
Abstract
Advanced practice registered nurses are successful in improving quality outcomes and filling provider care gaps in long-term care. However, little is known about the nurse’s transition to practice in this setting. A 12-month ethnography was conducted via participant-observation with nine advanced practice registered nurses in five long-term care facilities to understand practice environment influence on the nurses’ transition and on the reciprocal influence of the nurse on the practice environment. Transition was fraught with uncertainty as documented by five themes: where’s my authority, institutional acceptance, personal role fulfillment, provider relationships, and individual versus organizational care. These findings suggest that transition in this setting is complex, characterized by insecurity whether the individual is new to advanced practice or experienced. Transition in long-term care could be strengthened by formal programs that include clinical practice, reconceived mentorship for advanced practice registered nurses, and education designed to improve comfort and expertise with indirect care.
Keywords
As people age into middle and later life, they require more specialized care due to many factors, including comorbidities, additive life course adversities, and disabilities (Bednash et al., 2011). This medical complexity (Mather et al., 2015) calls for increased nursing in long-term care (LTC) settings, which face challenges to nurse staffing as LTC competes for nursing graduates at all educational levels. Advanced practice registered nurses (APRNs) have provided quality care in LTC globally for over 50 years yet most healthcare systems, including LTC, lack formal national training programs for APRNs which may be seen as a barrier to practice (Delamaire & Lafortune, 2010; Ploeg et al., 2013; Rantz et al., 2018). APRNs have asked for further training in all settings, and formal transition programs are positively correlated with nursing retention (Goode et al., 2016). Intentional transition programs are of interest to all global healthcare systems which employ an advanced practice nursing model of care in geriatric LTC systems. In this inductive ethnographic study, we explore the experiences and needs of APRNs in transition to practice (TTP) within the LTC setting.
Background
In the United States (US) nursing homes, APRNs are the most common providers specializing in geriatrics (3.21 APRNs per 1,000 beds vs. 1.37 for physicians), and physicians in geriatrics have shown a population-adjusted decline of filled graduate medical education placements of 23.3% between 2001 and 2018 (Petriceks et al., 2018; Ryskina et al., 2017). All APRNs are trained to care for geriatric populations according to competencies assessed by their respective accrediting bodies (American Association of Colleges of Nursing [AACN], 2016). Evidence shows that APRNs in LTC settings improve patient outcomes as well as staff skills through training and role-modeling (Blackburn et al., 2020; Kane et al., 2003; McAiney et al., 2008; Rantz et al., 2015; Unroe et al., 2015). Nursing homes with APRNS realize cost savings from increased care coordination and communication as well as reduced hospitalizations; in a 3-year study, Medicare expenditures were reduced by −$2,066 per resident (p = .34), a 10.4% reduction, in LTCs where APRN care was embedded with the goal to reduce hospital admissions through continuous provider-level coverage (Rantz et al., 2018; Tappen et al., 2017; Unroe et al., 2015).
Though the advanced practice model of nursing was first defined in the United States, this model has been adopted and adapted in multiple countries in response to increased demand for medical providers, increase in chronic needs of patients and the need for improving quality (Delamaire & Lafortune, 2010). Worldwide, research on these models is beginning to demonstrate efficacy in geriatric care and represent a potential next step in creating effective geriatric and long-term care systems (Berglund et al., 2013; Clark, Parker & Prosser, 2013; Delamaire & Lafortune, 2010; Ono et al., 2015). Despite APRNs’ demonstrated importance, little is known about how to support their transition into the LTC setting. New or graduating APRNs may have little training in LTC, which presents a unique, highly regulated, challenging practice environment. There are no national formalized transition experiences for APRNs in the US partially funded by Centers for Medicare & Medicaid Services as there are for their physician colleagues (Auerbach et al., 2018). Laws regulating APRNs’ practice differ by US state, so that the focus on TTP varies from supervised practice periods under collaboration with a physician to guided independent practice with another APRN. No evidence suggests that these programs are effective, and they add healthcare costs (National Council of State Boards of Nursing [NCSBN], 2014).
Nevertheless, a formal orientation period has been identified as more predictive of successful APRN transition than years of experience as an RN, reducing turnover and increasing APRNs’ confidence in their practice (Barnes, 2015; Cusson & Strange, 2008; Goode et al., 2016). TTP has been widely studied, with well-established formal transition programs for entry-level RNs, but less is known about this process for APRNs (AACN, 2021; Clipper & Cherry, 2015; Duchscher, 2008). There are thousands of accredited RN programs in the U.S., but of the few APRN programs, none focuses on LTC (American Nurses Credentialing Center, n.d.).
APRN TTP is characterized by multiple stages that can occur at different rates and in different ways, requiring adjustment of practitioners and the teams that they join (Chicca & Bindon, 2019; Fitzpatrick & Gripshover, 2016). According to Brown and Olshansky’s (1997) theoretical model, from Limbo to Legitimacy, this process may take as long as a year, during which they reflect on their practice, affirm it through feedback, and gradually assume increased responsibilities. Progression to expanded advanced practice is projected to be turbulent as the APRN experiences liminality, “straddling two identities while not feeling a part of either,” representing a perceived regression in expertise requiring recovery of confidence as well as skills (Brown & Olshansky, 1997). In fact, APRN transition is complex in nature and considered more fraught with liminal aspects than theorized registered nurse (RN) transition, such as the “Novice to Expert” model, creating unique challenges (Benner, 1982; Brown & Olshansky, 1997). With a foundation based in RN education, APRN practice advances from a relatively narrow diagnosis-task centered focus based on comfortable known nursing practices, to include broader, more independent indirect care such as organizational support and quality improvement. The four stages of the Limbo to Legitimacy model, Laying the Foundation, Launching, Meeting the Challenge, and Broadening the Perspective, progress the APRN from initial struggle to form a new identity to the establishment of legitimacy and acceptance of greater responsibility; though the stages are not necessarily uniform or linear (Brown & Olshansky, 1997). Internal and external threats that can alter or delay APRN transition require further study (Brown & Olshansky, 1997; Hill & Sawatzy, 2011). TTP programs to help APRNs advance through the stages of the Limbo to Legitimacy model have shown benefits, yet the ideal structure, content, and length of such programs as well as potential funding sources in LTC have yet to be identified.
Nursing care systems, such as LTC organizations, are complex settings in which small inputs can result in large nonlinear outcomes and vice versa. Complexity science is a fitting sensitizing framework to visualize LTCs as it posits complex adaptive systems (CAS) in which agents come together in a nonlinear, dynamic fashion to organically emerge through self-organization and feedback; the end system is different than the sum of its agent parts. Change agents, or attractors, draw attention, altering the system, either inhibiting or intensifying outputs as components reorganize themselves within the system (Braithwaite et al., 2018; Colón-Emeric et al., 2016; Turner & Baker, 2019). The individual APRN can be envisioned as representing a CAS with nursing knowledge and actions, personality, experience, and education, embedded within a larger CAS, the LTC (Figure 1; Benham-Hutchins & Clancy, 2010).

Theoretical model of APRN transition as embedded CAS.
As APRNs learn and understand themselves within their symbolic healthcare world, nonlinear and nonrational transformation occurs through their interpretations and understanding. The LTC organization is itself a CAS, within which the APRN CAS is embedded, acting as and responding to attractors. Organizational responsiveness is driven as the LTC mounts a collective response to attractors enabled by the emergence and organization of the system from within (Chandler et al., 2016).
The purpose of the present study is to understand the experiences of APRNs as they transition into the LTC setting as a new practice environment. This inductive ethnographic study, sensitized through a complexity science lens, will explore both the APRN and LTC as CAS with mutual influence. Specifically, we will focus on the values, beliefs, and behaviors of APRNs that influence their transition and simultaneously influence the LTC organization.
Research Design and Methods
The Texas Health and Human Services Commission and the Center for Excellence in Aging and Long-Term Services housed at the University of Texas at Austin, School of Nursing, received funding from Centers for Medicare & Medicaid Services to examine the impact of embedded APRNs on the LTC practice environment, specifically with respect to resident care quality outcomes, as part of a collaborative quality improvement multiple methods study “Transition to Practice in Long Term Care Settings in Texas.” Our specific component of the project addressed the impact of transition on the APRN and the reciprocal impact of the APRN on the nursing facility.
Ethnographic participant observations and interviews were used to understand the social and cultural context of transition into the first year of practice of a cohort of APRNs in LTC. (Agar, 2004). Ethnography is well-suited for exploring complex, multi-faceted change, which requires adjustment by both the practitioner and those in the environment into which the practitioner enters (Agar, 2004; Fitzpatrick & Gripshover, 2016). In an inductive ethnographic process, theoretical insights help inform hypotheses and interpretation of data, as opposed to validating theory though a representative sample (Wilson & Chaddha, 2009). Using inductive ethnographic methods sensitized by a complexity science theoretical perspective, we approached data gathering through the lens of symbolic interactionism with the understanding that participants create reality and express culture through “a system of meaningful symbols” in which “humans act toward things on the basis of the meanings that the things have for them” (Blumer, 1969, p. 2; Spradley, 2016 [1979], p. 6). Culture and social meaning can be found in the interactions that individuals have based on these systems of symbols (Blumer, 1969). Iterative collection of data through participant observation and interviews allows for ongoing analysis and synthesis of a shared culture revealed through interactions from the participants perspective as informed through the researcher’s inductive ethnographic methodology (Rock, 2001).
Sample/Setting
Recruitment of five Medicaid-eligible long-term care facilities (out of ~1,300 in the state of Texas), located in Central Texas, occurred through the Texas Health and Human Services Commission and the Center for Excellence in Aging and Long-Term Services housed at the University of Texas at Austin, School of Nursing. The five LTC facilities were solicited and volunteered based on willingness to participate in this quality improvement, demonstration project. Facilities were vetted to ensure Medical Director acceptance of APRN presence and oversight, as well as for administrative support of the project. Three facilities were traditional nursing home facilities (Medicaid eligible), one was a post-acute facility with long-term resident and acute care rehabilitation populations, and one was a long-term psychiatric nursing facility. A diverse qualified sample of APRNs (N = 9), hired through a large university’s Human Resources center, participated in the present study. They were chosen as part of a quality improvement study employing APRNs to provide direct patient care and oversee quality improvement initiatives within their assigned LTC facilities. This large multiple methods study employed, educated, and embedded APRNs within five facilities for 12 months, with an optional 1-year employment extension in the facility at 50% pay. The sample included all APRNs hired as part of the multiple methods study and were included in the qualitative sample (N = 9). All the participants agreed to consent to participate in research as part of their employment and facilities acceded participation through contracts to participate in the quality improvement project. The APRNs’ demographics, experience, and preparation varied, including APRNs with and without experience in the advanced practice role and with and without experience in the LTC setting (Table 1), so they were paired for the study’s duration as experienced APRNs each with a less experienced APRN, while one APRN worked independently. The quality improvement project was reviewed and approved by the Institutional Review Board of the University of Texas at Austin as a multiple methods study (#2019-01-0037). Anonymity and confidentiality were maintained through secured fieldnotes and transcripts (lock box or password protected secure online BOX storage system) and all names were changed to alias’s in all forms of dissemination.
Demographics of the APRN Sample (n = 9).

Data Collection
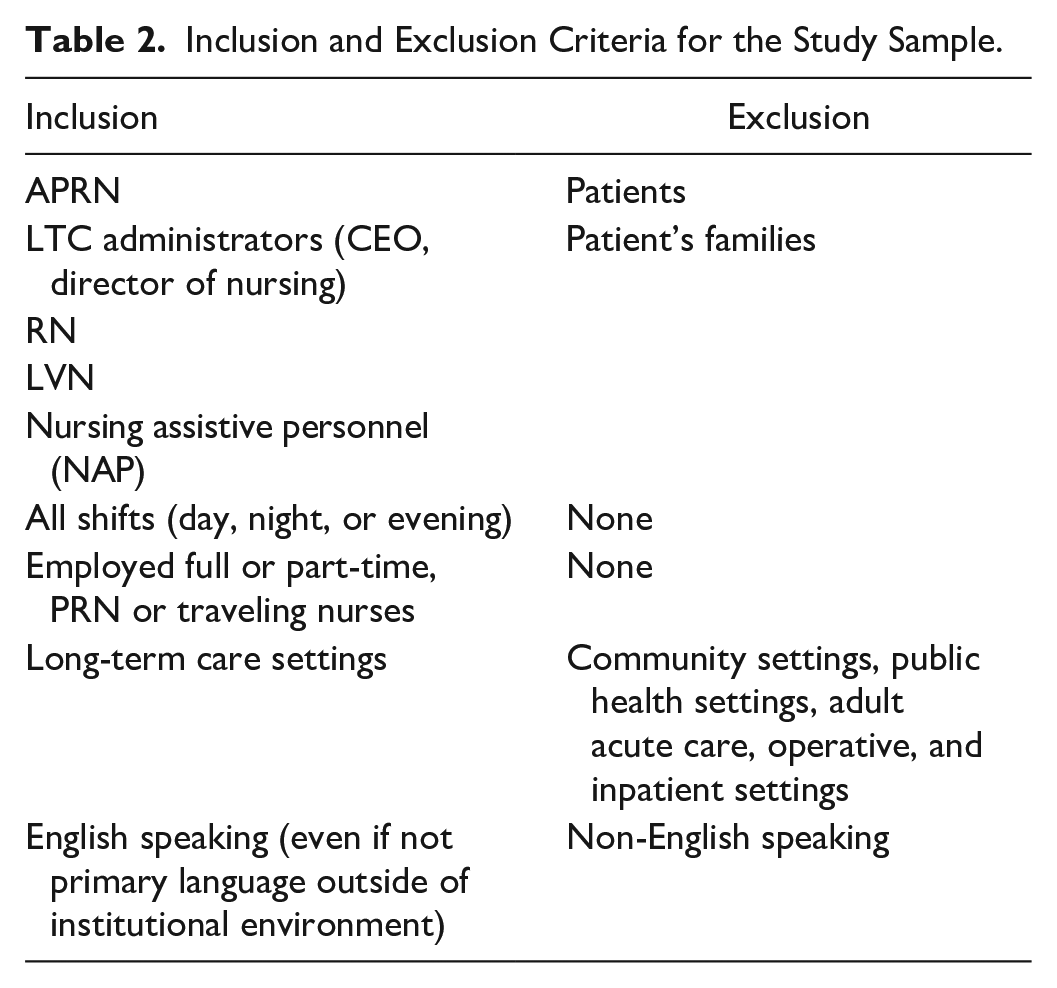
Data comprised observational field notes, semi-structured interviews, and researchers’ reflexive journaling, which informed further observations and interviews iteratively. Observations and interviews occurred during classroom education (months 1–2) and subsequently in the five LTC facilities (months 3–8). The primary and secondary authors spent extensive time in the field over the first 9 months observing the daily structure and function of each LTC site and the interactions of the APRNs with staff, residents, and other healthcare providers in the natural setting. Interviews took place in both structured settings with the primary author as well as spontaneously in the field as situation and time allowed. The interviews first focused on building rapport and were expanded in the facilities to include select LTC personnel (Table 2).
Inclusion and Exclusion Criteria for the Study Sample.
Interviews began with a list of guiding questions (Table 3) but evolved in accord with the ethnographic principle that answers guide further questions (“both questions and answers must be discovered from informants”; Spradley, 2016 [1979], p. 84). Questions focused on eliciting rich descriptions to understand lived experiences from a personal, cultural perspective; observations focused on interactions between participants and their organizational atmosphere, revealing culture. Structured interviews were recorded either via handheld device or via online video platform and later transcribed. Spontaneous interviews were captured with hand-written, or voice recorded fieldnotes.
Ethnographic Guiding Questions.

After month 9, protection of the vulnerable LTC population during the COVID-19 pandemic prevented in-person observation and interviews. However, by this time, researchers and participants had established sufficient rapport to continue interviews via teleconferencing where they were recorded for later transcription. This imposed isolation did require additional strategies to elicit rich descriptions from participants to ensure sufficient data for thematic analysis and synthesis especially given the shift in focus of LTCs to the COVID-19 response. Techniques employed included Spradley’s (2016 [1979]) ethnographic explanations on the part of the researcher to refocus the discussion specifically on the transition experience as well as multiple forms of ethnographic questions (experience questions, contrast verification questions, directed contrast questions) and descriptive questions all meant to help the participants relate their unique COVID-19 experiences to their ongoing transition experience.
Data Analysis
Analysis proceeded iteratively during the 12 months of data collection, with statements, quotations, and fieldnote patterns extracted manually and grouped into categories with subthemes and themes (Table 4). Complexity science informed the analysis through attention to the holistic nature of multiple moving CAS’s that constituted the daily structure and function of the LTC with special attention to attractors that influenced the APRN transition experience (Figure 1). Analysis proceeded iteratively yet stepwise in the following manner; (a) transcribed interviews and fieldnotes were continuously manually reviewed and cut into distinct excerpts, (b) like phrases and excerpts were posted to foam boards, (c) excerpts were analyzed periodically throughout the data collection process as new groupings or ideas were identified and were created through additional data, review with an ethnographic expert and review with participants, (d) grouped excerpts were combined initially into categories which were distilled and grouped further into preliminary final subthemes and themes, and (e) final themes/sub-themes were confirmed with both ethnographic expert and participants.
Categories, Sub-themes, and Themes.

Trustworthiness was maintained with reflexive journaling during data collection and analysis to address potential biases (Morse et al., 2002). Checkback and verification of synthesized findings were assessed with participants throughout the study, with feedback incorporated into further questions and observations to ensure credibility and trustworthiness. Frequent discussions of the iterative analysis with an ethnographic expert helped reactive, proactive, responsive findings to emerge, be interpreted, and become credible. Length of time and volume of data analyzed (>400 hours of observation time, >1,000 hours of interviews, and >50 pages of hand-written fieldnotes/journals) also increased credibility by ensuring sufficient experience to construct iterative questions, analyze observations, and build reliable themes through synthesis and reflection.
Findings
The stories of the APRNs, here pseudonymously named Alison, Charlotte, Kelsey, Carrie, Victoria, Sally, Jenny, Natalie, and Donna, present the effects of institutional acceptance, practitioner competition, and discomfort with quality improvement, as well as the APRNs’ struggle for practitioner legitimacy as they transitioned into their expected roles in LTC. The LTC settings’ transformation while the APRNs were present is woven into their stories. The APRNs’ transition was fraught with ambiguity for both novice and experienced APRNs; barriers to perceived legitimacy threatened practice, while environmental, financial, and personnel attractors affected their ability to reach residents and influence their respective nursing facilities. This is documented by 17 categories, 7 subthemes, and 5 major nonlinear themes (Table 4).
Theme 1: Where’s My Authority?
Live it to get it
Initial interactions between the participants and researchers centered on regulatory and classroom training, characterized by participants’ awe and paralysis yet tempered by excitement about their new role. The experienced APRNs were more engaged and asked more questions of the presenters; they congregated together and engaged in small talk, whereas the inexperienced APRNs focused quietly on their laptops. As Jenny, an APRN with previous experience confided, “these guys are drinking from a water hose”—a visual image of overwhelming information that the new nurses would have to “live” to understand.
Natalie, a newly minted APRN, asked few questions during presentations, but afterward expressed excitement: “we all just want to get out there.” Alison referred to her quietness during presentations as “absorbing information.” Overall, the experienced APRNs knew what questions to ask; the less experienced APRNs did not know what they did not know, reinforcing Jenny’s words that they would “have to live it to get it.”
Listen, I am one of you, only more
Once the APRNs entered the facilities after training, observations and interviews focused on how the culture of each facility influenced the APRNs’ ability to function and on their respective experiences of transition. When asked what she did to establish herself as a practitioner in her new environment, Charlotte related what most others reported: they resorted to basic nursing skills in the beginning to establish their bona fides as a “nurse” first. Charlotte wanted to be an asset, not a burden; her nursing skills were assets to bring to the table. Applying basic nursing skills benefitted the APRNs in two ways—establishing themselves as embedded caretakers, and engendering goodwill for staff partnerships. Charlotte thus found that staff readily partnered and brought concerns directly to her because of her willingness to “jump in anytime, anywhere,” which garnered her legitimacy and acceptance. It also facilitated visualization of potential problems.
This technique was tempered if an APRN was paired with an experienced APRN who focused on advanced role obligations. Donna and Sally, both experienced nurses, relied on basic skills to “be helpful” with a primary focus on establishing teamwork. They used the goodwill that they earned to recruit LTC staff, especially nursing assistants, as partners in patients’ care. As partners, the assistants were encouraged to bring concerns about residents to the APRN instead of waiting for an outside provider’s weekly rounds. Authority was given and found in the team when people needed help.
Theme 2: Institutional Acceptance
Hospitable environments: Facility layouts, provider space, institutional mission
Provider space and institutional mission influenced APRN transitions. Carrie and Kelsey were placed in a LTC facility for residents with psychiatric comorbidities at the edge of an urban area. The building had low ceilings, decaying boards, few windows, and outside areas with neglected grass. Two layers of 15-foot chain linked fence surrounded the facility. These field notes give an initial impression: Upon entering the building, I was greeted by a nurse with a grimace who demanded to see a badge—a general feeling of unwelcome. Carrie, our APRN on duty, would say “the asylum is run by the inmates,” referring to the insular, multigenerational staff who ran the place, unresponsive to management and outsiders.
This feeling of being unwelcome extended to the APRN’s workspace. Although each facility had to sign a contract to provide each APRN team an office with access to its computer network, this was not the case for Carrie and Kelsey, who found themselves relegated to a large conference room that served different purposes including storage, monthly dental cleaning visits, recreational therapy, storage, and the APRN office. Carrie was flustered, embarrassed, and sometimes on the verge of tears, describing it as “so dirty”—“I can’t work in this environment.”
In comparison, another facility was new, bright, airy, and welcoming, surrounded by newly planted trees and gardens. The smell of coffee from the in-house barista and not the smell of cleaners or body odors hit the senses. Yet despite this modern “culture of hospitality,” the facility split relatively evenly between traditional LTC residents and acute care rehabilitation patients, which created conflict. Preexisting physician/APRN care teams were unable to bill for the study’s APRN services provided to the acute care rehabilitation patients, so they prohibited access to those patients. Victoria, the APRN, stated she felt “redundant.”
Sally and Donna were located at a family-operated, older, rural facility. Sally believed that the facility would be backward, without flexibility, and requested an assignment change. However, the two APRNs were welcomed with an office space, independent APRN practice, and supportive administration who worked to hire one APRN post study. Despite Sally’s initial impression, the facility was clean, and the administrators and staff prided themselves on their local ownership, longevity of top administrators, and philosophy (The Eden Alternative, 2012). The LTC residents were not “residents” but “Elders,” preferably referred to by name. As Donna stated, “words have meaning,” and this approach allowed her to “refocus on people.”
Signal when ready
According to Blumer (1969), people act based on ascribed meanings of objects and people. Thus, the placement of the APRNs in the back or front of a facility had meaning. For staff and residents, such subtle visual signals demonstrated the organization’s perceived importance of the APRN. Administrators of each facility were vetted to ensure that they would support the APRN and the study’s goals. Nevertheless, the administrators’ understanding of the APRN’s role and support varied. The administrator for the psychiatric facility, expressed an interest to hire an APRN after the assignment, with time split between functioning as the Director of Nursing and as an APRN. The facility had difficulty maintaining a dedicated Director of Nursing and he believed that this would solve the problem, as well as eliminate having to pay a full APRN salary. Brian’s misunderstanding of the roles of the APRN and the Director of Nursing created conflict; during the year, the facility went through three directors, and one of its two APRNs resigned.
In contrast, another administrator expressed interest in working to extend an APRN contract beyond the first year. This interest was eventually rejected by her board, but she negotiated an 8-week extension so that the APRN could help with the COVID-19 pandemic response. This administrator consistently included the APRN in staff meetings, gave her a personal office accessible to staff, and collaborated with her on quality improvement projects. In this way, the APRN did not have to wait or ask to be included.
Theme 3: Personal Role Fulfillment
The confident self: Fake it until you make it
The nurses displayed varying levels of intrinsic drive to engage and seek transition experiences. Most expressed initial confidence in their abilities to perform as an APRN, but this was tempered by reality in the field. When Charlotte stated, “I’m confident, I’m smart, but. . .,” she let her voice trail off on the “but,” emphasizing her feelings of insecurity. Even though Charlotte had the initial disadvantage of being the only APRN placed on her own, she maintained self-confidence and demonstrated drive in her practice. She made the most of every experience; in the end, she said, “I learned so much”; “I try to make the best of whatever.”
Carrie, who began with high confidence given her previous APRN experience, was quickly discouraged and disappointed by a lack of staff engagement. She produced modules for the staff, but the facility “wore her down”: “everything I have done here has done nothing”; “at this point I’m done with this place”; “if I wasn’t dedicated to stay to the end, otherwise I woulda quit.” She believed that her intrinsic motivation to “make a difference” kept her engaged even though she met great resistance to her presence and her colleague APRN quit the psychiatric facility.
Theme 4: Provider Relationships
Oversight: Competition or indifference
In Texas, the usual APRN model for LTC relies on APRNs contracted with physicians (Medical Doctors or Doctors of Osteopathy) who as medical directors supervise nursing facilities. Medical directors oversee the general medical care provided to the facility’s residents, review charts, and set up protocols to ensure that medical care meets expectations for billing Centers for Medicare & Medicaid Services and complies with regulations. Given their salary expectations, medical directors are known to contract with multiple facilities and employ teams of contracted APRNs to evaluate residents several times a week (APRNs pay a fee to the directors to provide supervision of care for a portion of the reimbursement). This reality meant that the APRNs in this study shared responsibility for collaborating on resident care with the facility medical directors and a pre-existing network of APRNs providing on-call care who were already comfortable in their set processes. Most of the study’s embedded APRNs described conflict with their medical directors. The relationship ranged from “sometimes” valuable to “it’s an extortion racket” (in reference to the 15% fee paid to supervisory directors for services rendered “whether used or not”).
The embedded APRNs worked more closely with previously established and contracted APRNs than they reported working with the medical directors; only Natalie, Jenny, and Charlotte voiced active director support. As the APRN with the least nursing experience and the only APRN not paired with an experienced partner, Charlotte found this relationship invaluable when she had advanced-level questions. Jenny and Natalie were included as equals in all team quality and patient rounding meetings and were called upon to share their expertise on patient care and progression. Even so, only Jenny believed that the director might hire her on to the team at the end of the project, and Charlotte responded “potentially.” The medical directors did not support the embedded APRNs as partners in care.
Direct perceived competition threatened and delayed transition into the LTC setting. Two APRNs, Donna and Sally, encountered direct conflict with the medical director that required mediation by the facility administrator. One APRN attributed criticism from the contracted APRN and the medical director to a confrontational personal style and to her decision to evaluate resident laboratory findings that were waiting for attention. According to the administrator, the biggest issues that we had, had to do with how they integrate with the existing nurse practitioner and the medical director who has to oversee them. They don’t have a relationship prior to coming here, or you know, they don’t have any built rapport. It’s hard to give comfort level for moving forward.
The APRN who remained at the facility after the confrontation, Donna, stated that “Dr. X was worried about me taking money away from them,” and this “could be one of the biggest issues to this program working.”
Theme 5: Individual Care Versus Organizational Care
Role uncertainty
When the APRNs were hired for this project, they received two objectives; (1) to embed and round on residents in LTC facilities to provide for their daily resident care needs and (2) to collect and synthesize data to inform quality improvement projects and staff education, as well as identify additional data monitoring needs. Most APRNs initially focused on the first objective and on daily activities such as resident evaluations, team building, and establishing rapport. Uncertainty shifted their focus to establishing legitimacy by advertising their skills as nurses first, despite their advanced credentials.
The difference between those who limited their practice to direct resident care and those who were able to progress to quality improvement projects reflected their focus of care: the individual resident or the nursing facility as a system. Thus, APRN Victoria focused on “gaining access” to residents in the face of medical team resistance and barriers. Charlotte stated she was “overwhelmed and I don’t know where to start.” In a facility that suffered from in-fighting among staff, she reverted to her RN-level skills to gain legitimacy and peace before she could consider tackling the second objective. Other APRNs believed they were met with a borderline hostile environment, which prevented them from diving into quality improvement. Carrie identified missing compliance and safety issues early, but her focus remained on resident evaluations and order writing. It took months before she attempted to host a staff training to address facility quality improvement.
Discussion and Implications
The purpose of this ethnographic study is to understand the experiences of APRNs as they transition into the LTC setting as a new practice environment as well as the mutual influence of the APRN on the LTC environment. Our findings are consistent with previous studies suggesting that the transition to practice is complex, characterized by insecurity whether the individual is new to practice or experienced (Chicca & Bindon, 2019; Yeager, 2010). Brown and Olshansky (1997) envisioned APRN transition as consisting of stages in which a nurse builds a foundation as an expert: (1) laying the foundation, (2) launching, (3) meeting the challenge, and (4) broadening the perspective. However, as Brown and Olshansky (1997) were quick to point out, and as we observed in our study’s APRN participants, this progression is not linear, and the stages of progression are not mutually exclusive. Ideally APRNs would build on their previous nursing skills to focus on larger concepts such as quality improvement, through broadened practice. The present study shows that for our participants, transition was not guaranteed, regardless of previous experience. It was not linear or regular, and it relied instead on multiple intertwining attractors, which included institutional acceptance, personal role fulfillment, provider welcome, role confusion, and the struggle for legitimacy.
Practice-Based Transition
Conflicting factors affect APRNs’ TTP, and research has shown that a lack of formal transition negatively affects transition, whereas the presence of a program is positively correlated with reduced stress and increased retention (Cusson & Strange, 2008; Flinter, 2010; Han et al., 2018; Sullivan-Bentz et al., 2010). APRNs attend 2 to 3 years of preparatory graduate education, yet there is no formal national residency process after graduation (Auerbach et al., 2018). Residency, if offered at all, is usually offered by large organizations such as the Mayo Clinic or state agencies such as Texas Health and Human Services Commission (Center for Excellence in Long Term Care, n.d.; Hansen, 2013). Our cohort of APRNs had classroom training, but it was not paired with graduated practice, which has been identified as the best strategy for transition programs (American Nurses Association, 2020). Charlotte summed this up best: “training would have been more beneficial if I went to the facility first.” The recurring experience of paralysis and catatonia observed in the APRNs as they appeared “under water,” as not fully RNs but not fully APRNs yet, could be lessened and overcome with earlier hands-on experience capitalizing on the excitement to “just start already.” This would help meet APRNs’ needs for self-fulfillment and to feel valued as patient caregivers.
Reimagining Mentorship and Supervision
Current APRN mentoring in many states involves collaborative practice agreements for formal supervision with physicians, either permanently or through graduated practice for 2 to 5 years; yet this model is not effective and increases costs (NCSBN, 2014). These agreements may institutionalize oversight and reinforce subservience that interferes with collaboration (Martin & Alexander, 2019). A more useful and effective transition model consists of mentorship with an experienced colleague, with modeled behaviors, networking, and stress relief (Hill & Sawatzy, 2011; Kleinpell & Hravnak, 2005; Poronsky, 2012; Twine, 2017). Thus Charlotte, even though she had the least nursing experience, let alone APRN experience, found a mentor and guide in her medical director, who quickly and without judgment answered her questions about patient care. By the study’s end, Charlotte had great confidence in her practice, and she was a finalist for a similar LTC quality improvement job in another state. Conversely, Alison had multiple years of APRN experience, but the lack of welcome at her facility and the siloed care provided by the medical team prevented any mentoring or acceptance. Her stress increased, appropriate behaviors were not modeled, and no networking was allowed, resulting in her early resignation.
More attention should be given to differentiate between codified APRN oversight and desired support, which is more nuanced. Empowerment provides personnel with the resources and authority to capitalize on opportunities, which can increase accountability, proficiencies, and worker satisfaction (Almost & Laschinger, 2002). The APRNs in this study who received structural empowerment through access to patients and practice space demonstrated more successful transitions than did those who were frustrated in their efforts. Donna and Sally received office space, immediate access to patients, and even support in a dispute with the medical team regarding billing. Carrie and Kelsey were given none of these due to poor administration, and their lack of perceived power led to lack of real power as the medical director did not follow up on their recommendations.
Empowerment incudes autonomy. Nurses consistently rate autonomy as a primary reason for seeking an advanced practice degree (Havaei et al., 2016; Strachota et al., 2003). Quality care from APRNs is linked to practice authority, which is determined by individual state law (American Association of Nurse Practitioners, 2021). State health rankings from 2012 demonstrate that states’ care was closely correlated with full scope of practice for APRNs, implying better outcomes in states with more autonomous APRN practice (Oliver et al., 2014). In states without a period of physician oversight leading to independent practice, no safety issues have been identified, calling into question the model of physician supervision through collaborative practice agreements (NCSBN, 2014).
Some of the conflicts and hindrance to transition observed in this study can be attributed to this codified supervision instead of autonomous practice with mentorship. The power differential created by this arrangement impedes the development of true collaborative teams and controls APRNs instead of focusing on patient care. The relationship between physicians and APRNS should be reimagined for a better balance among mentorship, empowerment, and autonomy instead of the ineffective proxy of supervision.
APRN Education Opportunities
Our study suggests opportunities to increase transition success with structures and empowerment that reflect the first three steps of Brown and Olshansky’s (1997) transition model, which would allow APRNs to focus on broadening practice. The 2008 consensus model for APRN practice identifies the APRN as having a “component of indirect care” but “retaining a significant component of the education and practice focuses on direct care of individuals” (APRN Consensus Work Group & the National Council of State Boards of Nursing APRN Advisory Committee, 2008, p. 7). APRNs receive education in indirect care, but the APRNs in the present study were much more comfortable and vocal in their preference for direct patient care. These two sides of practice appeared at odds, and the APRNs felt conflicts between direct and indirect care served as attractors interrupting transition.
Further research can also be conducted to examine how differences in educational foundations between the Nurse Practitioner role and the Clinical Nurse Specialist influence their transition experience and influence on the LTC environment. In the US, the two types of APRNs have different identified scopes of practice; the Clinical Nurse Specialist is focused on a specialized area of nursing such as a disease or patient population with a systems approach on indirect healthcare activities, while Nurse Practitioners are focused on more general clinical practice concentrating on diagnosis, prescription, and whole person health (International Council of Nurses, 2020). In reality, healthcare services and administrators often view these roles interchangeably confusing outcomes and understanding of potential unique contributions (Mohr & Coke, 2018). Globally, the role of the Nurse Practitioner is better defined and even more protected through regulation and licensing than the Clinical Nurse Specialist, indicating further room for understanding and utilization of these unique advanced practice traditions (Cooper et al., 2019). Though no thematic differences were found in this sample, it is possible, given their different educational and practice focus, that Clinical Nurse Specialists and Nurse Practitioners will have different transition experiences in the highly regulated LTC practice environment, warranting further exploration.
APRN participation in quality improvement monitoring improves quality outcomes in a variety of settings, including LTC (Evans et al., 2019; Kaasalainen et al., 2016; Rantz et al., 2018; Unroe et al., 2015). Tappen et al. (2017) identified barriers to participation in quality improvement in nursing homes that were also found in our study: resistance to change, competing demands, leadership instability, and lack of organization-wide involvement. The dominance of clinical preparation in APRN education creates a perceived primacy of the direct patient experience, as we observed in Victoria’s nostalgia for her intensive care unit days and in Sally’s preference for patient care over paperwork. The AA N (2020) has identified the Doctor of Nursing Practice degree as a potential solution to the increasing complexity in U.S. healthcare which “requires a higher level of preparation for leaders who can design and assess care” (AACN, 2020). More research is needed to understand whether additional coursework is necessary or whether the APRN consensus model should be revised to better reflect the need for APRNs to be more proficient in indirect patient care upon graduation.
Limitations
Research in LTC settings may not be generalizable to other practice settings. Our sample was purposive, with APRNs hired to participate in a Texas Health and Human Services Commission quality improvement, demonstration program. The APRNs were from a variety of educational and practice backgrounds, but this was a qualitative study of their experiences, and TTP is conceptually similar for both experienced APRNs new to LTC and APRNs new to advanced level practice. Each APRN’s transition experience represents an interdependence between organizational culture and the participant. Though the purposive sample was small, the amount of data generated was large. This volume of data allowed for saturation of themes revealed by “informational redundancy” indicating no new or apparent information and signaling the sample was adequate and the findings trustworthy (Sandelowski, 2008, p. 875).
Current research has been limited by the COVID-19 pandemic, which forced the research team out of the LTC setting with approximately 2.5 months left in the observation period. This pathogen has ravaged and killed LTC residents disproportionately, causing unsettling distress and altering APRNs’ daily routines; however, this paradoxically amplified the APRNs’ transition experience. The crisis revealed those who were accepted as part of the solution within their facilities, cementing their successful transition, and exposed those who were not included. For example, Charlotte was an integral part of her facility’s consolidation and relocation plan for residents, and Donna’s tenure was extended 2 months to help with the COVID-19 response; but Jenny and Natalie were sidelined through isolation and not considered part of the core COVID-19 response team.
Conclusion
Although transition programs are well established for RNs, APRN transition in LTC is necessarily different, owing to the additional responsibilities inherent in advanced practice, a unique regulatory environment, as well as power structures imposed through collaborative agreements between APRNs and physicians. Given that LTC physicians have financial disincentives and are declining in number, APRNs need more support for practice into LTC settings, including intentional transition opportunities. APRNs’ unique focus on holistic, organizational, person-centered care makes them ideal providers to balance the needs of a population of residents, not patients.
Footnotes
Acknowledgements
The authors would like to thank the five participant nursing homes and their respective administrations for providing access and support, and to our nine Advanced Practice Registered Nurses for sharing their candid experiences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Centers for Medicare and Medicaid Services, Civil Money Penalties grant (TX-0418-TXCHHS-021) joint study between Texas Department of Health and Human Services and Center for Excellence in Aging Services and Long-Term Care center housed at the University of Texas at Austin, School of Nursing.