
Abstract
There is a paucity of research examining children’s experiences with cancer in India. Childhood ethics is an emerging field, focusing on the moral dimension of children’s experiences, to promote children’s participation in their health care. A focused ethnography, using a moral experience framework, was conducted to better understand children’s participation in decisions, discussions, and actions in three oncology settings in New Delhi, India. We interviewed key informants, retrieved key documents, and conducted semi-structured interviews and participant observations with children. All 22 children demonstrated interest in varying aspects of their cancer care. Certain factors facilitated or impeded their participation. Some children became distressed when they lacked information about their treatment or were not given opportunities to enhance their understanding. The results advance our understanding of the moral experiences of children with cancer in India for healthcare professionals, policy makers, families, and interested others.
Introduction
Childhood cancers account for 2% of all cancers, with as many as 198,700 newly reported diagnoses globally in 2018 among children age 0 to 14 (American Cancer Society [ACS], 2018). Eighty-two percent of these diagnoses come from low- and middle-income countries, such as India (ACS, 2018). Generally, childhood cancer has not been a targeted health priority in India (Arora et al., 2009). Rather, the priority has been the prevention of communicable diseases (Choudhury, 2007), which has resulted in a steady decrease in the under-five mortality rate (World Health Organization [WHO], 2015). Consequently, the proportion of under-five mortality due to non-communicable diseases, such as cancer, has increased (WHO, 2015). Cancer causes 2.9% of all childhood deaths for children aged 5 to 14 years in India and was ranked ninth in 2003 among causes of death. However, childhood cancer was ranked the first cause of death due to non-communicable disease in this age range (Office of Registrar General India Ministry of Home Affairs, 2003).
Gaps in the Literature
Only one study has been conducted to examine the experiences of children with cancer in India using their own perspective, and no studies discussed how experiences are affected by the local context and clinical practices (Behan et al., 2021; Sharan et al., 1995). However, understanding children’s perspectives has been an important focus in the international literature (Coyne, 2008; Day et al., 2016; Kelly et al., 2017). To our knowledge, Sharan and colleagues led the only study identified in India and was conducted with children with acute lymphoblastic leukemia in New Delhi. Sharan and colleagues reported that the child’s disease awareness did not relate to psychiatric morbidity. Three of 39 children informed of their illness did not experience negative psychological outcomes resulting from this knowledge and 61% of the children expressed emotional distress in their stories (Sharan et al.,1995). The health experiences of children in general have been under-examined in India. A scoping review of children’s health-related experiences in India revealed some of the ways that their lives have been affected by chronic illness, but none of the studies captured young people’s actual or desired participation in healthcare discussions or decision-making (Behan et al., 2021). This topic has been explored in high-income countries and highlights the fact that children wish to be involved in their healthcare and can have the capability to express their ethical views, yet frequently confront barriers to participating in their own care (Coad & Shaw, 2008; Coyne, 2008). It is unclear how much of this Western-dominated evidence is transferable to an Indian context, given how little is known about the latter. The term “capability” refers to children’s abilities to: (a) understand information regarding their health care and how various treatment options would affect them, and (b) form preferences for treatment options that best align with their interests (Carnevale et al., 2020).
Childhood ethics is an emerging field of inquiry examining children’s experiences and the moral dimension of children’s experiences (Carnevale et al., 2015; Soderback et al., 2011). Moral experience is defined as, “Encompassing a person’s sense that values that he or she deem important are being realised or thwarted in everyday life. This includes a person’s interpretations of a lived encounter, or a set of lived encounters, that fall on spectrums of right-wrong, good-bad, or just-unjust” (Hunt & Carnevale, 2011). Children’s moral experiences are being examined increasingly to promote the recognition of children’s participation, inclusion, and agency within a variety of contexts, including health care. As we move away from the views of children as passive recipients, so too, must we (as adults) move away from depending exclusively on statements from adults about children’s experiences, which warrants the focus on accounts from children themselves (Bluebond-Langner & Korbin, 2007).
Theoretical Underpinning
The study was oriented by a moral experience framework, which is used to understand individuals’ unique perspectives regarding their experiences within a local, social world (Hunt & Carnevale, 2011). The framework is based off of Charles Taylor’s (1985) socially based conception of hermeneutics, which posits that “a person’s self-understanding is always situated within a horizon of significance that orients what is considered as moral” (Montreuil & Carnevale, 2018, p. 2). Horizons of significance shape how things have meaning for persons and how they may value particular aspects of their experiences. To understand moral experience, it is important to examine the multiple layers of horizons of significance, including the macro- (historical, political), meso- (community, social), and micro- (family, identity, school) levels (Hunt & Carnevale, 2011; Kleinman & Benson, 2006). Thus, both the personal experience and the individual’s broader context are crucial when utilizing the moral experience framework. Previous studies have used moral experience as a guiding framework, including the moral experience of families with ventilator-assisted children (Carnevale et al., 2006), of children with HIV/AIDS in rural Tanzania (Sebti et al., 2019), of pediatric nurses in Brazil (Passos dos Santos et al., 2019), among others. To the best of the authors’ knowledge, no studies within the field of psycho-oncology have been conducted explicitly using a moral experience framework.
Aim of Study
The aim of this study was to use a moral experience framework to better understand the actual and desired participation in decisions, discussions, and actions among children with cancer in New Delhi, India.
Methodology
Methods
To achieve the above aim, a focused ethnography was conducted (Cruz & Higginbottom, 2013; Polit & Beck, 2012). Ethnography has its roots in anthropology and aims to understand the ways of life of a population by using local knowledge, contexts, and understandings gained from immersion in the target culture (Cruz & Higginbottom, 2013; Polit & Beck, 2012). Focused ethnographies are time-limited exploratory studies examining socio-cultural communities in their “natural” settings, enabling the researcher to better understand phenomena as they are practiced, not only as they are disclosed verbally.
Settings
In order to include diverse experiences, the study was conducted in three settings: (1) a pain and palliative care unit for children with cancer funded by a non-governmental organization (NGO hospital); (2) a pediatric oncology unit in a private hospital (private hospital); and (3) a pediatric oncology unit in a public hospital (public hospital), all within New Delhi.
The NGO hospital is a 10-bed hospital which is financially supported and run by a non-profit social support organization. The in-patients at the NGO hospital, as well as many other children with cancer in Delhi, benefit from the social-support programs it offers. Those admitted to this hospital who are still actively receiving treatment, are typically also attending a public hospital as out-patients for treatment while remaining in-patients at the NGO hospital. Certain patients at the NGO hospital have no remaining curative treatment options and are admitted for palliative care in order to obtain the best possible end-of-life care. Other pediatric cancer patients are seen at this hospital on an out-patient basis for medication administration, such as to receive antibiotics infusions to treat febrile neutropenia. All services are offered free of cost.
The public hospital has a high patient volume. During out-patient days, oncologists will see an average of 150 to 200 pediatric oncology patients with scheduled appointments per day. Each year, approximately 700 new pediatric oncology patients between the ages of 0 and 18 years old are consulted here. At the time of data collection, there were eight consultant oncologists, but only one pediatric oncologist who is assisted by junior and senior residents. Within the oncology department, there are seven in-patient beds for use by the pediatric oncologist, which are typically used for patients who require hospitalization during chemotherapy. Access to approximately 8 to 10 additional beds is available to pediatric oncology patients through the emergency department (depending on availability), which are used for oncologic emergencies. The remainder of the patients are managed on an out-patient basis, through an innovative and successful out-patient management program. The bulk of the direct healthcare service provision at the public hospital is provided at no to minimal cost to the patient.
The private, for-profit hospital sees approximately 50 to 80 new pediatric oncology patients each year. The patients either pay for services out-of-pocket or via three different types of insurance, which are private insurance, public/employers’ insurance, and insurance provided to those who are determined to be below the poverty line. Additional services that are provided to the children include nutrition, psychology consults, physiotherapy, and support groups.
Ethics
This study adhered to the Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans (TCPS-2; Canadian Institutes of Health Research, 2014), meeting approval of McGill University Institutional Research Ethics Board (A08-B24-16A) and the Institute Ethics Committee All India Institute of Medical Sciences (IEC-495/07.10.2016, RP-24/2016), Gene Bandhu Institutional Ethics Committee for CanKids India (ECG002/2016), and the Institutional Ethics Committee Max Healthcare Super Speciality Hospital (RS/MSSH/SKT-2/ONCO/IEC/16-11). Child assent and written parent/adult consent were obtained for all participants prior to data collection. No compensation was provided. All data were anonymized and kept confidential.
Participants and Recruitment
Purposive sampling was used to recruit study participants and key informants. A key informant is an individual who is “knowledgeable about the phenomenon of research interest and who is willing to share information and insights with the researcher” (Polit & Beck, 2012, p. 732). The aim of consulting key informants was to gain access to the community, gather an understanding of the community, learn about social and political influences on decision-making practices, choose sites and methods for data collection, become informed of potential key documents, and gain a preliminary understanding of moral experiences of children within the settings. Key informants primarily included healthcare providers working in pediatric oncology in New Delhi and young adult childhood cancer survivors. Key informants were recruited with guidance from stakeholders that the research team was already familiar with. Their role included providing local experience and advisory expertise on optimal ways to conduct participant recruitment, as well as, data collection, analysis, and interpretation. They also helped to identify relevant key documents (further described in the data collection section). Continued recruitment and consultation with key informants occurred throughout the course of the study. Data from key informants, such as their input, knowledge, and advice regarding the study, hospital documents, healthcare and community practices, and personal experiences/perceptions toward children’s health-related experiences, were collected only after signed informed consent was provided.
Inclusion criteria for study participants were: (a) a diagnosis of any cancer; (b) between the ages of 3 to 17 years old at the private and public hospital and ages of 5 to 17 years old at the NGO hospital; (c) able to speak Hindi or English; (d) receiving or have received care from any one of the study sites; and (e) in any phase of their illness trajectory such as a new diagnosis, treatment, palliative care, and/or remission. The study focused on young people above the age of 3 years, as we wished to target children who were able to speak about their experiences. The age of 17 years was the maximum age, as 18 years is the age of majority in India, which affects their legal rights to participate in decisions regarding their care. Young people in remission or survivors were included as potential participants as they could speak about their treatment, ongoing monitoring, and long-term follow-up. Participants were excluded from the study if healthcare professionals at the study site had concerns that participating in the study could pose a risk to the participant. At the NGO hospital, participants were also not approached if they had received their diagnosis within the past month. The slightly differing criteria for the NGO hospital were based on the recommendations of the institutional ethics committee of this site.
Recruitment of child participants was done by the student researcher at the private and NGO hospitals and by a staff research nurse at the public hospital. A person within the healthcare team at each site provided recommendations of eligible participants. The student researcher or research nurse were directed to those eligible to participate to explain the study, seek consent from parents/guardians, and seek assent from the child participants. Children gave verbal assent (with a witness present) if they were between 3 and 12 years, and either written or verbal assent (based on their preference) if they were between the ages of 13 and 17 years. At this time, demographic information about the child and family was also collected from participant’s parents or legal guardians, such as their relationship to the child, the child’s age, diagnosis, child’s level of education, information regarding child’s treatment and other health problems, language, and religion.
Data Collection
In preparation for the data collection period, the first author (Justine Behan)—a master’s student at the time—spent approximately 1 month visiting the healthcare settings to: (a) understand the specific routines of each setting; and (b) allow people in these settings including the members of the healthcare staff to become more familiar with the presence of the student researcher. Following this, the student researcher collected data during 3-months of field work (September 2016 to December 2016). Data collection methods included participant observation and field notes, interviews, and key document analyses (Cruz & Higginbottom, 2013; Polit & Beck, 2012). Participant observations were sought to include children during various interactions such as medication administrations, activities, and physician consultations. The observed events were chosen in order to provide insight toward the experiences of children in a pediatric oncology setting, particularly related to children’s interactions with family, healthcare providers, and other staff/adults, and their involvement in discussions, decisions, and actions. Participant observation data were recorded with field notes with children’s assent and parents/guardians’ consent. No data were collected from health care professionals who were in the field of view during the observations as they were not the primary informants.
The moral experiences framework and prior moral experiences research guided the development of two interview guides used to conduct the semi-structured interviews with the children in their preferred language of Hindi or English. One of the interview guides was designed for the young children up to and including primary school age, and the other was designed for secondary school aged children. The interview guides were further adapted in consultation with key informants, such as young adults that had cancer as children in India. The key informants confirmed that the interview guides were adapted and well-suited for the participants. Examples of questions asked include: “Can you tell me about your current hospital stay, or the most recent time you went to the hospital/saw a doctor?”; “What did you like or not like about experience?”; “Can you describe a situation (involving you or others around you) where you participated in discussions, decisions, and actions regarding your health?”. Please see the supplementary materials for the interview guides.
The use of interpreters for Hindi speaking children was necessary during the interview process as the student researcher did not speak Hindi. Efforts to mitigate the potential drawbacks of using interpreters entailed incorporating the strategies proposed by Temple and Young (2004) and Sleptsova et al. (2014). These strategies included: (1) having ongoing, mutual consultations between translators and researchers; (2) ensuring both parties clearly understood the project goals; and (3) allowing both parties to discuss differences in perceptions, particularly through the interpreter’s role as a “cultural broker” in helping professionals to better understand cultural differences. Two interpreters, who were both actively involved in the project, were primarily used. One of the interpreters was a pediatric oncology nurse, and researcher based in New Delhi, and a study co-author. The second interpreter was a master’s prepared researcher employed by the private hospital to conduct pediatric oncology research, and had a strong understanding of the study context. There was one additional interpreter used for one interview when the two primary interpreters were unavailable. All interpreters were given information on the study prior to conducting interviews and had frequent contact/ discussions with the student researcher in regard to the study.
The study team deferred to the family’s preference as to whether the child was to be interviewed alone or in the presence of the child’s parent(s). When interviews were conducted in the presence of the parent(s), the interviewer explained that the aim of the study was to hear the child’s perspective and parents were given an opportunity to speak at the end of the interview. The student researcher recorded parents’ involvement during the interview in field notes. All but one interview was done in the presence of at least one family member. The interviews were audio-recorded with parental and child permission. None of the participants in this study declined to be audio-recorded.
The third data collection method was analysis of key documents, which included local written materials considered by key informants as reflective of the community context or practice standards (Polit & Beck, 2012). Examples of key documents included: community documents regarding children; documents regarding the care of children at the study sites such as pertinent hospital protocols, practice standards, and position statements; codes of ethics; and any other texts identified by key informants. Key documents were analyzed to determine how children’s voices should be heard, and to gain insight into how children’s best interests and moral agency, which are central concepts in childhood ethics, were implicitly or explicitly understood or practiced within pediatric oncology settings in New Delhi (Carnevale et al., 2015). A summary of this analysis is in Table 1.
Summary of Key Texts and Other Contextual Factors at Settings.
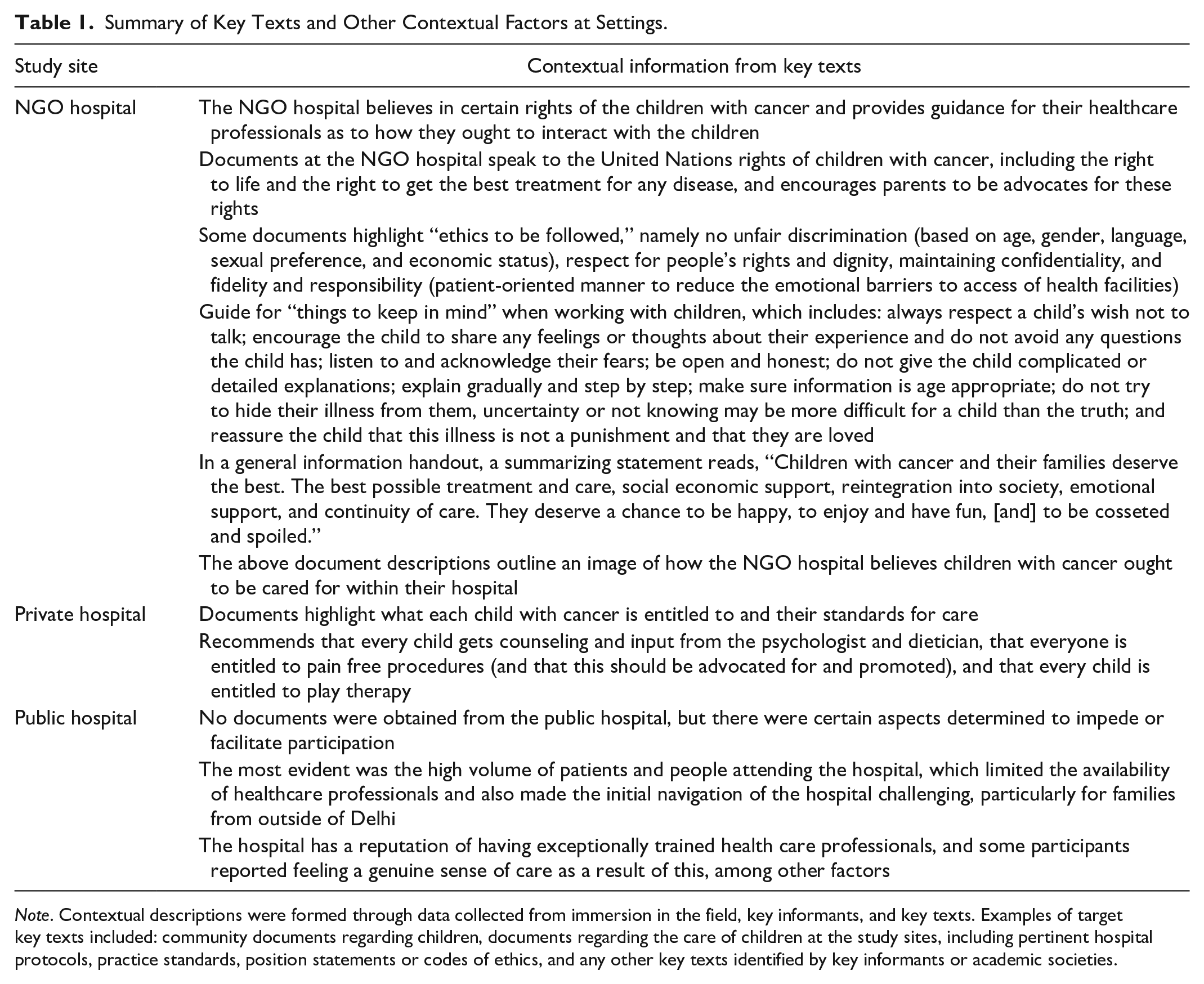
Note. Contextual descriptions were formed through data collected from immersion in the field, key informants, and key texts. Examples of target key texts included: community documents regarding children, documents regarding the care of children at the study sites, including pertinent hospital protocols, practice standards, position statements or codes of ethics, and any other key texts identified by key informants or academic societies.
Data Analysis
All data were transcribed verbatim by the student researcher who used Microsoft Word and Excel to manage and analyse the data. The data analysis was iterative, inductive, and continuous and was conducted in three phases (Polit & Beck, 2012). The first phase included consolidation and coding of all data derived from field notes, transcripts, and analytical notes from analysis of key documents, as well as any necessary clarification of information with participants. Initial open coding, a method through which codes (units of analysis) are generated through careful reading of field notes, analytical notes, and transcripts, was done (Benaquisto & Given, 2008). The student researcher used the research question, “What are children’s actual and desired participation in discussions, decisions, and actions in a pediatric oncology setting in New Delhi, India from September to December 2016?” as a guide to code the data. Subsequently, the key texts were tabulated, categorized per topic, and subsequently analyzed by taking detailed notes of what was considered good/bad, right/wrong, fair/unfair in the documents, which was guided by the following questions: In which situations involving children must it be determined what is the right/right, good/bad, or fair/unfair thing to do?; What matter is in question?; Who is involved?; How do norms/policies state the matter should be addressed?; How actively are children’s voices portrayed; and How are children’s best interests conveyed?
The second phase involved categorization of codes within sources and between sources (between the data from participant observation, interviews, and analysis of key texts), generation of questions for subsequent data collection, and ongoing consultation between the student researcher, the research team members, and key informants. The ongoing consultations allowed the student researcher to identify and discuss any personal biases during data analysis, ensuring the credibility of the research, as well as gain valuable insights toward cultural nuances that may have been overlooked.
The third phase of the analysis included axial coding (relating categories to each other), thematic analysis (organizing categories into themes), and comparative analysis (drawing connections between categories) (Polit & Beck, 2012; Wolf, 2012).
Results
The researcher spoke with many stakeholders and formally interviewed eight key informants, consisting of healthcare professionals, childhood cancer survivors, and young adult cancer patients (Table 2). Twenty-five eligible participants were approached for participation in the study and 22 consented. Two participants who were approached did not participate as they were deemed “too shy” to give verbal assent. In both scenarios, the parents were willing to provide consent for their child to participate, but due to time limitations of out-patient visits, the researchers did not have enough time to try different engagement strategies with these two children. Seeking a diversity of perspectives, participants were of varying ages, diagnoses, and experiences. Five of the participants were female and seventeen were male. Age and diagnosis of participants are found in Table 2. Each participated in a semi-structured interview, which lasted between 5 and 30 minutes, depending on the participant’s age and engagement. Eleven participants were observed through participant observation (Table 3). Participant observations lasted approximately 5.5 hours collectively and took place one to several times for each participant throughout the data collection period, based on the participants’ availability. Identified key documents were analyzed to further inform our contextual understanding of the three study sites which are outlined in Table 1.
Key Informant (n = 8) and Study Participant (n = 22) Characteristics.

Note. Diagnosis categories based on the International Classification of Childhood Cancer from Steliarova-Foucher et al. (2005).
Overview of Data Collection via Semi-Structured Interviews and Participant Observation.

Note. Total immersion in study settings was 3 months.
Children’s Actual and Desired Participation: Decisions, Discussions, and Actions
Children had a variety of experiences regarding their participation in decisions, discussions, and actions that affected them. In some cases, children preferred that decisions be made for them, whereas others desired involvement in health-related decisions. Some children, regardless of age, were distressed by their exclusion, particularly when they were lacking information and were missing an opportunity to further develop their understanding of their illness. The extent to which each child participated varied widely. Their expressions of preferences or engagement in activities that they were comfortable with seemed to be a starting point for participation. Certain factors, such as the healthcare professionals’ (HCP) attitudes, were found to be facilitators for participation; whereas barriers included the environment, unfamiliar settings, and the presence of cancer symptoms. Selected verbatim quotes were used to illustrate participants’ disclosures. Some translated quotes are in the third person and presented in the manner they were stated by interpreters and transcribed by the researcher.
Participation and capability for decision-making
Children demonstrated capabilities to participate in decision making, but were often excluded. At times, this exclusion contributed to heightened feelings of distress. They relied on their parents as primary treatment decision makers, who made decisions that they considered favorable and unfavorable for them.
Children’s exclusion from treatment-related decisions despite demonstrated decision-making capability
No children were observed or expressed being directly involved in treatment-related decisions. Participants relied on their parents as their primary treatment-related decision makers, and in some cases indicated their decision would have differed. Yet, they also displayed an understanding of their parents’ decisions. For example, one child explained: “. . .how can you take this decision. . .I am taking the IT the injection, intrathecal, in my spinal cord, so so I say that I, I do it in the sedation, but my mom and dad not (P#6, age 14, English interview).” Despite disagreeing with his parents’ decisions to opt for intrathecal injections without sedation, the child explained he would have done the same thing if he was in his parents’ position because of time constraints. This family was traveling from outside of Delhi. If the child received sedation, they would miss their train home. This highlights the participant’s capability to reason and understand his parent’s decision, and desire not to impose further financial burden by staying overnight. He demonstrated regard for others in his moral reflections.
Children’s exclusion from decision making and the opportunity to assent to treatment led to some difficult experiences. One participant, who was 1 week post lower leg amputation, expressed, “The doctor didn’t share with me about the surgery” (P#16, age 15, interpreted from Hindi). The child was not involved in decisions leading to his leg amputation, and only learned of the decision the morning of his surgery from his surgeon. He expressed feeling very sad at that time, and explained how he would have definitely made different decisions, but did not further elaborate. Given the expressed emotions and the emphasis placed on the undisclosed information, this child appeared clearly distressed by his exclusion.
Regarding their decision-making capabilities, participants expressed their food and temporary housing choices and discussed how the latter could affect the entire family. A participant said that if he was given an opportunity to decide, “I will choose the good things. . .to live, good place to live and good food to eat, good care” (P#22, age 15, interpreted from Hindi). Another participant recalled the challenges at the start of his illness, when his family first came to Delhi, “His legs weren’t working, his hair was falling off, so that time he was really sick and they had to figure out where to go” (P#8, age 12, interpreted from Hindi). It became clear that having a free and safe place to stay—one that could provide everything he and his family needed and avoid further financial burden—helped the participant feel better.
Children relied on their parents as primary decision maker
Participants reported that their parents, extended family members, and/or physicians made the treatment decisions. One child felt irritated that his parents were making the treatment decisions, but upon reflection recognized that decisions made for him were favorable for his health (P#6, age 14). Another child did not feel good about his father’s decisions regarding his cancer and stated, “I will choose the right way, good care” (P#5, age 15, interpreted from Hindi). In the context of decision-making children wanted “good things.” They talked about wanting good cancer care, food, and housing. Participants described how quality of care was important for them.
Discussions: children had varying engagement
Children engaged in discussions in varying ways. Some children felt their voices were listened to, whereas others did not voice their questions, or felt their questions were unanswered. Participants identified barriers that they faced in being able to “speak up.” The children spoke of their health concerns with various people, including their family members, nurses, physicians, other HCPs, friends, and children—including their siblings and other patients. Many children explained that they would speak with one of their parents if they had any concerns. Discussions with adults led to: (a) concealing or feeling good about their concerns and (b) developing varying understandings of their illness.
HCPs may foster or thwart children’s participation in discussions
Children’s willingness to ask questions was both favorably and unfavorably affected by HCPs’ attitudes and their feelings at the time of interaction. One participant stated, “The starting of the chemo I had questions. I asked [physician’s name] and he answered. It all went along” (P#3, age 15, English). In contrast, another participant stated, “She asked to the doctor, ‘why my legs and my hands are not working’, the doctor didn’t give any reply and he goes” (P#7, age 10, interpreted from Hindi). When the participant was asked how she felt when this happened, she responded, “Very bad.” This feeling of sadness was also present when a child felt there were barriers to asking questions he had, “Why the cancer occur? [. . .] the environment, and depression also, is stopping me to asking any question to the doctor. New doctor, new hospital” (P#6, age 14, English).
When children perceived their physicians and nurses to be “friendly,” they felt comfortable and were observed initiating and asking them questions without hesitation. Many children from ages 5 to 17 years reported feeling good or feeling better after speaking with their nurses or physicians, and engaged in discussions with HCPs who were “friendly” and “speak nicely.” One participant recalled his conversation with a psychologist who counseled him about his depression, gave him games to “pass his time” at the hospital, and shared stories of other people who had cancer including celebrities (P#6, age 14). This encounter helped the participant feel better and encouraged.
Children relied on their parents to facilitate discussions with HCPs
Children had various health concerns, which they would often share with one of their parents who would then communicate these concerns to HCPs. For example, one participant said she would tell her mother if she had any questions, both at home and at the hospital (P#5, age 7). Her mother would then facilitate the communication for her shy child, which was observed through participant observation. Two participants explained that usually their father speaks to the HCPs, and that they in turn speak with their father (P#8 and P#9, ages 12 and 10).
Children shared their concerns with other patients
Some of the participants recalled speaking with other patients. Being in an environment with other people with cancer helped them to speak more openly. Because everyone around him had cancer, one participant felt he could speak freely about his cancer (P#3, age 15). Another participant spoke about her experience as a patient on an adult ward. She did not like being on the ward with no one her age; however, when patients would speak with her, she said that she felt good (P#11, age 11).
Children averted discussions about their cancer
Children had a lot of questions, concerns, and assumptions about their cancer and sought to discuss these concerns with their HCPs, parents, and other patients. Depending on adults’ willingness to engage with the child, discussions were thwarted or revealed children’s views. Some of their concerns were particularly profound. For example, one 10-year old participant expressed concern about his own mortality. He was hesitant to ask questions or initiate this discussion with his HCPs. He attributed being “very sick” as a barrier to initiating a discussion about his prognosis. In contrast, a physician, who recognized the child’s capability to understand, discussed the diagnosis and treatment with the child. While the child welcomed this discussion, he remained “very sad” because he still did not understand why the cancer occurred. He added that the conversation helped him to “build up his patience” to take and tolerate the chemotherapy (P#6, age 14). Other children hid their concerns from their parents. These children felt isolated as they tried to protect the well-being of their parents. One participant described needing to be courageous otherwise his mother would break down emotionally. Some children were never directly told about their cancer. One participant stated, “Nobody has told me.” She recalled the story of how she came to know she had cancer: When I was ill for the first time in [city in India] I was in pain [. . .] I was under the chemotherapy session in the chemo room [. . .] I was unaware till then because we never knew about the disease and neither had any idea of the consequences and the procedures. Suddenly the nurse asked me which kind of cancer I was suffering from. That was all of a sudden, then I asked these people about my illness. Then I thought that if in case I am suffering from such a disease also I should not be asking my parents about it. They might be already troubled and tensed and me asking about it again to them would make them more tensed and disturbed which I never wanted to do [. . .] I came to [hospital name] [. . .] I came to the cancer department of the hospital for the first time [. . .] the dietician of the hospital she spoke to me. She told me what kind of cancer I have. The type is ALL and will be cured with treatment [. . .] (P#13, age 17, translated from Hindi).
Children had varying understandings of their cancer
Children’s capability to understand their illness was clearly evident. Many children, as young as six, stated explicitly that they had cancer, showing an awareness of their illness, even in cases where they had not been told directly. For example, one participant (P#8, age 12) displayed a good understanding of his lab values and discussed whether a blood transfusion would be necessary prior to his next chemotherapy. He knew exactly when his next chemotherapy was scheduled, who his dad had spoken to, and what was happening with his care. It was common for many children to know their precise schedules, when they had appointments, and what would happen at the appointments.
Some participants described their beliefs regarding their illness and their expected treatment outcomes. One participant shared her beliefs about the functioning of her hands and legs with the onset of radiation: “[. . .] before that starting radiation, she was thinking if I take the radiation my hand and my leg will be work, but these are not working” (P#7, age 10, interpreted from Hindi). After surgery, the participant learned of the tumor involvement in her spinal cord and that she may not regain function in her extremities; however, she maintained her initial belief. Another participant described her illness as a blood infection. She explained that her blood would be replaced with new blood; once complete, she would return home (P#11, age 11). One participant attributed her illness to “God’s wish and his will,” and drew meaning from her family’s cancer experiences with her great grandfather and grandfather (P#13, age 17, translated from Hindi). Hence, children created their own interpretations of their illness, particularly when they were not given explicit information.
Actions: Children participated in a variety of treatment and non-treatment-related actions
Children’s actions in the settings were shaped by various factors. Participants’ parents were observed encouraging “polite behavior,” possibly shaping how the child was supposed to behave. Some children seemed to be taught by “modeling.” For example, one father modeled wearing the oxygen saturation monitor for his child (P#5, age 7). Previous experiences were also shown to affect children’s actions. Children who had undergone radiation therapy multiple times went about receiving the treatment in a calm manner, as if they were experts.
Children engaged in actions in their cancer treatment and therapy
Children assumed the role of treatment receiver, which included bearing a number of painful injections during chemotherapy administration and consequently feeling “bad.” One child described it as, “I just have to sit there and bear the pain” (P#3, age 15, English), whereas a 3-year-old participant pointed to his bandage, where he had received an injection earlier that day. An older participant on maintenance therapy indicated chemotherapy was a painful experience, but had a greater appreciation of the benefits now (P#13, age 17).
Children engaged in play/entertainment with themselves and others
Children expressed that play and entertainment helped them feel happy. Children participated in play with others or themselves, and often played with electronic devices. When one participant was asked what he liked best about the hospital, he shouted, “Playroom” (P#2, age 3, English). Many children, regardless of age, recalled their enjoyment of playing with electronic devices, which helped pass the time and seemed to make living with cancer somewhat easier. At one hospital, the TV room served as an area for children and parents to spend time, watch TV, and speak with one another.
Children also described their experiences of exclusion from play or the inability to play in the same way they could prior to their illness. For one participant (P#7, age 10), her interactions with her friends changed following her diagnosis. Another participant felt excluded during his hospitalization because nobody invited him to play (P#9, age 10). Another participant described that he was unable to engage in certain activities after his leg amputation, “[. . .] right now I can’t play games because I can’t walk and I can’t jump and before the disease I was like to play hide and seek and catch” (P#21, age 9, interpreted from Hindi).
Continuing education, or not, while undergoing cancer treatment
All participants had stopped attending school at the onset of their cancer trajectory. Some returned once they started maintenance, continued studying, or wrote exams. Others continued attending school until they were not well enough to go. The following highlights some of their experience. One child’s friends were curious about him missing school. He eventually told them everything about his illness, and felt his friends were fine with it (P#3, age 15). Another participant explained that an organization was helping him to continue his education throughout treatment (P#9, age 10). One participant described being corporally punished for his poor attendance before his teachers learned about his cancer. When he explained to his teachers about his cancer, they asked about his treatment, and it then became easier for him (P#6, age 14). By knowing about his illness, he could explain to his friends and teachers why he was absent and gain their support, rather than be punished for his absences. Key informants explained that many children feared returning to school because of the stigma of having cancer, highlighting that openly disclosing their cancer was not a positive experience for all children. One of the survivors explained that when she returned to school after her cancer treatment, she went to an entirely different school to avoid telling anyone that she had cancer.
Discussion
As this study addressed an under-investigated domain with a heterogeneous sample, the results highlighted the diversity of children’s perspectives and did not aim to generalize. The results revealed a range of ways in which children of various ages and illness trajectories experienced their inclusion or exclusion in decisions, discussions, and actions that affect them. Whereas some children preferred to have decisions made for them, others desired involvement in their health-related decisions. Some children, regardless of age, were distressed by their exclusion, particularly when they lacked information about their treatment, were excluded from opportunities to further develop their understanding, and/or were prevented from sharing their views, preferences, and input on major decisions. All children demonstrated capabilities for and interest in participation in aspects of their care. However, the extent to which each child actually participated varied widely. Certain factors facilitated children’s participation, such as the HCPs’ attitudes, while others impeded their participation, such as the environment, unfamiliarity with the setting, and/or severity of cancer symptoms.
The minimum level of participation that children engaged in was the expression of their preferences. Preferences have been described as a precursor to the act of participation, which can relate to a person’s previous experiences and can motivate participation (Imms et al., 2016). Children as young as three shared their preferences with ease, especially through play, an activity experienced before their cancer diagnosis. Similarly, children who had previously undergone a treatment were able to express their preferences in relation to that treatment. For example, children voiced preferences regarding sedation during intrathecal injections, injection sites, and the size of bandages needed after an injection. This aligns with research conducted outside of India, which has demonstrated that a child’s previous experiences contribute more to their understanding of their illness than their age (Bluebond-Langner, 1978). More recent research has also shown that illness conditions, such as the stage of treatment or presenting symptom distress, orient children’s communication preferences more than their ages (Kelly et al., 2017).
A systematic review of the literature on adolescents with cancer highlighted the importance of understanding their participation in treatment decision-making (Day et al., 2016). This knowledge can help reduce the possibility of increased or prolonged suffering resulting from practices that do not align with patients’ needs or preferences (Day et al., 2016). Similar views have been reflected in the Indian literature, such as by Seth (2010), who argued that research on culturally-adapted communication is needed in Indian pediatric oncology. In a study conducted in Mumbai, India in which 31 parents were interviewed, 13 felt that their child was already aware of their disease status without being told directly and parental anxiety and collusion were major barriers to formal support or open communication with their children (Muckaden et al., 2011). Nondisclosure and non-discussion are also common occurrences in the adult oncology setting in India (Chawak et al., 2020). Chawak and colleagues explain that family caregivers and oncologists are the primary medical decision makers, and that patients are often not asked about their preferences. The paternalistic style of oncologists serving as the primary decision maker for adult patients is endorsed by some patients, as they did not have enough information and knowledge to make the decisions (Chawak et al., 2020). Despite the benefits of “patient-support paternalism,” Chawak and colleagues emphasize the importance of introducing communication skills training for oncologists to address patients’ unmet communication needs. Health care professionals need training on how to share information, to be empathic, and to encourage patients to participate in medical encounters if they desire. This aligns with the action steps brought forward by Chatterjee and Choudhury (2011) in their paper on the need for medical communication skills training in the Indian setting.
Children’s exclusion from cancer-related discussions and decisions is frequently “justified” as a means of protecting them from upsetting information because they are too “immature” to understand. Additionally, concepts of dharma, karma, non-maleficence, and beneficence, as well as socioeconomic influences, may also play an important role in parents’ and children’s perceptions of cancer and decisions regarding care (Ganguly et al., 2020; Thombre et al., 2010). For example, Participant 13, who was unaware of her diagnosis initially, attributed her illness to God’s will. She was also reluctant to talk to her parents about her illness due to fear of causing them additional stress. Additionally, Participant 6 spoke about understanding his parent’s decision to do his intrathecal chemotherapy without sedation, as this choice gave his family enough time to catch the train home rather than staying overnight in Delhi and incurring greater financial costs. Regardless of children’s perceptions of their participation in care, our results demonstrate that children can be distressed by their exclusion from care-related discussions, decisions, and actions. The situations in which they were excluded were highly significant and memorable to them. This notion not only challenges the premise that exclusion is protective, but highlights the impact of exclusion on their moral experiences. Research in the adult oncology setting in India reported that adult patients attempt to self-regulate and remain positive to protect their family’s well-being (Chawak et al., 2020). Similarly, childhood ethics research conducted in several countries emphasize the notion that children are active agents, and that exclusion can be isolating (Carnevale, 2016). Results from our study support this research (Carnevale, 2016). For example, one child reported feelings of sadness and distress when he was not informed of his leg amputation until the morning of the surgery, whereas another recounted feeling “very bad” when a doctor did not answer their questions about cancer. Despite the exclusion reported by many of our participants from their care, the United Nations Convention on the Rights of the Child states that “children, including young children, should be included in decision-making processes, in a manner consistent with their evolving capacities” (2009). Through analysis of children’s agency in the health-related literature, Montreuil and Carnevale (2016) states that children’s agency can be defined as “children’s capacity to act deliberately, speak for oneself, and actively reflect on their social worlds, shaping their lives and the lives of others” (p. 8). Given that children can express themselves in various ways such as by verbal communication, nonverbal expression, writing or art-making, a child’s agency does not necessarily depend on adults as facilitators. Child agents have moral views that they value, and which can differ from the views of adults (Carnevale, 2016). Thus, children’s silence can be a result of their desire to conform to social norms, rather than their immaturity (Bluebond-Langner, 1978; Carnevale, 2016). Indeed, adults’ attempts to protect children such as by leaving their questions unanswered, can enhance children’s feelings of isolation, frustration, and fear (Bluebond-Langner, 1978; Carnevale, 2016). Consequently, involving children in their own care is not only a moral imperative, but an ethical one as well.
Some participants in this study became aware of their cancer without being directly told. Some children did not want to ask their parents questions about their illness and diagnosis because their parents were already distressed and did not want to worsen their parent’s condition. This phenomenon is well understood in literature from outside of India. The seminal ethnographic work of Blueblond-Langner (1978) with children with leukemia found that children with cancer were attentive to their parents’ needs. This work and more recent literature recommend telling children what they want to know and answering questions they are asking, but to do so in their own terms (Bluebond-Langner, 1978; Rosenberg et al., 2016). Bluebond-Langner (1978) justifies this recommendation through her findings that children with cancer have different questions, concerns, and needs at different stages of their illness—corroborating the results of our study.
Throughout the research process, reflexivity was required in order to generate knowledge that recognizes differentness and to navigate the researcher’s “dual position both within and outside the phenomena” (Ben-Ari & Enosh, 2010, p. 2). Reflexivity therefore means that researchers should: (1) be aware of how one’s perceptions, beliefs, and cultural/social contexts shape identity; and (2) consider how these factors may simultaneously influence the research process (Ben-Ari & Enosh, 2010). Therefore, the student researcher took steps to maintain reflexivity as suggested by Ben-Ari and Enosh (2010). First, the researchers self-reflected on any pre-existing expectations toward the study settings, participants, and overall research process prior to commencing the study. The period of self-reflection allowed the researchers to question the meaning of differences between their expectations and actual experiences, thereby generating “new understandings that lead to a higher level of conceptual integration” (p. 7). Second, the researchers engaged in open, ongoing discussions with co-researchers and stakeholders to address potential biases, questions, and concerns, allowing divergent perspectives to be heard and contested (Cohen & Crabtree, 2006). Third, the researchers created safe spaces for children to be interviewed such as adapting to their communication preferences and engaging in play to increase their comfort with interviewers. Finally, the student researcher took reflexive notes in order to revisit, question, and discuss her research decisions with co-authors and stakeholders (Cohen & Crabtree, 2006). The discussions and ongoing communications within the research team created a richness in perspectives that allowed the authors to integrate, process, and analyse the data.
Strengths and Limitations of the Study
Important strengths and contributions of this research included the use of an ethnographic study using a moral experience framework to explore the involvement of children with cancer in decision making processes. This was the first time the moral experience framework was used in psycho-oncology and contributed to the paucity of literature examining children’s health experiences in India. Important topics on Indian children’s experiences with cancer such as their moral dilemmas, emotional experiences, and what causes them distress were identified, which may potentially improve how pediatric healthcare is carried out in India. This may contribute to better physical and psychosocial outcomes for children. However, study limitations should be acknowledged, which relate primarily to data collection. The cultural and language limitations of the student researcher, requiring the use of interpreters, may have resulted in missed nuances in participants’ disclosures. Some interview responses provided by children may have been influenced by the presence of their parents and/or a hospital staff member who conducted interviews at the public hospital. This influence may have affected the study in favorable and unfavorable ways. For example, the child may have felt more comfortable to speak in the presence of their parent, or alternatively, they may have withheld some information they did not want to share with their parents. Finally, although the moral experiences framework has been useful in understanding moral dilemmas encountered by individuals and families in healthcare contexts (Carnevale et al., 2006; Passos dos Santos et al., 2019; Sebti et al., 2019), the concept of a “moral experience” is still relatively new and has not been extensively examined with children. Therefore, there is limited knowledge regarding the moral experiences of chronically-ill children, specifically how they perceive everyday events which may help to realize or thwart their values and beliefs. In addition, it is particularly challenging to relate what a “moral experience” is to what it ought to be, which can present ethical concerns. Children may experience distressing moral experiences in their care. Resisting an unfavorable medical treatment such as needle pokes, does not necessarily mean the treatment is ethically wrong, particularly when the treatment is deemed lifesaving and necessary. In addition, predominant views of childhood depict children as vulnerable beings with limited agential capacities (Montreuil & Carnevale, 2018), making it difficult to balance children’s moral agency with their need for protection/best interests. Thus, there is a need to clarify how children’s moral experiences relate to and influence healthcare ethics.
Implications of Study and Future Directions
There is a lack of normative standards, including the availability of ethical position statements, regarding children’s participation in treatment-related decision-making in India. Future development of these standards should be attuned to the child health care context in India, centered on the promotion of children’s best interests—which include an interest to be heard and participate in decisions that affect them—while bearing in mind the interests of families, HCPs, as well as institutional and societal resources (Carnevale, 2016; UNCRC, 1989). This process requires ongoing examination of the “moral terrain” of pediatrics in India (Carnevale, 2013). This ethnographic study provides research evidence to help promote this work.
Muckaden et al. (2011) highlight a difference in the psychological issues in pediatric palliative care in India and in the West, and state that research and training of staff dealing with these children is of paramount importance. Muckaden et al. explains that pediatric palliative care is still new in India and that wider understanding, application, and acceptance of this specialty is essential for improving care of children with advanced cancers. Our ethnographic research helps address some of this gap, with regard to children with cancer. Clinical practices could be developed to help promote children’s participation in treatment-related discussions and decisions, in ways that children prefer. Practice development will need to be adapted to Indian contexts, taking into consideration the views of parents and HCPs. A North Indian initiative reported the implementation of training programs for physicians on how to elicit children’s informational preferences (Seth, 2010). Future work should also include nurses and other HCPs that care for children with cancer.
In keeping with the foundational tenets of childhood ethics that oriented this research (Carnevale et al., 2020), and the paucity of data on children’s own experiences in India and internationally, our research focus was centered on the moral experiences of children. Nonetheless, other important research concerns that warrant their own investigation include: understanding parents’ moral experiences; the moral dimensions involved in parental striving to be a “good parent”; and the influences of dharma, karma, non-maleficence, and beneficence in parents’ decisions regarding their child’s care. Additionally, while we did not collect data on children and families’ socioeconomic backgrounds. Families from various socioeconomic backgrounds seek care at each of the respective sites, including high-income families who sometimes seek care at the public hospital. At each of the study sites, the cost of cancer is high, averaging at US$764 over a 14-week period (Ahuja et al., 2019). These costs often contribute to negative impacts on caregivers’ psychosocial health (Mardakis et al., 2019), and likely also influence children’s moral experiences. Given that some of our participants have alluded to the impacts of cost on their care, a future investigation regarding the impacts of socioeconomic status in pediatric cancer care can further inform children and parents’ moral experiences.
The Indian Pediatric Oncology Group (InPOG) describes a hopeful picture regarding the viability of continued collaborative research in pediatric oncology in India (Arora & Bakhshi, 2016). This national cooperative group has promoted multicentre clinical trials to understand biological differences in disease, assess responses to treatment, and ultimately improve childhood cancer survival in India (Arora & Bakhshi, 2016). This group can build on the results of our study to design additional research and develop clinical practices that can help improve the experiences of children with cancer in India.
Conclusion
Although participants demonstrated the necessary capability and interest to participate in decisions, discussions, and/or actions related to their cancer care, the extent to which they participated varied widely across ages and settings. For children who wished to learn more about their illness and treatment, exclusionary actions from parents and/or healthcare providers that thwarted their desires exacerbated children’s feelings of distress, often leading to a profound sense of loneliness, sadness, and anxiety. Thus, most children valued gaining knowledge about their health and relied on their parents and healthcare providers to help realize their desires for inclusion in care. Through the moral experience lens, this study helped to uncover children’s values, desires, and needs, and the factors that contribute to positive and negative moral experiences within the pediatric oncology setting in India. In particular, this study highlighted the importance of supporting children’s desires to be involved in care and providing useful guiding evidence for children, families, HCPs, policy makers, researchers, and interested others.
Footnotes
Acknowledgements
We wish to thank the child participants and their families for their incredible openness and willingness to participate in the study. We would like to acknowledge the staff at the study settings who were supportive throughout the study process, the interpreters and translators who made this research possible (Kamlesh Chaudhary, Pralav Bhansali, and Mithool Jain), Crystal Noronha of the VOICE (Views on Interdisciplinary Childhood Ethics) team (![]() ), and Yi Wen (Jenny) Wang for her support in editing the final manuscript. VOICE is supported by Social Sciences and Humanities Research Council—SSHRC (A) and Canadian Institutes of Health Research (CIHR).
), and Yi Wen (Jenny) Wang for her support in editing the final manuscript. VOICE is supported by Social Sciences and Humanities Research Council—SSHRC (A) and Canadian Institutes of Health Research (CIHR).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Justine Behan was the recipient of the following awards: Mitacs Globalink Research Award [IT07976]; Global and Indigenous Health Nursing Travel Award; McGill University Travel Bursary; Mobility Graduate Award; and the Mitacs Master’s Award for Outstanding Innovation. Argerie Tsimicalis is the recipient of a Chercheur-Boursier Junior 1 Award from the Fonds de recherche Québec-Santé (FRQ-S). Ramandeep Singh Arora, Franco A. Carnevale, Sameer Bakhshi, and Bani Bhattacharjee disclosed no funding support.
Author Biographies
![]() ), Montreal, Quebec, Canada.
), Montreal, Quebec, Canada.