
Abstract
In Canada, different categories of nursing professionals, including registered nurses and practical nurses, often “collaborate” to provide care to patients. How their collaboration is currently conceptualized in the literature varies; and these conceptualizations are not always contextualized by the complex sociopolitical environment in which nursing professionals work. The purpose of this study was to explicate how different categories of nursing professionals (registered nurses and practical nurses) worked together to provide patient care after a provincial health authority implemented a new nursing care delivery model to “optimize” patient care. The authors used Smith’s institutional ethnography to guide the study, and data collection methods included observing, conducting interviews, and identifying the texts activated through the nursing professionals’ work. Data analysis focused on the social organization of the nursing professionals collaboration, while keeping the complex contexts within they completed their daily work in view. The article concludes with recommendations for future research.
Across Canada, different categories of nursing professionals, including nurse practitioners (NPs), registered nurses (RNs), registered psychiatric nurses (RPNs), and practical nurses (PNs) often “collaborate” to provide patient care. Over the years, what their collaboration actually means has been conceptualized in different ways, including different scopes of practice and nursing care delivery models, as well as a desire for nursing workforce “optimization.” These conceptualizations, however, lack a full exploration into the key contextual factors, such as the complexity of patients’ care needs and hierarchal nature of healthcare settings, that define all nursing professionals’ work. To-date, few studies have fully considered the complex sociopolitical environments in which different categories of nursing professionals work together to provide patient care. In this qualitative study, the authors sought to explore the articulation of how categories of nursing professionals’ (specifically RNs’ and PNs’) work together within the context of such larger forces after the implementation of a new nursing care delivery model. This model, the “Organizing Nursing Team Resources for Accountability Collaboration and Communication” (or ONTRACC model), shifted nursing care from being delivered by RN-PN teams, who worked together as “buddies” and cared for an assignment of patients together, to RNs or PNs who worked independently and cared for a smaller assignment of patients. It was developed by nursing leaders within the health authority over a period of several years.
The authors used D. Smith’s (1987, 1990, 2005) institutional ethnography (IE). D. Smith (2005) proposed IE as an “alternate sociology” to examine how work processes are coordinated. Although the collaborative nature of nursing work is well-known, this study contributes to new knowledge in two ways: (a) it explicates the organization of nursing professionals’ work in the context of the largely unseen sociopolitical relations of everyday life after the implementation of the ONTRACC model, and (b) it suggests some of possible directions for future research. Study results are presented through a detailed description of how the RNs’ and PNs’ work together was socially organized through the new ONTRACC model, as well as a re-articulation of the meaning of collaboration within the nursing profession.
What is Currently Known? Current Conceptualizations of “Collaboration”
In many studies that explore collaboration between different categories of nursing professionals, researchers conceptualize their working together in terms of their scopes of practice, particularly the “maximization” or “fullness” of these scopes. According to Oelke et al. (2016), nursing professionals maximize their scopes of practice when they work “to the full range of roles, responsibilities and functions that [they] are educated, competent and authorized to perform” (p. 46). Although all regulated nursing professionals are educated at a university or college-level, the minimum education requirements for each category differ. NPs require a master’s degree, RNs require a baccalaureate degree, and RPNs and PNs require a 2-year diploma. Each nursing professional’s individual scope of practice is related to their education, but other factors, like workplace policies, also determine what they “are allowed to do” (Nurses Association of New Brunswick and New Brunswick Association of Licensed Practical [NANB & NBALPN], 2015).
Many studies that focus on the maximization or fullness of scopes of practice are undertaken by researchers with healthcare/nursing managerial backgrounds, who use mixed methods approaches (Dubois et al., 2012; Lankshear et al., 2005; Oelka et al., 2016). In the healthcare management literature, researchers tend to view the maximization of scopes of practice as a complex phenomenon, with the barriers and facilitators to maximization being of particular interest. In line with the maximization of scopes of practice being a complex phenomenon, there are inconsistency with how different categories of nursing professionals’ (NPs, RNs, RPNs, and PNs) scopes of practice are enacted across Canada. For example, Butcher and MacKinnon (2015) reviewed different nursing regulatory documents and found many variations around these roles and little collaboration between different nursing groups. Consequently, these nursing professionals’ tasks, roles, and how they work together varies from province/territory to province/territory and practice setting to practice setting. Particularly, the scope of practice for administering medications varies for PNs across Canada; and prior to the roll-out of the ONTRACC model, the provincial PN groups and the health authority worked to expand the PNs’ scopes of practice to include medication administration in “acute” settings. As a result, the PNs employed by the local health authority needed to upgrade their qualifications by completing a medication administration course. After the PNs completed this course, they received mentorship from an RN, usually a clinical nurse educator, to practice administering medications to patients in their practice setting. It was only after most of the PNs completed their mandatory medication administration education that individual units started independent patient assignments.
Some researchers, who explore nursing scopes of practice, are also interested in different nursing care delivery models, including the mixes of nursing staff or different ratios/numbers of each nursing professional category (Dubois et al., 2012). According to Prentice et al. (2022), “[n]ursing care delivery models refer to the organization and structure of how nursing care is provided” (p. 1). Much of the literature with respect to nursing care delivery models is descriptive in nature and focuses on either the division of biomedical tasks (e.g., administration of medications) or on the model itself (e.g., team-based models; Canadian Nurses Association, 2010; Dubois et al., 2012). Studies that focus on the division of biomedical tasks (i.e., interventions to treat diseases) also often discuss task/role overlap or “shared practice boundaries” (Scholes & Vaughan, 2002), which are frequently reported as a cause frustration and tension. While the literature on nursing care delivery models often provides interesting information about the tasks/roles of different categories of nursing professionals, there a is need for more attention to the contextual factors, such as the complexity of patients’ care needs and hierarchal nature of healthcare settings, that are an integral part of all nursing professionals’ work together.
Studies that focus on the models themselves often consider the implementation or evaluation of team-based nursing care delivery models. In such models, teams of different categories of nursing professionals work together to complete specific activities for a group of patients (Prentice et al., 2022). Some researchers argue that these team-based structures support collaborative practice. Other researchers suggest that the outcomes for team-based models are less positive than the dominant reports and are more cautious about team-based structures (MacKinnon et al., 2018). For example, MacKinnon et al. (2018) suggested that a new team-based nursing care delivery model led to fragmented, task-oriented divisions of patient care between the RNs and the PNs (MacKinnon et al., 2018). Their research used IE to examine what was actually happening in a team-based nursing care delivery model in two hospitals in British Columbia (MacKinnon et al., 2018).
A more recent conceptualization of nursing professionals’ collaboration in the literature is nursing workforce “optimization.” Coe et al. (2023) define an optimized nursing workforce as, “one in which outputs (number of patients seen) and outcomes (clinical quality) are maximized with the same inputs (numbers of nurses) or when minimized inputs produce the same outputs” (p. 1). Many researchers who are interested in nursing workforce optimization have economics, healthcare/nursing managerial backgrounds and use quantitative approaches (Ganann et al., 2019, Lukewich et al., 2018). Often optimizing the nursing workforce overlaps with maximizing scopes of practice to create more flexibility for managers trying to use staff as efficiently as possible (MacKinnon et al., 2018, p. 2). Across Canada, with the legacy of neoliberal (i.e., market-oriented) policies and increased transfer of public services to private ownership, there is concern about the financial sustainability of the publicly insured healthcare system; and a great deal of scrutiny is placed on both healthcare delivery and spending. Healthcare staff salaries account for around 60% of most Canadian hospitals’ overall budgets, and historically, decision-makers have seen reductions in the number of healthcare staff to be a way to contain costs (Canadian Institute for Health Information [CIHI], 2019). More recently, however, the shortage of health care workers, exacerbated by the COVID-19 pandemic, has led to new issues of concern and reasons to optimize the nursing workforce for greater efficiencies.
Several studies have found efforts to contain costs through “minimized inputs” (e.g., reduced numbers of RNs) lead to less favorable patient care outcomes. Aiken et al. (2002) found reduced overall numbers of RNs to patients (i.e., RN-to-patient ratios) have been shown to have a negative impact on patient death rates (Aiken et al., 2002). Other researchers have found reduced RN-to-patient ratios have had a negative impact on lengths of stay (Thornblade et al., 2018), complications (Falk & Wallin, 2016), and “failure to rescue” (Tourangeau et al., 2006). Several studies have linked nursing care delivery models that include only RNs, which eliminate PNs and unregulated care assistants, to better patient outcomes (Aiken et al., 2014; North et al., 2013; Thornblade et al., 2018). Although these studies suggest higher levels of RN staffing mean better care for patients, these studies only consider select patient outcomes (e.g., patient death rates) or are based on patients’ own perceptions (Aiken et al., 2012). Importantly, select patient outcomes (e.g., patient death rates) do not represent everything there is to know about what is going on in nursing and in-patient care; and patients’ own perceptions do not easily accommodate aspects beyond interpersonal relationships and a patient’s experience of receiving care (see for example Rankin & Campbell, 2009).
Method
D. Smith’s (1987, 1990, 2005) IE was used to explicate how different categories of nursing professionals worked together after the implementation of the ONTRACC model. Smith (2005) describes IE as a way to look at the puzzles of everyday life and to study people’s actual experiences as they are for them (p. 1). Institutional ethnographers are particularly interested in how people’s everyday activities are socially organized in a particular way as they go about the routine activities of their daily lives. IE was an appropriate choice for this project because it allowed the researchers to explore what is actually happening, from the standpoint of frontline nursing professionals completing their daily work.
Institutional ethnographers begin from the standpoint of people living their everyday lives rather than from within established discourses that are aligned with society’s ruling institutions (Grahame, 1998). Although D. Smith’s (1987) IE approach begins “locally,” in this study, from the standpoint of, RNs and PNs, it maps out “translocally” to consider the work of other people elsewhere (Campbell & Gregor, 2002). Consequently, institutional ethnographers often begin collecting data in a “local” setting (e.g., a hospital unit) through observations and interviews. They often use texts to see how something maps out “translocally.” D. Smith (1987) recognizes how society is text-based and the activation of institutional texts, including government, regulatory, union, and health authority documents mediate people’s work and influence their understandings of their experiences. Nursing professionals activate texts when they use vital documents, such as clinical pathways, checklists, flowsheets, and graphics, to guide their care activities for patients who are recovering from different procedures. They also activate texts when they unconsciously adopt the terms used in these documents to talk to and document about their patients. Texts play an integral role in the social organization of nursing professionals’ activities on any given shift, and they provide clues regarding the way these activities interface with structures of power on their units and beyond. For example, when a charge nurse writes a PN’s name under a RN’s name on a unit’s nursing assignment white board, that PN knows they will need to coordinate all their patient care activities with that RN. When viewed in this way, the nursing assignment white board is a text that maintains a certain hierarchy, whether or not the PN, RN, or charge nurse perceive it that way. In IE, the term “ruling” describes the socially organized hierarchies that shape people’s lives; and texts are usually involved in ruling (Campbell & Gregor, 2002, p. 32).
Ethical Considerations
The authors obtained ethical approval from both Horizon Health Network’s (2018-2578) and the University of New Brunswick’s (008-2018) Research Ethics Boards (REBs) before starting recruitment for the study. All informants, both standpoint and secondary, were sent the consent form after they indicated their interest in the study. The first author could not guarantee absolute confidentiality, as the shadow shifts took place openly. However, she could assure that all interviews would be confidential and that any informant could withdraw from the study at any time. Data was encrypted and stored on a password protected laptop in a locked office. It will be stored for 7 years, then deleted. This study was partially funded through a New Brunswick Health Research Foundation (NBHRF) grant.
Context
The two orthopedic units were selected because the patients had similar healthcare needs (similar acuity). Both units had similar numbers of beds, with most of the rooms being semi-private (two bed). There were some isolation rooms (single bed) and several “ward” rooms with four to six beds. Although the ONTRACC model, was introduced to these orthopedics units at a similar time, one unit (Saint John Regional Hospital, [SJRH]) was further along with its implementation plan than the other (Dr. Everett Chalmers Regional Hospital, [DECH]). Consequently, while the standpoint informants on this unit (SJRH) almost always worked in independent assignments, the standpoint informants on the other unit (DECH) still sometimes worked together as “buddies.” In this article, the authors only report on data that was collected from informants who had experience working in independent assignments.
Recruitment
The authors recruited eight frontline RNs and six frontline PNs to be standpoint informants from two orthopedic units at two different hospitals within one provincial health authority. The authors placed flyers around the units and sent out an invitational email to all the nursing professionals employed on the units. All of the frontline RNs and PNs had a minimum of 1 year of experience working on their current unit. Ten secondary informants, who came from various backgrounds, including nurse managers, nursing educators, nursing practice advisors, other allied health professionals, and a patient, were also recruited. Tables 1 and 2 summarize the informants’ (n = 24) demographic information.
Standpoint Informants.
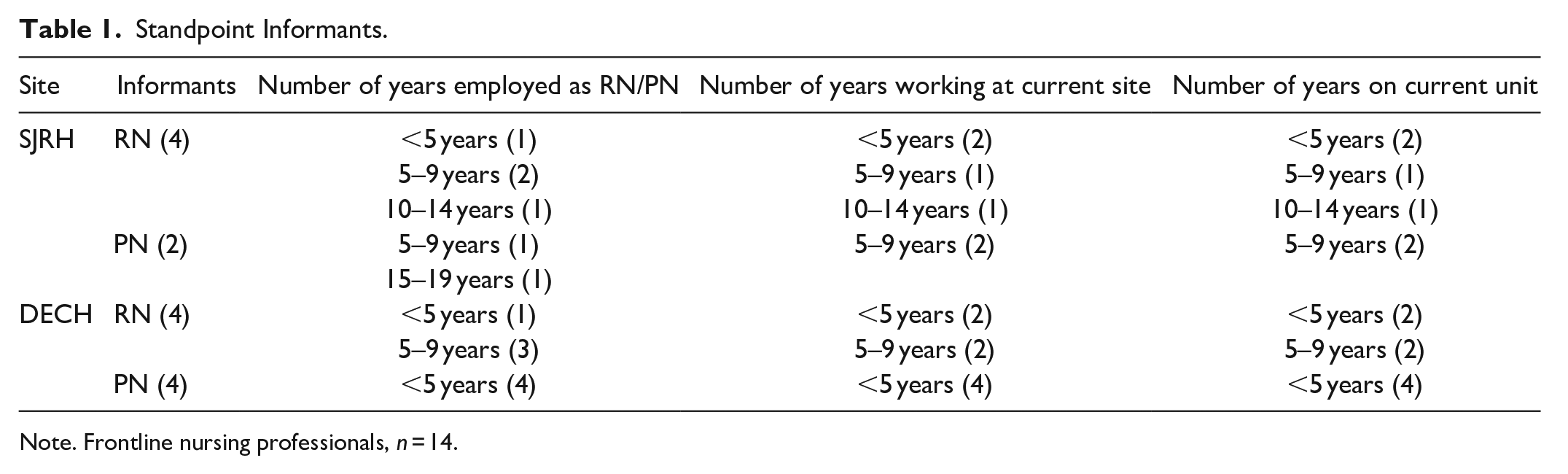
Note. Frontline nursing professionals, n = 14.
Secondary Informants.

Note. Nursing leaders, n = 8, other, n = 2.
RN who previously worked as an PN included in RN group.
Data Collection Methods
Data collection methods included: observing/shadowing standpoint informants, making field notes, conducting interviews, and identifying the texts activated through the standpoint informants’ work (Creswell & Porth, 2017; Deveau, 2008). The first author shadowed each standpoint informant (RN or PN) for a minimum of one 8-hour shift, then completed an individual, semi-structured interview with each of them. The observations made during these shadow shifts enabled the first author to see the realities of the nursing professionals’ work, both together and with their patients. The shadow shifts were done on weekdays and weekends over a 2-month period, depending on the standpoint informants’ schedules. Throughout the shadow shifts, the first author paid particular attention to things like the challenges and tensions the nursing professionals experienced during their shifts. Due to the private nature of some nursing work (e.g., bathing), observations were limited to shared spaces (e.g., the nursing station). The observations were recorded using a field notes template developed by the authors, which focused on the chronology of events on the unit (the unit routines) and included descriptive notes of the nursing professionals’ activities. No personal information was recorded in the field notes. The first author read and re-read these notes after each shift for completeness and added further details when necessary to ensure nothing was missed.
After each shadow shift, the first author interviewed each standpoint informant (the RNs and PNs). Examples of interview questions included: (a) Can you tell me about a typical day at work?; (b) Can you tell me what makes your day run smoothly?; (c) Can you tell me about the challenges you experience in your work?; and (d) When you shared patients’ care with other nursing professionals, how do you decide who does what? The first author also asked questions about things she observed during the shadow shifts, such as, “I saw you doing this today. Can you tell me what was going on?” Probes were used to encourage the standpoint informants to further share their stories and descriptions of their everyday experiences or empirical knowledge of their work. These interviews lasted approximately 30 to 60 minutes and were audio-recorded and transcribed with the informants’ permission. During these interviews, the standpoint informants often suggested the first author contact someone else to learn more about something (e.g., a practice guideline). Consequently, standpoint informant interviews generated a list of secondary informants. These secondary informants were nursing professionals who did not work the frontlines, such as nursing leaders and nurse managers, other allied health professionals, and a patient. These secondary informants were invited to be interviewed through email. Once the secondary informants indicated interest, consent was obtained, and interviews were scheduled. The secondary informants were asked questions that focused more on identifying the ruling that organized the standpoint informants’ work. These interviews also lasted approximately 30 to 60 minutes. With the permission of the secondary informants, these interviews were also audio-recorded and transcribed.
D. Smith (1987) recognizes how society is text-based and the activation of certain, overarching institutional texts, or “boss texts,” mediate people’s work and influence people’s understandings of their experiences. The first author paid attention to any texts used during the observations/shadowing, usually health authority documents, or mentioned during the interviews, usually health authority, regulatory, or union documents. Eventually, a “chain” of texts and work processes (Ng et al., 2013) emerged by attending to the connections that both the standpoint informants and secondary informants revealed through their interviews or work.
Analytic Methods
The focus of data analysis was on explicating how the nursing professionals worked together after the implementation of the ONTRACC model and the social organization of their work. IE has a “distinctive ontological shift” from other qualitative methodologies (Rankin, 2017a, 2017b). Rankin (2017a) cautions institutional ethnographers must resist looking for categories, patterns, or themes in their data, which is a “misstep.” Rather the process of analysis is “rather like grabbing a ball of string, finding a thread, and then pulling it out” (DeVault & McCoy, 2002, p. 755). Data collection and data analysis occur simultaneously during an IE study (Campbell & Gregor, 2002), and the first author immersed herself in the data by examining the field notes and reading/re-reading the interview transcripts. From these data, the first author used the IE concept of “disjucture” (D. Smith, 1987) to identify disconnections between what was supposed to be happening and what was actually happening during the shadow shifts. The authors then imported the interview transcripts into NVivo and used NVivo’s notes and query functions to highlight uses of “authorizing language” (e.g., “collaboration”) or terms and concepts imported from other texts and discourses (Rankin, 2017a) and added comments. The informants’ uses of authorizing language provided clues to how their descriptions of their experiences were embedded in ruling relations.
The authors then used several of Rankin’s (2017a, 2017b) strategies to begin managing and working with the data, particularly “indexing” and “mapping.” The first author used indexing to create a “cross-reference” for linked work processes and texts (Rankin, 2017a). The first author created folders for the authorizing terms (e.g., scopes of practice) the informant frequently used and indexed all data (written descriptions of work processes and texts) related to these terms in the folders. For example, when both the standpoint and secondary informants talked about “collaboration” and “working together,” they frequently talked about nursing scopes of practice, so the first author created a “scopes of practice” folder. Next the first author put quotes from interviews and documents (e.g., practice guidelines) related to scopes of practice in that folder. What was inside the folders then became the ends of the analytic threads the first author followed to untangle how the RNs’ and PNs’ work was organized beyond their units. The first author then used mapping to display what was happening in words and pictures and track ruling relations (Rankin, 2017a). Specifically, the authors’ mapping work included a diagram that plotted out the various texts that organized the RNs’ and PNs’ daily lives. An example of one of these texts is the clinical pathway document that outlined the standardized care plan for all hip arthroplasties. This mapping work showed how the nursing professionals’ work was ruled both locally (e.g., hospital managerial staff) and translocally (e.g., provincial nursing regulatory bodies), and was shaped by many ideologies, including biomedicalism. Biomedicalism is problematic because it constructs patients as medical problems (e.g., a hip fracture) to be solved and suggests these medical problems are their only issues.
Findings
The first author noted a “disjuncture” (D. Smith, 1987) or “disconnection” between the nursing professionals’ own knowledge and experiences of their work together and the “ruling representations” of this work (Ng et al., 2013, p. 54). What stood out during the first author’s shadow shifts was a disconnection between the stated goal of ONTRACC model, to organize nursing work to improve “Accountability,” “Collaboration,” and “Communication,” and how the RNs and PNs were actually working more independently without their “buddy.” The nursing professionals were more individually accountable but spent less time collaborating with each other on their units. This disjuncture became the problematic of this study, or the “puzzle” (D. Smith, 2005, p. 39) that the authors further explored through three specific analytic threads.
In this section of the paper, the authors describe the three analytic threads, which included: (1) keeping things running smoothly through working together, (2) new scopes of practice with “complex” and “predicable” patient assignments, and (3) the work of the charge/resource nurse. In an IE, the findings and discussion are methodologically and theoretically linked (McGibbon et al., 2010). Therefore, the findings section of this article includes both the analytical threads, as well as related discussion regarding the ways the nursing professionals’ work together might be considered in light of the goal of IE. Importantly, although relevant literature is incorporated, the intent is to demonstrate the social organization of nursing professionals’ collaboration rather than to compare it to others’ findings (Campbell & Gregor, 2002; McGibbon et al., 2010; D. Smith, 1987).
Analytic Thread 1: Keeping Things Running Smoothly Through Working Together
The nursing professionals explained how they felt accountable to “[keep] things from going off the rails,” but to do this, they needed to “do more with less.” Such comments reflected discourses of “optimization” and “efficiency.” When the nursing professionals talked about “keeping it together” and being “efficient,” they often described their “routines” or provided chronological accounts of their days. The nursing professionals’ chronological accounts often revealed the tacit knowledge they used to prioritize patient care activities to “[keep] things running smoothly” for everyone. As one PN (DECH) explained, I try to get as many people washed up before breakfast as possible. I find that that’s huge, ‘cause I want them up in the chair for their meals, if I can get them up. The odd time, you know, sometimes you don’t get to them, and you don’t get them up in a chair for breakfast, but you know I try ‘cause then x-ray comes and gets them for recheck x-rays, and then physio comes.
Through this tacit knowledge, this PN knew how their work (e.g., helping patients “up in the chair”) linked to the work of other healthcare workers (e.g., dietary staff). Some of the nursing professionals worried managerial staff and other decision-makers (“higher-ups”) did not understand or value their routines and made changes “willy nilly.” As an RN commented, “They [the higher-ups] don’t know how we make things work here. If they did, they would not always be changing things.” Through such comments, the first author detected tension among the nursing professionals—particularly, when they talked about managerial staff and other decision-makers (i.e., “higher-ups”) who “don’t work the frontlines, don’t know what we do.”
The first author noticed how disruptions to routines (i.e., unexpected situations), such as when the nursing professionals needed to attend to emergent patient needs (e.g., pain) were a source of stress. One PN (SJRH) noted, [Sometimes] I’m just off my game or whatever, and my time management is not the greatest, or sometimes. . . there is more care to this patient, and I don’t get everything I want to get done before . . . breakfast trays come. Then I fall behind.
Several of the nursing professionals talked about how unexpected situations made them “[feel] behind,” or “overwhelmed.” In most interviews, the nursing professionals agreed “teamwork” and “helping each other out” was important to “get things back on track.” However, they also discussed how this could be challenging. With the independent assignments, they did not have anyone formally assigned to help them or who knew their patients’ histories. Consequently, the nursing professionals needed to “grab whatever hands are available.” As one RN (SJRH) explained, “You have to speak up and say I need help, I need you. Can you do this while I do that. . . That’s kind of the [key]. . . the key is to know when to ask for help.”
Some of the nursing professionals confided that asking for help was not always easy. One RN (SJRH) explained, Yeah. So you probably, like, noticed I haven’t really interacted much with the [PNs]. . . I’m not really close with them [the PNs who are working today] at all, like the [PNs] that I [regularly] work with, like for all my shifts, like I’d be more inclined to go, like ask them for help just cause I’m closer with them, I know them more – if that makes sense.
This RN was not working with the PNs they knew and only interacted with a few of the other nursing professionals during the shadow-shift. The word trust was used frequently in many of the interviews, particularly with respect to asking for help. One RN (DECH) explained she preferred working with certain colleagues. This RN (DECH) shared, “I trust [this PN] a hundred percent, [they are] super diligent, I worked with [them] many times.”
The temporospatial nature of nursing care also made it difficult for the nursing professionals to ask for help. The nursing professionals’ work with both each other and their patients was situated both temporally and spatially on their units. Although the nursing professionals were often spatially in proximity to each other (sometimes even in the same room), temporally they were present with their own patients for extended periods of time. This meant that the nursing professionals were frequently unavailable to help each other out when needed. In the interviews, the nurses consistently talked about feeling torn between helping each other out and caring for their own patients. For example, one PN described how she feels frustrated when they ask someone for help and they forget.
So, then I have to kind of go to them again and be like, are you going to do that or I can get somebody else to do it, and then they’ll be like, ‘oh I was going to, I just was doing this’ and then we just you know, so that can kind of get a little frustrating if you try to ask somebody else for a set of hands and then they forget which is perfectly fine ‘cause I’ve done it before too.
Many of the nursing professionals expressed concern that there were simply not enough “bodies” on the unit during each shift.
Mapping Keeping Things Running Smoothly Through Working Together to the System
The nursing professionals’ used their tacit knowledge to develop “routines” to “keep things running smoothly” for everyone on their units. When the nursing professionals described their “routines,” their talk was infused with terms like “optimization” and “efficiency” which carried institutional traces. Sometimes when the nursing professionals fell behind, they felt like they “weren’t efficient enough.” Many of the nursing professionals also indicated how they felt their routines and other personal strategies to be efficient were undervalued by “higher-ups.” Changes implemented by the “higher-ups,” like the ONTRACC model, seemed to be viewed suspiciously, but generally accepted.
The nursing professionals’ use of the term “higher-ups” demarcated how the nursing professionals’ knew their knowledge of their “routine” and what kept things running smoothly was located below the managerial staff’s knowledge of what would work better. Foucault (1970, 1988) and many other postmodern philosophers (e.g., Baudrillard, 1994, 2001) argue that knowledge is always positioned, attending to the power relations at play in the processes of knowledge production. As Rankin and Campbell (2009) note managerial knowledge, often overrides whatever else is known and can reach “into the heads of [nursing professionals] who learn to reinterpret their own professional judgement and action in its own light.” As such, the “higher-ups’” knowledge overrode the nursing professionals’ knowledge of their own work as they changed their longstanding routines, to make the ONTRACC model work.
When the nursing professional’s routines were disrupted, they used “teamwork” and “helping each other out” to “get things back on track.” The first author frequently observed many of the nursing professionals’ work processes grind to a halt when other staff members were unavailable when needed. For example, many patients required the assistance of two nursing professionals to safely ambulate to the bathroom. If a patient who was a “two-person assist” rang their call bell to go the bathroom, the nursing professional assigned to this patient needed to wait until someone else was available to help to complete this work process. As McGibbon et al. (2010) notes, “hospital work processes depend materially and conceptually on nurses engaging in the work of others” (p. 1369). Although authorized, or managerial, explanations of the ONTRACC model emphasized how it would “enhance and improve the process of collaboration and effective decision-making in clinical settings” (HHN, 2018a, p. 13), the nursing professionals were more individually accountable. With the independent assignments, the nursing professionals were no longer formally assigned a “buddy” who knew their patients’ histories and was responsible for “pitching in” and “picking-up the slack.” Instead, the nursing professionals needed to find someone who was not busy with their own patients.
The first author observed the nursing professionals preferred to approach nursing staff members (either RN or PN) who they knew well and “trusted” for help. Unfortunately, the implementation of the ONTRACC model coincided with rotation changes which meant the nursing professionals were no longer working with the same group of staff, who either followed or partially followed the same rotating shift schedules. As one RN (DECH) explained, So our rotation, before, . . .you would have your, your full partner and you would have half partners with you, but now we’ve changed that you’re not going to have a full partner, so. . . So you’re going to be working with everyone.
Many of the nursing professionals expressed unhappiness over their changed rotations and worried their units would lose “that family feel.”
The nursing professionals talked about there never being “enough hands.” Most of the nursing professionals were assigned three or five patients each, with one RN noting being assigned three patients as a “very, very good day.” As McGibbon et al. (2010) have noted, temporally, nursing professionals are present with their patients for extended periods of time. The nursing professionals frequently reported it was difficult to find someone who was not “tied-up” with their own patients to help them when needed. According to a Canada-wide study conducted by Singer et al. (2016), the nursing units in hospitals with the highest nursing staff-to-patient ratios are intensive care units, with an average of one patient per nursing staff member. The nursing units in hospitals with the lowest nursing staff-to-patient ratios are long-term care units, with an average of six patients per nursing staff member (Singer et al., 2016). Surgical units are in the middle with an average of three patients per nursing staff member (Singer et al., 2016).
Within the provincial health authority, there are no mandatory minimum staffing ratios for RNs and PNs. The separate unions that represent RNs and PNs drew attention to the issue of minimum staffing ratios during the 2018 provincial election, where they recommended these minimum ratios to party candidates (NANB & NBNU, 2018). No action to mandate minimum staffing ratios has yet been taken, however, by the elected conservative government. Importantly, minimum staffing ratios consider number of “bodies” working, but do not consider other key factors that contribute to nursing professionals’ workload and patients’ safety, such as having a mix of senior and novice nursing staff working alongside each other to ensure less experienced nursing staff are adequately supported (McLeod & Collins, 2021). Although most of the patients on the orthopedic unit had somewhat predictable care needs, their care often required two staff members (e.g., “two-person assist” to ambulate to the bathroom) and emergent patient needs (e.g., pain) frequently arose. Although some nursing professionals liked working more individually, and felt there was less “duplication” of care, others missed working with “buddy” who they knew “had their back.”
Analytic Thread 2: New Scopes of Practice With “Complex” or “Predictable” Patient Assignments
One nursing leader (RN), a project coordinator, noted that the purpose of the new ONTRACC model was to “[look] at patient care through a new lens and [to see] how autonomy and working to the full scope of practice would be beneficial both, you know, for patients, your organization and employees.” The term “full scope of practice” was frequently used in many interviews, particularly when the nursing professionals talked about the types of patients they were “allowed to care for.” When asked to describe their scopes of practice, the nursing professionals frequently used the biomedical language of chronicity and acuity. For example, one PN (SJRH) explained the PN scope of practice, in terms of the patients they were routinely assigned.
So many of our patients, as [PNs], they’re chronics, so they’re stable. . . [During shifts,] they usually sleep, were incontinent, went to the bathroom. . . that kind of thing. Maybe they’re medicated for pain; that usually seems to be the norm; usually, sometimes they’re fine, they sleep, they’re good. . . [S]ometimes there’s other issues, but if there is a lot of other issues . . . then sometimes that person will end up going to an RN anyway.
This PN (SJRH) used the biomedical language of “chronics” and “stable” to categorize these patients. During the shadow shift, however, the first author noted that many of the PNs’ patients also had complex care needs. For example, many of the PNs’ patients experienced serious psychosocial challenges, including: homelessness, substance use disorders, and social isolation/loneliness.
These categories (“complex” vs. “stable/predictable”) created tensions and frustrations, particularly when the authorizing explanations of these categories were at odds with the nursing professionals’ knowledge of their own competence or holistic knowledge of patient care. As an RN (SJRH) noted, [The PNs] don’t feel competent enough at times anymore because, when you were buddied, you would have, they would be with you with the post-op, so you may do like the initial assessment, but then they would go and do the hourly checks on them ‘cause you would be busy doing something else, right. Where now, they never get a post-op, and I think that they do not like that, just in the fact they don’t feel like they’re being treated as if they’re not competent when they’re more than competent enough to do it. It’s just that’s how it’s been, like the RNs, that’s just, we were told that’s how it’s going to be, and you know what I mean.
As this RN explains, post-operative (post-op) patients were nearly always assigned to the RNs when before the PNs worked with the RNs to care for these patients. Some PNs expressed frustration with how certain types of patients were always “complex” and consistently assigned to RNs. One PN (SJRH) described how they “miss[ed]” being involved in the care of “complex” patients.
But I miss the, the, receiving the patient from the OR - you know, doing that kind of stuff, working with the IVs and like, you know, accepting them as up to the floor with the RN. . . But other than that, there’s really, I’m pretty much working to my full scope. I feel like that’s the only thing I really miss is just kind of working with that fresh, like the fresh post-op patient.
This PN later explained how they were sometimes assigned to care for patients prior to minor, same-day procedures, such as a kidney stone removal, but these patients were usually reassigned to an RN when they returned to the unit post-operatively. Although this PN explained how they understood” the line needs to be drawn somewhere,” they found it challenging when they could do many of the tasks required to care for post-operative patients and had previously been involved in their care. This PN felt they could safely care for certain post-op patients and found the re-assigning of patients post-operatively was “disruptive to everyone, patients and us. Makes it hard to get to know people.” The regular re-assignment of patients also went against what the nursing professionals knew about quality patient care.
Mapping Scopes of Practice to the System
While this IE began “locally,” from the standpoint of nursing professionals, the authors mapped out “translocally” to consider the influence of the work of other people through relevant institutional texts (Campbell & Gregor, 2002). The nursing professionals’ understanding of their “scopes of practice” and “whom they were allowed to care for” was embedded in biomedical discourses (e.g., “chronics”). The biomedical language of patient acuity (e.g., “stable/predicable”) was also used in practice guides and policies to categorize RN patients and PN patients. For example, a practice guide co-written by the Nurses Association of New Brunswick and the Association of New Brunswick Licensed Practical Nurses (Nurses Association of New Brunswick and Association of New Brunswick Licensed Practical Nurses, 2015) stated, “RNs, because of their greater depth and breadth of foundational knowledge, care for patients with more complex care needs and less predictable outcomes” (p. 7). Similarly, a health authority policy stated, “[f]or patients who are less predictable and more complex, more RN intervention will be needed; for patients who are more predictable and less complex, PNs may practice more independently.” (HHN, 2018a, p. 13). This categorization of patients by biomedical level of acuity devalues any patients’ needs that are not physical, but as important, such as psychosocial concerns (e.g., homelessness).
Several authors (e.g., Kelly et al., 2022) have questioned how biomedical knowledge takes priority and undermines nursing professionals’ own knowledge of their patients. Kelly et al. (2022) found both biomedical and medical-legal ruling discourses infiltrated the documents nursing professionals are required to use to “treat” their patients. On both orthopedic units, most of the post-operative patients were recovering from scheduled hip or knee replacement surgeries and were usually discharged a few days later. The care activities of these patients were guided by standardized “care paths” forms. These forms coordinated the care of these patients, with checklists of sequenced “desired outcomes,” such as “up in chair” on the day of surgery and “ambulate three times” on post-op day two (Horizon Health Network [HHN], 2018b). Although the PNs’ patients were “[l]ess complex, more predictable, low risk for negative outcomes” (NANB & ANBLPN, 2015, p. 15), they frequently had heavy care needs (e.g., frequent toileting), and these care needs were complicated by multiple medical diagnoses, such as diabetes, heart failure, Alzheimer’s disease, and dementia. They were often admitted for more extended stays and had challenging psychosocial needs (e.g., homelessness). Standardized “care paths” did not guide their care. In this respect, some of the “chronic” patients would benefit more from the “enhance[ed] RN role and . . . the elevat[ed] expectation around leading care teams, coordinating patient care and developing nursing care plans” (NANB & ANBLPN, 2015, p. 15).
During interviews, the nursing professionals were sometimes uneasy with their “full” scopes of practice and the boundaries of their roles, which made each unit’s hierarchy somewhat ambiguous. The following is description of the PN role: The [PN] works collaboratively with the [RN] to “provide nursing services within the continuum of care that acknowledges the separate and overlapping roles.”(RN/[PN] Collaborative practice). The [PN] provides care under the direction of an RN or a qualified medical practitioner (as described in the [PN] Act). . . [PNs] provide nursing care under the direction and in collaboration with an [RN] or Medical Practitioner, or Pharmacist, for custodial convalescent, sub-acutely ill, chronically ill, and assists the [RN] in the care of acute ill patients. (NANB & ANBLPN, 2015, pp. 15–16).
There is a clear disjuncture between the textual presentation of this PNs’ work in their role description and their everyday reality. The choices of language in this description reflect a view that PNs are not independent thinkers like the RNs. The PNs, however, were assigned to their own patients and did not actually “provide nursing care under the direction” of the RNs. The ONTRACC model increased accountability and responsibility of the PNs without a concomitant increase in professional recognition or renumeration.
Analytic Thread 3: Work of the Charge or Resource Nurse
The charge nurses (SJRH) and resource nurses (DECH) were the only healthcare staff members who received a report on every patient’s information at the start of each shift. Their shift reports included details of the collective knowledge around the patients’ care needs, including details about medical orders, physiotherapy, radiology reports, and discharge plans. As such, the ONTRACC model placed heavy responsibilities on the charge/resource nurses. These responsibilities positioned the charge/resource nurses as “vessels of knowledge” who monitored the statuses of all the patients and sometimes took on the overflow work of the other healthcare staff on the unit. Taking on the overflow work of other healthcare staff frequently happened in emergent or urgent situations (e.g., when a patient fell). In these situations, the first author observed the charge/resource nurses call physicians to negotiate new medical orders and then help carry out the new orders. As charge/resource nurse explained, Yeah, I’m more or less putting out small fires. If something’s going on, then I’m the one calling the doctor to say, this is going on, what, what do you want me to do about this. . . so if anything’s going on you’re going in to assess the patient and then you’re calling the doctor to find out what they want done or if they need to come up and see them.
Sometimes, if the unit was short-staffed, particularly on evening or nightshifts, the charge/resource nurses had their own patient assignments on top of their resource/charge duties. The charge/resource nurses used terms like “monitoring,” “watching,” “overseeing,” and “coordinating” to describe their roles. In many ways, the charge resource nurses were responsible for making sure the work of the unit went forward.
The ONTRACC model caused the other nursing professionals to rely more on charge/resource nurses for advice or to answer questions about specific patients’ care needs because they had the most sense of what was happening on the unit. The charge/resource nurses received complete “shift reports” on all the patients. As a holder of some knowledge of every patient, the charge or resource nurse knew from reports, charts, and other records some of what was happening with everyone. As one PN (SJRH) explained, I always go to the charge nurse if I think that there can be a change of some sort.. . . She knows all the patients. So, you know, [the charge nurse] knows what is going on with everyone’s patients. I always go to the charge nurse or [the orthopedic CNS] if, ‘cause there’s both of them there, usually, so if it’s an ortho patient, sometimes I’ll just go to [the orthopedic CNS] instead of the charge nurse because they talk to the surgeons.
It made sense to this PN to go straight to the charge nurse, who had some knowledge of their patients, rather than explain the scenario from scratch to another nursing colleague (RN or PN). Notably, the charge/resource nurses were not directly involved in many of the patients’ assessments or care; and their “knowledge” was a different type of knowledge than the more intimate knowledge the other nursing professionals had with their patients.
One important part of the resource/charge nurses’ work that the first author did not expect involved the creation of “good patient assignments.” As a nurse leader, an educator, explained, “You can’t just assign “the back wall” . . . If the assignment isn’t good, it isn’t going to work. It needs to be the right patient for the right [nursing professional], you know?” One charge/resource nurse explained how the creation of patient assignments was “very important. To avoid the creation of problems later.” As one PN (SJRH) explained, But if someone’s not doing well – then they should be with an RN. Often what they’ll do is they’ll. . . swap out a patient because my patient kind of went down the tubes, so we need to switch it up. But sometimes, if that will even happen, like at 3:30. At 3:30, there’s a new assignment, right? So if a patient wasn’t doing well throughout the day, at 3:30, the charge nurse will put that patient with an RN.
Notably, when the assignments were deemed good, and the nursing professionals felt things “go well.” Bad assignments, however, were a source of frustration and tension among the RNs and PNs. When PN assignments were “bad,” then one or more patients deteriorated, and these patients needed be reassigned to an RN. The RN would then need to quickly “get up to speed” on a patient they did not yet know while attending to the patient’s urgent needs. The RN’s increased workload also likely impacted the care of their other assigned patients, some of whom would be reassigned to the PN. Sometimes, when patients “really went down the tubes” or the RN who took over was inexperienced, the charge/resource nurses would need to oversee the reassigned patients’ care.
Mapping the Work of the Charge or Resource Nurse to the System
The charge/resource nurses were in the stressful position of having to keep track of all patients care needs from hour-to-hour and to use this knowledge to keep the hospital’s work processes moving forward. The charge/resource nurses documented their knowledge on unit worksheets printed from the hospitals’ health information systems. Although these worksheets had some information about each patient (e.g., medical diagnoses) when they were printed, the charge/resource nurses needed to write by hand key information from their shift reports and throughout the day (e.g., discharge plans). Thus, these sheets became running tabulations of the key information known about all the patients, including: diagnostic imaging and laboratory results, details about required ambulation/mobility aids, and all surgical procedures done. The charge/resources greatly valued their worksheets and knew they were important to the organizational work of the unit. Despite the importance of these worksheets to the charge/resource nurses organizational work, to respect the confidentiality of patients’ personal health information and follow certain professional, legal, and ethical obligations, these worksheets were shredded the end of each shift. Consequently, all the charge/resource nurses’ knowledge work remained largely undocumented.
In the health authority’s, “Surgery Inpatient Standards,” there are descriptions of all the roles/responsibilities of all the various hospital staff who are involved in surgical patients’ care (HHN, 2016). The first author noted the description of the charge/resource nurses’ “roles and responsibilities” is shorter than any of the other staff members (HHN, 2016). According to this description, the charge/resource nurses:
- Facilitate care coordination and communication among disciplines
- Effectively communicate within the unit and across department/services within the facility
- Facilitate coordination of transfer plans
- Provide resources and consultation to the nursing care team (HHN, 2016, p. 20).
Although, this textual representation of the charge/resource nurses work focuses on “coordination,” “communication,” and “consultation,” it does not reflect how the resource nurses were heavily involved in the work processes of other staff members’ (including the physicians and surgeons). The first author observed the nursing professionals and other hospital staff were particularly reliant on the resource nurses to see what needed to be done and doing it, even if it is not in their job descriptions. Consequently, the charge/resource nurses work has the character of traditional women’s work, in which women “take up the slack to advance a project” without receiving credit (Campbell, 1988, p. 40). Long-term, this may be problematic. McGibbon et al. (2010) found nursing professionals experienced additional stress when they took on the extra work to accommodate their hospital’s work processes.
The description of the charge/resource nurses’ “roles and responsibilities” omitted their important task of making patient assignments, which took up a substantial amount of time. The charge/resource nurses found it difficult to explain how they made patient assignments, they often referred to guidelines that were co-authored by the two provincial nursing regulatory bodies (NANB & ANBLPN, 2015). According to these guidelines (NANB & ANBLPN, 2015): When assessing the [patient’s] needs, consideration must be given to the [patient’s] level of complexity, predictability and risk of negative outcomes: i. Level of Complexity—the degree to which a [patient’s] condition and care needs can be easily identified and the variability of their care requirements. ii. Predicatbility—the extent that a [patient’s] outcome and future care needs can be anticipated. iii. Risk of Negative Outcome—the likelihood that the patient will experience a negative outcome due to their health condition or response to treatment. Both [PNs] (with an established care plan) and RNs can autonomously care for stable [patients] with less complex, predicable and low risk care needs. When the [patient] becomes more complex, less predictable and their risk of a negative outcomes increases, the need for consultation and collaboration increases, The results of the consultation may result in certain aspects of care being transferred to the RN or there may be a need of all aspects of care to be transferred to the RN.
In referring to these guidelines and talking about “level of complexity,” the charge/resource nurses unintentionally activated the dominant biomedical and medical-legal discourses. This is problematic when this powerful discourse overruled the charge/resource nurses’ professional judgment. Interestingly, the charge/resource nurses had difficulty articulating what “level of complexity” meant outside of different types of patients (e.g., post-operative patients) or specific nursing tasks (e.g., administering “high risk” medications). They frequently stated things like, “you know, like fresh post-ops” or “very acute patients.”
While the charge/resource nurses knew it “needs to be the right patient for the right [nursing professional],” they also felt other factors, particularly the spatial proximity of the patients remained important. The charge/resource nurses wrote the nursing professional’s patient assignments on a large white board in front of the nursing station. Three to five bed numbers (not room numbers) were written next to each nursing professional’s name. There was sometimes a disjuncture between the reality of the nursing professionals’ assignments and what was written on the white board. As one RN (DECH) explained, I go into the room [a four-bed room], and I don’t have very much time ‘cause I know I have like so many other things I need to do. So, . . . like I always feel like I’m in a rush and you know apologizing, like I’m sorry like I have to go, or like I’ll be right back, and then when patients like get frustrated about you know the wait or something and like you can, you get where they’re coming from.
This RN also described how if they were only looking after one patient in a four-bed room, they could not “ignore” the other three patients or tell them, “sorry, you are not my patient today.” The first author routinely observed that the nursing professionals took on work outside of their independent assignment of patients. When they entered a four-bed room, they often ended up getting glasses of water for the other patients in the room. Consequently, when a nursing professional was assigned to care for a patient in a four-bed room, their work expanded to accommodate the needs of the other patients in that room.
Reflexivity and Limitations
None of the authors worked for the health authority or in the hospitals at the time of data collection. They were, however, all RNs, and thus reflected own their experiences, assumptions, values and beliefs around nursing professionals working together through various activities (e.g., reflexivity journals and reading/re-reading transcripts). The authors were accustomed to using institutional language, like “collaboration” or “scopes of practice,” which do not provide descriptive accounts of what is actually going on, and needed to train themselves out of this habit. They also needed to remember their standpoint informants were the expert knowers and they needed to learn from them about their experiences. While the authors nursing practice experiences helped them understand some of the data, they worked in academic settings at the time of the study. They also needed to remember their own previous practice areas were different from the orthopedic unit. For example, the first author’s practice experience was intensive care where RNs are assigned only one or two patients who require constant monitoring. Although the first author’s own nursing knowledge helped her understand some of the terms the nursing professionals used (e.g., give report), but the first author needed to regularly ask what these terms meant to these nursing professionals on their units.
There were some limitations to this study, which may have led to some underdeveloped or missing threads. Due to the private nature of some nursing work, observations were limited to shared spaces, such as the nursing stations, storage areas, and the medication rooms. They did not include observing any private care, like bathing or toileting. The authors may have also missed some insights by limiting their data collection to the two orthopedic units. While the RN or PN title does not change, RNs and PNs experience differences in their work depending on their workplaces. MacKinnon et al. (2018) argue that readers of IEs need to consider the context of studies to determine the transferability of the findings themselves. The RN and PN standpoint informants worked in a specific context, and their experiences may not represent all other RNs and PNs. The data was also collected during a time of change when the RNs and PNs were adjusting to the ONTRACC model.
Implications and Conclusion
It is widely accepted the nursing professionals, such as RNs and PNs, need to “collaborate” or work together to provide patient care. How this “collaboration” is conceptualized in the literature varies (e.g., workforce “optimization”), but conceptualizations are often notably aligned with ruling institutions’ established discourses (Grahame, 1998). As a result, these conceptualizations often lack exploration into the contextual (e.g., patient complexity) and sociopolitical factors which define the environments in which nursing professionals’ work. Researchers who explore nursing professionals’ “collaboration” can easily become confined by established discourses (e.g., biomedicalism) because these discourses are readily available to them. This phenomenon has serious consequences for frontline nursing professionals because their everyday experiences may not be represented or accounted for in these discourses (McGibbons et al., 2010).
This qualitative study, guided by IE, began from the standpoint of frontline nursing professionals (both RNs and PNs) after the implementation of a new nursing care delivery model, the ONTRACC model, on two orthopedic units. Thus, the authors attended to the nursing professionals’ location at the “line of fault” (D. Smith, 1987, p. 53) between their everyday experiences and managerial (i.e., “ruling”) priorities that the ONTRACC model introduced. Managerial (i.e., “authorized”) explanations of the ONTRACC model emphasized how it would “enhance and improve the process of collaboration” (HHN, 2018a, p. 13). However, the first author observed the model actually organized the nursing professionals to work more in isolation (through independent assignments). As a result, the nursing professionals were more individually accountable, but less oriented to collaborate with each other. From the observational, interview and textual data collected, the authors identified three analytic threads: (1) keeping things running smoothly through working together, (2) new scopes of practice with “complex” and “predicable” patient assignments, and (3) the work of the charge/resource nurse. Through these analytic threads, the authors found important gaps in the established discourses on nursing professionals’ “collaboration.”
One of the most startling gaps in the established discourses is the lack of accounting for the value of nursing professionals’ tacit knowledge of their units and the “routines” which they use “to keep things running smoothly.” Also, few established discourses account for the challenges associated nursing professionals’ necessary presence at their own patients’ bedsides, which limits their availability to “help each other out,” causing frustration for everyone. These deficits are remarkable given how frequently the nursing professionals mentioned them during the shadow-shifts and interviews. How the nursing professionals know their patients (e.g., “stable” vs. “complex”) is also a much-neglected area of study. This gap is jarring given how the biomedical model was used to inform the creation of patient assignments and other staffing decisions despite its insufficiency to describe patients’ individual care needs. Finally, the work of charge/resources nurses, particularly their taking on the overflow work of other healthcare workers is largely absent. This overflow work will not be seen as problematic until it is focused on by an analytic lens. As the findings of this study suggest, there is an assumption that nursing professionals will “do more with less” and “pick up the slack.” This will continue to happen until, as McGibbon et al. (2010) argues, unaccounted for nursing work is made visible.
This research may have implications for how nursing leaders implement nursing care delivery models in other settings. Many of the texts discussed in this article exist beyond the RNs and PNs’ units and may have relevance to other contexts. Additionally, many of the sociopolitical concepts (e.g., gender) that were relevant to this study have a presence in nurses’ everyday practice experiences everywhere. Butcher et al. (2018) argue, however, that readers of IEs need to consider the context of studies to determine the transferability of the findings themselves. The RNs’ and PNs’ standpoint informants worked in a specific context, and their experiences may not be representative of other RNs and PNs in other healthcare settings. The implementation of the ONTRACC model is likely different on units where unexpected or emergency patient needs frequently arise. On such units, there may likely more frequent re-assignments of patients, which would subordinate holistic standards of nursing care futher. The experiences of nursing professionals working together in other contexts (e.g., the emergency department) is a recommended direction for future research.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding to partially support the research of this article from the New Brunswick Health Research Foundation.