
Abstract
American institutions of nursing education have integrated cultural competence as a pillar approach to addressing health disparities. The theoretical frameworks, priorities, and solutions that national organizations pursue and endorse have far-reaching implications. The American Association of Colleges of Nursing (AACN) is one such organization. The purpose of this project was to critically analyze the AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses to excavate dynamics related to language, power, and inequality. Findings of this critical discourse analysis indicate: (1) the centrality of the AACN’s assumed authority and lack of relationality with readers, (2) nursing insularity and narrow theorization of culture and power, and (3) the harm of whiteness and colonialism as pedagogy. Accountability and repair include transparency, taking note of resources and viewpoints available and endorsed on organization websites, and updating (or refuting) outdated and harmful approaches.
Keywords
Introduction
According to the International Council of Nursing (2012), nurses are to “promote an environment in which the human rights, values, customs, and spiritual beliefs of the individual, family, and community are respected” and to advocate “for equity and social justice in resource allocation, access to health care and other social and economic services” (p. 2). Recently, the disproportionate impact of COVID-19 on people of color (Fortuna et al., 2020) heightened awareness of existing health disparities in the United States, and health equity is now included in the National Institute of Nursing Research’s (NINR, 2022) strategic plan. Health equity and other NINR lenses represent a shift away from individualist utilitarian philosophies and toward relational care (Beauchamp & Childress, 2019; Meehan, 2012).
Research on relationality is framed by critical theory, in which each person represents intersections of various socially-constructed identities, including race, ethnicity, gender, class, and others (Dickman, 2022). Philosophically, critical theory assumes that all research and all human actions are political in that they enact values in the world and affect the world around them (P. L. Chinn, 2010). In research, the concept of relationality addresses power and trust relationships between participants and researchers (Hall & Callery, 2001). Critical discourse analysis involves examining how the ways of speaking about things normalizes and privileges some perspective and frames of thinking about things while marginalizing others. Relationality in the context of CDA examine how institutional power helps normalize the dominant perspectives with minimal consideration and marginalized perspectives. Relationality explains how discourse is shaped by social relations of power and hegemonic ideologies (Hoagland, 2007). In the broader context of healthcare, relationality reflects self-inquiry regarding what is happening, what one is avoiding, and how one can relate more fully in complex realities (Doane, 2016). The AACN, with its assumed authority in nursing education, exercise power through language choices and messaging that generate consent, transmit ideologies, and convey values.
The American Association of Colleges of Nursing endorses critical theories and critical race theories in The Essentials: Core Competencies for Professional Nursing Education, which defines quality in nursing education and outlines the necessary curriculum content and expected competencies of graduates from baccalaureate nursing programs (American Association of Colleges of Nursing [AACN], 2021). Critical theories and critical race theories in nursing involve examining power relationships between individuals and social structures (K. Crenshaw et al., 1995; Morrow & Brown, 1994). Grounded in sociology, critical theories have existed for decades, but recently various forms of them have come into mainstream discourse among proponents and detractors (McWhorter, 2021; Murray, 2019; Pluckrose & Lindsay, 2020; Sowell, 2019). Due to the focus on power dynamics between individuals and social structures, critical theory is a fitting framework to study the approaches used in nursing to address health inequity.
To frame the study, we chose the specific tradition of critical theory known as emancipatory knowing, defined as “the ability to recognize social and political problems of injustice or inequity, to realize that things could be different, and to identify or participate in social and political change to improve people’s lives” (P. Chinn & Kramer, 2011, p. 64). Emancipatory knowing has been used as a critical approach in nursing scholarship (Fontana, 2004; Peart & MacKinnon, 2018). This project, guided by critical theory/emancipatory knowing, aimed to analyze approaches to health inequity endorsed by the AACN (2023b).
Nurses’ ability to mitigate racism has been brought into question in the literature, and this has been attributed to a focus on cultural competency that tends to depoliticize disparity by ignoring power differentials (Altman et al., 2021; Johnson et al., 2021). The research question was, “What power dynamics exist in the discussion of health inequity in nursing education?” Therefore, the purpose of this article is to critically analyze the American Association of Colleges of Nursing’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses.
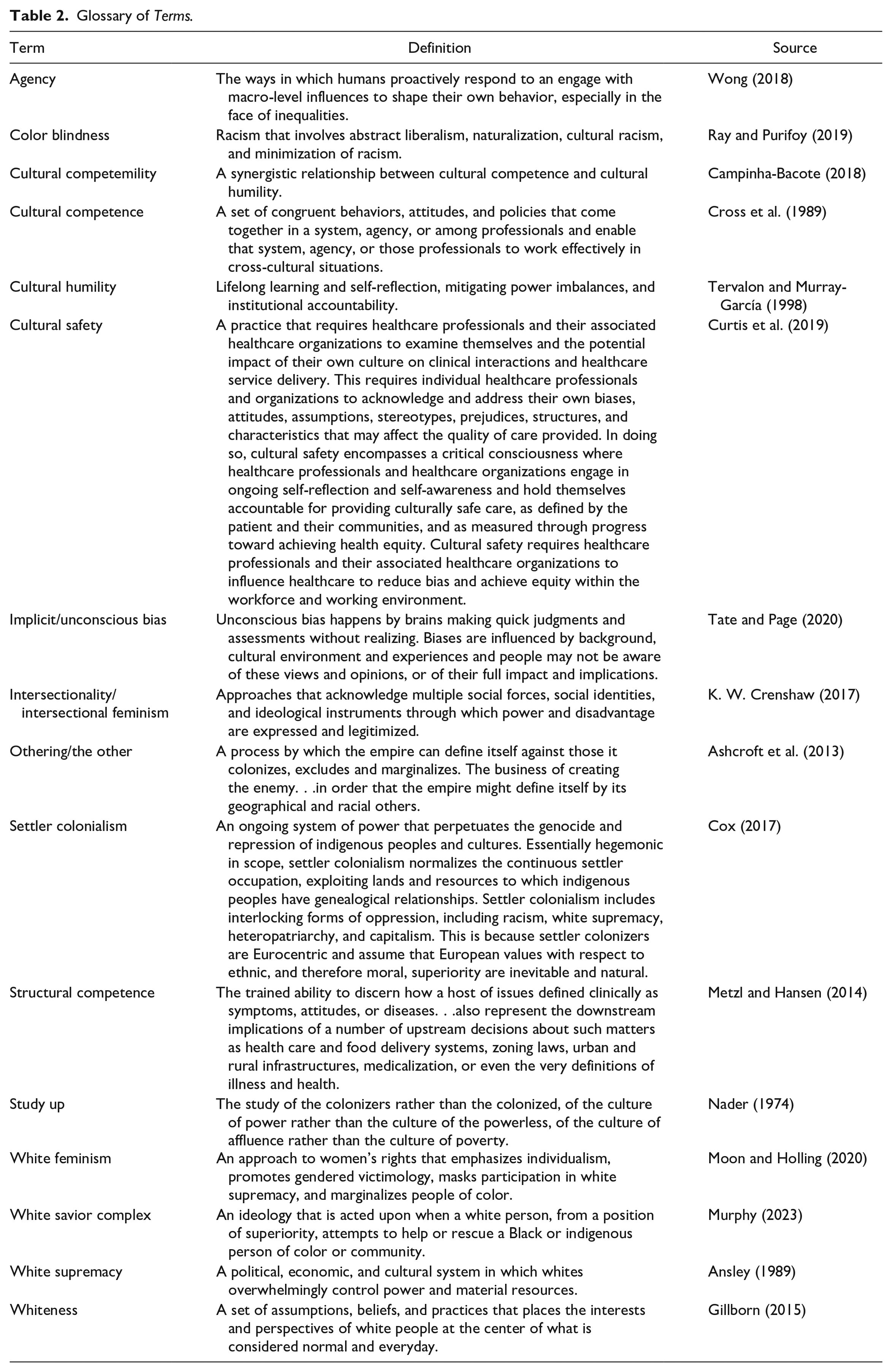
Tool kits are aggregate resources, articles, and other practical information related to a specific topic which became popular in the 1980s. Tool kits are intended to provide an overview of a topic with linked resources to provide more detailed information to inform and change behaviors (Barac et al., 2014). Tool kits are typically developed by subject matter experts who draw on their knowledge, experience, and research to create resources that can help individuals or organizations address specific concerns or challenges. This expertise and investment in developing a tool kit can lend credibility to its content, making it a valuable resource for those seeking to learn more about the topic. The tool kit we analyzed was developed by a committee of national expert educators and clinicians as part of a grant from the California Endowment (Calvillo et al., 2009). While the Tool Kit is not mandatory for educators, the AACN provides it as an online resource for teaching transcultural nursing care. The Tool Kit provides a list of competencies (Table 1), nursing models, reference lists, case studies, websites, and other resources designed to enhance teaching-learning activities. Two authors (KIA & SB) had used the Tool Kit previously in teaching baccalaureate-level nursing courses. For clarity, Table 2 provides the glossary of terms (italicized) used in the paper.
Cultural Competencies in the Tool Kit.

Glossary of Terms.
American Nurses Association and the American Association of Colleges of Nursing
In the introduction section of the Tool Kit, the AACN champions cultural competence—or a set of congruent behaviors, attitudes, and policies for professionals to work in cross-cultural situations—as a solution to health disparities. The notion of cultural competence arose in the 1960s and 1970s amid racial unrest and a call for women’s rights in response to the emerging evidence of what was then called health care disparities (Drevdahl et al., 2008). When viewed through a critical lens, this approach to addressing concerning evidence cannot be separated from the gendered and racialized composition of nursing nor from white feminism, which emphasizes individualism and masks white supremacy.
Historically, national nursing organizations have engaged in systematic exclusion. In 1965, the American Nurses Association (ANA) recommended the baccalaureate degree as minimum preparation for nurses to facilitate professionalization, which resulted in the disenfranchisement of schools of nursing available to those racialized as people of color. While the ANA stated it desired to advance the educational level of nurses, it later acknowledged that not all nurses had access to the new benchmark educational level and were effectively marginalized (American Nurses Association [ANA], 1976; ANA, 2022).
As an entity separate from the ANA, the AACN establishes quality standards for nursing education and enforces those standards through its accreditation arm, the Commission on Collegiate Nursing Education (CCNE). Only baccalaureate and graduate nursing programs in the United States are allowed to become AACN members and submit manuscripts to the Journal of Professional Nursing, the association’s journal. The AACN/CCNE does not provide support or accreditation to associate-degree-level nursing programs for registered nursing or licensed practical nursing, which excludes nearly half of new-graduate nurses (Campaign for Action, 2022). When viewed through a critical lens, the histories and positions of the ANA and AACN/CCNE both affect nursing today.
In the United States, white women actively investing in whiteness, or the assumption of white people’s perspectives as normal, have historically dominated the profession of nursing (Applebaum, 2016). For example, from 1916 until 1964, the ANA purposefully and systematically excluded Black nurses (ANA, 2022). The composition of the nursing workforce does not reflect the overall US population. For example, in 2020, the proportion of the US population identifying as white non-Hispanic was 57.8%, which had decreased from 63.7% in 2010; whereas, about 80% of US nurses identified as white and 17% identify as People of color or other (AACN, 2023a; Jensen et al., 2020). The composition of the nursing workforce remained unchanged between 2013 and 2020 (AACN, 2023a; Budden et al., 2013). It is important to note that demographics do not merely capture descriptive statistics of social structures; they signal legacies of epistemological hierarchy and silencing of peoples and their ways of knowing (de Sousa, 2015). Given the historical context of nursing in the U. S., we chose a critical lens to analyze the Tool Kit.
Literature
We searched the literature related to approaches to studying health disparities. Using the search terms “cultural competence,” “nursing,” and “emancipatory,” we found the concepts of cultural competence, cultural humility and competemility, emancipatory approaches, settler colonialism, and implicit bias, which are discussed in the following subsections. We then used these concepts to inform our coding schema.
Cultural Competence: Theories and Concepts
In the literature, we found that cultural competence has undergone a myriad of definitions and theoretical frameworks. While Cross and colleagues used the term in 1989, Dr. Madeleine Leininger had been the first individual to coin this term (Cai, 2016). Leininger (1970) had proposed the anthropological concept of culture in nursing in her book, Nursing and Anthropology: Two Worlds to Blend, and described culturally congruent care, the original term for culturally competent care. Leininger’s theory, Culture Care Diversity and Universality, is featured in the Tool Kit. The various definitions of cultural competence have common elements: Diversity, cross-cultural interactions, self-reflection, importance of cultural knowledge, adapting healthcare behaviors to reflect cultural understanding.
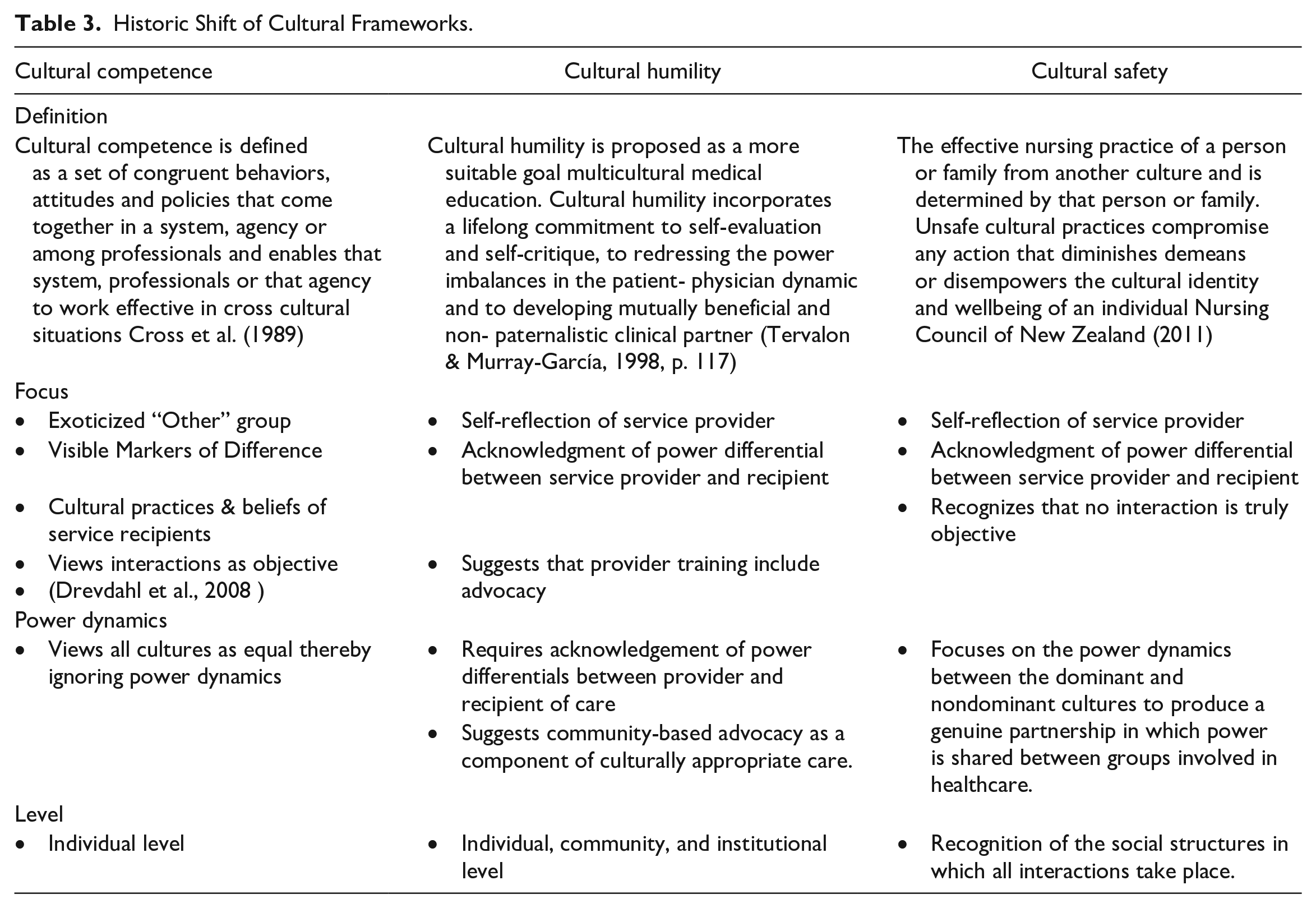
In the literature, we found under-theorization in nursing cultural competence, as evidenced by the exclusion of other academic disciplines and non-U.S.-originated theories. Drevdahl et al. (2008) assert that the calls for cultural competence have been unheeded in nursing, with no accountability, little evidence of effectiveness, and vague and contested definitions (Drevdahl, 2018; Drevdahl et al., 2008). Drevdahl et al. (2008) further contend that the focus on cultural competence turns the lens onto The Other, or the excluded and marginalized; ignores the culture of the service provider; essentializes people; contains static checklists of cultural beliefs and practices; and ignores invisible markers of difference and structural factors, such as poverty and racism, which affect health equity. Wesp et al. (2018) contend that the current approach to cultural competence aids to preserve negative stereotypes and discriminatory behaviors. A review of cultural competence literature conducted in the year 2000, prior to the creation of the Tool Kit, found that cultural competency was not connected to measurable outcomes, that inequities were barely acknowledged, and that interventions to decrease inequities were not explicated (Brach & Fraser, 2000). The notion that anyone could be competent in another’s culture has struck some as arrogant (Curtis et al., 2019). Cultural competence has been theorized at the individual-level framework (Curtis et al., 2019), making it unsuitable for mitigating systems-level concerns. When viewed through a critical lens, the focus on individual-level praxis is consistent with the foundations and mechanisms of colonial projects, which obfuscate examinations of power in favor of efforts that promote notions of neutrality and objectivity (Patel, 2015). Table 3 shows the historic shift from cultural competence toward other frameworks such as cultural humility and cultural safety.
Historic Shift of Cultural Frameworks.
Cultural Humility
Cultural competence has undergone numerous updates through various models and theorizing. For example, in 1998 Tervalon introduced cultural humility, defined as lifelong learning and self-reflection, mitigating power imbalances, and institutional accountability. Then, Campinha-Bacote (2018) coined the term “cultural competemility” as a synergistic relationship between cultural competence and cultural humility. Campinha-Bacote asserts that her biblically-based six-construct cultural competence model forms the foundation for cultural competemility. When viewed through a critical lens, cultural competemility does not address power dynamics in inequitable systems.
Emancipatory Approaches
P. L. Chinn’s (2010) emancipatory knowing in nursing centers on power relations, historical and political contexts, and dynamic social structures of oppression. Wesp et al. (2018) suggest the adoption of a theory-driven emancipatory approach and assert that a focus on cultural competence alone is reductive, promotes color blindness, or minimization of racism; and it ignores intersectionality, or multiple social forces of power and disadvantage.
Reflecting emancipatory knowing, cultural safety and structural competence (Table 4) both seek to address the ways dominant cultural norms and values can lead to the marginalization and oppression of certain groups. Cultural safety involves promoting awareness of the impacts of socio-political and economic issues (Ramsden, 2002) and patients’ rights (Papps & Ramsden, 1996). Structural competence has been developed by medical researchers and anthropologists and slowly being adopted nursing education (Woolsey & Narruhn, 2018, 2020). The theoretical training in structural competence consists of five core competencies: (1) recognizing the structures that shape clinical interactions; (2) developing an extra-clinical language of structure; (3) rearticulating cultural formulations in structural terms; (4) observing and imagining structural interventions; and (5) developing structural humility (Metzl & Hansen, 2014). Structural competence is a framework for understanding and addressing how structural factors such as poverty, racism, and colonialism induce health inequities and contrasts with the former attribution of health inequities to individual behavior, genetics, or cultural factors. Emancipatory approaches offer alternatives to traditional cultural competence.
Emancipatory Approaches: Cultural Safety and Structural Competence.

Settler Colonialism and Implicit Bias
Post-colonialist investigators examine the effects of unequal power on the past and the present, including the effects on social structures such as healthcare (Anderson et al., 2003). For example, Waite and Nardi (2019) describe nursing and nursing education as evolving within the context of American colonialism, and Choy and Brush (2005) describe American nurses as instrumental in manipulating notions of health and setting the stage for widespread labor export. McGibbon et al. (2014) explain some nursing assumptions that support settler colonialism such as the subscription to a paradigm of equality, the belief that colonialism is a thing of the past, and that indigenous people should just get over it. Several authors assert that it is this perceived death of colonialism, much like the post-racial rhetoric of the Obama era, that paradoxically ensures its survival (Bonilla-Silva, 2015; Love & Tosolt, 2010). According to postcolonialist investigators, the practices of justice, including transparency and accountability, are not possible, due to the hierarchical nature of the settler colonialist discursive environment.
Historically, colonialism has not been part of nursing’s consciousness or political agenda (McGibbon et al., 2014). McGibbon et al. (2014) argue that nursing itself has been colonized through the imposition of Western values, knowledge, and practices, which have marginalized and devalued other forms of knowledge and ways of being. They assert that decolonizing nursing requires a shift away from Eurocentric perspectives and an embrace of diverse ways of knowing and being. This can be accomplished by recognizing the role of colonialism in shaping nursing education and practice, challenging dominant narratives, and promoting critical reflection and action.
Liboiron (2021) invites interrogation of assumed access and entitlement to land, including the pursuit of colonial goals on stolen land, as central to settler colonialism. Student nurses are socialized within this racially hierarchical system, while people of color and sexual minority groups experience poor health outcomes (K. C. Iheduru-Anderson & Wahi, 2020).
According to K. Crenshaw et al. (1995), both implicit and explicit biases and discrimination stem from living in a society where racism is deeply embedded, such as in settler colonialist societies. The emphasis on implicit bias, or unconscious bias, implicates the individual, not structures, and reduces the phenomenon of racism to categorization of people (Tate & Page, 2020). K. Iheduru-Anderson et al. (2021) challenges nursing’s silence on racism and the assumed ignorance of many nursing faculty due to their assume or assigned racial identity. Racism ignorance is a part of white racial identity that may contribute to its exclusion in nursing discourse and the widespread embrace of implicit bias and cultural competency instead of anti-racism and other emancipatory approaches.
The literature supports that cultural competence is not sufficient on its own, and that a theory-driven emancipatory approach that seeks to challenge power dynamics in cultural interactions is necessary to promote health equity. We used the findings from the literature on cultural competence, cultural safety, structural competence, settler colonialism, and implicit bias, as well as our dialog, to critically analyze the discourse of the Tool Kit.
Methods
Critical Discourse Analysis
The specific method we used was critical discourse analysis (CDA), a qualitative analytic approach rooted in constructivist ontology that focuses on how discursive structures constitute social practice, thus both manifesting and shaping power (van Dijk, 1993; Van Dijk, 2007). Critical discourse analysis “is a theoretical and analytic approach that recognizes discourse as a form of social practice. Discourse reflects and creates dynamics of power, dominance, resistance, and social inequality” (Valderama-Wallace, 2017, p. 363). This qualitative method is derived from linguistics and is used in the postmodern turn, in a variety of disciplines for a variety of purposes (Wodak, 2001). The purpose of CDA is to illuminate implicit power dynamics by examining discursive strategies. Given the institutional power claimed by the AACN throughout the national landscape of nursing education, this critical qualitative method allows for an examination of their interests and priorities. Ethics approval was not required for this review.
Data Analysis
Similar to Valderama-Wallace (2017), we analyzed the entirety of the Tool Kit for the following: (1) specific words, phrases, and concepts related to racism and root causes; (2) the structure, headers, and order of the tool kit and the overall tone and verb tense; (3) use of discursive structures and the presence of agency; (4) hidden and implied ideas and stances; and (5) power and connection to broader social contexts. As such, this analytical method shed light on how the AACN and this tool kit might perpetuate various forms of inequality and oppression.
We met monthly online from April 2022 to April 2023 to analyze the data and discuss our interpretations. All the authors engaged in analysis between meetings, discussed our findings and degree to which we agreed during our meetings, and also wrote the manuscript as we engaged in the analysis. We followed the steps of CDA data analysis outlined by Ziskin (2019). All meetings were recorded for group reference, and SB took notes in each meeting. First, each author read through the material multiple times. Second, each author completed a CDA worksheet (Supplemental File 4) for the Tool Kit, which included macro considerations such as the problem the authors sought to address as well as an examination of authors, endorsers, target audience, medium, and overview of major discursive findings. Then, we met to compare our findings and discussed areas of discrepancy until we reached consensus. Additionally, we considered micro discursive structures including repetition, cohesion, tense, sentence modes, and lexicon.
The worksheet and the meetings were used to create memos and annotations. Fourth, from the findings on the worksheet we created codes and conducted focused coding. Fifth, we created narrative reconstructions from points emerging from Steps 1 and 4.
Consistent with qualitative research methods, we served as both instruments of data collection and of critical analysts. We analyzed the macro and micro discursive structures with a particular focus on the power dynamics and engaged in ongoing dialog to ensure shared analytic findings. All authors were in involved in the analysis, and discrepancies were resolved through dialog and consensus. One author, who has had experience publishing CDA, served as the primary research team member who analyzed micro discursive structures. During the meetings when we focused on analysis and wrote concurrently, this team member presented findings from her analysis, and we discussed them as a group. Despite varying levels of familiarity with CDA, everyone has had experience with critical analysis and there were no analyses that the entire group disagreed on. We then sent the manuscript to an expert in emancipatory knowing and research for review, feedback, and validation of findings and discussion. The expert approved the findings and discussion without suggestions for revision. All authors approved the final version of the manuscript.
Positionality
Consistent with critical approaches and the constructivist ontology underpinning qualitative analysis, positionality in research is the practice of delineating one’s own position in relation to the study, with the implication that the researcher’s position may influence aspects of the study, such as the data collected or the way in which it is interpreted (Qin, 2016). Positionality can be used to denote how and from where nurses construct meanings for themselves relationally and how they act in accordance with these meanings (Rushton, 2023).
Interested in nursing’s role in health inequity, the authors of this article participated in a series of synchronous online discussions called “An Overdue Reckoning on Racism in Nursing” (Nurse Manifest, n.d.). The discussions were structured with the Principles of Reckoning (Canty et al., 2022), where nurses of color shared their experiences, while white nurses focused on listening to them. We conceptualized antiracism as anything that challenges and attempts to dismantle systems of advantages and disadvantages based on white skin color, also known as white supremacy (Canty et al., 2022). In the discussions, themes emerged of nurses experiencing and witnessing racism against nurses and patients alike, including times during nursing school.
We are a diverse group of nurse faculty working in nursing education institutions across the United States (US). We are diverse in terms of racial, ethnic, religious, and class identification as well as place of origin and US geographic location. KIA identifies as a middle-class Black woman of African descent born in Nigeria, with no religious affiliation and currently living in rural Midwest of United States. SB identifies as an upper-middle class white woman who has Presbyterian religious roots and a master’s degree in philosophy and religion with a concentration in women’s studies, and who was born and is residing in the eastern United States. CVD identifies as a middle class daughter of Tagalog and Ilocano immigrants, living in the San Francisco Bay Area with no religious affiliation. RN identifies as the middle class daughter of a Pacific Islander immigrant and white mother, living in Seattle, Washington in United States. What brought us to our current locations has been shaped by ongoing histories of colonialism, as settlers and members of colonized peoples. When we came together for this analysis, we shared written positionality statements with each other; but to be clear, our positionalities have embodied the research questions we ask, how we have approached this project, and our writing. Consistent with critical theory/emancipatory knowing, threads of our scholarly collaboration include collective and critical dialog, reflexivity, writing, and a commitment to structural change for socially just nursing education.
Findings
General Discursive Findings
The three overarching discursive findings that emerged from our analysis of the Tool Kit were: (1) the AACN’s assumed authority, lack of relationality with readers, and ongoing neglect; (2) nursing insularity and narrow theorization of culture and power; and (3) the harm of whiteness and colonialism as pedagogy. Of note, the term “diverse” is used throughout the Tool Kit and seems to refer to people who are not white. The term is vague and implies that some patients cannot speak of their experience, leaving the reader to wonder if this is attributed to a presumed incompetency of patients from diverse backgrounds.
The AACN: Assumed Authority, Lack of Relationality, and Ongoing Neglect
A Google search of the terms “AACN” and “cultural competence” on February 2, 2023, resulted in the Tool Kit as the first item listed. That this 2008 tool kit remained active on the AACN website indicates ongoing support for its content, cited resources, and theoretical underpinnings. The AACN’s neglect of the Tool Kit website is evidenced by lack of updated resources, recent communication, critical reflection of harm perpetuated by previous work, and numerous dead links, comprising nearly half of the links provided (Supplemental Files 1 and 2). In the Tool Kit table titled “Additional Cultural Competency Web Resources,” 54% of the links were dead. Supplemental File 3 is an excerpt of where a review of one of the links leads. The authors and the AACN have not updated the links they provided as resources, nor have they removed nor replaced the Tool Kit. The AACN’s lack of communication about how this document is outdated, and that it espouses narrow and potentially harmful conceptualizations, indicate a failure of the AACN to account for the conscious efforts across various disciplines and social movements to evolve language central to social justice praxis (American Psychological Association [APA], 2019; Gaby & Caren, 2016; McConnell-Ginet, 2020).
The AACN’s detachment from the readers of the Tool Kit, indicated by lack of the authors’ stated positionality, is an embodiment of assumed authority and a neglect of relationality with AACN members and various people impacted by the stances and strategies championed in the report. Further, they do not make their method or process explicit, which is a manifestation of a form of leadership where accountability and transparency are not priorities. The authors state that the work is not meant to be comprehensive; however, this places the onus on nurse educators to teach themselves and engage in trial and error—at the cost of their labor and at the risk of harming their students and patients. The authors’ use of passive language serves to uphold the authors and their writing as infallible, while rendering invisible those engaged in doing. Examples of passive language include: “. . .the key elements considered essential. . .” “It is suggested. . .” (p. 2) “Someone is treated. . .” (p. 3) “Religious rituals may be performed, believing they will assist in restoring health,” “. . .which have been found effective. . .” (p. 9). While the Tool Kit authors encourage readers to seek information in additional resources, this theoretical ambiguity and eclecticism is salient.
Nursing Insularity and Narrow Theorization
Three of the Tool Kit’s competencies (One, Three, and Four) specify the importance of social factors, safety, and social justice; however, much of the Tool Kit focuses on narrow understandings of culture, as evidenced by truncated mentions of economic and social factors. The lexicon of the Tool Kit naturalizes authority and obfuscates explicit examination of power dynamics. According to Fairclough (1985), to naturalize something through language is to make it appear as “natural,” “obvious,” and “right.” The lexicon of the Tool Kit naturalizes authority and obfuscates explicit examination of power dynamics. Some terms we found in our analysis, such as “larger society,” acculturation,” and “majority cultural view,” when examined critically, serve to naturalize the inequitable power dynamics central to settler colonialism by not acknowledging the role of power in social relations.
In addition, definitions of key concepts are absent. For example, while the Tool Kit authors define health disparity and stereotyping, they do not provide definitions for race, equity, competency, social justice, nor cultural competence itself. Next, the authors discretize the report, and by extension nursing, into the following sections: Education, practice, and research. While this is a common approach to organizing nursing reports and initiatives, it is not the only epistemological possibility. Other epistemological possibilities include emancipatory knowing, defined further as “the human capacity to be aware of and critically reflect on the social, cultural and political status quo, and to determine how and why it came to be that way . . . focused on ways to reduce or eliminate inequality or injustice” (P. L. Chinn et al., 2022, p. 4).
The Tool Kit authors’ argument for cultural competence-based strategies to address health disparities focuses on nurse theorists only, thus centering nurses and Eurocentric, colonial lineages of nursing theory, rather than surveying or inviting lessons from an expansive body of epistemological and ontological understandings of culture and health disparities from multiple disciplines and communities (Freire, 1996; Giroux, 1997; Liboiron, 2021; Tuck, 2009). The Tool Kit authors present paths to solutions strictly from the stance that nurses and established nursing education machinery are the only ones of relevance. For example, the Tool Kit authors highlight five nurse-theorized models related to culture, focusing on cultural competence, transcultural nursing, transcultural health care, and health traditions. They offer an overview of each model’s basic premise, key concepts, and assumptions with no mention of possible limitations or areas requiring greater attention. Only one model, Leininger’s Cultural Care Diversity and Universality Theory/Model, actually defines health. In addition to theoretical insularity, the authors advocate for teaching strategies rooted in whiteness and colonialism.
The Harm of Whiteness and Colonialism as Pedagogy and Strategy
Uneven cohesion is evident when the authors abruptly shift from listing models and resources to offering teaching strategies meant to “foster cultural competency” delineated by classroom or clinical settings. This arrangement of ideas by the authors naturalizes the notion that these two settings require different teaching strategies with no evidence to support this. The listed teaching strategies lack theoretical clarity, such as the following example: “Explore student’s own cultural backgrounds; family origin; advantages and disadvantages of belonging to own ethnic/racial group; own biases; prejudices and stereotypes about own group and others; similarities and differences between own group and others” (AACN, 2008, p. 9).
Furthermore, suggesting content and offering strategies without nuanced guidance posits that faculty can select from this buffet with a hegemonic “one size fits all” approach.
Whiteness and colonialism are present in their use of “ethnic/racial group,” as though there is no clear distinction between the two. Present in this one suggestion to “assign students to perform their own cultural self-assessment” (AACN, 2008, p. 9) are the conflation of race and culture, and the false separations and acontextual binaries of advantages and disadvantages as well as similarities and differences.
Additional strategies reflecting whiteness and colonialism serve to reduce culture to food, symbols, cultural healers, and religious leaders (AACN, 2008, p. 9). The theoretical connections between culture, health disparities, and cultural competence are unclear. Whiteness and colonialism are evident in this narrow theorization of culture, compounded by the undertheorization of power and systems of oppression, which leads to the mixing of culture, bias, cultural patterns, and an emphasis on differences. Statements such as “The most effective intervention services should respect and incorporate the practices of the families from cultural and linguistic groups that differ from the mainstream culture” (AACN, 2008, p. 10) normalize whiteness and Eurocentric teachings of nursing and cultural competence which treat those not categorized as white as The Other.
The authors present strategies through imperative sentences, each phrase beginning with a declarative verb, including assign, use, explore, construct, share, discuss, sensitize, understand, conduct, ask, arrange, develop, and critique. The Tool Kit authors do not address the audience directly with guidance about how to identify, plan for, and connect the strategies. Whiteness and colonialism are evident as the Tool Kit authors present acontextual strategies as relevant without guidance about the cultures and environments of the learning settings themselves.
Further, the Tool Kit’s recommendation to “use role play to better understand racism, stereotyping, and cultural conflict,” may perpetuate harm to students and faculty involved unless done so with very specific objectives with appropriately trained facilitators, and clear protocols for addressing harm and promoting repair. This reflects a focus on personally-mediated racism. Further, contradictions about stereotyping are evident: The authors advise the readers to ensure students are able to “understand” and “confront” stereotyping, while the strategies themselves reflect stereotyping by encouraging faculty to “develop cultural congruent nursing care plans for specific cultures,” “develop simulated living experiences” to immerse students in “other life contexts” such as an “LEP patient,” see “patients in poor ethnic urban neighborhoods,” and design “a collaboratively planned meal for a diabetic Hispanic or hypertensive Chinese patient.” While a number of strategies reflect critical stances—including being mindful of religious calendars, engaging in self-reflection, critiquing “health pamphlets, brochures, and other media” for cultural and linguistic competence—most of them essentialize and reduce culture as fixed characteristics. Strategies that do not incorporate structural factors such as colonialism, racism, and classism can perpetuate harm by naturalizing culture and race as biological.
Another contradiction is that Competency Five dictates “Participates in continuous cultural competence development.” That this 2008 tool kit is still present and unrevised on the AACN website in 2023, and thus endorsed by the AACN, demonstrates that continuous learning has not taken place, as evidenced by the absence of more critical theories such as cultural safety, structural competency, queer theory, and antiracism, for example.
The Tool Kit authors recommend interaction with cultural representatives but do not draw attention to potential power dynamics that could perpetuate harm. For example, the authors advocate learning from and using “consultation with cultural experts,” interpreters, “cultural brokers,” and “navigators.” Perhaps the Tool Kit authors do not mean for this consultation to be voyeuristic nor extractive, but the document is missing explication of how schools of nursing might approach, compensate, and support such consultants in their own endeavors. Next, the recommendation to “consider alternative therapies available in specific communities, and arrange field trips to herbal stores, botanicas, bodegas and other ethnic stores, cultural healers, etc.,” suggests that only those classified as non-whites use alternative therapies or herbs in the management of health and wellness. This is a manifestation of othering. Whiteness and colonialism as pedagogy, AACN’s assumed authority, and narrow theorization are all evident as discursive findings from our analysis of the Tool Kit.
Discussion
While critical theories have gained national attention in recent years, nurse theorists have long been identifying problems with cultural competence. For example, Drevdahl et al. (2008) states, Although culturally competent care may be useful for the nurse providing individualized care, we contend that culturally competent practice is most likely not the answer to eliminating health disparities: it is an in-sufficient construct to address the complexities contributing to existing health disparities (p. 22).
From a critical perspective, we see that a myriad of cultural differences makes the idea of cultural competency insufficient; that is, the lack of attention to the roots of marginalization of certain groups makes the elimination of health disparities and inequities unattainable by cultural competence alone.
As the factors and processes that impact health are expansive, nursing and nurses have much to learn from outside of nursing, as well as from silenced peoples from within nursing. The Tool Kit authors, however, consistently write with a declarative tone, assuming an authoritative voice with little acknowledgment of ontological richness from disciplines such as education, sociology, and the humanities. Their selection of models to include in the Tool Kit lacks a critical stance by communicating investment in the narrow epistemological stances of linearity, a focus on concepts over processes, an obfuscation of the role of power dynamics and systems of power, and an emphasis on the biomedical gaze. Leininger’s very attempt to pursue universality is, itself, an essentializing and authoritative approach to the myriad ways of being (AACN, 2008, p. 6). This narrow gaze toward universality, however, is aligned with the assumed authority of the AACN and this tool kit, and a lack of reflexivity sanctioned by claims to expertise and need for auto regulation as a profession. Purnell’s Model of Transcultural Health Care, in particular, reduces the complexities and contexts of health and culture to linear stages with a myopic biomedical focus, and it limits the legibility of culture into a “person’s cultural needs,” as though culture is not a living system of ways of being, doing, and believing but rather factors to view through a deficit framework of needs (AACN, 2008, p. 7).
The Tool Kit authors frame culture itself in such a way that it is only relevant within the context of difference, prejudice, discrimination, provision of health care, and disparities, painting it with a lens focused on difference as harm, difference as negative, and difference as something for health providers to accommodate. The bulk of the teaching strategies presented in the Tool Kit facilitate the othering and positioning of people who are “diverse,” (meaning not white, Christian, cis-gender, and/or heterosexual) into spectacles to observe and capture, with little attention to positionality. The common conflation of culture with race in nursing indicates problematic theorization of culture, race, and racism. The skewed theorization of culture in nursing focuses on advantages and disadvantages, similarities and differences, and sociocultural differences in an effort to attribute health disparities to culture, rather than tending to structural factors and processes (Drevdahl, 2018). There are opportunities for nursing to learn from theorists outside the discipline of nursing, including Yosso’s (2005) Community Cultural Wealth Model, which names six forms of cultural capital that students of color bring to learning environments: familial, social, navigational, resistant, linguistic, and aspirational. There is a wealth of knowledge and epistemological richness that nursing organizations have disregarded.
The Tool Kit authors seem to assume that nurse educators are prepared and competent to integrate the listed strategies in their teachings, which reflects a lack of attention to culturally responsive and trauma-informed pedagogy (Carello & Butler, 2015; K. Iheduru-Anderson & Waite, 2022). Nurse educators may perpetuate harm by employing such strategies while ignoring structural factors such as colonialism, racism, and classism. When a critical stance is not taken, educators ignoring nursing’s role in oppression veer closely to white supremacy and white savior complex.
Attendance to the culture of the dominant, including medicine and nursing, is absent, as if only The Other have culture, thereby making the dominant culture of whiteness the standard. Contrasting with the normalization of whiteness is Giroux’s (1997) border pedagogy, which embraces difference, recognizing that all learners are socially and culturally situated. Giroux’s pedagogy compels learners to function as border crossers, moving across physical, cultural, and social borders (Giroux, 1997). This pedagogical maneuver facilitates the learner’s ability to not only look on the socially constructed Other but also to study up. Additionally, intersectional feminism, which involves recognizing overlapping oppressions, offers an alternative to white feminist approaches. Border crossing, intersectional feminism, and studying up may be the antidotes to normalizing whiteness as pedagogy, and future research should explore these. Further, McGibbon et al. (2014) recommended several strategies to promote decolonization in nursing. They proposed the use of counter-narratives to engage diverse perspectives, engaging in critical reflection and dialog, fostering cultural safety and humility, promoting the integration of Indigenous knowledge and perspectives, and advocating for social justice and equity.
Implications for Practice
AACN brands itself as the voice of professional nursing (AACN, n.d.). Assertions of professionalism are claims to status (Shirley & Padgett, 2006). In contrast, a reflexive practice demonstrates humility, intellectual curiosity, and a commitment to accountability. Professionalism with a lack of reflexivity allows the maintenance of the status quo of racism in nursing, which is protected through emphases on empathy, individualism, homogeneity, and conflict avoidance (Barbee, 1993).
The degree to which an organization is able to engage in reflexive practice is determined in part by the composition of its decision-makers and the degree to which they see themselves as accountable to entire communities. Organizations with diverse decision-makers from a range of backgrounds are better able to engage in reflexive practice, to challenge assumptions and biases, and to consider a wider range of perspectives. In contrast, organizations with homogenous decision-making bodies may be more likely to reinforce existing biases and assumptions because they lack diverse perspectives.
In light of our findings, we present the following queries. First, how does the AACN reconcile their endorsement of critical theories in The Essentials (AACN, 2021) in light of the absence of such theories in the Tool Kit? The presence of the Tool Kit in its current form implies a contradiction and a lack of alignment with the AACN’s overall principles and values. The Tool Kit should be updated to draw on a range of theoretical frameworks and perspectives to make it current and relevant. While The Essentials highlights the need for nurses to understand and address social determinants of health, health disparities, and structural inequities, and emphasizes the importance of cultural humility and sensitivity in providing patient-centered care, the relevant theories are absent from the Tool Kit aimed at helping educators achieve these goals.
Second, will the AACN continue to promote the Tool Kit and, more broadly, promote cultural competence as a remedy to health disparities? If so, this expectation assumes that the culture of a people is static and monolithic, rather than evolutionary. It negates structural factors and varying life experiences of individuals that affect their views of the world, health beliefs, needs and practices. It can also reduce individuals to harmful stereotypical boxes, perpetuating marginalization.
Third, will educators’, scholars’, journal editors’, and peer reviewers’ historical and ongoing investment in epistemic and ontological stances continue to uphold tool kits as useful vehicles for addressing concerns? As living documents, tool kits must be updated for relevancy and reviewed for dead links. This could include adding new sections or resources, removing outdated information, or reorganizing the Tool Kit to promote its continued use and effectiveness.
Structurally, AACN has positioned itself at the apex of nursing education authority, defining academic instructions, practice, skills, and providing guidelines and other essential standards of nursing education that must be adopted by nursing educators nationally. Although readily available, the AACN website is not the go-to resource for associate degree educators whose programs are not accredited by the sister agency CCNE. By representing itself as the highest authority, AACN through the Tool Kit endorses cultural competence as the way to engage culturally diverse individuals and groups safely and equitably. This ongoing investment in cultural competence persists on stolen land, virtually unquestioned by national nursing organizations, eclipsed by good intentions around diversity. Given the vast physical topography of nursing and nursing education, stretching from colleges and universities to clinical sites, the examination of theft of land is needed.
It may seem unimaginable to those who have not suffered from racism that healthcare providers could exhibit discrimination and bias toward healthcare recipients. A recent shift in healthcare to focus on implicit bias as the source of inequities and disparities implicates the individual, not structures, and reduces the phenomenon of racism to categorization of people (Tate & Page, 2020). This shift might also be a form of interest convergence, where those with certain types of power in nursing see that they need to be open to some form of critical work but may hide behind implicit bias, when they could be addressing and discussing structural racism and settler colonialism. Neither cultural competence nor implicit bias is sufficient to address these complex issues.
Conclusion
This critical discourse analysis of the AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses was framed with critical theory/emancipatory knowing. Our findings suggest that the AACN should revisit its provision of resources for nurse educators and incorporate emancipatory approaches for addressing health disparities. As colonialism has been pervasive globally, our findings may hold implications for non-US nursing settings.
Managing knowledge and demarcating what counts as knowledge relevant to nursing reflect epistemic transactions and the social relationships among nurses in assumed positions of leadership (Perron & Rudge, 2015). Given the biomedical foundations of nursing and ongoing efforts to delineate what is distinct about nursing (Perron & Rudge, 2015), we have the opportunity for epistemological reckoning, excavation, expansion, and clarity. The continued presence of the Tool Kit on the AACN website is an endorsement of cultural competence as a way to engage and address the needs of culturally diverse individuals and groups safely and equitably. However, emancipatory approaches are absent. In a profession with 80% representation of those classified as White, power dynamics are reflected implicitly and explicitly through system policies and practices, including those represented in the Tool Kit. In establishing stances and providing resources, a regular review is critical to include theories and models that address the roots of health inequity.
Supplemental Material
sj-jpg-1-gqn-10.1177_23333936231214420 – Supplemental material for A Critical Discourse Analysis of AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses
Supplemental material, sj-jpg-1-gqn-10.1177_23333936231214420 for A Critical Discourse Analysis of AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses by Kechi Iheduru-Anderson, Claire Valderama-Wallace, Sharon E. Bigger and Robin Narruhn in Global Qualitative Nursing Research
Supplemental Material
sj-jpg-2-gqn-10.1177_23333936231214420 – Supplemental material for A Critical Discourse Analysis of AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses
Supplemental material, sj-jpg-2-gqn-10.1177_23333936231214420 for A Critical Discourse Analysis of AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses by Kechi Iheduru-Anderson, Claire Valderama-Wallace, Sharon E. Bigger and Robin Narruhn in Global Qualitative Nursing Research
Supplemental Material
sj-jpg-3-gqn-10.1177_23333936231214420 – Supplemental material for A Critical Discourse Analysis of AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses
Supplemental material, sj-jpg-3-gqn-10.1177_23333936231214420 for A Critical Discourse Analysis of AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses by Kechi Iheduru-Anderson, Claire Valderama-Wallace, Sharon E. Bigger and Robin Narruhn in Global Qualitative Nursing Research
Supplemental Material
sj-pdf-4-gqn-10.1177_23333936231214420 – Supplemental material for A Critical Discourse Analysis of AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses
Supplemental material, sj-pdf-4-gqn-10.1177_23333936231214420 for A Critical Discourse Analysis of AACN’s Tool Kit of Resources for Cultural Competent Education for Baccalaureate Nurses by Kechi Iheduru-Anderson, Claire Valderama-Wallace, Sharon E. Bigger and Robin Narruhn in Global Qualitative Nursing Research
Footnotes
Acknowledgements
The authors wish to extend their gratitude to Dr. Peggy Chin for her invaluable feedback with the review of the manuscript content and connect to critical analysis of documents.
Contributions of authors
1. Conception of the project and inviting others to work together: Bigger, S.
2. Design of the article and the acquisition, analysis, or interpretation of data for the article: Bigger, Sharon, Iheduru-Anderson, Kechi, Narruhn, Robin, Claire Valderama-Wallace.
3. Drafting and revising the manuscript for important intellectual content: Bigger, Sharon, Iheduru-Anderson, Kechi, Narruhn, Robin, Claire Valderama-Wallace.
4. Approved the version to be submitted and published: Bigger, Sharon, Iheduru-Anderson, Kechi, Narruhn, Robin, Claire Valderama-Wallace.
The authors met on a regular schedule to work on the manuscript from inception to the final product. The order of authors was discussed and agreed on by all authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval Statement
Not applicable for this type of research.
Permission to Reproduce Material From Other Sources
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.