate PWA in care decisions also poses ethical and moral concerns. Government and accrediting bodies have created guidelines, mandates, and laws to facilitate equal access for individuals with disabilities (e.g., Americans with Disabilities Act., 1990; The Joint Commission, 2024). A wealth of evidence suggests healthcare accessibility could be improved for PWA through training healthcare workers on Supported Conversation for Adults with Aphasia (SCA™), an evidence-based set of skills and techniques to encourage and facilitate conversation with PWA (Heard et al., 2017; Horton et al., 2016; Kagan et al., 2001, 2024; Lee & Azios, 2020; Power et al., 2020, 2024; Simmons-Mackie et al., 2007; Sorin-Peters et al., 2010). SCA™ uses a variety of techniques to acknowledge and reveal the competence of PWA. Examples of these techniques include simplifying language, using visual aids, using appropriate tone of voice, gestures, and providing opportunities for turn-taking (Kagan, 1998). However, current literature shows that US healthcare systems have not adequately integrated these techniques into clinical practice.
Little is known about the complex care coordination efforts PWA experience after stroke and the influence that healthcare workers have on care transition success and engagement for PWA across the care continuum—spanning acute care to outpatient or community settings. Identifying the magnitude of the gaps in care coordination and communicative access PWA face is essential to improving patient outcomes and for generating future transitional care interventions. Currently, no research explores the experiences of care transition and communicative access from the perspective of people with varying severity of aphasia and their communication partners. Additionally, no current evidence describes the barriers and facilitators of care transition and communicative success from the perspectives of people living with post-stroke aphasia. The overall purpose of this study was to identify, from the perspective of PWA, concepts which they define (1) as the most critical facilitators to transitional care and communicative success, (2) as transitional care and communicative barriers.
Methods
A qualitative descriptive study design (Sandelowski, 2000, 2010) was employed for this inquiry to directly capture the experiences of participants with communicative access and transitional care in healthcare settings. This method allowed for a detailed exploration of the phenomenon of transitional care and communicative access barriers and facilitators from the perspective of subject matter experts. A theoretical approach was instrumental in this study, providing structure to organize the qualitative descriptive methods. Theory guided the development of semi-structured interview prompts and the initial coding scheme, as well as informed the construction of relationships between codes. The theory of Human Scale Development (Max-Neef, 1991) served as the theoretical framework for this study. Human Scale Development provides a taxonomy of nine fundamental human needs along with examples of satisfiers of these needs. The nine fundamental needs (i.e., subsistence, protection, affection, understanding, participation, leisure, creation, identity, and freedom) exist as a system of interactive and interrelated components. The system has no hierarchy except for the need for subsistence (i.e., to stay alive). For individuals with aphasia (PWA), the challenges posed by communication impairments can significantly impact their ability to fulfill fundamental human needs. Inaccessible communication, disruptions in social interactions, and diminished self-esteem can arise from these communication barriers (Hilari & Northcott, 2006; Zanella et al., 2023). The theory of Human Scale Development provides a robust framework for addressing these challenges By focusing on meeting fundamental human needs through community participation, the theory of Human Scale Development shifts the focus from the individual’s limitations or disabilities to their capability. Further, needs are not viewed solely as indicators of individual or collective shortcomings in Human Scale Development; they can also signify potential strengths of an individual or collective. Emphasis can, therefore, be placed on building supportive communities and creating more inclusive environments where PWA can meaningfully participate. Thompson and McKeever (2014) have also synthesized this theory into the nursing discipline and provided a theoretical framework for using the theory of Human Scale Development in nursing interventions for PWA. Building upon this emphasis on inherent human potential rather than limitations and considering Thompson and McKeever’s (2014) synthesis within nursing for PWA, our analysis focused on the three fundamental needs that were prominent in the participant data and current literature on transitional care and communicative access: Participation, Protection, and Understanding. These three concepts provided the most insightful lens through which to understand the critical facilitators and barriers to successful transitional care and communicative access for PWA within the scope of this study. Thus, Human Scale Development (Max-Neef, 1991) served as a framework for this study to expand on their previous theoretical work and seek the perspectives of PWA to illustrate how the healthcare system satisfies or inhibits the fundamental human needs of people experiencing aphasia.
Recruitment
Recruited participants met the following inclusion criteria: ≥18 years of age, self-reported diagnosis of aphasia caused by a cerebrovascular accident ≥4 months before participating, and self-reported pre-morbid fluency in written and/or spoken English. The duration of at least 4 months post-onset of aphasia was selected to establish aphasia chronicity. Participants were also asked if they wished to have their communicative partner join in the interview process. Individuals who wished to participate without a communicative partner or support person were not excluded. Communicative partners and/or support persons who were ≥18 years of age, self-reported being the primary care partner or communicative/support partner for the individual with aphasia, and fluent in reading and speaking English were eligible to participate. Communicative access was ensured for every individual participating in the interviews. As communication partners may have differing opinions and suggestions than individuals with aphasia, careful consideration was taken to ensure each participant was the protagonist of the interviewing sessions. This study was reviewed and approved by the Institutional Review Board at Portland State University (227809-18) on August 01, 2022. Verbal informed consent was obtained from each participant and communicative partner before any data was collected. The consent process detailed the study’s purpose, procedures, risks, and benefits, and importantly, emphasized the participants’ right to withdraw from the study at their discretion.
Voluntary, purposive sampling was conducted through Portland (Oregon) metropolitan support groups for PWA and their care partners. Recruitment efforts occurred in partnership with the Aphasia Lab research team at Portland State University through newsletters, fliers posted in the Aphasia lab, and social media postings. The Aphasia Lab at Portland State University is a research facility located in downtown Portland dedicated to advancing scientific understanding of aphasia. While the Aphasia Lab does not provide direct clinical services, it offers research opportunities for PWA. Clinical speech-language therapy and community support group options for people with aphasia (PWA) and their care partners are available through the broader Speech and Language Department at Portland State University. Subjects were invited to participate in an audio-recorded semi-structured interview in person at the Aphasia Lab to ensure real-time communicative access through multiple communicative modalities (e.g., writing down keywords, gestures, drawing). If participating in person was not accessible or feasible for the participants, interviews were offered to be conducted over Zoom. Only one interview was conducted via Zoom. Interviews were conducted by the same feminine-presenting nonbinary, baccalaureate-prepared interviewer who studied and was employed in neuroscience nursing. The interviewer was trained in SCA™ and utilized multiple methods (e.g., shortened sentences, writing, gestures, etc.) to acknowledge the competence of the PWA and to support the participant’s expression of their thoughts. The researcher conducting the interviews was a graduate student researcher affiliated with Washington State University with no prior relationship with the participants. All other researchers were faculty members affiliated with Washington State University or Portland State University who had no direct contact with the participants for this study. Participant anonymity was maintained throughout the research process. Participants were assigned unique identifiers, and all identifying information was removed from data collection and analysis materials. Confidentiality was ensured by storing all data securely on password-protected computers, in accordance with IRB guidelines, with firewall-protected servers accessible only. As an act of reflexivity and disclosure or potential sources of research bias, this project was formulated from the personal experiences of the interviewer/researcher who identified as the primary care partner to an individual experiencing aphasia.
Procedure
Data collection occurred from May to July 2023. An interview guide was created, and audio recorders were used for the semi-structured interviews. Prompts and targeted questions in the interview guide were open-ended, with a loose organizing structure guided by tenets of the theory outlined in the section above. Topics for the 12, open-ended questions explored the type of communication encountered during healthcare interactions, barriers and facilitators to quality communication healthcare settings, barriers and facilitators to accessing healthcare, and explored suggestions for improvements to healthcare interactions/communication for PWA.
Interviews were audio recorded and lasted 60 to 90 min. Each interview lasted until the participant had enough time to fully convey their experiences with communicative access and transitional care in the healthcare system. While the concept of data saturation is debated in applied healthcare research (Braun & Clarke, 2021), our sample of eight participants (i.e., four individuals and two dyads) exhibited sufficient diversity across key dimensions (i.e., healthcare access, caregiver support, aphasia duration/severity, and age at diagnosis) to address study objectives. These dimensions of diversity allowed for a nuanced understanding of PWA’s perspectives on transitional care and communication challenges—specific to the represented sample (see discussion section for more on the limitations of the sample). Participants were given a $30 gift card as a thank you for their participation.
Interviews occurred in a quiet, private room after informed consent was verbally obtained from participants and any accompanying communicative partner. Participant interviews were professionally transcribed. Detailed field notes were recorded during and upon the conclusion of the interview. Detailed field notes served multiple purposes. First, field notes recorded nonverbal communicative expressions or difficulties with verbal communication occurring during the interviews. This feedback and familiarity with the interviews provided guidance when minor revisions to the transcriptions were warranted. Audio recordings were reviewed by the interviewer and field notes were expanded upon based on both the verbal and nonverbal communication modalities expressed by the participant to give a rich, narrative of the thoughts conveyed by each participant using principles of SCA™. An example of these detailed field notes is provided below (Field note_003):
He hits his palm against the table as he begins his sentence: Basically, healthcare. . . I have to because they say (points to the word doctors on the page) . . . and they say (points to the wall parallel to him; the location of the computer room where his mom is located during the interview) . . . I have to. That’s it. And healthcare. Wait and wait and wait and wait.
I clarify what he is saying again by rephrasing what I believe he said. He agrees. He then begins to use non-verbal communication methods to describe what the healthcare workers do when he goes to be assessed by them. He takes his hand and gestures like he is stabbing his arm with a vaccine. He puts his hand over his heart to illustrate the auscultation of heart sounds.
Field notes also served as a method for documenting memos and reflexivity journals after each interview.
Analysis
Directed content analysis was utilized according to the description provided by Hsieh and Shannon (2005) to analyze the transcribed documents. A directed approach to content analysis is more structured and elaborates on existing theories or prior research that may be incomplete. The fundamental needs, identified in the theory of Human Scale Development, guiding this study provided direction for the construction. All data were deidentified and stored using only subject identification numbers. Before coding any text, a coding manual was created based on the guiding theoretical framework, a review of literature, and a preliminary review of the first two transcripts. The coding manual was revised iteratively before being utilized to recode previously coded data. This process involved reading and rereading the text multiple times until all meaning units (i.e., segments of text containing a single idea) were successfully captured with first-level codes. First-level codes consisted of predominately descriptive, In Vivo, and conceptual coding (Miles et al., 2020). Second-level coding grouped conceptually similar codes together into concepts and categories. All transcripts were read by at least two coders, and codes were reviewed by a third member of the research team. Meetings to discuss or resolve any discrepancies in coding were held by the coding team until each member was satisfied that the codes and concepts fit the data. When consensus was achieved, findings were presented as supporting statements with illustrative, deidentified quotations. Presentation of thematic quotations is recommended to improve the clarity, accessibility, and utilization of the findings to guide future research (Sandelowski & Leeman, 2012). Multiple tactics were utilized to derive conclusions, thereby supporting the rigor of the study findings. These tactics include noting patterns, clustering, data displays, literature triangulation, analytic memos, and checking for researcher effects. Standards for reporting qualitative research (SRQR) were followed in the creation of this publication (O’Brien et al., 2014).
Trustworthiness
Steps were taken to reduce the impact of observer bias including: (1) highly structured and routine collection of data with one interviewer, (2) triangulating data with guiding theoretical frameworks and literature, (3) seeking guidance and feedback from research mentors and experts, (4) incorporating reflexivity journals to critically analyze positionality at each step of the process, (5) documenting analytic memos throughout the research process, and (6) continuous incorporation and documentation of informal participant validation strategies, such as discussions during the interview to assess and challenge the researcher’s interpretations of the data (see field note example in Methods section for more context).
Results
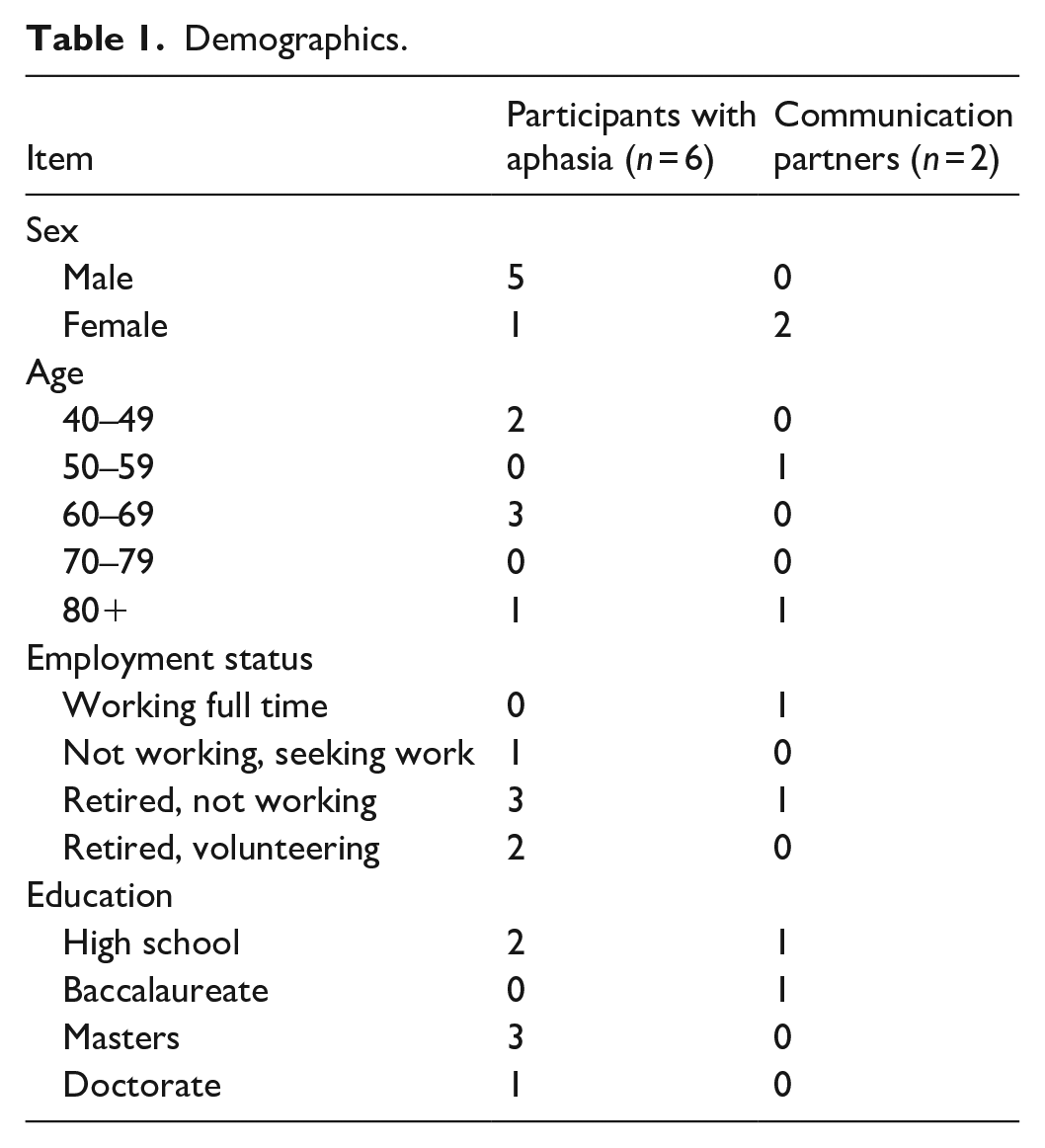
Six persons living with aphasia agreed to participate in this study, and two communication partners agreed to support communication during the interviews. The demographics of this sample are further described in Table 1. Three participants self-reported their aphasia symptom severity to be “mild,” one participant reported their aphasia as “moderate,” and two reported their aphasia symptoms to be “severe.” Two participants were joined by their communication partners.
Demographics.
A summarized clinical profile of relevant aphasia symptoms for most participants is provided in Table 2 using limited Comprehensive Aphasia Test (CAT; Swinburn et al., 2023) scores to give more context to the types of aphasia impairments the participants experience. Data on CAT scores were obtained for participants who previously consented to share data across studies within the Aphasia Lab. These data were not available for all six participants diagnosed with aphasia. Where standardized tests often focus on specific linguistic domains (e.g., comprehension, naming), these categories may not holistically capture the full spectrum of communication difficulties faced by PWA. Standardized tests may also exhibit limited sensitivity for individuals with mild or severe aphasia due to underrepresentation of these populations in test development samples. Consequently, these tests may lack precision in assessing the full range of aphasia severity, particularly for individuals with milder or more severe forms of the condition. Perceived aphasia severity is complex and influenced by factors beyond linguistic deficits (e.g., personal and professional identities, activity preferences, psychosocial impact, family support or lack thereof, emotional or financial stability). These factors significantly influence an individual’s subjective experience of aphasia and their perception of symptom severity. For example, Participant 1 experienced significant communication challenges in their daily life despite scoring in the unimpaired range for all subtests on the CAT. While their overall scores suggest unimpaired language function, their Naming subtest score is close to the cut-off, potentially indicating a subtle decline in expressive language skills compared to their baseline performance. This highlights the crucial role of considering self-reported symptom severity as a valuable reflection of the lived experience of aphasia alongside standardized test scores.
Participant Scores of Comprehensive Aphasia Test (CAT).*
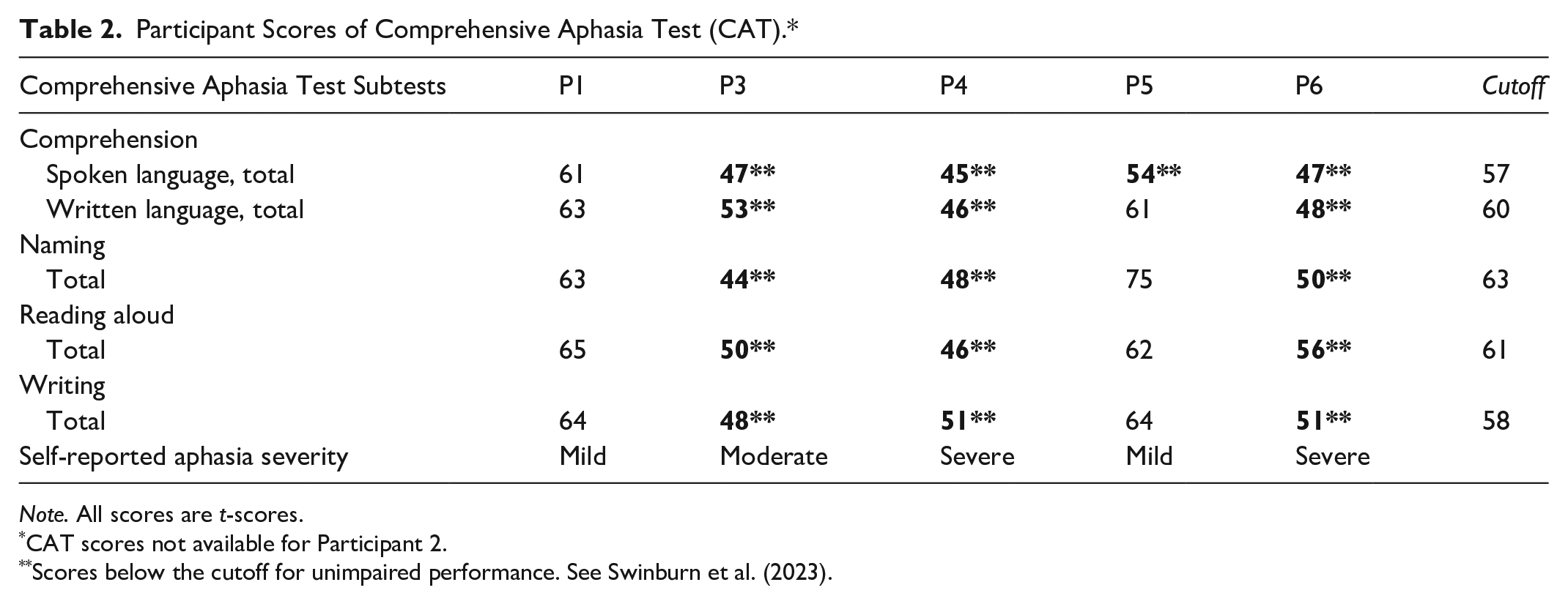
Note. All scores are t-scores.
CAT scores not available for Participant 2.
Scores below the cutoff for unimpaired performance. See Swinburn et al. (2023).
Most participants with aphasia within the sample self-reported their gender to be cisgender male (83%). Communicative partners self-reported to be cisgender female (100%). The sample was entirely comprised of individuals who self-identified their race as non-Hispanic white (100%). The mean age of the sample was 60.2 years, representing a sample relatively younger compared to the average age at stroke (i.e., 69.2 years; Kissela et al., 2012). Time since stroke event that caused aphasia symptoms ranged from 5 months (n = 1) to 11 years (n = 2) prior to interview, with three participants reporting stroke within the 2 to 3-year timeframe. Stroke type was reported as a left-sided ischemic cerebrovascular accident for all participants experiencing aphasia. English was reported as the first language for all participants with aphasia and their communication partners. Patient-centered supporting statements are presented in the headings of the three Needs, guided by the theory of Human Scale Development (Participation, Protection, Understanding; Max-Neef, 1991). Findings are described below with headers for the fundamental needs and supporting statements. Barriers and facilitators are presented for each fundamental need. To maintain an uninterrupted narrative for the reader, barriers are presented first, followed by facilitators. A diagrammatic representation of the summarized results is also presented in Figure 1.

Summary of barriers and facilitators to transitional care and communicative access for PWA.
The Need for Participation
Within the framework of the theory of Human Scale Development, the fundamental human need for participation is satisfied by interacting, expressing opinions, and sharing in settings of participative interaction (Max-Neef, 1991). Using the conceptualization of participation provided in Human Scale Development, barriers and facilitators to participation are described below.
Barriers
Participants reported their participation in social interactions were significantly impacted by public perceptions of aphasia and a lack of post-stroke aphasia representation in public discourse. Lack of public understanding created anxiety. The Communication Partner for Participant 4 described their anxiety when interacting with the public: And a lot of people don’t know what aphasia is without telling them my husband has aphasia. He needs a moment to talk. You know. . . it’s just a lot for a person. Participants described the complexities of navigating life in their communities with this public misperception of their communicative and cognitive abilities. Participant 2 described these complexities: We’re like lepers. . . Like, it’s like you’re lepers. And this is the issue. Participant 5 stated: If you’re not hurt or you’re not seen, you’re invisible and people can’t – and sometimes they want you to be invisible because you’re going to be infringing on their freedoms or how they do things, and they might have to do something differently
Participants reported their interactions with the public were dependent on how others responded to their aphasia symptoms. This social stigma often led to withdrawal and careful management of social interactions, as Participant 6 explained: This is a hard question because I can try to communicate and not try to communicate. Lack of public knowledge of aphasia hindered community reintegration. Participant 5 explained: One friend said, “You talk too much.” And I thought that’s because sometimes I don’t know what the word is and so I - so I describe it. . .I’m like, okay, be very careful not to do that. The Communication Partner for Participant 4 recounted Participant’s reluctance to speak in public scenarios: if we went somewhere together, he would be quiet. . . He wasn’t confident in talking. Participant 3 described how they would disengage from inaccessible conversation: Because, you know, people go fast, and it’s just like, alright, f*ck off. Just like – [sticks up middle fingers]. As I said, when that happens sometimes, I’ll just [Pretends to nod off and look at wrist to simulate looking at watch]
Reflecting on their family’s response, Participant 4 shared their father’s initial misunderstanding of their aphasia: My father was like. . .he changed his thinking of what I was doing – he thought I was lost. They explained that their father initially lacked knowledge about aphasia and mistakenly believed his child’s personality was diminished. However, with greater exposure to their post-stroke communication challenges, his understanding gradually improved. Some participants placed the onus on their aphasia diagnosis for excluding them from participating instead of viewing the experience of aphasia as a communication disability mediated by environmental factors. When asked what makes it difficult to participate in life events, Participant 6 responded: Because I can’t speak.
Participants felt stroke healthcare workers also often lacked aphasia awareness. The Communication Partner for Participant 4 described how the nurses lacked the skills to communicate their requests: Communication was difficult. He would be asked to do things, but he didn’t know what they were asking. They weren’t good at gestures – they’re like, “Touch your nose,” and nobody would show him. Participants observed a lack of understanding of aphasia and the communication needs of PWA across the stroke care continuum. The Communication Partner for Participant 4 further illustrated this by giving the following example: The physical therapist, she talked too fast. . . and he’s getting frustrated ‘cause he’s not understanding what she wants him to do.
The Communication Partner for Participant 6 emphasized the need for healthcare workers to understand the communication needs of PWA: They could learn that people with brain injuries might need a little time to process, to which Participant 6 agreed—they talk very fast. Participants experiencing more severe expressive impairment also noted how healthcare workers would solely talk to the communication partner by default. Participant 6 described this: No, it’s not talk to me. . . Do you. . . talk to me, yes. And she’s [points to communication partner] talked to me, yes. But healthcare talk to me, no. The communication partners felt that participants with aphasia were generally included in healthcare conversations; however, care partners also observed that while participants with aphasia were physically present during healthcare conversations, these interactions were not always truly accessible to allow for meaningful participation. The Communication Partner for Participant 4 gave an example of this inaccessible communication by stating If I’d go get lunch, the doctor would come talk to him. . . And that would frustrate him ‘cause he doesn’t know how to answer them. And he’s pretty much going “my wife’s not here.” Not able to say that. Participants also noted how healthcare workers did not recognize the importance of their communication partnerships. The Communication Partner for Participant 4 described healthcare worker’s lack of understanding on the importance of their communication partnerships: it’s like they didn’t understand. . . That he doesn’t know what they’re saying when they’re talking about his care. If there’s not anyone there to help him, and Participant 4 agreed—that’s true.
Suggestions for improving communicative access for all people with communication disorders so they could participate fully in their healthcare were shared. Participants highlighted the variability of aphasia symptom presentation and the need for individualized care. A sentiment from Participant 1 summarized the changes they would like to see in healthcare workers:
Think about each of the people as individuals. And, you don’t have to spend more time with any of us, but if you take the time to care, it will make their life that much better. . . Someone with aphasia, that little help or something, it means a lot. It’s not like they can go on to the next thing. . . this person is piecing back together in their life.
A major sentiment among participants was the crucial need to better educate healthcare worker on supporting communication for PWA. Communicative strategies suggested by participants to facilitate better communicative access included providing options (e.g., yes/no questions if necessary), slowing down speech rates without being condescending, simplifying messages, allowing time to process/respond, showing patience for the person trying to get the message out, providing more context during conversation, repeating questions, and writing short keywords.
Facilitators
Communication partnerships significantly impacted participation and, as a result, had a profound influence on the lives of PWA. Across most interviews (n = 5), participants described how communication partners facilitated healthcare conversations after their stroke. Participants trusted their communication partners, who were pivotal to their care transition and communicative success. Communication partners relayed and interpreted important healthcare information and facilitated the involvement of the PWA when communication with healthcare providers was inaccessible or communication breakdowns occurred. The communication partner for Participant 6 described how they ensured the participant with aphasia’s opinions were still considered: I turn to him – and ask him does he – do you want to try that? Do you think that’s a good choice? Participant 6, when asked if they would feel comfortable going to an appointment by themselves, emphasized the crucial role of their partner in healthcare appointments: No. Because she is my sidekick. Concerns arose regarding independent appointments, with participants expressing worry about understanding information without their partner. Communication partners also described a sense of anxiety and uncertainty with not attending medical appointments alongside the participants with aphasia and reflected on the negative outcomes which could occur from their absence. Field notes recorded from care partner support groups attended by the research revealing a fear of “what would happen if or when my health declines? Who is going to be their advocate if I’m not there.”
Partnerships with friends and family encouraged and supported participation in life events. Participants described how community partnerships impacted their care transition success and filled care gaps. Participant 5 described how a neighbor, a medical doctor, explained their brain imaging after their stroke event as Participant 5 was unable to get these answers from their care team:
He sat in the living room, and he told me what it meant and not to panic. It was going to be okay. And he said, ‘You’ve got some work ahead of you, but it’s going to be okay’.
Finding community through establishing new connections with others who have experienced aphasia was crucial to community reintegration and to prevent feelings of isolation. The Communication Partner for Participant 4 emphasized the importance of support groups:
He’s questioning how long’s this [aphasia recovery] gonna take. ‘Why am I this way?’ And we had nothing to compare it to. So, I looked up the support groups so that he could see other people with aphasia and talk to them. And it seemed to help to talk to other people who had a stroke.
Participant 1 found these new connections with others experiencing aphasia also allowed for resource sharing: You need to get with other people and see what they’ve done. And what’s working for them. Some participants also found purpose in advocating for PWA. Participant 2 stated: I wish that everybody would be an [aphasia] advocate period. I’m lucky that I can do it.
The Need for Protection
Within the theory of Human Scale Development framework, protection encompasses the individual’s need for physical and psychological security, freedom from harm and uncertainty, and a stable environment (Max-Neef, 1991). The concept of protection emphasizes the broader need for a secure and supportive healthcare environment, encompassing freedom from harm, uncertainty, and unforeseen complications. Barriers and facilitators of protection are presented below.
Barriers
Participants felt the healthcare system was too overburdened and busy to address their care needs. Across all interviews, participants described how resource scarcity and overburden in the healthcare system created barriers to healthcare access. Elaborating on the concept of resource scarcity, Participant 1 described access to inpatient rehabilitation as a privilege: And was like so good that I got in there because, you know, you gotta– you’re the lucky one that gets to go. Participants with aphasia described how limited resources made it feel like they were “pushed out” of the system to make room for other patients. Many participants further described how healthcare staff were “busy all the time” and how staff did not have time to communicate with them. Note should be made that the average stroke onset date for the participants coincided with the global pandemic. Half (n = 3) of the participants experienced a stroke event amid the coronavirus global pandemic and, thus, were exposed to the strained US healthcare system in response to the COVID-19 Public Health Emergency. Nonetheless, all participants noted resource scarcity and overburdened healthcare systems was common—regardless of stroke onset date. They also faced extended waitlists to access the specialty stroke care services they needed both in the outpatient and inpatient settings. The Communication Partner for Participant 4 elaborated on their frustration with the delay in seeing inpatient physical therapy: This is just the critical care unit. And they’re like, ‘Oh, you can’t get up until you see the physical therapist’. And it’s like, ‘Well, when am I going to see the physical therapist? We’ve been here since Monday. Today is Saturday. We haven’t seen any therapy’.
Participants commented on the extended waitlists to access specialty stroke care services through outpatient referrals, with waitlist times ranging from 6 months to >2 years. Some reported feeling dismissed by healthcare services—leaving the participants to deal with their unmet healthcare needs without guidance. For example, Participant 4 described how they had rehabilitative goals in the hospital but was told they had to wait until they were admitted to inpatient rehab, and this led them to worry about their future recovery progress, stating so not knowing that was – it was kind of – I didn’t like that. Because being able to wait – I would get home, and it – then it’s like, oh, now what? Participant 1 described how this uncertainty in healthcare access and unmet care needs left them feeling vulnerable and described this experience by stating And I was just like I don’t know why you guys are doing this. And I go, “Is there anything that I can do to stay?” And it was an emotional experience. Many described navigating the system without understanding the next step in stroke or aphasia recovery. Participant 1 summarized the disconnect as: But it was like, Your week’s up. Here you go.’ And then you have the rest of your life to live. Further, insurance limits on speech and other therapy services, post stroke, created barriers to meeting their rehabilitative goals. While resource limitations impact stroke recovery broadly, the effects of resource scarcity are significantly exacerbated for individuals with post-stroke aphasia. The participants highlight how these structural barriers to care hinder optimal health and well-being for PWA. The ability of PWA to navigate healthcare systems and access crucial information and resources is contingent upon the communicative accessibility of their healthcare providers and services, and/or their access to a supportive care partner. Participants also felt the healthcare education and care conversations provided to them were either inadequate or inaccessible. Many described how they felt ill-prepared to manage care for their newly acquired chronic conditions. For example, the Communication Partner for Participant 6 reported not being told of a serious post-stroke complication, seizures, before Participant 6 was discharged and explained, yeah. I had no idea what happened. And – and no, I had no idea that it could’ve happened. Similar findings emerged with two participants, who experienced strokes as complications from cardiac procedures, stating they did not feel well-informed about the risk of stroke due to the procedure. Others described how they sought external resources to provide guidance when healthcare services failed to prepare them for life after a stroke. The Communication Partner for Participant 4 described how they were only told the intervention for treating spasticity, without a rationale, by a healthcare worker: I had no idea about the shortening of muscles or nothing at this time. And one of the nurses. . .She said just spread it out. And then she said also lay it on a pillow. . . Nobody said if you don’t do it, it’s gonna stay that way.
Information received from healthcare teams was often inaccessible because medical jargon was used throughout conversations or in education materials. The Communication Partner for Participant 6 expanded on how inadequate education led the dyad to feel overwhelmed when they encountered other people with chronic aphasia in support groups: It was so scary because there were people that talked funny. And here we were just under the impression it was such a temporary [condition]. Persons with aphasia and their communicative partners relied on themselves to find educational resources to contextualize their experiences, seek out additional physical or speech therapy options (e.g., community programs, digital applications, online speech exercises, etc.), and even coordinate other medical procedures (i.e., left atrial appendage closure procedure). Each participant noted how not all PWA are able or willing to navigate the healthcare systems after a stroke for a range of factors (e.g., knowledge of the healthcare system, the severity of their post-stroke sequelae, availability of support person to help facilitate care coordination efforts, etc.). Participant 1 noted: what happens to the person going out and they injure their brain or have a stroke? I mean, they don’t know who to talk to. Thus, inconsistent resources and support, unpredictable care transitions, and inadequate information regarding potential risks or complications contributed to feelings of uncertainty and vulnerability among the participants. Thus, the participants’ need for “protection” was not always met by the healthcare system.
Facilitators
As demonstrated by the described barriers, the healthcare system for post-stroke management is complex and scattered across multiple settings or systems. Some commented that access to more therapy—after reaching insurance limits on care—were siloed in community programs outside of the healthcare system. Care gaps were circumvented by finding community programs to gain access to necessary care. Thus, it was incumbent on the person with aphasia and their care partner to learn this complex system of long-term care for stroke management in the absence of healthcare service support. Many described how these coordination efforts require significant amounts of personal “drive,” “motivation,” and “tenacity.” Participant 5 summarized why self-determination was crucial in navigating the healthcare system: some of these are not tenacious like me to know that you don’t take no. You just keep going until you get yes. Participant 1 described the complexity of the system for stroke transitional care as: You have to have that drive, even that [non-profit organization] –I kept calling them and I kept emailing them. And I just kept doing it, and that’s what got me in. . . It was like that’s the type of determination that gets you places.
Self-advocacy, and advocacy via the communicative partner, were described as an important facilitator to address gaps in healthcare workers’ understanding of aphasia. Participant 5 gave the following advice to other PWA:
It would be a good idea to be your own advocate and say, ‘I need your patience while I tell you what I need. And I need you to listen carefully because what I’m telling you is a lot of work’.
Participant 3 also described how they advocated for themselves during healthcare conversations. stating, what I do is when I go to—there [healthcare interactions]—I slow down. Basically, okay, slow down, so that way, I can slow down so you can—and speak. Slow down is much better. Recognition of their inherent value consistently emerged across all interviews. Participant 2 commented on how PWA should be recognized for having intellect—regardless of their communicative abilities: You know, people are very positive—and very, we’re good, and we have intellect. Participants identified this innate ability to believe in themselves as a facilitator for care transition and communicative access success. Thus, the ability to be self-reliant and self-advocate met their needs for protection.
The Need for Understanding
Within the theory of Human Scale Development framework, “Understanding” encompasses the individual’s capacity for comprehending their environment, acquiring knowledge, and making sense of social and cultural contexts (Max-Neef, 1991). The concept of understanding was conceptualized as being satisfied by healthcare workers having supportive communication policies, which facilitated improved knowledge and self-esteem for the individual. The interconnectedness of the nine ontological needs within the Human Scale Development framework stems from their inherent interdependence and the holistic nature of human existence. While recognizing potential overlap among the concepts in this framework, the concept of understanding primarily addresses participants’ capacity to comprehend their health, navigate healthcare, and make informed decisions. Barriers and facilitators to this operationalization of understanding are presented below.
Barriers
Healthcare conversations were reported as being primarily focused on organizational or institutional interactions (e.g., physical assessments, prescribing medications/treatments, etc.). Participant 5 described how regimented healthcare interactions are by stating, what makes it difficult is I think many health people have an agenda. That they already know what they’re going to do, and they haven’t gotten to know me. The Communication Partner for Participant 4 also noted this one-directional and transactional conversation by describing all of their assessments, they would be the same. And got to where he’d hold his arms up before they’d even ask. . . He knows what they’re going to come ask. When asked how healthcare workers communicate with them, Participant 3 described the limited nature of these healthcare conversations: Take this. Let me know. Participant 1 commented on the impact of transactional healthcare conversations: Because when it’s transactional and stuff – it’s ultimately –your care doesn’t – it suffers. Some participants also focused on larger systemic/institutional structures that act as barriers for healthcare workers and, consequentially, the care the participants received. Participant 5 expressed how they sympathized with the clinicians operating within these strict insurance structures stating, I think with some of the insurance structures, you do only have fifteen minutes, and they have to run you through. Participant 1 described how insurance requirements interfered with the quality of healthcare received:
The speech therapist at [medical facility reference] was like, ‘We need to come up with our next goals. . .’ And I was like I don’t even– like you hear me. I have all these problems. Write down our next sequence and let’s get on. But for them, they were making this list. . . that my physician would see, and the insurance would see. But oftentimes, that would get in the way of treating me.
The Communication Partner for Participant 6 also identified how interactions with healthcare providers who lacked compassion served as a barrier: I also know that many times they [healthcare workers] have not been as compassionate as I think they could be. I think it would make a person like my husband feel much more comfortable if they would check out of being so professional and check in to being human.
These experiences with one-sided healthcare and the need for individualized care exemplify how systemic barriers impede PWA’s ability to comprehend their healthcare, navigate the system, and participate in care decisions, which hinders their need for “understanding” from being met.
Facilitators
Participants emphasized that healthcare workers who fostered understanding through supportive communication, which in turn improved their knowledge and self-esteem, empowered them to actively engage in healthcare decisions. These patient-centered interactions, characterized by genuine care and a focus on human connection, motivated participants to be involved in their healthcare outcomes, significantly facilitated successful care transitions, and improved communicative access. Successful interactions with compassionate healthcare workers strengthened them during uncertain times in their stroke recovery, enhanced their comprehension of care plans, and empowered them to navigate the healthcare system effectively. For example, Participant 5 described how their primary care showed compassion in their prompt response to a repeat brain imaging and how this provided immense relief: [Primary Care] already read it [MRI]. . . It was two hours later – “You did not have a stroke. There’s other things we’re gonna keep watching. How is everything going?” And I cried. The need for healthcare workers to be compassionate and empathetic was further echoed by Participant 6 and their Communication Partner. Participant 6 had a stroke event as a complication of aneurysm repair surgery, and the dyad spoke fondly of the cardiothoracic surgeon who performed the procedure. The Communication Partner for Participant 6 discussed the profound impact of cardiothoracic surgeon’s compassion: We had the emergency surgery [aneurysm repair] – after that, [cardiothoracic surgeon] came out. He held my hand and told me thank you for bringing him. . . ‘He’s going to be okay now’. . . When we were [later] in the hospital, after the stroke, this same doctor came to visit him and we said, ‘Oh, you’re the doctor that saved our life’.
Discussion
This qualitative inquiry described, from the perspectives of PWA, the most critical facilitators and barriers to transitional care and communicative success. This study identified how successful navigation of stroke care transitions is a complex and multifaceted process for PWA. Communication serves as a synergistic satisfier (i.e., a concept that satisfies multiple ontological needs; Max-Neef, 1991) with the theory of Human Scale Development, and findings demonstrate how a lack of accessible communication has profound impacts on the quality of life with respect to needs for participation, understanding, and protection. Thus, results expand on the utility of Human Scale Development (Max-Neef, 1991) in illustrating how the healthcare system interventions either satisfy or inhibit the fundamental human needs of PWA.
Barriers to resources, care access, and reintegration into community spaces were identified by PWA. To our knowledge, this is the first study documenting concerns of PWA regarding public perception affecting their interactions in community environments. This study further contextualizes findings from the National Aphasia Association’s (2022) aphasia awareness survey where an increased 40% of respondents were “aphasia aware” compared to the 7% of respondents in 2020. Despite surveys demonstrating increasing levels of public awareness, the findings indicate more work is needed both in the public and healthcare spheres. Results also extend recent research documenting how healthcare staff often lack the skills to communicate with and fully address the care needs of PWA (Baker et al., 2020; Carragher et al., 2024; Manning et al., 2022). Further, these results expand on a wealth of research documenting the asymmetrical nature of healthcare conversations for PWA (Baker et al., 2020; Carragher et al., 2021; Gordon et al., 2009; Loft et al., 2022; van Rijssen et al., 2022) and how organizational barriers (e.g., insurance limitations) can hinder care for people with complex medical needs (Gordon et al., 2018; Sommers et al., 2011). Participants also noted that current models of healthcare delivery/services in the United States are insufficiently resourced to support patient-centered care efforts, which aligns with findings by Carragher et al. (2021). Our findings resonate with current nursing literature on health inequities and disparities in access to quality healthcare experienced by people with disabilities globally (Bourne et al., 2021; Tosetti et al., 2023; Wolbring & Deloria, 2024).
Participants reported feeling unprepared and uninformed about post-stroke rehabilitation processes and this finding is consistent with previous studies (Anderson & Marlett, 2004; Eames et al., 2010; Hersh & Armstrong, 2021; Rose et al., 2019). Moreover, participants call to action the need for healthcare workers to be better educated on accessible communicative strategies and how to integrate techniques into clinical practice. These findings emphasize the importance of patient-centered communication and the need for nurses to continue to advocate for patient-centered approaches in all healthcare interactions with PWA. By actively listening, using inclusive communication strategies (e.g., SCA™), and empowering individuals with aphasia to participate fully in their care, nurses can significantly improve the quality of care provided and enhance the overall healthcare experience for this vulnerable population. These findings underscore the need for ongoing education and training for nurses on accessible communication strategies and the unique challenges faced by PWA. Continuing education efforts should be funded and supported by healthcare systems to best equip nurses and other healthcare workers on accessible communication and aphasia. Cross-disciplinary training programs on accessible communication strategies, developed in collaboration with speech-language pathologists, should be integrated into all levels of nursing education globally. This training should be accessible to practicing nurses through continuing education courses and disseminated to the broader healthcare community via presentations at international stroke conferences to foster interprofessional collaboration.
Accessible communication strategies are crucial for individuals with diverse communication needs. Increasing the accessibility of healthcare environments—including adequately equipping nurses and other healthcare workers to converse with individuals experiencing communication impairments—would significantly benefit a substantial portion of the population. Thus, there is much work to do—focusing on multiple avenues of improving healthcare delivery models in the US—to support and educate healthcare workers on supportive communication and, in turn, provide the groundwork to provide accessible care to people with communication disabilities.
Facilitators to care transition and communicative access success were identified. These findings, compounded with research describing the disconnects and dismissal of unmet education needs for PWA and their care partners (Hersh & Armstrong, 2021; Shafer et al., 2019), highlight the critical need for accessible, effective, and comprehensive health education for PWA and their families. The voices of participants in this study add to the collective evidence describing the significant impact of empathetic, patient-centered, and compassionate interactions from healthcare workers on outcomes (Barker et al., 2023; Durkin et al., 2022; Nätterlund, 2010; Rose et al., 2019; Sinclair et al., 2016; Smith-MacDonald et al., 2019). Participants found necessity in the function of the care partners to act as proxies for healthcare decisions, particularly when aphasia symptoms were severe, which aligns with findings by Hilari et al. (2007). Communication partners also noted how assuming responsibility for the roles of advocate, educator, and coordinator—in the absence of healthcare providing these services—creates anxiety and uncertainty for the outcome of the participant with aphasia, especially if/when the care partner could no longer serve in those roles.
Limitations
The process of collecting and analyzing data for this study was carefully structured to limit bias in the results (Miles et al., 2020); however, the limitations of the study may have influenced the findings. First, voluntary, purposive sampling was used to recruit individuals, and there may have been selection bias trending toward the healthier and more highly motivated individuals who agreed to participate in this study. Most participants who agreed to participate in the study were connected to support groups or therapy services through the Aphasia Lab. Additionally, the study lacked funding for transportation to the in-person interviews. We offered interviews to be conducted over Zoom, but it is possible we could have widened the participant pool by interviewing people in their homes. Second, specific note should be made on the demographics of the sample. The sample was comprised of primarily cisgender males who all identified as non-Hispanic white, were highly educated, and all reported speaking English as their first language. Important additional insights may be found in participants who are not represented in this sample. Thus, more research is needed on the experience of participants with aphasia from marginalized and underrepresented groups. Third, this study relied on participants recounting their experiences with healthcare workers’ behaviors and communicative strategies. The study design did not explore the influence of healthcare worker behavior on engagement with healthcare services. Lastly, the researcher’s presence is acknowledged to affect results in qualitative research (i.e., observer bias). The researcher’s career in neuroscience nursing and personal experience as a primary caregiver to a person experiencing aphasia increased the likelihood of observer bias.
Conclusion
In conclusion, the findings of this study highlight the many care gaps in healthcare delivery for PWA. Findings demonstrate how the resilience of PWA and their care partners serve as the main facilitator in care transition success for individuals experiencing this life-changing event. More research, resources, and clinical care are needed to address the care gaps these vulnerable patients face. Action is required to educate the workforce of healthcare workers and the public on how to be more accommodating to people with communication disorders. Individuals should not be deprived of their right to safe and autonomous care due to a lack of communicative access or resources. Improvements in care transitions and communicative access have the potential to promote empowerment for PWA and improve communication across the continuum of care.
Footnotes
Acknowledgements
The author would like to thank Dr. Cynthia Corbett for her advisement on initial study design, Ms. Stacey Steele for her help with participant recruitment, and Ms. Chelsea C. Thomas for her assistance with preliminary data analysis.
Author Note
Dr. Celestina Barbosa-Leiker is now at California State University, Fullerton, Fullerton, CA as the Dean of the College of Health and Human Sciences. Lonnie A. Nelson is now a Professor in the Cancer Prevention Program of the Public Health Sciences Division and a Faculty Lead of the Indigenous Cancer Health Equity Initiative at Fred Hutch Cancer Center in Seattle, WA.
ORCID iDs
Ethical Considerations
This study was reviewed and approved by the Institutional Review Board at Portland State University (227809-18) on August 01, 2022.
Consent to Participate
Informed consent was verbally obtained from each participant and communicative partner prior to data collection and outlined the study’s purpose, procedures, risks, and benefits, and emphasized the participants’ rights to withdraw from the study at any time.
Author Contributions
All authors have contributed to the manuscript based on ICMJE criteria. Author ABT conducted the study and substantially contributed to drafting the manuscript. Authors CRVS, GF, LAN, and CBL substantially contributed to the conception, design, and interpretation of the data and work. The authors have read the manuscript and approve the submission to Disability and Research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sigma Nursing Honor Society, Delta Chi-at-Large Chapter, the Carl M. Hansen Foundation, and the Washington State University Libraries.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The deidentified data generated and/or analyzed during the current study are not publicly available to safeguard participant confidentiality, but metadata (e.g., codebooks, data displays, interview materials) are available from the corresponding author on reasonable request.