
Abstract
In dementia care, the concept of dignity has garnered substantial attention from both researchers and policymakers. However, the concept often remains vague and open to interpretation, potentially leading to misunderstandings and suboptimal care for people with dementia. As healthcare professionals occupy a critical role in upholding dignity, exploring their viewpoints on this complex concept is paramount. In this study, we explore Danish healthcare professionals’ views on the dignity of people with dementia and discuss these perspectives against existing theoretical accounts. We employed thematic analysis of data collected during facilitated discussions with a total of 99 healthcare professionals, including nurses and healthcare workers, during which we posed the question, “What is dignity to you?” and documented their perspectives. Through a systematic process of data coding and interpretation, we identified recurring patterns in their responses. This approach allowed us to uncover the depth and complexity of their viewpoints, providing valuable insights into the multifaceted nature of dignity as perceived by healthcare professionals. Our findings revealed that healthcare professionals possessed a nuanced understanding of dignity, recognizing both a subjective element and a universal aspect applicable to all individuals, aligning with theoretical interpretations. However, conceptual ambiguity remained a challenge.
Introduction
As the global population continues to age, projections from the UN's World Population Prospects indicate that by 2050, the proportion of people aged 65 or older worldwide is expected to increase to 1 in 6 (16%), marking a significant rise from 1 in 10 (10%) in 2022 (United Nations, 2022). While dementia is not a natural part of all aging, aging is the greatest risk factor for many neurodegenerative disorders, including dementia (Wahl et al., 2019). This means that the prevalence of dementia too is on the rise. According to recent estimates from both the World Health Organization and a publication in Lancet Public Health regarding the global prevalence of dementia, there are currently an estimated 55 to 57.4 million people living with dementia worldwide. This number is projected to nearly triple by the year 2050 (Nichols et al., 2022; WHO, 2023). As dementia reduces the cognitive functions of people with dementia, it affects their ability to perform day to day activities (Shuman et al., 2017). This decline in cognitive functioning and the accompanied vulnerability and need of care that people with dementia experience means that many eventually move into an assisted living residence or a nursing home. It is estimated that approximately two thirds of all people who die of a dementia illness, do so in a nursing facility (Alzheimer’s Association, 2023).
As the number of people with dementia rises and their vulnerability becomes more apparent, the necessity of providing high-quality care that enhances their quality of life while preserving their dignity becomes increasingly imperative. In fact, in recent years, substantial emphasis has been placed on the notion of dignity in dementia care, which has recurrently been championed as a fundamental right and imperative of care (Jacelon et al., 2004; Zirak et al., 2017). Dignity has become a key principle of care, and professional caregivers are often said to have an obligation to safeguard the inherent dignity of patients or residents (American Nurses Association, 2015; International Council of Nurses, 2021; United Nations, 1948). Furthermore, dignity is not only part of the imperative of care but is also sometimes enshrined in the law. For instance, in Denmark, a decree on dignity policies for elderly care was passed in 2019, requiring every municipal board in Denmark to adopt dignity policies for municipal elderly care. The aim of the law was to establish overall benchmarks and principles for dignified elderly care and hence to ensure the promotion of the dignity of the elderly (The Ministry of the Interior and Health, 2019).
In addition, dignity has become a prominent field in research on the care of elderly people in general (Clancy et al., 2020; Jacelon, 2003; Lothian & Philp, 2001) and of those in residential care and nursing in particular (Baillie et al., 2009; Calnan et al., 2005; Dwyer et al., 2009; Franklin et al., 2006; Hall et al., 2009, 2014; Oosterveld-Vlug et al., 2013, 2014). Against this backdrop of studies on dignity in nursing care and gerontology, scholars have argued that dignity could be promoted in dementia care through various measures and interventions (Johnston et al., 2016; Manthorpe et al., 2010; Tranvåg et al., 2013) as well as by understanding the various attributes that constitute the dignity of persons living with dementia by including the perspectives of individuals living with dementia, family members and professional caregivers (Clancy et al., 2020; Šaňáková & Čáp, 2019; Tranvåg et al., 2014, 2019).
Dignity as a Vague Concept and the Problem of Conceptual Inconsistency
Confusion remains regarding the practice of dignified care, as noted in a 2019 concept synthesis of dignity in Nursing Ethics (Hasegawa & Ota, 2019). In fact, despite an overt emphasis on dignity both in practice and research, the concept often remains open to interpretation. Back in 2003, Macklin (2003) insolently declared that “appeals to dignity are either vague restatements of other, more precise, notions or mere slogans”. If this is true, dignity might reflect different phenomena or attributes that are potentially nonconvergent, such as respect for individuals’ preferences and desires, values and lifestyle, autonomy and empowerment, and simply feeling comfortable with oneself (Granero-Molina et al., 2016). If dignity is just vague restatements of other phenomena, then it raises the question, what are healthcare professionals actually promoting, when they are asked to promote dignity? If efforts to promote dignity are centered around particular phenomena, then ensuring practical promotion relies on having a shared understanding and agreement about the concept in question.
Ensuring a shared conceptual agreement and definition of dignity is crucial to avoid misunderstandings and potentially undignified care for individuals with dementia, as conceptual inconsistency may lead to violations of dignity for people with dementia (Jacobson, 2009; van der Geugten & Goossensen, 2020). Consequently, it is key to study healthcare professionals’ perspectives on dignity, in order to establish whether their understanding of dignity on the one hand represents a consistent phenomenon and on the other hand actually correspond to theoretical accounts of dignity.
Aim
The aim of this study is to explore healthcare professionals' perspectives on the concept of dignity in dementia care. This study is conducted as part of the larger research project DEMENTIA ID, which explores healthcare professionals’ perspectives on ethical dementia care, with the overarching goal of enhancing their confidence as ethical decision-makers through engaging them in ethical dialogues. This study specifically focuses on healthcare professionals' perspectives of dignity in dementia care. Through analysis of facilitated discussions, we aim to identify the main themes that emerge from their views and compare them to theoretical accounts of dignity. By combining empirical analysis with theoretical exploration, we aim to deepen our understanding of the complex phenomenon of dignity in dementia care.
Methods
This qualitative study examines the perspectives of healthcare professionals on dignity in dementia care within a Danish municipal setting. Epistemologically, we employed a qualitative descriptive approach, using template analysis, to uncover and understand the phenomenon of dignity from the perspectives of healthcare professionals (Bradshaw et al., 2017). The findings were subsequently discussed against the backdrop of theoretical accounts of dignity to assess convergence and conceptual consistency.
Intervention, Setting, and Participants
This study was conducted as part of the CARE intervention, which was developed and tested in a collaborative intervention research project supported by Velux Foundation. The project was carried out between the National Institute of Public Health at the University of Southern Denmark (SDU), Rudersdal Municipality, and the Danish Alzheimer Association. The CARE intervention was designed for professional caregivers and aimed at promoting knowledge of and dialogue about ethical decision-making to improve their ethical self-efficacy. The intervention was piloted at three different care facilities in Rudersdal Municipality over 1 year, from December 2021 through November 2022, involving a total of 99 healthcare professionals as participants (see Table 1). Participants were identified and recruited using convenience sampling (Stratton, 2021) by Rudersdal Municipality.
Participants’ Sociodemographic Characteristics.

This category is comprised of the titles of Social- og sundhedshjælper (Social and health care helper) and social- og sundhedsassistent (Social and health care assistant).
This category is comprised of people with no formal education pertinent to dementia care.
The intervention consisted of two workshops held a week apart, totalling seven sessions. This included three sets of two workshops each, along with an initial pilot workshop, with approximately 25 participants in each workshop. During the intervention, themes such as autonomy, privacy, best interest, informed consent, and dignity were extensively discussed. The discussions of each concept were complemented by a bioethics lecture on the pertinent notion, with one lecture provided for each concept delivered to the participants. Prior to the lecture on the notion of dignity, the facilitated discussion was held to ensure that participants' preconceptions of dignity were not influenced. The discussion both contained an unprompted exercise, in which participants, in groups of 5 to 10, were asked to discuss what the notion of dignity meant for them, as well as a facilitated plenary discussion of dignity, thus generating insights into healthcare professionals’ perspectives on the notion of dignity.
Data Collection
The primary data comprised healthcare professionals’ perspectives on the dignified care of people with dementia, collected through two methods during the intervention. First, observational notes were taken using a standardized protocol during facilitated plenary discussions, which explored participants’ views on dignity. Second, we handed out a reflection sheet with the text “Dignity to me is . . .” to the participants and invited them to brainstorm and discuss their perspectives on dignity with their peers and write them down. These reflection sheets was collected to allow for text analysis. In total, 99 healthcare professionals participated, providing testimonies that ranged from brief statements to lengthy explanations. Data were collected between December 2021 and November 2022. Both the testimonies collected and statements that emerged during the plenary discussions were transcribed by the second author. All written statements are presented verbatim in the translated form.
Data Analysis
To identify the participants’ perspectives on dignity, we conducted a thematic analysis of all testimonies recorded using the reflection sheets as well as of the observational notes taken during the intervention. Thematic analysis was chosen due to its suitability for exploring and interpreting the perspectives of healthcare professionals on dignity in dementia care. This approach allows for the systematic identification of recurring themes within the data, facilitating a comprehensive understanding of the complexities surrounding the concept of dignity. The data were coded using QSR NVivo software (QSR International Pty Ltd, 2020) and analysed using thematic analysis to classify the relevant overarching themes (Braun & Clarke, 2021). Following the framework proposed by Braun and Clarke, all data were initially fully read by the first [FS-J] and second author [RK] of the study. Preliminary coding of all data was then conducted individually by multiple coders [FS-J, RK, SL], to ensure comprehensive coverage and subsequently compared, to enhance the reliability of the coding process. The codes, corresponding to perspectives on the notion of dignity, were developed directly from the data. Based on these codes, themes were constructed from clusters of thematically corresponding codes. Subsequently, the codes were sorted into potential overarching candidate themes. All potential themes were reviewed and refined to establish whether a given theme exhibited a coherent thematic pattern. Finally, we identified the essence of the themes, and a narrative for each theme was established. Throughout the analysis of the data, we continually engaged in peer debriefing among the authors to enhance the validity and reliability of the analysis (Braun & Clarke, 2021).
While we employed a rigorous qualitative methodology to identify themes in our data, it's important to acknowledge the potential influence of our positionality on the findings of this study. As researchers engaged in the exploration of public health ethics and dementia care, our positionality is shaped by our academic training. Our backgrounds encompass diverse disciplines, including public health, bioethics, and sociology, which have collectively informed our understanding of the complex notion of dignity in dementia care. While these backgrounds have equipped us with the theoretical frameworks and analytical skills necessary for examining healthcare professionals’ perceptions on dignity, we recognize the potential for the introduction of biases in our analysis as a limitation. For instance, preconceived theoretical notions regarding the relative and universal aspects of dignity may have impacted the true openness of our approach.
Ethical Considerations
The study was approved by the Research Ethics Committee (REC) of the University of Southern Denmark (SDU) (Case No. 20/61405) and by RIO Legal Services (No. 11.154). It was conducted in compliance with the General Data Protection Regulation (EU) 2016/679 and the principles of the Declaration of Helsinki. All participating healthcare professionals in Rudersdal Municipality were informed that participation was voluntary, and that data would be handled confidentially and that we would make appropriate efforts in anonymising data. While it is difficult to achieve full anonymity, identifying details of the healthcare professionals were omitted, as they were
Results
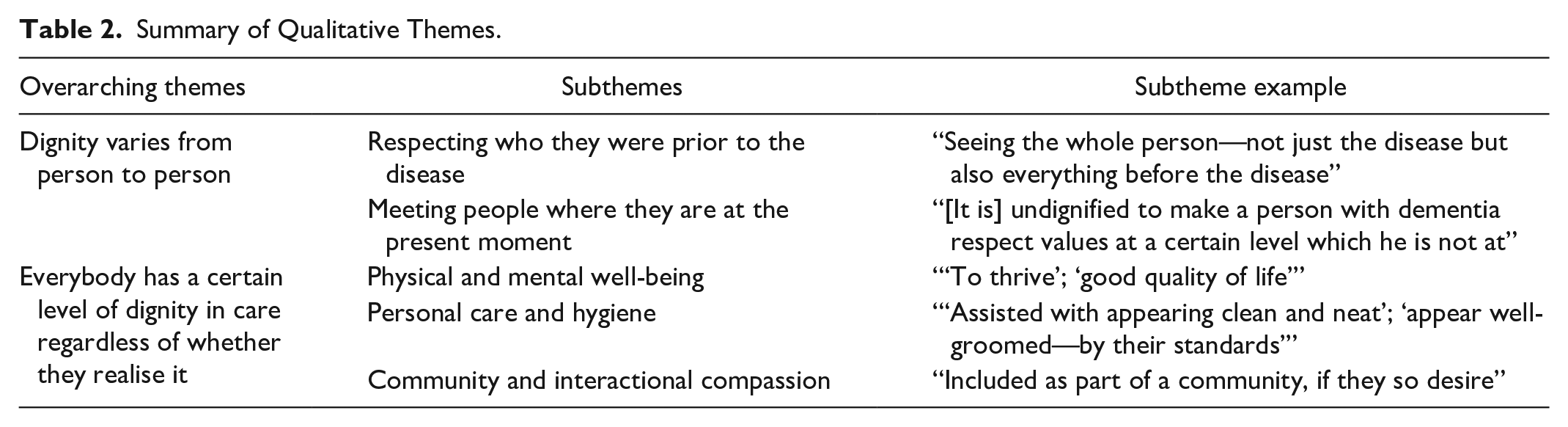
Healthcare professionals’ perspectives on the notion of dignity were composite and multifaceted. In fact, their perspectives on dignity and what constitutes the dignified care of people with dementia differed in terms of various attributes. Nonetheless, we identified two overarching themes, with respective subthemes, which were pervasive in the healthcare professionals’ perspectives (see Table 2).
Summary of Qualitative Themes.
Dignity Varies From Person to Person
One theme that was prevalent among healthcare professionals’ perceptions of dignity was related to the idea that dignity is highly dependent on individuals and varies from person to person. Numerous healthcare professionals supported the idea of person-centred and individualistic account of dignity. Take, for instance, the case of one healthcare professional who recorded that “dignity is individual” and “[you have to] depart from the individual person; see the individual.”
Others pointed to the fact that dignity had to do with the specific needs of people with dementia and that an “awareness of needs” was quintessential in ensuring that people with dementia received dignified care. An important element of providing dignified care was said to involve “addressing the needs of the individual,” and healthcare professionals had to “regard everybody as individuals” and assess “what their values are.” A general point in many of the healthcare professionals’ perspectives on dignity was that “dignity varies” and that one should “recognise [this] diversity.”
Therefore, a widespread predisposition was the idea that the notion of dignity is highly individual and should correspond with what an individual finds to be dignified. In other words, what is dignified for one person may not be so for another. This dimension in the healthcare professionals’ views on dignity pertained, as a healthcare professional noted during the discussion, to the importance of “retaining one’s personality without that personality being exceeded.” However, the concept of dignity being relative and varying from person to person, lacked clear agreement regarding the specific temporal personal characteristics on which it relied. There was disagreement over whether this relative dignity should be founded on the pre-disease identity of people with dementia or their current state of being.
Respecting the Person Prior to the Disease
Respect for people with dementia as they were prior to the onset of the disease was a predominant idea among the healthcare professionals’ perspectives on the notion of dignity. Various statements clearly illustrated that attaching importance to the “life story” and previously held values and standards constituted an important element of this understanding of dignity. As one respondent noted when asked about what dignity means, “[It means to] appreciate what the person used to be like – for example, if they cared a lot about being well groomed.” Similar views were expressed by other respondents, who explained that dignity is about adopting a more holistic view and “seeing” the whole person behind dementia. This position was vividly expressed by a healthcare professional who noted that dignity is about “seeing the whole person—not just the disease but also everything before the disease.”
This holistic view regarding the individuality of the dignity of people with dementia meant that previously determined or expressed values should be respected, including various preferences in terms of music, lifestyle and religion. For instance, one healthcare professional noted during the facilitated discussions that if a person with dementia and his family has always cared about their appearance in the eyes of their family, then helping them accomplish this is part of maintaining their dignity when the family comes over. The healthcare professional also noted that had the previous self of the person with dementia been able to decide, they would have cared about their appearance, even if they had known that they might not have cared about it at a later point.
Meeting People Where They Are at the Present Moment
Although a clear dimension of dignity involved maintaining the previously held values and individuality of people with dementia, as another healthcare professional noted in the discussions, “there is a lot of talk about the extent to which one should hold on to the person’s former identity.” In sharp contrast to adopting the notion of respect for the personality of the person prior to the onset of the disease, other healthcare professionals argued that the notion of dignity involves respect for the transformative nature of the disease and thus entails respecting who the person with dementia has become. Numerous healthcare professionals stated that an important dimension of dignity involves acknowledging the present identity of the person. For instance, one healthcare professional highlighted the importance of the fact “that we meet the person with dementia where they are; that we meet them where they are NOW.” Others agreed, asserting that it is “undignified to make a person with dementia respect values at a certain level which he is not at.” Many healthcare professionals championed respect for present values, preferences and needs, calling for the acceptance of the present situations of people with dementia and for the persons whom they have become. Similarly, others noted that dignity is the act of respecting “where they are, in the context they are in—their wants and needs.” In this vein, the notion of self-determination was considered important. Various of the written perspectives on the notion of dignity stated that “self-determination,” “independence,” and “liberty” were important characteristics in maintaining the dignity of people with dementia. As one healthcare professional wrote, it is important to at least “maintain a sense of control.” The notion of self-determination was regarded as a constituent part of dignity, as several perspectives on the notion of dignity emphasized the importance of “self-determination,” “independence,” and “liberty” in maintaining the dignity of people with dementia. For instance, one healthcare professional emphasized the significance of “maintaining a sense of control.”
Everybody Has a Certain Level of Basic Dignity in Care Regardless of Whether They Realise It
While participants to a large degree acknowledged that everyone possesses a certain level of dignity in care, irrespective of their awareness, participants also highlighted that assessments of what is in fact dignified in dementia care are context dependent. The individual concept of dignity may clash with alternative perceptions of what constitutes dignity for people with dementia. Consequently, dignity becomes a negotiation process involving the perspectives of individuals with dementia and other stakeholders. For instance, one noted during the discussions, while some individuals with dementia may tolerate certain conditions, like living in unclean environments, others may advocate against such conditions, asserting that they are undignified regardless of the individuals’ awareness. A similar interpretation of the negotiation between the various perspectives on dignity, was highlighted by another healthcare professional during the discussions, who stated the following: “It is the assessment of the individual what they think is dignifying. The staff then assess exactly what they think is dignifying for the individual person with dementia along the way.”
The notion that certain aspects contribute to the dignity of people with dementia, irrespective of their awareness, was a prevalent perspective among healthcare professionals in both the discussions and written testimonies, contributing to a key theme. This perspective was articulated in various ways by participants.
Physical and Mental Well-Being
For instance, in the discussions and written testimonies, the healthcare professionals suggested that dignity for people with dementia contains an element of thriving or flourishing in everyday life. For instance, one healthcare professional argued that dignity for a person with dementia could be defined by feelings of ease and contentment. Others noted that “to thrive” or have a “good quality of life” was an important element of dignified care for people with dementia. This position was emphasised by another healthcare professional, who claimed that dignity meant that care was provided in ways that supported “well-being both physically, mentally and socially.” Moreover, the notion of being kept safe, without pain and without suffering, both in everyday life and in end-of-life situations, was highlighted as an important element of this universal dimension of dignity that belongs to every person with dementia regardless of whether they realise it.
Personal Care and Hygiene
Although the notions of “thriving” and “well-being” for people with dementia were not further specified in the healthcare professionals’ perspectives on the notion of dignity, many of them agreed upon a particular component of the shared dimension of dignity—namely, assistance with personal care and hygiene. This point was underlined by two respondents, who wrote that dignity implies that people with dementia are “assisted in appearing clean and neat” and that they should “appear well groomed—by their standards.” Others noted, using more specific imperatives, that dignity implies that people with dementia are “assisted in maintaining personal hygiene and that their home is tidied up” or that they are assisted in keeping their hair and nails nice and clean and that they have clean clothes and well-kept feet.
Community and Interactional Compassion
Another important theme in the healthcare professionals’ perspectives on the notion of dignity referred to an interactional, or social, element, that involved both meeting and respecting the needs of people with dementia in relation to participating in social engagement, as well as respect in encountering or interacting with people with dementia. Many healthcare professionals championed the view that community participation and engagement with other people are fundamental aspects of dignity. This view was expressed in various forms—for example, by asserting that dignity entails that people with dementia are helped to “get out and kept part of society, where they’ve always been” or, as noted in a similar vein but with respect to the idea of meeting people where they are in the present, that they are “included as part of a community, if they so desire.” Other respondents accentuated the importance of ensuring that people with dementia maintain profound and important relations to other people—in other words, that they remain “something for somebody else.” In this context, the healthcare professionals also pointed to the idea of respecting sexuality and the capacity for love as central elements of the dignity of people with dementia. One participant highlighted the social aspect of the dignity for people with dementia, arguing that dignity entails “the absence of loneliness and isolation and the presence of community.” Close to this view was the notion of dignified death, whereby a dying person should never be alone. One of the most prevalent themes in healthcare professionals’ views on the notion of what constitutes dignified care and dignity for people with dementia had to do with maintaining compassionate and interactional respect when engaging with people with dementia. As one healthcare professional said, one of the most important elements of dignity is that people with dementia are “met by others with empathy.” Several others noted that compassion and empathy are quintessential in ensuring dignity and that “patience and empathy” are imperative to the notion of dignity in dementia care. In this context, one participant stated that “the lack of room for being accepted is undignified.” Similarly, others pointed to the idea of being accepted as a dimension of the notion of dignity. For instance, one healthcare professional stipulated that dignity entails “recognising them [people with dementia] as people” and that people with dementia should be “heard and seen” and “listened to.” As observed in one of the dialogues between healthcare professionals, what constitutes dignity in dementia care is that “they [people with dementia] should all feel that they are worthy of love and that we [the healthcare professionals] are genuinely engaged in their care.”
Discussion
In this study, we found that healthcare professionals hold different ideas about what dignity entails and which dimensions or domains it encompasses, indicating a diversity of perspectives. While some participants emphasized that dignity varies from person to person and that people with dementia should be met where they are in their disease trajectory, others argued that everyone has a certain level of basic dignity that should be respected, regardless of their awareness. For instance, it was asserted that nurturing the social care of people with dementia and preventing their loneliness plays a role in upholding such basic dignity. Such variation in perspectives on dignity points to a potential lack of consensus regarding its definition and raises the question of whether dignity is a complex concept encompassing multiple domains or alternatively, as asserted by Macklin (2003) and others, that dignity might sometimes serve as a restatement of other, potentially more precise concepts.
Despite these differing viewpoints, many healthcare professionals stated that dignity includes a subjective, or personal, dimension. This aligns with other studies that specify that at least a certain part of what we call dignity varies from person to person and depends on that person’s values. For instance, Dwyer et al. (2009) documented that nurses highlighted the importance of promoting a person’s identity by individualizing care, arguing that an important part of dignity lies in respecting each individual’s identity. Other studies similarly highlight the importance of individuality for respecting dignity, arguing that dignity is interwoven with respecting the character of the person with dementia (Hall et al., 2014; Oosterveld-Vlug et al., 2013). The perspective that dignity is relative to the person to whom it applies, is also reflected in other interpretations, suggesting that personal dignity is subjective and varies between individuals and over time (Jacobson, 2007; Leget, 2013; Nordenfelt, 2004). Similarly, these findings that dignity is relative to the person, correspond to other studies that emphasizes the importance of person-centered care and respecting individuality (McIntyre, 2003; Palmer, 2013). Such subjective or person-centered dignity not only differs from person to person but also changes throughout life (Nordenfelt, 2004).
However, while such subjective elements of dignity were acknowledged, many healthcare professionals also championed a more universal application of the notion. Even though people with advanced dementia might have lost the idea of what used to be dignified to them, it was widely recognized that they still possess some form of dignity that should be respected. This acknowledgment aligns with previous arguments on the notion of dignity, which emphasize that all persons have a basic human dignity (Nussbaum, 2008; Pullman, 1999). This underlines that dignity also contains an external element, meaning that a basic level of dignity is in part identified by others and encompasses the value or worth ascribed by others. (Franklin et al., 2006; Nordenfelt, 2004). Such acknowledgment of this external dimension aligns with what Daryl Pullman calls basic dignity, which is fundamental to all human beings: “One does nothing to earn it and nothing can take it away” (Pullman, 1999). Similarly, such interpretation of the notion also correspond with Martha Nussbaum’s account, that people with dementia retain an inherent dignity grounded in their capabilities to potentially lead a flourishing life as sentient beings (Nussbaum, 2007). According to Nussbaum, dignity is rooted in essential human capabilities necessary for leading a flourishing life, including life, bodily health, bodily integrity, senses, imagination and thought, emotions, practical reason, affiliation, other species, play, and control over one’s environment (Nussbaum, 2008). While Nussbaum’s account of dignity has been critiqued for lack of specificity and contextualization in dementia care (Soofi, 2022), her capacity-based account of dignity establishes a relatively inclusive threshold, recognizing the inherent value of sentient beings who experience pain and pleasure.
While such a capability-based approach encompasses a range of potentially relevant capabilities, we found that healthcare professionals largely acknowledged certain domains as being inherent constituents of this type of dignity that all individuals have. One interpretation of such universal dimensions of dignity were healthcare professionals’ perspectives that physical appearance is important for upholding dignity. Other studies argue that given the vulnerability of people with dementia and their dependency on personal care, promoting dignity involves ensuring they are well-groomed and appropriately dressed (Hall et al., 2014).
Although healthcare professionals’ perspectives on dignity encompassed various conceptual understandings, the lingering issue of conceptual vagueness associated with the notion of dignity remains. This study’s findings highlight the need for a clear, operational definition of dignity in dementia care, acknowledging its components to ensure consistency and quality in caregiving practices.
Implications for Healthcare Professionals
Our study also underscored the existence of diverse interpretations of the notion. This draw attention to the conceptual vagueness surrounding the concept of dignity. An ambiguity which poses a potential challenge, as promoting a specific view of dignity relies on achieving conceptual consistency and agreement regarding its definition. In fact, asymmetrical conceptual understandings of dignity might, in effect, sanction certain violations of some dimensions of dignity when it comes to people with dementia (Jacobson, 2009; van der Geugten & Goossensen, 2020). If no clear and agreed-upon understanding of the notion exists, misunderstandings and misinterpretations can arise. For this reason, definitional uniformity on dignity in dementia care is important. Inconsistencies in definitions and policies surrounding dignity can lead to variations in care practices and undermine the ideal that all people with dementia should have the same quality of care. The diverse interpretations of dignity point to a need for comprehensive training programs aimed at healthcare professionals to understand and uphold dignity in dementia care. These programs might either ensure a consistent understanding of dignity and enhance awareness, sensitivity, and skills in providing dignified care to people with dementia, or at the very least actively acknowledge this multifaceted understanding of dignity, emphasizing that although the specific meaning of dignity may vary, every individual requires and deserves a fundamental level of dignity in their care.
Strengths and Limitations of the Study
The multifaceted qualitative approach of this study, which combined both unprompted records of healthcare professionals’ views on dignity and insights from plenary peer discussions, provided clearer insights into the fundamental aspects of healthcare professionals’ understanding of dignity. However, it is important to acknowledge certain limitations. Firstly, while the data we collected from healthcare professionals were rather diverse, including concise statements and rather comprehensive explanations about the notion of dignity, much of the data was brief sentences without further elaboration, which may have limited the explanatory quality. Additionally, limitations related to participant sampling and the transferability of the study must be considered. As we utilized convenience sampling within a single municipality, the findings may not be fully transferable to other contexts. In similar vein, we acknowledge a limitation regarding the influence of sex and gender on our analysis of healthcare professionals’ perspectives of dignity. Given the predominantly female composition of our sample, it is plausible that perceptions of dignity may be influenced by such factors. While our analysis did not explicitly examine the impact of sex and gender on participants' perspectives, future research should delve into this aspect to better understand how considerations of dignity may vary across different sexes and genders. This would provide a more comprehensive understanding of the factors shaping perceptions of dignity in dementia care. Furthermore, although we obtained data from a relatively large sample of healthcare professionals, conducting in-depth interviews with the respondents would potentially have yielded more reliable results.
Conclusion
In this study, we explored healthcare professionals’ perspectives on the concept of dignity in dementia care. We found that their views on dignity varied, encompassing both a relative dimension, where dignity varies from person to person, and a basic dimension, where everyone has a certain level of dignity that should be respected, regardless of their awareness. While this distinction between relative and universal dimensions of dignity corresponds with both theoretical accounts and previous research, the divergence in understandings also highlights the ongoing issue of conceptual vagueness.
Footnotes
Acknowledgements
This research was carried out as part of the project titled “DEMENTIA ID,” at the National Institute of Public, University of Southern Denmark, and has received funding from the Velux Foundation, within the frame of the program, HUMPraxis. The research was carried out under the Grant agreement nr. 27773. We would like to thank Amalie Oxholm Kusier, Carsten Hinrichsen, Maj Britt Nielsen, Ida Nielsen Sølvhøj, Simon Kinch Riis-Vestergaard and Sofie Smedegaard Skov for their much-appreciated comments on an earlier draft of this manuscript in the spring of 2023. They have all given their permission to have their names published.
Author Contributions
Frederik Schou-Juul has involved in conceptualization and study design; data curation; formal analysis and investigation; methodology; project administration; supervision; writing—original draft manuscript; writing—review and editing. Rebecca Amalie Struwe Kjeldsen has involved in conceptualization and study design; data curation; formal analysis and investigation; writing—original draft manuscript; writing—review and editing. Lucca-Mathilde Thorup Ferm has involved in data curation; writing—review and editing. Sigurd Lauridsen has involved in conceptualization and study design; funding acquisition; methodology; project administration; writing—review and editing.
Data Availability Statement
The data supporting the results of this study are available from the first author of the study upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Velux Foundation under grant number 27773.