
Abstract
Although many large Chinese cities have begun to implement hospice services, hospice care is still a relatively new concept in many parts of the country, especially in smaller cities. The purpose of this study was to gain a better understanding of health care providers’ (physicians and nurses) perceptions of the facilitators and barriers to hospice care implementation in a fourth-tier city. Using a qualitative descriptive approach, semi-structured, open-ended interviews were conducted with 15 health care providers. Two major categories for developing hospice care were identified: (a) prospective facilitators and (b) perceived barriers. In addition, there is currently much ambiguity regarding what agency should oversee hospice services if implemented, who should be responsible for payment, the importance of developing interdisciplinary care teams and concerns about worker shortages. Future research is encouraged to investigate attitudes towards hospice care across various local healthcare systems and to promote the development of local hospice care support.
Introduction
End-of-life (EOL) care serves as an overarching concept that may include palliative care, supportive care and hospice care (National Cancer Institute at the National Institutes of Health, 2024). Palliative care remains accessible across all phases of a severe illness, even while patients are undergoing active treatments such as chemotherapy, radiation therapy, or immunotherapy for cancer (American Cancer Society, 2019). Hospice care, on the other hand, directs its attention towards addressing the medical, psychological, social and spiritual aspects of EOL care, as well as symptom management for patients during the terminal phase of an incurable disease (Park et al., 2012; Shiel, 2018). Hospice care in China draws upon hospice philosophies from Western cultures (Huang, 2015; Ling et al., 2020; Lu et al., 2018), and its adoption and implementation within the country remain relatively recent. Subsequently, it is unclear whether hospice care is of interest to practitioners and patients or how feasible it is to implement hospice programs, especially in smaller-tier cities in China.
Chinese cities are categorized into different tiers based on five indicators: concentration of commercial resources, city transport hubs, degree of activity for urban residents, lifestyle diversity and future plasticity (New Tier 1 City Research Institute, 2023). Thus, city classification is determined by various economic development levels rather than population (Wang et al., 2017) (see Table 1). To date, the focus has been on implementing hospice care in top-tier cities like Beijing. In 2017, five districts were selected as the first batch of the national pilot cities for hospice care. These included the Haidian District of Beijing, the Putuo District of Shanghai, Changchun in Jilin Province, Luoyang in Henan Province and Deyang in Sichuan Province (National Health Commission of the People’s Republic of China, 2018). Subsequently, in 2019, 71 diverse cities/districts (e.g., Nanjing, Shenyang and Haikou) were chosen to participate in the second batch of the national pilot cities for hospice care. These cities are involved in developing local hospice care services, indicating an increasing attention and interest in hospice care among the general population (Ni et al., 2021; Ning, 2019).
Chinese City Tier System.

Despite the increasing initiation and endorsement of hospice services by more and more cities, there remains a lack of research into the experiences and attitudes of health care providers regarding hospice care, as well as the developmental process of hospice services in these pilot cities. In addition, since most of these pilot settings are located in first and second-tier cities, it is crucial to understand hospice care in lower-tier cities and to encourage the inclusion of health care providers from economically less developed areas in research. The aim of this study was to explore the perceived facilitators and barriers to implementing hospice care among health care providers in a smaller tier city (Binzhou) in China.
Binzhou, a fourth-tier city, was selected as the study site for a few reasons. Older adults (aged 60 years and older), a group most likely to use hospice services if available, accounted for 21.8% (854,900) of the total Binzhou population (Binzhou City Bureau of Statistics, 2021). Moreover, terminal conditions well suited to hospice care—late-stage cardiovascular and cerebrovascular diseases, cancer and respiratory diseases—were common causes of death in Binzhou (Zhang & Lin, 2014). Developing hospice programs may benefit older people with terminal or incurable conditions by meeting hospice care needs among older clients and their family members.
Additionally, some barriers within the Chinese healthcare system significantly impede the advancement of hospice care. For example, oncology nurses from four hospitals in Beijing encountered challenges in providing hospice care to terminally ill cancer patients due to perceived lack of financial support and fear of medical disputes (Zheng et al., 2021). Currently, hospice services are not fully covered by health insurance and are not considered essential nursing care, resulting in insufficient funding for training and staff recruitment by hospice care agencies (Zheng et al., 2021). Concerns about potential medical disputes arising from providing hospice care reported by Zheng et al. (2021) often stem from differing perceptions between health care providers and patients (or their relatives) regarding treatment plans and outcomes. These systemic issues are challenging to address at the individual level and require systemic changes within the healthcare system.
Methods
We used a qualitative descriptive approach. This approach is minimally theorized, provides an inclusive summary of an event, and obtains data from naturalistic inquiry (Sandelowski, 2000). Our research was approved by the Institutional Review Board for Human Subjects Research at Miami University, where both authors were working at the time of the research (approval no. 02142r).
Participants
Participants were physicians and nurses who practiced at Binzhou Medical University Hospital and Binzhou Renmin Hospital, both of which are highly rated and a likely starting point for hospice services in Binzhou (Yang et al., 2017). Given their pivotal roles in shaping the Chinese healthcare system, physicians and nurses would serve as the primary executants of hospice services if available and would be involved in the initial stage of implementing hospice services and pilot programs (Lu et al., 2018). Participants were recruited through the Chinese social media platform WeChat by sharing the research invitation via “Moments” and using a snowballing method, where initial participants reposted the information to reach other health care providers, who then directly contacted the researcher if interested. Inclusion criteria were: (a) official household registration in Binzhou, (b) a minimum of 2 years of experience serving or taking care of terminally ill patients, and (c) a practicing physician or nurse. All participants provided written informed consent and received a copy of the consent document in Mandarin Chinese.
Data Collection
Participants completed semi-structured interviews composed of a set of open-ended questions. Interview questions were based on previous studies regarding hospice use in China (Ni et al., 2019; Zheng et al., 2021) as well as through input from peer experts (i.e., two gerontology faculty members and an academic social work researcher who studies hospice care; see Supplemental File for the Interview Guide). The interviews explored the current state of end-of-life care and hospice services within the local healthcare system. Discussions covered interdisciplinary team practices, training needs, feasibility, facilitators, and barriers of hospice care, as well as potential medical disputes, financial support, and essential human resources. All interviews were conducted, audio-recorded, transcribed, and coded in Mandarin Chinese to ensure the participants’ meanings were not changed through the translation process. All personal identifiers were removed. Interviews were conducted via the video program WeChat and lasted approximately 1 hr each.
Data Analysis
We analyzed data for categories with the help of Dedoose software. First, a combination of the inductive and deductive coding approaches was implemented. Inductive codes were primarily identified during the coding process and developed based on key meaning units in the transcripts, which are closely relevant to the data themselves. Although most coding forms are data-driven, some pre-existing coding frames are also used. Specifically, deductive codes correspond to facilitators and barriers identified through an extensive literature review. These are incorporated into the categorization during the code creation and the deductive coding process. Next, we used the code co-occurrence function in Dedoose as a starting point to identify categories. This helped us understand how study participants naturally discussed certain concepts jointly represented by codes. We looked for overarching patterns across the data and extracted excerpts with high co-occurrence, which enabled us to determine overarching schemas and present findings under categories. We also examined the data for repetition, similarities and differences across the data, sorting and arranging important quotes and expressions into exemplars.
Trustworthiness
Based on the sample recruited and data collected we were able to capture a reasonable range of experiences to address the aim of the study (Braun & Clarke, 2021). Data trustworthiness was confirmed through member checking (i.e., participant validation) (Carlson, 2010; Creswell & Miller, 2000; Hadi & José Closs, 2016). The researchers sent the major categories (translated into Mandarin Chinese) to the participants via WeChat. Participants were asked if they thought the study results accurately reflected their experiences and were invited to submit comments or discuss with the first author (Carlson, 2010; Creswell & Miller, 2000; Hadi & José Closs, 2016). All the responded participants confirmed the credibility of the interpretation, and none of them had further clarifications or concerns. Data trustworthiness was also supported though peer debriefing (Carlson, 2010; Creswell & Miller, 2000; Hadi & José Closs, 2016). Several faculty research experts reviewed the study results and provided written feedback to the researchers who then incorporated the additional feedback (Creswell & Miller, 2000).
Results
Participant Demographics
The study included a total of 15 participants, with 8 physicians and 7 nurses. Table 2 shows the study participants’ demographic characteristics. Eight of the participants were from Binzhou Medical University Hospital. The mean age of health care providers was 46.9 years (SD = 9.6), with a range of 29 to 59. Female participants account for 53.3% of the total sample (n = 8). All participants self-identified as Han Chinese (n = 15). Participants were highly educated (86.7% had earned a bachelor’s degree or higher). The average length of service in caring for terminally ill patients was 23.4 years (SD = 11.3), with a range of 3 to 37. Over one-fourth of participants work in the oncology department (26.7%), followed by cardiovascular medicine (20.0%), respiratory medicine (20.0%), geriatric health care (20.0%), and pain medicine (13.3%). The average length of interviews was 56 min, with a range of 37 to 79 (SD = 12.0). Only four participants had not heard of hospice care.
Demographic Characteristics (n = 15).
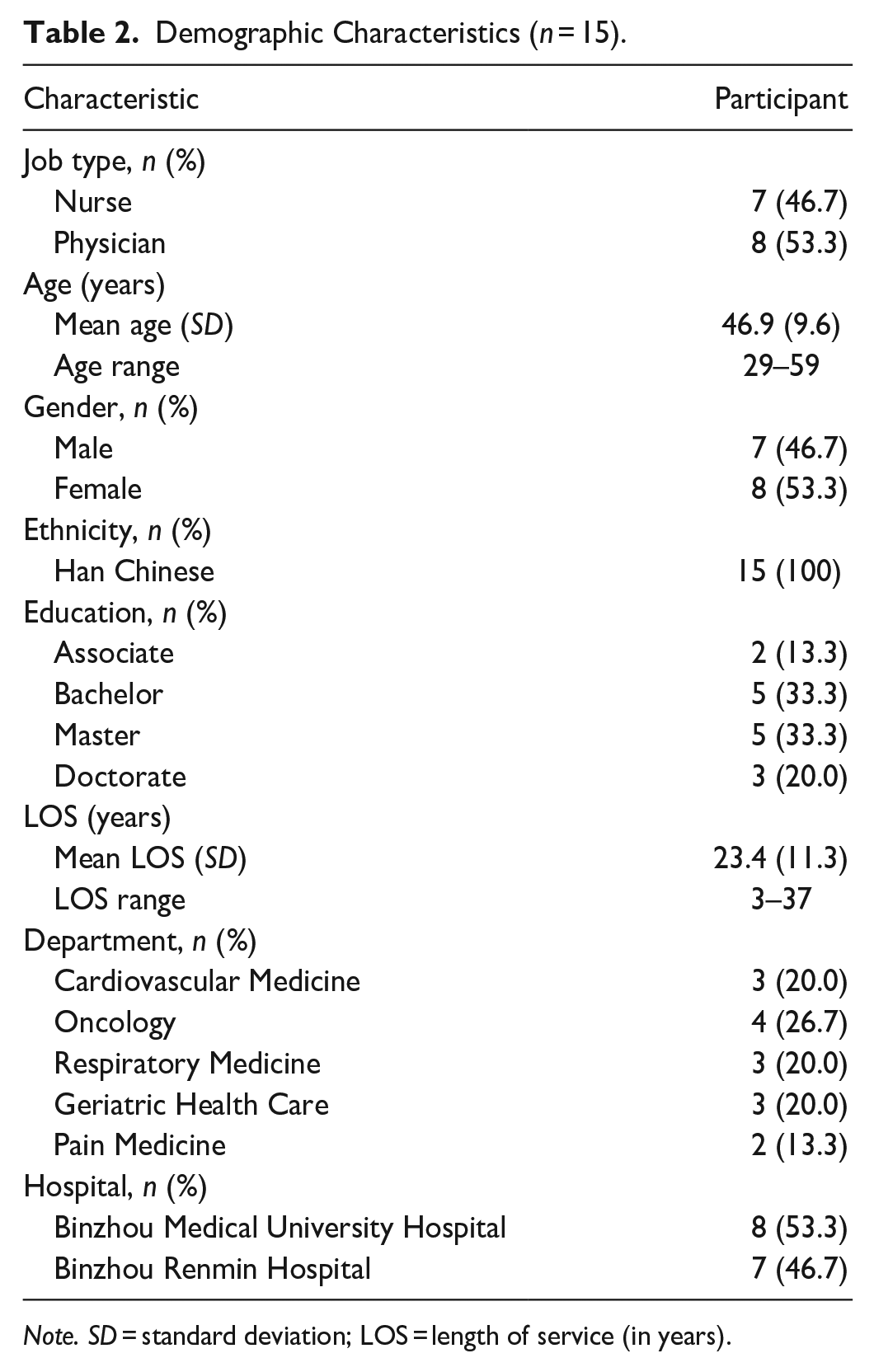
Note. SD = standard deviation; LOS = length of service (in years).
Two major categories related to developing hospice care were identified: prospective facilitators and perceived barriers.
Category 1: Prospective Facilitators to Developing Hospice Care
There were some notable facilitators identified regarding potential hospice care implementation in Binzhou. Two sub-categories are summarized under the main category framework, including “national-level promotion” and “accessible medical resources on hand.”
Sub-Category 1: National-Level Promotion
At the government level, approximately half of the participants (n = 7) demonstrated that the attention and initiatives on hospice care from the national level are facilitators of implementing hospice care in Binzhou, characterized by national policy initiatives, medical resource redistribution, and decreasing medical disputes.
The majority of participants (n = 11) had already heard about hospice care before the interview; roughly half (n = 5) were able to define hospice care based on their understanding. Even though Binzhou has not yet established a specific and comprehensive hospice care agency, health care providers have begun learning about hospice care through national-level policies and hospital education. Their understanding of hospice care values has been gradually increasing.
Two participants suggested that the government-led healthcare system has the advantage of redistributing medical resources. A nurse explained: The government definitely is the one who makes decisions. They are the main leader in running the healthcare system. Once they approve hospice care citywide, other affiliate units will swiftly respond to their demands, like increasing funding allocation, assigning more workers, providing pertinent medical facilities, etc.
A physician noted, “If there is a growing demand for hospice care in the future, the government will ask these two units [the Binzhou Health Commission and the Finance Bureau of Binzhou] to allocate more grants for hospice care and cut funds from other areas.”
In addition to the advantage of resource redistribution within the healthcare system, a few participants (n = 4) also indicated that decreasing medical disputes is another facilitator when implementing hospice care. A nurse said: Medical dispute is usually a severe problem in the field of medicine. Patients often argue and fight with us. Previously, the hospital had a patient beat the doctor and caused the doctor to be hospitalized.. . . Hospice care is for those terminally ill patients; their families may be more upset than ordinary patients. Having law protection is good for us.
Sub-Category 2: Accessible Medical Resources on Hand
The majority of participants (n = 13) discussed that owning abundant and accessible medical resources is a significant advantage of implementing hospice care in Binzhou. Abundant medical resources consist of well-equipped facilities, medical staff with a high level of expertise, and a strict quality management system in operation. For example, a nurse proudly said: You know, Binzhou Medical University Hospital is a 3A hospital. We are the largest central hospital in the northern part of Shandong Province, which is downstream of the Yellow River. Therefore, we also receive patients from neighboring cities such as Zibo, Dongying, and Dezhou. We have a high level of medical resources and personnel in the Binzhou area, which can be considered a potential advantage.
Overall, participants seemed to feel confident that Binzhou was well equipped to implement hospice care should the barriers such as a payment method and additional staffing be met.
Category 2: Perceived Barriers to Developing Hospice Care
Perceived barriers identified by participants consisted of four distinct levels in the healthcare system, including governmental, hospital, societal, and patient/individual levels. Four sub-categories are summarized under the main category of barriers, including “deficient policy design,” “human resource shortage,” “insufficient mobilization of hospice care associations,” and “unknown about hospice care and potential resistance.”
Sub-Category 1: Deficient Policy Design
At the government level, participants (n = 10) focused on the lack of institutional design and policy support for hospice care, as well as unclear responsibilities among relevant government departments. One nurse stated: Right now, I am unclear if there are existing hospice care policies in Binzhou. I do not think there are any. I have not heard from my director and other colleagues yet. Even though we have pain relief practice, this is covered neither by health insurance nor hospice care policy.
A physician noted that clearly assigning duties for each government department outside hospitals involved in hospice care is essential. He mentioned: There has been established cooperation for us with the Binzhou Health Commission. Basically, if we want to acquire financial support and receive a budget, we need to submit our hospital’s needs to our governing body—the Binzhou Health Commission. They will then submit it to the Finance Bureau of Binzhou to get approval for the budget. Since hospice care has not been well-established in Binzhou, I am not quite clear if we go through the same procedure or via different government departments to gain budget.
The participant explained that the Health Commission is a government department managing the local healthcare system, including sanitation, public health, epidemic prevention and control, drug and medical equipment supervision, medical qualification review, and so forth.
Additionally, other barriers included inadequate health insurance coverage and lack of standardized payment methods for hospice care. Some noted that cost was a big consideration, including who would bear the cost of care. There was additional concern regarding lower income patients for whom out-of-pocket payment would likely be a barrier to hospice care. One physician demonstrated a need for a clearly-defined long-term payment method for hospice care in place.
Sub-Category 2: Human Resource Shortage
At the hospital level, all participants (n = 15) spoke about the issues of insufficient personnel, especially the difficulties that would be associated with assigning a large number of health care workers to a newly established hospice care unit. Some referenced the working pressure they experienced during the pandemic. A physician indicated that the greatest obstacle to fully carrying out hospice care is the shortage of health care professionals. He explained: We are a small city, but you just imagine a large population base is being served by a small number of health care workers in several hospitals. Currently, hospitals are severely understaffed with health care workers. Especially during the pandemic, my workload is much higher. Basically, I have to see at least 15–20 patients on average per day. The tasks are heavy in my department.
In addition, with regards to the lack of sufficient people to take on roles required for hospice care, one physician noted that a multidisciplinary team traditionally focuses on medical practices among different departments based on specific cases. In other words, a multidisciplinary team is established specifically for individual patients and their unique cases, often involving multiple disciplines. The participant explained, “For example, treating an older patient with colon cancer involves professionals from the oncology, coloproctology, geriatric, anesthesiology, pain medicine departments, and so on.” He also pointed out, “We do not have someone taking charge of patients’ emotional conditions. It would be great if a professional here could help patients alleviate their anxieties. We do not have those professionals currently.”
Several participants (n = 5) specifically highlighted the insufficient personnel components in the multidisciplinary team, particularly the lack of psychological/emotional counselors, despite these teams being well-established in high-level hospitals with a primary focus on medical practice. A nurse also noted the demand for psychological/emotional counselors in the multidisciplinary team, stating, “During the Covid-19 pandemic, many of my older patients and their families were very anxious and scared of getting infected. I think they need more humanistic care. Nobody really provides this kind of support with a psychological background.” Therefore, incorporating psychological and emotional professionals into the multidisciplinary team is crucial for providing psychological comfort to patients in need.
Sub-Category 3: Insufficient Mobilization of Hospice Care Associations
At the societal level, a few participants (n = 3) illustrated that inadequate mobilization of social forces such as hospice care associations had hindered the development of hospice care in Binzhou. A physician specifically identified this issue and said: Except for official support, unofficial support and recognition from broader society are important. You know, in Binzhou, we have a variety of associations; I can think of, like the health commission, writer, lawyer, scientific technology, photography, environmental protection, and construction industry. But I have never heard about a local hospice care association. I am not sure if there is one at the province level or nationwide. That kind of association is important as many people from the grassroots level can participate.
Another physician also expressed a similar perspective regarding the importance of social organizations: “We are a small city. Compared to bigger cities, we have fewer medical organizations. . . . I have not heard they have a group focused on hospice care.”
The previous two sub-categories focused on government and hospital levels, respectively. Yet, participants also underscore the significance of unofficial power in the broader society.
Sub-Category 4: Unknown About Hospice Care and Potential Resistance
At the patient/individual level, another significant barrier regarding the implementation of hospice care is the lack of familiarity with hospice care and potential rejection of its practice philosophy. Participants (n = 6) noted that few patients in Binzhou are knowledgeable about and familiar with hospice care. One physician mentioned: As far as I know, many patients may not even know what hospice care is. They may only know that if they have late-stage diseases, they need to go to the hospital for emergency treatment, such as entering into ICU [intensive care unit]. They may not realize hospice care is another option.
This issue identified by participants also raised another pertinent obstacle—potential resistance among some patients and families toward hospice care. Four participants brought up this concern during interviews. A nurse said: The biggest challenge is likely the patients’ families. They are ultimately willing to have their loved ones stay for as long as possible. Symptom relief may be acceptable to them, as they are willing to reduce their loved one’s suffering. However, they may not be able to accept the termination of further treatment. This may not be the case for all patients’ families, as they may also want their loved ones to live longer.
Overall, a large number of patients may have yet to hear about hospice care and are likely unfamiliar with what kind of services they will receive from hospice care. In addition, certain individuals may not accept the value of hospice care. A physician indicated, some patients and families have to accept hospice care to avoid expenses generated from extended hospital stays, surgeries, or ICU because of financial strain.
Discussion
Exploring health care providers’ perceptions of the facilitators and barriers to implementing hospice care, particularly in smaller-tier cities, is a novel area of research. In our study, we identified two major categories for hospice care implementation: prospective facilitators and perceived barriers. Notable facilitators include “national-level promotion” and “accessible medical resources on hand.” Perceived barriers encompass four levels: governmental, hospital, societal, and patient/individual. These barriers are further divided into “deficient policy design,” “human resource shortage,” “insufficient mobilization of hospice care associations,” and “unknown about hospice care and potential resistance.” Exploring the implementation determinants (i.e., facilitators and barriers) of hospice care will provide local health care providers and policymakers with valuable insights into existing strengths and foreseeable challenges. This knowledge can uniquely contribute to the field of hospice and EOL care by guiding the development and delivery of effective hospice services, ultimately improving their quality and accessibility.
Palliative care is in various stages of development and integration into health care in many countries (Brant & Silbermann, 2021), and factors influencing this development have been the focus of study. In an analysis of system-level characteristics that influence the implementation of palliative care in Canada, England, Germany, and the USA, researchers concluded that legislation, regulation (e.g., education and training), financing, and public knowledge and perceptions were common barriers (Klinger et al., 2014). Although cost is often a major concern when accessing a care service, others have argued that offering high-quality EOL care involves addressing a range of barriers beyond merely financial constraints (Finkelstein et al., 2022). A systematic review of 29 studies focusing on barriers to palliative care utilization by oncology patients identified barriers included those related to the patient and family, health care providers, and the healthcare system or policy (Parajuli & Hupcey, 2021). Although none of the included studies were conducted in China, the findings are important. At the patient level, for example, some studies found that negative stereotypes and a lack of understanding toward palliative care lead to misunderstanding and distrust of the service’s nature. Care providers, who often have insufficient training, were often reported to equate palliative care with “giving up” and communication barriers between patients and caregivers were also linked with a lack of hospice care utilization. In the healthcare system, organizational/structural aspects such as less-defined work duties of care teams, a focus on treatment rather than palliative care, shortages of health care professionals, and long waiting times were barriers frequently observed in the included studies.
In contrast, facilitators of palliative care have also been identified. For example, in Klinger et al.’s (2014) cross-country comparison, facilitators in addition to stable funding included advance care planning, and standards of practice and guidelines for hospice and palliative care. Indicators of progress to achieving quality EOL care have also been proposed and point to important facilitators. These include access to pain-relief medicines, patient-centered care, integrating EOL care services into the universal health system to increase the likelihood of lower cost of care, establishing monitoring mechanisms and regulation standards toward EOL care services, creating required training educational programs for health care professionals to improve their knowledge regarding EOL care services, initiating public education to increase knowledge and awareness about available EOL care, and establishing community networks of palliative care (Finkelstein et al., 2022). These indicators provide a fundamental blueprint for a country in the initial stage of developing its EOL programs.
Since this literature on barriers and facilitators to EOL and palliative care has predominately focused on Western countries, the findings of our study fill an important gap. Participants’ perspectives on facilitators and barriers to hospice care share some similarities to those found in studies conducted in other parts of the world. For example, with respect to identified barriers in this study, human resource shortages are commonly found in low-to-middle-income countries and as well as in high-income countries, such as the United States (Brant & Silbermann, 2021; Finkelstein et al., 2022; Parajuli & Hupcey, 2021). Compared to more developed nations, human resource deficiencies are more severe in highly population-dense countries like China. According to Global Health Workforce Statistics from the World Health Organization (WHO), China had 23.87 medical doctors and 33.05 nursing and midwifery personnel per 10,000 in 2020 (World Health Organization (WHO), 2023). The data reveal a massive personnel gap between supply and demand in the Chinese healthcare system. It is not surprising, therefore, that in a city with a resident population of approximately 3.9 million, many participants noted that the issue of insufficient staff might significantly limit the implementation of hospice programs in local hospitals.
In contrast to experiences in other countries, insufficient mobilization of social forces (i.e., hospice care associations) is a unique barrier identified in this study. Participants noted that broadly promoting hospice care to people from the grassroots is essential. Utilizing social forces, like social hospice care organizations, is vital in this process. A city-wide hospice care industry association has the capacity to establish technical service standards, industry norms, and professional qualifications pertinent to hospice care, thereby fostering the advancement of hospice care in Binzhou.
While significant progress has been made in implementing hospice and EOL care services in high-income countries (e.g., Canada, UK, Germany, and the United States) (Klinger et al., 2014), China is still in the initial stages of implementing these services. This development has led to regional variations in the country. As previously noted, in contrast to a fourth-tier city, the first and second-tier cities are more likely to be familiar with hospice care and have established operational procedures for hospice care (Lu et al., 2018; Ni et al., 2021; Ning, 2019; Shu et al., 2021). Currently, even though there is a national hospice care organization (i.e., Rong Foundation), it is located in Beijing. The study city, like many others in China, are without an official hospice care agency nor covered hospice care services with medical insurance. As a result, hospice care has not become widely known among the general public at the societal level in China. These barriers need to be overcome to successfully establish hospice care.
Lack of knowledge about and resistance to EOL care services are not only found in the Chinese cultural context (Ni et al., 2019), but also exist in some developed countries with advanced EOL care programs around the world (Finkelstein et al., 2022; Klinger et al., 2014; Parajuli & Hupcey, 2021). Although the general public is familiar with medical treatment in the modern healthcare system, they may not be aware of or accepting of EOL and hospice care services as a component of modern medicine, with its focus on comfort, maintaining dignity, and providing emotional and spiritual support. Some resistance to hospice care among certain patients and their families is foreseeable across nations due to heterogeneities in culture, social norms, values, religious beliefs, and intense desires for healing and survival.
In addition, while there are identified governmental barriers in other countries, such as financial challenges, legislative issues, and lack of integration of EOL care into existing healthcare system (Brant & Silbermann, 2021; Finkelstein et al., 2022; Klinger et al., 2014), the barriers identified at the governmental level are unique in Binzhou. Deficient policy design is a primary barrier to implementing hospice care in Binzhou, specifically lack of specific implementation and operational policies, unspecified duties and responsibilities among relevant government departments, and insufficient health insurance coverage, along with the absence of standardized payment methods for hospice care.
There is uncertainty about how to proceed through the government bureaucracy in order to implement hospice care in Binzhou. Previous literature noted that the work duties of palliative care teams are less defined, which is one of the primary structural barriers in the United States (Parajuli & Hupcey, 2021). The lack of clearly defined duties was also identified in this study, but participants focused more the specific procedures for hospice care approval across central government departments, pointing to the role of government bodies in designing operational policies and spending coverage. Clearly-specified duties for these governmental bodies with respect to hospice care services is an important starting point for successful implementation of hospice care services and ensuring hospice care providers have the support they need.
Accessible and abundant medical resources were regarded as facilitators for implementing hospice care in this study. This phenomenon can be explained by the highest practice level of studied hospitals. All the study participants were recruited from the top two local hospitals, and the researcher perceived confidence from participants about their medical environment, resources, and techniques. This also demonstrates that medical hospitals are the starting point for carrying out hospice care with rigorous regulations and reliable medical practices. Overall, although challenging, it is still feasible to implement hospice care in the study city and similar settings in China since hospice care is recommended to be combined with current health care services.
Limitations of the Study
Although important insights were gained from the participants in this study, the findings may not be representative of the perspectives of health care providers in other settings where hospice services may be more established. The rich and detailed information collected from this study was based on the medical environment, social context, and healthcare system in the study setting. Even though the study results have reference value for other cities at an equivalent tier and plans for establishing hospice services, the influence of distinct regional cultures also need to be considered. Future research is suggested to explore perspectives related to hospice care in other settings in China.
In addition, this study explores perspectives of hospice care among physicians and nurses without further inquiring into patients’ attitudes and understanding. It is important to also understand the perspectives of patients, families, Baomu (i.e., hired family caregivers), administrative personnel in long-term care facilities, and government officials to guide the implementation of hospice care in China.
Implications for the Broader Applicability of Hospice Care Implementation
Recognizing the significance of health care providers’ professional knowledge and experience, alongside the potential impact of hospice care education they can receive, emerges as a pivotal aspect deserving attention in hospice care. Health care providers play fundamental roles in providing support and comfort to terminally ill individuals. Therefore, integrating these considerations into future hospice care research is essential for enhancing training programs and ultimately improving the overall hospice care experience for patients and their families. Additionally, local governments may gradually promote the concept of hospice care within communities, schools, nursing facilities, and workplaces. This strategy can strengthen public understanding of hospice care and reduce excessive spending on medical treatments.
Despite the fact that hospitals are the initial executants of hospice care, we cannot solely limit hospice services inside medical institutions. In the long run, the overall goal is to develop hospice care extensively by expanding it to a broader scope beyond 3A hospitals. Hospice care is a type of EOL care that emphasizes pain management, symptom alleviation, and spiritual care rather than hastening or postponing death (American Cancer Society, 2019). In other words, patients may not need special medical treatment at the end of their lives; hospice care does not require medical technology as the equivalent of urgent medical surgeries. For a patient who chooses to use hospice care, it may be more practical to age in place in the communities, stay in a long-term care facility (e.g., nursing home), transfer to a local health clinic in rural areas, or remain in homes based on their preferences. Hospice care should be set up in a long-term care facility that combines medical care and nursing care. In the terminal stage of life, patients may not need or prefer to stay in hospitals, but they need more attentive care and considerate companionship.
Conclusion
Establishing a comprehensive EOL care system, inclusive of hospice care and palliative care, is essential to improve the quality care for patients with terminal diagnoses. This study described facilitators and barriers that need to be considered to support the introduction of hospice care outside major cities in China. Presently, there is significant ambiguity concerning the oversight agency for hospice care implementation, payment responsibility, the necessity of interdisciplinary care teams, and concerns regarding workforce shortages. Future research is encouraged to explore attitudes towards hospice care within local healthcare systems. Advocacy for community-based hospice care support structures will also be important.
Supplemental Material
sj-docx-1-gqn-10.1177_23333936241273199 – Supplemental material for Perceived Facilitators and Barriers in Implementing Hospice Care: A Qualitative Study Among Health Care Providers in Binzhou, China
Supplemental material, sj-docx-1-gqn-10.1177_23333936241273199 for Perceived Facilitators and Barriers in Implementing Hospice Care: A Qualitative Study Among Health Care Providers in Binzhou, China by Heshuo Yu and Kate de Medeiros in Global Qualitative Nursing Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.