
Abstract
Injection drug use has long been a topic of investigation, whether through a health or criminal justice lens. Whilst these bodies of literature offer important perspectives, missing from the extant literature is evidence, particularly involving women who use drugs, and more specifically evidence about the health beliefs of these women. To address this knowledge gap, we undertook an ethnographic study of homeless women in downtown Ottawa who inject drugs. This included interviews, observations, and artifact analyses. In this paper, we report on these ethnographic data to show the context and nature of the subjective lives of women who use injection drugs and their beliefs and perspectives on health. We use these data to make recommendations for nursing and healthcare practice moving forward.
Introduction
Intravenous injection drug use has a long been considered a social aberration. Initially, it was criminalized and viewed as weakness of character or will (Petersen, 2002). The advent of HIV then fostered a new perspective about infectious disease transmission via drug paraphernalia, and persons who use drugs (PWUD) were seen as vectors of illness and disease (Ettorree, 2007). Thereafter, efforts were made to reposition injection drug use as a sign of mental illness, with addiction and substance use being subsumed under this broader category. More recently, the focus for PWUD has been on the needless loss of life caused by preventable overdose deaths (Special Advisory Committee on the Epidemic of Opioid Overdoses, 2021). In all such cases, injection drug use is positioned as loathsome.
In contrast to these perspectives, within the context of this paper, we see drug use as a manifestation of systemic societal structures which intersect and fail to serve certain – often marginalized and vulnerable – people. As one of the potential outcomes of this oppression and resulting deprivation, we believe drug use should not be a criminal act, nor something to be corrected by the judicial system; we also do not feel that overdoses are a sufficient reason to study drug use either. Drug use is a healthcare issue that warrants care and compassion. From this perspective, the aim of our study was to explore the subculture of persons who identify as women who were experiencing homelessness and who use injection drugs (WUID) and to present an understanding of what was meaningful to these women when making healthcare decisions. Each component of our research was scrutinized for information about the items and elements which predominated participants’ days. We wanted to learn more about participants’ notion of health and what they wanted regarding nursing care. Our theoretical position was one of critical theory (Guba & Lincoln, 2005), such that we did not seek absolute truths, but sought to understand the lived cultural realities of women who agreed to participate in our study. We wanted to use this information to help nurses provide care that fit within this culture.
Literature Review
Despite the aforementioned changes in focus regarding injection drug use, this practice continues to be tracked via criminal justice metrics and research – almost always with the purported focus of understanding and mitigating harm, albeit from a variety of perspectives regarding the concept of harm. Little research. focuses purely on understanding the lives and lived experiences of PWUD as it relates to the concepts of health and healthcare. Furthermore, much of the healthcare literature is about PWUD but not from them (for example see: Bernstein & D'Onofrio, 2013; Brubacher et al., 2008; Huber et al., 2009; Kievlan et al., 2015; Ti & Ti, 2015; Walley et al., 2012), Moreover, from our review of the literature, much of the research on PWUD includes either samples of exclusively male participants or male and female participants, with limited research samples comprising only females (see: Firestone & Fischer, 2008; Lankenau et al., 2012; Neale et al., 2007; Roy et al., 2011). Current evidence about the implications of sex and gender on PWUD experiences is thus lacking. The profound health needs of these women further emphasizes their need for relevant and accessible health and nursing care. Indeed, not only does experiencing homelessness negatively impact the health of women (Speirs et al., 2013), but also WUID are more likely to experience ‘physical and sexual violence, HIV and hepatitis C transmission, and injection-related harms’ (Collins et al., 2019, p. 43). We believe that, as the need for healthcare increases, so must the availability of accessible healthcare for these women.
Methods
We undertook an ethnographic study of the subculture of women who use injection drugs (WUID) and who were experiencing homelessness in downtown Ottawa, Canada. At the time of this research, this city’s population was estimated to be one million and has been noted to lack a robust and creative housing first plan for vulnerable populations.
Our overarching goal in this research was to learn about the lives of the participants, who self-identified as women, from their perspective. For this paper, we reported on the observation and artifact data to show what these data revealed, in addition to the words participants used to describe their lives. We generated information about how women saw their lives to gain information that would assist in tailoring nursing services to their wants, needs, and routines. The study was not, however, intended to be a feminist gender analysis or an objective exposition of WUID; rather, our purpose was to learn more about the everyday life, patterns of behaviour, and activities that were inherent in the lives of women experiencing homelessness who use intravenous drugs to enable a better understanding of how healthcare might be better provided.
The author team consisted of two PhD prepared primary health care nurse practitioners (CK, POB) and an RN PhD candidate (MH). All three authors provided clinical primary healthcare services to WUID at the time of this research. CK engaged in interviews and observations, collected artifacts, and asked the participants to take photos of images they felt related to health.
Due to concerns regarding the collection of identifying information from the women and thus the potential to have others identify the participants as women who use drugs, codes were created to sign the consent forms. That is, due the possibility of having study data apprehended by police, enabling law enforcement agencies to identify the participants as drug users, it was felt to be a risk we could not take. Whilst the use of codes protected the women, it meant we were unable to seek out the women for clarification and discussion of their photographs.
Despite ethnographic research having differing main approaches and strategies, Hammersley and Atkinson (2019) described five main principles that underpin such research. These are as follows: (a) participant behaviour should be observed in everyday environments, (b) data should be obtained from a variety of sources, (c) data collection should be mostly unstructured, (d) the sample should include a small number of cases and (e) analysis must evolve from the interpretation of the data to build an interpretation of participant behaviour.
As such, to understand the WUID subculture, the overarching study included participant observation, artifact collection, and unscheduled and scheduled unstructured and semi-structured conversations. Field notes, audiotapes, and personal records documented the research (see Figure 1). In this case, the photos were understood to represent something each woman felt related to their health. Ethnographic research process.
Further, the study employed critical ethnography which explores social injustice and hopes to facilitate change (Carspecken, 1996; Madison, 2012). Critical theory aims to ‘call into question the social and cultural conditioning of human activity and the prevailing sociopolitical structures’ (Kincheloe et al., 2011, p. 172). From this perspective, it is not the method of data collection that differentiates critical ethnography, but rather, the lens of analysis that attempts to ‘disrupt the status quo’ (Madison, 2012, p. 5) and unveils ‘taken for granted assumptions’ (Madison, 2012, p. 5). Thus, we analysed the data for insights about new ways to enhance health care services for WUID experiencing homelessness.
Research ethics approval was obtained from the Research Ethics Board at the University of Ottawa (REB approval # H05-14–08). No external funding was obtained for this study.
To fulfil the principles of ethnography (Hammersley & Atkinson, 2019), the current study ensured WUID were observed in healthcare settings and in a women's-only social program. Artifacts were gathered, including posters and flyers, along with drug use equipment. Additionally, WUID took photographs of items they felt were related to their health. Face-to-face audio-recorded interviews also occurred with WUID, who spoke about their lives and their ideas about health and healthcare – some of these results have been published elsewhere (Kitson & O’Byrne, 2021; Kitson & O’Byrne, 2020). Lastly, field notes were compiled and included in the research analysis, which was structured using thematic analysis (Guest et al., 2011).
Some study participants contributed to more than one aspect of the study; for example, interviews and photographs. This potential overlap was sought to enhance the description by allowing data collection from the same woman in different contexts. Congruencies and discrepancies of such content can identify commonalities and unique attributes of cultural norms. Therefore, the subculture of a cohort of WUID experiencing homelessness in a Canadian urban environment was explored in a multifaceted and in-depth manner.
Study Procedures
Participant Observation – Data Collection
Congruent with ethnography, participant observation was part of the study (Angrosino & Rosenburg, 2013; Hammersley & Atkinson, 2019; Polit & Beck, 2016). Participant observation enhanced understandings about reported subcultural norms, thus increasing appreciation of, and insights about, the unwritten rules that shape when and how the women act. The naturalistic setting of these observations, moreover, provided an unstructured environment for data collection about the experiences of WUID accessing care. Participant observations were conducted in various settings, including healthcare appointments, receiving care in a women’s shelter, a women’s drop-in program for those at risk of bloodborne infections, and chance meetings. Over the course of the study from June 2014 through December 2014, CK spent 104 hours completing formal participant observations in six different locations.
Verbal and written consent was obtained prior to observation. Formal written consent was provided by the healthcare providers at the first observation as well (Byrne, 2000). Participant observation proceeded with the healthcare provider asking the client – in the absence of the researcher – if the researcher could be present during the appointment. If permission was given, prior to the start of the appointment, an overview of the research and the participant role was provided for the client by reviewing the consent form. If the women agreed to participate, the form was signed using a designated code format; no compensation was offered as the women were attending a self-initiated health care interaction.
The researcher remained as unobtrusive as possible whilst observing the waiting area, office, and clinical examination rooms (Hammersley & Atkinson, 2019; Jorgensen, 1989; Robinson Wolf, 2012). Questions that arose about the researcher’s role were answered frankly (Madison, 2012; Robinson Wolf, 2012). For example. some women asked if the research study would change their experience of healthcare and this question generated a response explaining that it was a step to continue the process of change. No questions arose in the waiting areas. The examination room questions were mostly addressed when written consent was obtained.
The waiting area and examination rooms were described with words, and a map was drawn to assist analysis. As per Hammersley and Atkinson (2019), the study aims were used to focus the observations. General field notes were recorded as soon as possible after leaving the site and were later reviewed for themes. Subsequent analysis was completed by the then PhD student CK and supervisor POB.
Artifacts – Data Collection
Collecting artifacts enabled more to be known about what people do and the knowledge they use (Murchison, 2010). Hammersley and Atkinson (2019) stated that ‘the ethnography of everyday life demands attention to its material features, and how social actors engage with physical things’ (p.133). The artifacts were studied and analysed for what they portrayed and what they revealed about the culture of WUID and their health. Norum (2008) indicated that artifacts enrich data from other sources, such as interviews, and describe sources other than traditional objects. Artifacts, including various articles and posters, were gathered from places that WUID frequent. Needle exchange program equipment were also collected.
Artifacts can also be created by participants (Norum, 2008), and photographs by participants. for example, can bring attention to alternate perspectives and communicate at a different level than words (Musoke et al., 2015). Imagery can be ‘innovative’ (Prosser, 2013, p.196) and provide new insights (Prosser, 2013), which ‘capture a realistic slice of life’ (Poindexter et al., 2010, p.83).
Women were recruited to take photographs whilst receiving information about the study, before or during their interviews or participant observation. The women were required to sign a written consent to take photographs, with a caveat that photographs should not contain identifying features of people and the camera must be returned with a minimum of five photos. The women received $20 compensation for their time and effort. The women also signed a second form to confirm receipt of their compensatory money. As noted, the need to ensure the women could not be identified eliminated follow-up discussions about the photographs.
Data Analysis
Data analysis occurred following the work of Guest et al. (2011), with additions from others (Byrne, 2000; Hammersley & Atkinson, 2019; Jorgensen, 1989; Norum, 2008). Analysis occurred for each data collection element individually and then for the three forms in unison. (See Braiding the Data.) More specifically, we used an inductive method of thematic analysis, as described by Guest et al. (2011), because this approach helped ‘identify and examine themes from textual data in a way that is transparent and credible’ (p.15). Guest et al. (2011) developed this approach to capture the ‘stories and experiences voiced by study participants’ (p.16) and to subsequently use these findings to solve ‘real-world problems’ (p.17). Because our intention was to know more about the lives and thoughts of WUID regarding health and nursing care, thematic analysis provided a structure to represent the participants’ narrations.
Practically, data analysis involved segmenting identified items. The segments encompassed a single point on an image or, in text, the start and end of an idea. Once identified, these segments – both in image and in text – were labelled, which was the process of using one or a few words to describe the content of each segment. For the photographs, this involved identifying key elements within the images, such as key items that were visible or the elements that participants put in focus. The goal of labelling was to describe the segment’s content, and to do so using visible elements of the segment (participants’ words, visible items in observation, etc.). Once produced, labels were entered in a codebook (MS Excel), with the listed codes on the vertical axis and data references on the horizontal axis.
After labels were entered in the codebook, similarities and differences were noted, and those that were similar were clustered. Each cluster was assigned a code, which captured the commonality within the clustered labels. Guest et al. (2011) suggested that the more defined codes are, the better the consistency of identification in the data and the cleaner the resulting themes can become. Each code was short and descriptive to cue its intention and substance.
These codes were a second level of analysis, slightly more abstract and filtered than the labels and the raw data. As codes were developed, they were defined and added to the codebook. Existing codes were accepted or revised when the intent was clarified, or new codes were added. All unique data were coded and reviewed for commonalities. If new codes resembled existing ones, they were considered with the perspective of (a) being added to the cluster, (b) revising the current code or (c) adding a new code. Upon determining that a coded item was irrelevant to the research aim, it was discarded in the discussion of findings. This did not mean the finding was incorrect or not noteworthy; it simply denoted a lack of relevance to the study. The codebook was thus an ongoing iterative work ensuring thorough consideration and complete exploration of the data collected. When data were coded to the satisfaction of the process, all content under each code was reviewed and sorted into a meaningful sequence.
Some codes did not fit with the developing coding schema. Guest et al. (2011) highlighted that such outliers can be negative or deviant cases, with negative cases being those that refer to a point that differs from those indicated by most participants, and deviant cases being those that follow a theme, but deviate from the main thinking of the group and extend the continuum of responses. In both cases, because outliers may provide salient information not discussed by other participants (or may be irrelevant), Guest et al.’s (2011) work about the decision to include or exclude outliers was followed. These authors recommended considering the relevance of each case in relation to the study’s aims and theoretical framework, and then in relation to if the case represented content that would change policy or an intervention. If the case was determined to be irrelevant, it was discarded. If the case was relevant, further review occurred to ensure the case was indeed unique and had not been previously identified, or that it represented an addition to an existing theme. A search for an explanation of the outlying case was considered. When variance was adequately explained, and there was a fit with the existing framework, a decision was made to include seemingly stray content without changes (Guest et al., 2011). Therefore, the fate of outliers was determined on an individual basis after a thorough and thoughtful review of the data and possible implications of the information within the aims and the broader context of the study. Guest et al. described that this process is important because it helps guard against ‘cherry picking’ (2011, p.113).
After the coding sequence was completed, including a review of outliers, codes were clustered into themes, which were titled to capture the common point in these codes. These themes were then developed into larger narratives that encompassed the broader sentiments in the participants’ statements and the observation and artifact data. This step completed analysis.
Braiding the Data
Ethnographic studies traditionally combine interviews, participant observation, and the gathering of artifacts to complete a rich and multidimensional understanding of a group or culture (Creswell, 2011; Ellingson, 2011). Denzin and Lincoln (2013) likened the work of qualitative researchers to the work of bricoleurs; that is, to people who make quilts or montages. In ethnography, data are woven together as a bricolage creating a recognizable ensemble of detail gathered from methods used to create a composite from individual data. Polit and Beck defined the term as having to do with postmodern qualitative research which utilizes ‘a complex array of data’, derived ‘from a variety of sources, using a variety of methods’ (2012, p. 721). Kincheloe et al. added that bricolage is an approach in critical ethnography that incorporates multiple lenses to allow ‘fluidity and goes beyond a traditional triangulated approach for verification’ of data (2011, p. 172). Ethnography melds voices, images, observations, and collected matter to formulate an understanding of a culture, which is WUID who were homeless in the current study.
This research understands the observation, artifact and interview data as braided into a strong representation of the gathered data from multiple sources. The strains entwine and become one another, holding each other together whilst making individual contributions to the whole. A braid implies that when multiple data collection methods are used, they can illustrate findings with similarities and others that deviate and sit at the margin, thus illuminating difference. Others have used the word weave (Fetters et al., 2013), but it is the image of a braid that this study used to represent the thick, nuanced description of the data. This enabled an understanding that can inform nurse care.
Results
Participant Observation
The observational data showed that, overall, when WUID accessed healthcare in shelters or in a clinic for PWUD, they were received and treated in ways that, outwardly at least, appeared to be non-judgemental. WUID responded to healthcare providers’ questions with seeming openness and honesty when their drug use was acknowledged and accepted respectfully. The caveat was that the influence of drugs, mental health issues, and sleep and food deprivation, altered some interactions. That is, a few women’s responses were muted if they were high or on the nod – that is seemingly sleepy – or irritable due to lack of nourishment and/or rest and/or drug withdrawal. An understanding of the situational context of behaviours, with the women’s safety prioritized, appeared to be important in providing services to WUID.
Interactions with Healthcare Providers
Observations highlighted that acknowledging, accepting, and applying the social context of WUID within facilitated care provision was important, especially in transitional residential settings where women returned for safety and security. In such spaces, women’s interactions with healthcare providers were grounded in a timely needs-based dialogue. Examples included women returning to a safe refuge because of a need for sleep or a recent altercation or abusive interaction, whereby both the environment and the staff provided physical security and emotional support. Meanwhile, appointment-based healthcare in formal clinics was fraught with limitations, including WUID missing appointments if, for example, they had other priorities such as needing or obtaining drugs, or otherwise felt they could not meet with a healthcare provider. Arriving for a scheduled appointment was often indicative of a specific, sometimes urgent need, such as a court mandated assessment or a wound that had become painful or abscessed.
These two mechanisms for obtaining services (i.e., drop-in and schedule appointments), although different in setting and intent, were spaces where WUID could access care that they deemed accessible and acceptable. Although the settings provided WUID with options within a ‘western’ approach to healthcare, the women for the most part demonstrated expected behaviour, such as politely waiting, being deferential to authority (i.e., healthcare) figures, and complying with instructions from staff. When the women were unable to maintain expected behaviours, consistent messaging and respect from staff and healthcare providers garnered eventual, or at least partial, responses to requests that were intended to enhance safety and enforce rules. Whilst one cannot be certain the women raised or were forthcoming about all pertinent details of their lives during the observed interactions, the women seemed comfortable enough to disclose at least some details of their drug use and related issues during the interactions with staff and healthcare providers. Two examples of participants being forthcoming about their drug use were as follows: I can’t say, what other places or that would be good for women. Maybe some place like [name of downtown health centre with a needle exchange program and health centre]. … They have special times at [name of clinic and recreational drop in for women at risk of blood-borne infections] for the woman’s drop in, where it’s only the women that are going to be seen in the clinic. I think places like this and maybe [name of another health centre] or [name of another health centre] that might be another good place. But these places that deal with people that use, stuff like that, I think these places are the best for anyone to go to for help. But the mainstream, I’d be too scared to (go). Participant AC I’ve been here to see that, what’s her name, doctor she used to be at the [name of shelter with a needle exchange program]. I came to see her a lot, she’s good. Boy, she had a lot of people too. … She was just comfortable to talk to, she didn’t look down on you or wear gloves and make you feel, I don’t care if she would have but she didn’t, like she wasn’t afraid to touch you. Participant AF
Healthcare Environment
The observed healthcare environments were set up similarly to most primary care clinics, with a waiting room, a reception desk, and examination rooms. In these settings, the reception desk created a barrier between the waiting room and the clinic examination area, where the women interacted with providers. Whilst this is a common layout, in the observed settings the separation was pronounced. In some observed clinics, the barrier was a locked door, a half-wall gate, or a metal divider that could be pulled down to close the area. These barriers were imposing and provided a distinct separation between clients and providers. In one community healthcare setting, the door to the needle exchange program was opened and a barrier did not exist. PWUD could freely access the space and staff to obtain harm reduction equipment. In this same area, other clinical venues were physically barricaded by solid, locked doors. It would seem, from the clinic’s closed door that there was a strong intent to keep clients out, until they were formally invited in. By controlling entrance and the client being nominated as a visitor in this space, the physical healthcare environment limited access in ways that made it clear that the clinic staff were the ones to maintain the ebb and flow of healthcare provision. What the boundaries emphasised then was an underlying us and them; in other words, the division of my space and your space, and the need for an invitation to enter.
In contrast, when healthcare was provided in a residential shelter, the providers were among the clients and physical spaces provided less obtrusive divisions. Some care occurred in the women’s rooms, which removed the physical and perhaps interpersonal barriers. Even here though, office doors had the ability to become half-wall gates and were lockable, should staff be absent from the office or feel the need to have time to themselves away from clients.
Despite these obvious barriers, observation identified positive and open interactions in the formal examination rooms and offices. It seemed that once everyone was in their place at the prescribed time and in the proper manner, the playing field was understood – in that those involved knew their place and role – and participants could begin the business of what brought them together. In such interactions, the women appeared relaxed in dress and posture; they were also interactive and responsive. Healthcare questions were asked, and information seemed forthcoming. Again, there were differences depending on the circumstances that engaged the healthcare provider and the woman. As noted, less structured environments meant interactions could take place in an individual’s room, the staff office, or the hallway. Private spaces often lead to more intimate details of a health need, although this was not an absolute. Although the environments exhibited means of physically controlling interactions, the result was, for the most, an amicable interaction, which was manipulated through the use of space. Interview data supported this finding; see the following quotations: Living here, at [name of women’s shelter], thank heavens for this place. I was able to get off the streets … I have shelter, I’m still left with some money at the end of the month, I still have little ways of making money here and there. And I’m surviving, I get what I need, and in a very safe environment to do it. … They have twenty-four-hour staff, so they protect me from my boyfriend, and from a lot of the drug stuff. … I’m safe here. I’ve been searching for this for many years. I don’t think a day goes by that I don’t tell one of the staff members how grateful I am. Participant J I have my [mental health] worker, I have been just trying to deal with the small things, because I get overwhelmed really fast with stuff. … he’s a very, very good worker, he has been helping me a lot, with mainly questions and stuff here and there, to work on myself. It’s helping a lot. … I don’t think I’d be where I’m at today if I didn’t have the [mental health] worker with me. … He answers questions, and he was the one that suggested coming here. He advocates for me, like this morning, he went to get legal aid for my family court and just other things about appointments because I have a really hard time remembering stuff. He helps me get all that organized. So, it helps a lot. Participant I
Recreational Programs
These observations primarily occurred in a women’s only recreational program. Those who identified as women were invited to participate in the program if they were at risk for bloodborne viral infections; this included women who used drugs and/or women involved in sex work. The program objective was to provide a break from the routines of these practices. The program provided activities, such as crafts, self-care (haircuts), meals, and games with small prizes. The women could also access primary healthcare and the needle exchange program.
The participants dressed casually and appeared relaxed and comfortable in the environment, where they typically gathered around a large central table and interacted mostly with each other, discussing everyday topics such as clothes, food, and weather. There were also conversations about housing, sex work, and drug-related issues. Some of the activities involved preparation for memorials or other events related to PWUD. The women seemed to know each other, and even when they were unfamiliar to the researcher and new to the program, they were known to the other attending women. It seemed there was a closeness in this community of women that was created through their common concerns and issues.
Attendance dropped around cheque day (that is commonly the end of the month when government assistance cheques were issued) and peaked in the days leading up to cheque day. At these latter times, food was the primary focus for those who attended.
Although several staff were present, they often did not interact with the women therapeutically; they started and guided activities and served meals and were available for individual client needs as they arose. On the surface, it seemed that this group was a gathering, like any other women’s group, providing a social and activity-related arena. One might assume that having staff present could assist with conflicts or interactions the women found uncomfortable. Instead, the two groups seemed to be separate and communications were functional and requested rather than interventional. It appeared the purpose of the drop-in for women at risk of bloodborne viral infections was to create a safe space away from the hustle of life on the street. The staff appeared to support women’s activities rather than provide interventional mediation or to intercede in social interactions. Again, interview data supported these findings: I just go down to [name of clinic and services for those at risk of blood-borne infections]. I pick up there, they have women’s day on Wednesday, they have haircuts. … And they have dinners for women. It’s nice, they have a big screen, they play videos and sometimes they have bingo. There are several places that women can take advantage of [name of church#1 drop in for women], … [name of church#2 drop in for women]. … And at [name of clinic and services for those at risk of blood-borne infections], they they give a $30 voucher once every 3 months for clothing, sheets, bedding, whatever you need.… And the community shop is right beside [name of church#1 drop-in for women]. I can go to the [name of church#1 drop in for women] and maybe have a game of bingo, a bite to eat and then go to the community shop and get other stuff. Participant E I usually just go to [name of suburban health centre with a needle exchange program and safer injection site]. I’m usually there, two to three times a week. And they give you coffee and tea and you can volunteer there and they give you money. The draw is once a week, so if you get drawn, like the draw is today, if I get picked today, I work next week and I make twenty bucks, just filling up condom things, or making stems or making the pipes for whatever. It’s a good program. … I come here just to have something to eat and something to do during the day, and to try to stop the constant talking in my head- ‘you need to get it, you need to get it, you need to get it’ Participant AJ
The overall participant observation finding was that WUID are women whose needs and wants are similar to those of all women; that is, to converse, to be social, and to partake in a common meal. There was, however, an underlying aspect of their lives and culture: their drug use and all that the lifestyle entailed, which permeated conversation and determined aspects of attendance. The meeting place provided a common space, safety, and comradery.
Artifacts
Twenty-one cameras were given to women to take photographs of anything they thought related to health. Two cameras were not returned and two sets of photographs were eliminated: in one case, the woman was housed; in the other case, the woman did not use intravenous drugs. In total, we reviewed 17 sets of photographs. Other artifacts included needle exchange program equipment from a public health site, posters and crafts made by women from a recreational facility, and articles published by agencies that advocate for PWUD.
Categories of Artifacts.
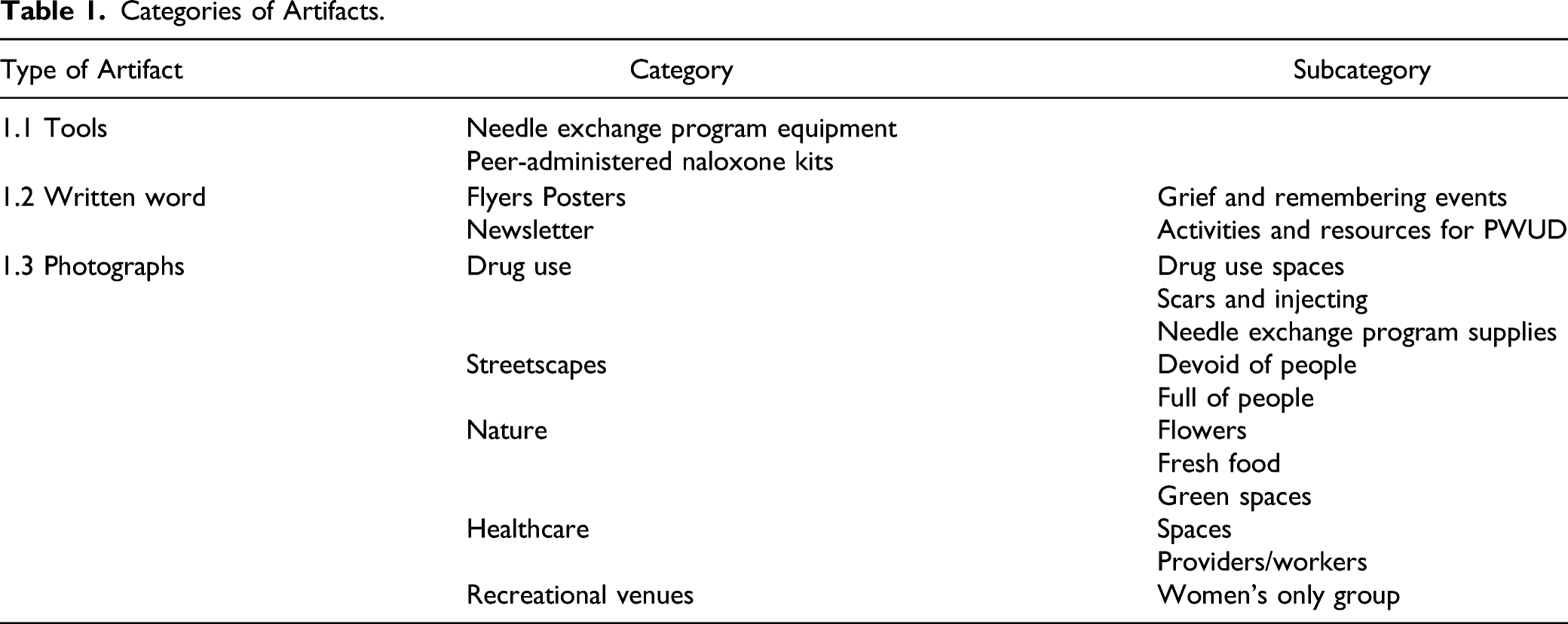
Tools
The tools the participants could obtain included needle exchange program equipment and peer-administered Naloxone kits used for reversing opioid overdoses. This injection equipment was provided to help prevent infection and skin wounds, decrease transmission of bloodborne viral infections, and promote habits for injecting drugs and disposing of equipment that minimize the transmission of these infections (Figures 2 and 3). Needle exchange program equipment with permission from Ottawa public health. Peer-administered naloxone kit with permission from Ottawa public health.

Community agencies provided these tools to help PWUD use injection equipment only once and to provide overdose care for each other. Whilst the needle exchange equipment was supplied by many services, such as shelters, community health centres, and the public health unit, the peer-administered Naloxone kits were distributed exclusively by the public health unit.
The equipment then was provided with an unspoken willingness for healthcare providers to provide harm reducing equipment to those who inject drugs, but with the caveat that this assistance must occur in a distanced and removed manner. Equipment was provided, but PWUD had to take it away to use it. The distributing agency provided equipment to save lives, but it was ultimately the responsibility of the person injecting drugs to use the provided equipment safely as intended and to take the initiative to save others (Naloxone). Injecting drugs and overdosing was to remain hidden, away from mainstream healthcare settings and facilities, which only provided help from what seemed to be the detached sidelines.
These tools were, moreover, packaged and presented in a medicalized format; that is, sterile, standardized, and ordered. This presentation showed a distinction between the ideas of clean versus unclean and the boundaries of order versus disorder. If peer-administered Naloxone was to be an accepted overdose prevention tool and injection equipment was either sterile (e.g. needles, syringes) or clean (e.g. cookers, tourniquets), one must consider how cleanliness – as a concept – was held out as a social and healthcare ideal to those considered by many to be unclean. These objects, the needle exchange program equipment and Naloxone kits, identified a meeting of two cultures: that of healthcare and the lived experience of drug use. How the equipment was used was not revealed by observation but was displayed in some photographs.
Written Word
The items of written words, flyers and posters identified programs and activities for PWUD, a review of which showed that most were provider-led, rather than initiated or organized by PWUD. The exception was a PWUD-led advocacy group, which advertised a weekly breakfast for PWUD. This event was prepared by and offered to PWUD and provided a space to come together and be nourished, both regarding social interaction and food.
With this one exception, flyers and posters promoted events related to the sequelae of being directly or peripherally involved in drug use. Events centred on recognizing the death and grief suffered by PWUD and those who knew them. The advertised events recognized those who had died or suffered through drug use; for example, the International Overdose Awareness Day, Drug User Memorial Day, and the Day to End Violence Against Sex Workers. These events commemorated tragic outcomes and memorialized the deaths and misfortunes PWUD incurred.
In contrast, the aforementioned local peer group, which supported research about PWUD and promoted solidarity and improved conditions for PWUD, produced a newsletter endorsing the belief that PWUD should directly influence the services provided for and to them. Their motto nothing for us without us indicated the need they felt for the voices of PWUD to be heard. Additionally, a health centre initiative to serve PWUD published a newsletter promoting services and events and provided health tips to readers. The newsletter included pieces contributed by PWUD. The brightly coloured, newsy two-page document was written in an informal and welcoming manner, and its harm reduction tone suggested acceptance, respect, and an interest in the health and safety of PWUD. These newsletters were informative and captured some of the issues PWUD face, and did so with involvement from PWUD.
Photographs
The women used photographs to highlight what they thought represented anything to do with their lives and health, and told some of the story of the everyday lives and culture of WUID from their perspectives through these images. Participants’ photographs produced a unique insight into their viewpoints and illustrated the items they felt represented health as it pertained to their lives and lived experiences. This produced a novel viewpoint derived from WUID.
The photographs included (a) places where drugs were used, (b) physical bodily features that identified drug use, and (c) needle exchange program supplies in other environments. As part of this, participants photographed rooms and scenes where drug use was evident. These photographs captured images that were messy and cluttered and which distinctly contrasted with the sterile and ordered world of healthcare. Regarding the signs of drug use, the photos contained images of WUID with scars and abscesses. It was noteworthy that our participants chose to photograph their bodies (without faces) showing evidence of substance use, because, during the observations and interviews, the participants reported or demonstrated efforts to hide these markings. Additionally, the women photographed equipment they obtained and used for injecting drugs. The women may have been expressing the idea that single-use equipment was important when one was trying to be inclusive of what health meant to them. There was a consensus that such equipment aligned with health, and was thus something they should desire, obtain, and use.
Participants also photographed streetscapes that were devoid of connection to human life, giving the appearance of isolation, loneliness, and an anonymous existence. The street was empty in some photographs and in another contrastingly full of unknown, anonymous people, illustrating a sense of isolation, aloneness, and separateness, despite congestion and business.
The sidewalks looked stark and disconnected in their focused gaze. In reflecting on what the experience of homelessness might mean and how it may relate to the photographs, we speculated that there may be a connection with the street as a space where WUID live, i.e., their home, alongside a concurrent sense of not belonging and a fear of experiencing negative and uncaring comments about their lifestyle and embodied drug use from distant unfocused bodies around them. The photographs collectively provided insight into the viewpoint of WUID regarding elements of their lives.
Interestingly, the participants also photographed fresh fruit, vegetables, flowers, and gardens. Nature, as represented by plants and food, are socially understood as healthy. The photographs of plants and fresh foods, then, may have captured participants’ perceptions of a means of being healthy. That is, to eat well and to enjoy the beauty, quiet, and calmness of nature. Alternately, the images may have been a glimpse into what was seen as life outside the culture of drug use. The photographs were taken from a distance, perhaps reflecting the void between homelessness and street life, and between eating shelter meals and the desire to be healthier. These images may, in other words, have been efforts to describe health in terms of an aspired life without drugs, of seeking an alternate life, as was identified in the other components of this research. (For these data, please see Kitson & O’Byrne, 2021; Kitson & O’Byrne, 2020.)
Data analysis also identified that participants photographed places they frequented, such as social service and community spaces. Participants also photographed downtown clinics, a women’s program, a needle exchange program, pharmacies, and a methadone clinic. These photographs also captured WUID and the equipment used. It was in these spaces where interactions between WUID and service providers occurred. The photographs were of places where drug use was more likely to be known and accepted. The healthcare venues, by purpose of the task to take photographs of images reflecting health, seemed to be considered important spaces relating to health.
Absent from the photographs were images of hospitals, ambulances, and uniformed providers (e.g., paramedics). Whilst possibly circumstantial, in that there were no hospitals near the downtown core in our city and/or no ambulances may have passed whilst the participants used the cameras, their absence was notable.
Lastly, participants photographed places where they hung out. Socializing in a safe environment and the need to connect with others thus appeared to be part of what the participants associated with health. In these spaces, WUID could relax and interact socially without the pressures of working, buying or seeking drugs, or being seen by police.
Together, the photographs showed social places and activities that were designed and designated for PWUD. Notable in these photos was that they showed signs denoting acceptance at the entrance: these were spaces that were open for and to PWUD. The images that were taken to show the inside of these spaces captured recreational activities and social engagement. They were seemingly safe spaces that were devoid of references to and reminders of injection drug use.
Taken together, the content of the observations aligned with other aspects of data collection; for example, maps of the examination rooms and waiting areas (such as locked doors as barriers) illustrated the divide between healthcare providers and patients. The space was divided such that a guest (patient) needs an invitation (open door) to enter and is otherwise not welcomed. Our participants’ photographs also provided evidence of a divide between the two worlds, which was additionally consistent with content of the study interviews, whereby comments often reflected the viewpoint of the women being seen as unwanted junkies who desired to lead a so-called socially normal life.
Discussion
As part of our larger ethnographic study about WUID in a downtown Canadian urban centre, we undertook participant observation, artifact reviews, and interviews. In this paper, we reported on the findings from these data collection approaches – with a specific focus on the mute evidence – from which we identified that the lives, practices, spaces, and contexts of WUID were structured but in a manner that differed from the rule bound environments that housed healthcare. In other words, our data showed that regimented and organized healthcare structures differed from how WUID organized their lives. These data raised a few interesting points for discussion.
Firstly, this study demonstrated a need for integrated, flexible models of healthcare for WUID which must be adaptable to their current context and align with their personal prioritization of needs. For example, whilst the WUID in this study often experienced difficulties in attending formal, appointment-based healthcare encounters, they seemed receptive to care that was provided within the spaces and places they were already visiting for services – such as shelters – without the confines of pre-determined check-in times. The need to prioritize the avoidance of drug withdrawal symptoms (feeling dope sick) is well described in previous research with PWUD and should be recognized as a central feature of daily tasks for WUID as well (Motavalli et al., 2021). Adding to the literature is that WUID must also prioritize getting money/capital for drugs to evade the sickness withdrawal creates, which leads to complex and often dangerous situations that negatively impact women’s health. Further, the state of the toxic illicit drug supply (Mayer et al., 2018; Public Health Ontario, 2020; SACEOO, 2021) further emphasizes the need for low barrier, readily accessible nursing services that are acceptable to and create safety for WUID. Our data support such findings.
Secondly, the photographs we reviewed suggest that WUID desire community-based care and have an aversion to impersonal, institutionalized healthcare settings. Participants took photos of local pharmacies and community-run clinics to represent their experiences. None of the photographs contained images of hospitals or emergency services, such as paramedics or police, despite the setting of this study taking place in the downtown core, where ambulances and police frequent. This aligns with the literature that PWUD report stigma and discrimination when accessing healthcare through hospitals and urgent-care clinics (Biancarelli et al., 2019; Chan Carusone et al., 2019; McCradden et al., 2019; Muncan et al., 2020). Our findings reinforce those of Muncan et al. (2020), that, ‘drug use stigma, in many ways, structured the healthcare experiences of PWID’ (Muncan et al., 2020, p. 3 of 9) which can result in delayed care and poorer health outcomes. This stigma has been reported in the literature as findings that healthcare providers hold people who use drugs in low regard and describe them as drug seeking (McCradden et al., 2019; van Boekel et al., 2013).
Thirdly, a need to focus on women’s only activities and programming were highlighted within this study and were of central concern when considering the barriers WUID experience when trying to access care. Women’s only programming appeared to create a safe space where WUID could access basic necessities and perform activities of daily living, such as eating, socializing, and maintaining personal hygiene. Boyd (2004) explored the daily struggles of WUID navigating their substance use, which often revolved around personal safety – women described frequent experiences of sexual and physical violence when using drugs. Although supervised consumption sites offered a safer place to use, researchers have reported that WUID described these settings as masculine spaces, wherein women continue to experience harassment and feelings of vulnerability (Boyd, 2004). Women’s-only programming for recreational, nursing, and healthcare services is therefore likely an important facilitator when considering how to tailor services to WUID.
Study Recommendations.
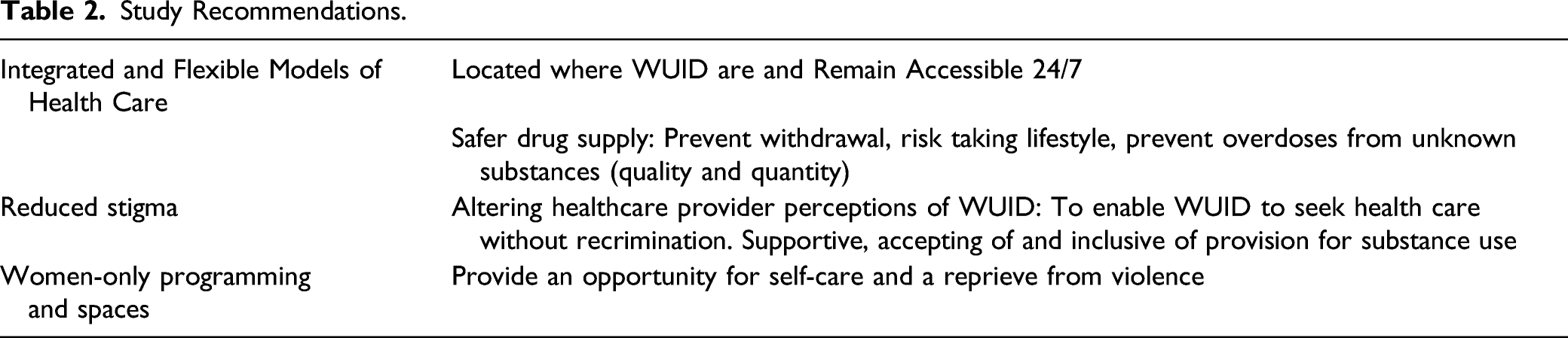
Lastly, the artifacts brought forward in this study demand a reimagining of healthcare services and what nurses can offer. Diagnosis and treatment were not emphasized; instead, safety and control were represented through the presentation of Naloxone kits and sterile injection supplies. WUID care for themselves and others in their communities through these harm reduction approaches, and their healthcare should reflect this. Given the central task of obtaining and consuming drugs each day, it is crucial to ensure WUID have low barrier access to relevant and appropriate services, such as opioid agonist therapies (methadone, buprenorphine/naloxone, slow-release oral morphine, etc.), injectable opioid agonist therapy, and a safer supply of drugs assisted by nurses who embrace the need. Once the basic need to avoid drug withdrawal, WUID may be able to focus on how they want to care for themselves. Our ethnographic data helped identified the items WUID felt described them and their health. These data help inform, in a bottom-up way, conceptualizations of health for WUID. See Table 2.
Limitations
The study was not without limitations. Perhaps most important here is the absence of the women’s spoken voices about the photographs and artifacts we collected. Whilst interview data were collected, these did not focus on the muted evidence. Our purpose here was to examine what the muted data were able to contribute to our knowledge about WUID and their experience of health and healthcare. Focusing on participant observation and artifacts may have limited the opportunity to hear their words, but the women have communicated in other meaningful ways. The artifacts have provided items that enable a different approach to furthering an understanding of the lives of WUID. The photographs provide wordless images that clearly portrayed some of what the women believed represented their health. Additionally, the opportunity to complete member checks, that is reviewing the interpretation of the transcript with participants to ensure agreement (Carspecken, 1996; Hammersley & Atkinson, 2019), was not available due to ethical concerns. The need for these checks to strengthen validity/credibility has been noted (Carspecken, 1996; Denzin, 1994; Lincoln & Guba, 1985; Speziale & Carpenter, 2007). However, there is also discussion of alternatives to traditional member checking, such as prolonged engagement in the study setting (Padgett et al., 2004). Informal discussions WUID leant credibility to the findings as their words reinforced our interpretations. This immediate checking may be more useful as delays in a request for interpretation can change findings due to intervening circumstances and evolving perspectives (Hammersley & Atkinson, 2019; Horsburgh, 2003; Janesick, 1994). Additionally, ethnographic research methodologies often use artifacts as muted evidence (Hodder, 1994), further signalling that member checking is not necessarily required. As such, this study yields new insights about WUID.
Conclusion
The participant interviews, observations, and artifacts discussed herein provided a rich description of the subjective lived experiences and perceptions of health among our sample of WUID, which adds to the existing, albeit sparse, literature on Canadian women experiencing homelessness who inject drugs. Their lifestyle, one that sidles between two worlds, the world of drug use and the world the women viewed as ‘normal’, creates a chasm such that, when the two cultures meet, there is a need to adjust, to reconsider, and to adapt. If nursing is to help bridge this divide, there needs to be an acceptance and an understanding of the lives of WUID, and an attempt to meet on a common ground that meets the needs of WUID. The artifacts and observations examined here can help increase our understanding and assist in the development of culturally sensitive nursing care for WUID. The proposed recommendations, as described above, may go far in achieving this need and enhancing the overall health and healthcare of WUID. In this way, we can turn our attention from moralizing and criminalizing drug use, and instead focus on how to provide effective healthcare for WUID. Whilst societal changes may occur over a prolonged period to address the balance of who receives nonjudgmental and equitable healthcare, certainly the more immediate and malleable change should come for healthcare providers, and in particular nurses regarding how they go about the business of providing services. In other words, we hope for larger societal changes, but aim for more immediate changes to help improve care and the lives of WUID in the short-term. We hope our findings can contribute to some such changes and some such improvements in the lives and experiences of WUID when seeking and obtaining nursing care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.