
Abstract
Social support is known to be essential to cope with the physical and psychological aftermath following coronary heart disease treatment. Consequently, patients experiencing loneliness may be placed in a vulnerable situation. The aim of this study was to provide insight into the nuances and complexity of loneliness and its impact on health behaviour in the early rehabilitation period following treatment. The study used a hermeneutic philosophical approach. Patients classified as lonely were interviewed in either a focus group (n = 7) or in an individual interview (n = 10). We analysed the empirical material using inductive content analysis. The analysis illuminated various dimensions of patients’ perceived loneliness; ‘Loneliness as an emotional pain’, ‘A changed, but unmet need for social support’ and ‘Striving for symmetry in relationships’. Loneliness negatively influenced patients’ ability to adapt to the critical event and manage health behaviour changes. Insight into the mechanisms that aggravate loneliness may inform future social support interventions.
Introduction
In the early rehabilitation period following surgical, invasive or medical coronary heart disease (CHD) treatment, patients have a crucial need for support from social network members, in order to cope with the physical and psychological repercussions, as well as to manage health behaviour changes and navigate a new way of life (Junehag et al., 2014; Pryor et al., 2014). However, in Western society the number of people who live alone has increased in recent decades (Cacioppo & Cacioppo, 2018) and therefore, an increasing number of patients may not necessarily have a primary caregiver in their social network to provide the care and support needed in the rehabilitation period. Also, social interaction patterns have changed in society, as social networks based on, for example, civic engagement, have decreased (Cacioppo & Cacioppo, 2014; Putnam, 2000). These societal patterns might partly explain why studies of the general population have found that 5–30% of adults experience loneliness as a chronic state (Christensen et al., 2012; Hawkley & Cacioppo, 2010; Heinrich & Gullone, 2006; Victor & Yang, 2012).
Loneliness as a phenomenon is a complex issue, as perceived social support is affected by both subjective and objective components. It is typically defined as a distressing feeling that accompanies the perception that one’s social needs are not being met by the quantity or especially the quality of one’s social relationships (Hawkley & Cacioppo, 2010). The social integration literature highlights the fact that the feeling of loneliness is not solely predicted by the number of members in a person’s social network, but rather by whether the social interaction produced by it satisfies the needs a person might have in their given life circumstances (Cohen, 2004; Hawkley & Cacioppo, 2010).
Consequently, patients who, in advance of the CHD event experienced sparse or inadequate social support are in a particularly vulnerable situation, as the increased need for social support in the early rehabilitation period may result in an even greater discrepancy between their social needs and the available social support, leading to an increased feeling of loneliness. Furthermore, especially in Scandinavian countries, the welfare state handles most of the practical and informal support needed in the rehabilitation period, which is a reason why home visits from social network members and the accompanying emotional support may be less frequent (Oorschot, 2005).
Loneliness has important consequences in patients recovering from a CHD event. In studies investigating patient-reported outcomes, it has been found that, for example, disease-specific quality of life (Leifheit-Limson et al., 2010), subsequent depressive symptoms (Barefoot et al., 2003) and patients’ ability to perform self-care (Hawkley & Cacioppo, 2003; Vassilev et al., 2014), are negatively affected by loneliness. Also, in prognostic studies loneliness is shown to increase the risk of mortality nearly two-fold (Barth et al., 2010; Brummett et al., 2001; Christensen et al., 2019).
Age and gender norms may affect an individual’s need for social support and consequently, how a potential accompanying feeling of loneliness materializes. The literature on sex and gender differences in the prevalence of loneliness has been inconsistent, and no consensus has been reached. A meta-analytic review has revealed a small but significant gender difference, suggesting that males are slightly lonelier than females in childhood, adolescence and young adulthood, attributing these differences to a number of factors including age-normative expectations and gender-related influences. However, these differences disappear in middle adulthood and old age (Maes et al., 2019). Literature on age differences in the prevalence of loneliness has revealed that loneliness levels differ across the lifespan and tend to increase from age >75 (Luhmann & Hawkley, 2016). In the light of this evidence patients with CHD may have an increased risk of suffering from loneliness as CHD is most frequent in age >65 and in men (Authors/Task Force et al., 2016).
In the present study, we set out to explore the experience of loneliness and draw attention to the patients’ perspectives. The aim is to provide insight into the nuances and complexity of loneliness as well as its impact on wellbeing and health behaviour in the early rehabilitation period following CHD treatment. Research involving patients who experience loneliness has the potential to improve our understanding of social support deprivation and the consequences experienced, and thus to enhance nursing care in clinical practice as well as inform future social support interventions for this vulnerable patient population.
Method
Design
In the present study, we made use of a hermeneutic philosophical approach, as it is suitable for understanding and interpreting social phenomena and actors (Gadamer, 1976; Geanellos, 1998). One of the main concepts in Gadamer’s philosophical hermeneutic approach is that interpretation and understanding is considered an ontological principle where the interpreters’ pre-understanding plays an active role. In this approach, it is vital that the interpreters confront their pre-understandings, in which history, tradition and experiences are embedded.
A fundamental pre-understanding applied in the present study was, that the feeling of loneliness is mainly initiated by lack of quantity or quality of social support from network members and only to a minor extent related to a person’s subjective expectations and needs for social support. A further pre-understanding applied was that social interactions with network members are basically desirable and that loneliness is a distressing feeling that reduces quality of life. Our experience with hospitalised patients who had limited or inadequate social support is that these patients often had reduced resources to handle the physical and psychological aftermath of the CHD event.
In the hermeneutic philosophical approach understanding the other can never be fully achieved but rather appears through the fusion of the horizons of participants and researchers. In this approach, new understandings can emerge in a dialectic process of the hermeneutic circle, that is, de-contextualization of the whole into parts and re-contextualized into a new whole by fertilization with the pre-understanding (Geanellos, 1998). In this inquiry, interpretation is an act that takes place in the medium of language that when successful enriches the researcher with a deeper understanding of the phenomenon under investigation (Agrey, 2014).
Selection of Participants
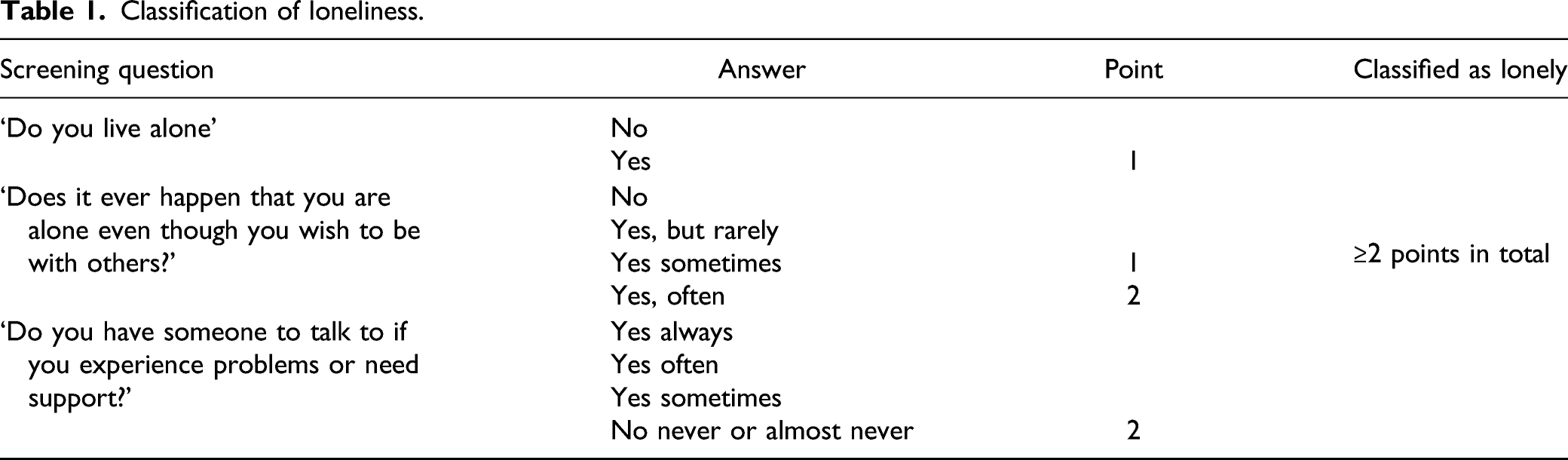
Classification of loneliness.
Patients classified as lonely were re-approached by Blakoe, M. and invited to an interview session 8–12 weeks following discharge. In total, 32 accepted the invitation and were asked to provide contact information. The invitation to either focus group sessions or individual interview sessions was sent approximately 4 weeks following discharge, by phone, mail or email, as a result of which 17 accepted participation. All participants interviewed lived alone and had a Danish ethnic and cultural background. The type of interview session participants were invited to was chosen at random.
Data Collection
In total 17 participated in either focus group or individual interview sessions. Participants consisted of 12 males aged 53–88 years and five females aged 62–74 years, which reflects the distribution of age and sex in a CHD population, that is, overrepresentation of males. Data were not gathered on gender identity.
In order to gain a nuanced insight into the importance of loneliness we chose to use two complementary interview methods; focus group interviews and individual interviews. The former has the advantage that participants who are in similar life situations can be inspired by each other’s statements, and through discussions of the topics bring forward commonalities and differences (Jamieson & Williams, 2003; Krueger, 2014). However, we experienced a tendency to discuss the phenomenon of loneliness in more general terms in the focus group sessions. Consequently, following the two focus group sessions, we chose to enrich the empirical material with individual interview sessions with a more in-depth approach (Dicicco-Bloom & Crabtree, 2006).
Two focus group sessions were conducted in hospital, consisting of three and four male participants respectively and lasted 55 and 70 minutes each. Focus group sessions were facilitated by Blakoe, M. and Bernild, C. acted as an observer. Initially, in the focus group session, the authors encouraged participants to honour confidentiality within the group, as lack of social support and loneliness can be a personal and sensitive issue. Also, to respect patients’ integrity, the authors endeavoured to be tactful on the depth of the questions asked in the sessions.
Participants invited to an individual interview chose whether the interview was to be conducted in a meeting room in hospital or at the participant’s home. 10 individual sessions were conducted, six in participants’ homes and four in hospital. Sessions lasted between 30 and 98 minutes and were conducted by Blakoe, M.
A semi-structured interview guide was used in both the focus group and individual sessions (Dicicco-Bloom & Crabtree, 2006), however, the interview had a more in-depth approach in the individual sessions. The interview guide was founded on the literature on the challenges and experiences of recently hospitalized cardiac patients and the role of relationship and communal coping when making lifestyle changes. The wording of the questions was guided by the philosophical hermeneutic approach which stresses that questions asked must strive to be genuine in a search for meaning (Agrey, 2014). The interviewer avoided directing participant narratives by using open-ended exploratory questions. The questions were focused on participants’ perception of loneliness during hospitalization and in the early period following discharge and on potential barriers to seeking out social support in the social network or local community. Furthermore, the interview guide focused on how the participants experienced that loneliness had affected their health behaviours following CHD treatment. Additional questions were asked when appropriate.
Participants represented both urban and rural areas in Denmark, which intentionally contributed to a richer variation of participants’ life circumstances and thus, supported the trustworthiness of the findings (Elo et al., 2014). All interviews were audio recorded and transcribed verbatim.
Analysis
Gadamer’s philosophical hermeneutic approach does not offer a methodology or method for analysis. Even so, he stated that a systematic approach is needed in order to reach understanding (Gadamer, 1975). To analyse the substantial amount of empirical material using a systematic approach, we made use of inductive content analysis (Elo & Kyngas, 2008; Graneheim & Lundman, 2004), as it is suitable for analysis of multifaceted phenomena. In the inductive content analysis, the process consists of breaking the empirical material, that is, one interview transcript, into smaller parts (meaning units), then condensing the meaning units and making sub-categories and subsequently collecting them into new wholes (categories) across all interview transcripts.
The written transcript was read several times to make sense of the data. In total 129 meaning units, that is, sentences expressing both manifest and latent content were highlighted and condensed. The condensed meaning units were grouped under 14 sub-categories and subsequently three main categories using content-characteristic words. We strove to grasp the meaning and significance transmitted in the interviews throughout the sorting and analyses of the empirical material, in conjunction with our normative pre-understanding. In accordance with the hermeneutic circle, the process was not linear but carried out going back and forward at all steps of the analysis, as illustrated in Figure 1. The process of the analysis; examples of selected meaning units, condensed meaning unit, sub-categories, category, and the hermeneutic circlewith green arrows.
Woven into the process of analysis was the interviewer’s immediate impression of the situational context in the interview session. Some sex differences in the experience of loneliness in patients with CHD should be expected, but since the difference were expected to be marginal (Maes et al., 2019), we chose not to focus on sex differences in the performance of the analysis.
Blakoe, M. and Bernild, C. read the transcript of the interviews. Blakoe, M. performed all coding and analysis in discussion with the Bernild, C., and the analysis was modified until agreement was reached. Furthermore, the abstraction process was discussed with the co-authors Hoejskov, I.E., Palm, P., Berg, S.K. and with an expert group of cardiac nurses experienced in qualitative research methods.
To support dependability, we sought to document the research process in as much detail as possible, and the results of the analysis are supported by representative quotes. The consolidated criteria for reporting qualitative research (COREQ) was used to guide reporting of the findings (Buus & Perron, 2020). Participants are anonymized in the presentation of the material and quotations are identified using participants’ age, sex and type of interview session. Participants were not provided with an opportunity for members checking in the analysis process.
Ethics
Patients approached in this study received written and oral information on the purpose of the study and the right to withdraw at any time with no consequences for their treatment. The investigation was approved by The Danish Data Protection Agency (jr.number: VD-2018-490) and the regional ethics committee. The study conforms to the Declaration of Helsinki (18) and the ICMJE Recommendations for the Protection of Research Participants (2021).
Findings
The analysis of data resulted in identification of three different dimensions of living with loneliness following CHD treatment: Loneliness as an emotional pain; The changed, but unmet need for social support; and striving for symmetry in relationships. Each dimension consisted of multiple meaning units (see example in Figure 1).
Loneliness as an emotional pain
In relation to the CHD event, both during hospitalization and the first days following discharge, participants experienced a vacuum that arose between an increased need for practical, emotional and informational support, and a lack of adequate response from social network members. Participants described this feeling of loneliness as an emotional pain, which resulted in a sense that life became meaningless, and this affected their sense of having value as a human being, as illustrated in this quote: Often when I sit and watch television in the evening, I think… hmm.... why does no one ever come over to visit me?… mmm… are you not worth anything or what? That’s what I am thinking ... and you are probably not then. (Female, individual interview)
Participants also expressed the feeling that their hospital admission resulted in a sense of disconnection from everyday life – a feeling that persisted following discharge. This sense of disconnection from everyday life was experienced as unpleasent and as difficult to overcome and it contributed to a hesitation in reaching out to their network members. In relation to the first days after the return home, one participant said: I didn’t feel lonely … I would rather say a little alone … out on a desert island. I knew I could call people, send text messages or go on skype … I knew that. But my world right here and now, that was not their world at all … I drove in another lane … another detour… and my detour was not as fun as theirs. (Female, individual interview)
Loneliness as an emotional pain could simultaneously coexist with an acceptance and recognition of oneself as a person who likes to be alone. However, most participants described themselves as involuntarily alone due to circumstances in life, or as a necessary but undesirable opt-out from existing relationships due to disappointments or feelings of being disconnected from network members.
The Changed, but Unmet, Need for Social Support
The early period following discharge to home was generally experienced as filled with uncertainty on how to handle everyday life, and how to deal with potential symptoms of a relapse. Social support was expressed as vital in order to absorb the shock that came from having undergone treatment for CHD. The changed, but unmet, need for social support in relation to the CHD event was verbalized by a participant in this quote: I had a big need ... not for a long visit, but like … to feel that someone had understood what I had just been through … because it is difficult to tell people … are you aware that I have stood and looked down into the abyss? (Female, individual interview)
As this quote illustrated, the participant had a need to be understood, but also an uncertainty towards network members’ capability of fully relating to the personal experience of the CHD event. Likewise, participants described that even though there was a possibility to talk to social network members about their experiences and doubts associated with heart disease, this was not always enough to calm worries or to absorb shock.
Some participants described a feeling of being forgotten by the social network, which resulted in disappointment and frustration toward social network members. This frustration was reinforced by whether the social network members were expected to engage voluntarily. This is verbalised in the following quote: There are some from my network that I am still quite disappointed with… I almost feel like saying, I think you’ve been very…mmm… unfair to me. I was there for you when you needed it. You did not even ask me how I was. You did not even call. (Male, individual interview)
Regarding performing health behaviour changes and adequate self-care following discharge, social support from the network member was likewise expressed as being vital. In relation to physical activity one participant said ‘Yes, because my son-in-law he came and said, “You have to go out and do some workout.” And then you want to do it, right… to help him, and also to help myself’ (Male, focus group).
Similarly, regarding nutritional intake one informant said ‘When I got home, she often came by with food, and then we sat and ate together. And it helped a lot that you do not just have to sit and eat the food alone’ (Male, individual interview).
In general, participants described how social network members could motivate different aspects of health behaviour such as physical activity and nutritional intake by providing information on healthcare advice and as a motivating factor to follow it. By contrast, a lack of social support and the associated feeling of loneliness had a demotivating influence on health behaviours as stated in this quote: ‘You know, if you are a little depressed and if you just have to sit at home all alone, well then nothing happens’ (Male, individual interview).
The participants also described how network members could act as a bridge to the healthcare system by helping the patient to navigate the available healthcare services.
Striving for Symmetry in Relationships
Even though all participants recognized that the emotional and physical aftermath of CHD treatment had increased their need for emotional and/or practical support, especially following discharge, they also verbalised a need for reciprocity and symmetry in their relationships. This was verbalised in relation to practical support, for example, cleaning or shopping, and in relation to emotional support, for example, to talk through thoughts and feelings related to the CHD event. The concept of balance was expressed as a wish to provide social support back, or sometimes, to strike back against the disappointments related to lack of social support. One participant said ‘That’s how it is .... Then they [i.e. the network members] come and whine when they are in hospital “why don’t you come and say hello?”. There you see, you didn’t care either’ (Male, individual interview).
The payback of the social support benefits or disappointments was both related to events in the past and in an imagined future. Another way of striving for symmetry was by trying to maintain normality in the interaction with social network members, for example, by talking about topics other than illness, for example, talking about politics. The need to maintain normality in the interaction also served a need to forget the heart disease for a while.
For some participants, a close relationship with relatives was more ambivalent. As this informant said when asked if she would have wished to have more frequent visits from the family following discharge ‘Then I almost think I would have asked them to leave. It seems grotesque… I wish they had been there… and would also like them to leave again’ (Female, individual interview). This ambivalence was explained as caused by a lack of mental surplus to socialise as a result of the heart disease that coexisted with an increased need for social support.
Participants also stated that social and cultural norms could act as a barrier to seeking social support from the network, as articulated in this quote: I don’t think you can do that at all [i.e. ask your network members for help]… not in today’s society … demand that all sorts of people should come and help you. I think we have a society that is very poor in this regard. (Male, focus group)
Thus, participants experienced both dyadic and cultural barriers that diminished their own initiative to reduce loneliness.
Discussion
A pre-understanding in this study was that loneliness is a distressing feeling that can be more of a problem when coping with CHD. Another was that the feeling of loneliness is mainly initiated by lack of quantity or quality of social support from network members and only to a minor extent related to a person’s subjective expectations and needs for social support. In the process of analysing the empirical material, nuances and complexities were added to this pre-understanding of loneliness in patients coping with the physical and emotional aftermath following CHD treatment. It became clear that the experience of loneliness when coping with heart disease was made up of several dimensions. We discuss these dimensions in relation to psychological, sociological, and health and nursing care perspectives in the literature. The ambition is to gain new understandings through interaction between the empirical and the theoretical, and in this way expand and enrich the empirical findings.
A consistent finding in this study was the participants’ experience of shock related to the CHD event and the fundamental uncertainty to which it led. This experience created a pervasive deprivation in relation to social support and consequently, an increased feeling of loneliness as an emotional pain which affected their sense of having value as a human being. This experience was expressed by both male and female participants. This finding is in line with the social integration literature which posits that loneliness engenders with other negative emotions, such as anxiety, depression and self-critique (Cacioppo et al., 2000; Cacioppo and Patrick, 2008; Wiesmaierova et al., 2019). Furthermore, loneliness can be related to stigma (Cacioppo and Patrick, 2008), which might further enhance the subjective feeling of loneliness. Several participants also described how they involuntarily had to opt-out of relationships, due to disappointments or feelings of being socially disconnected because of network members’ behaviour. These findings may partly be explained by evidence from the psychological sciences that indicate that people who feel lonely have an increased sensitivity to social threats (Cacioppo & Cacioppo, 2014; Hawkley & Cacioppo, 2010).
One participant expressed the feeling of being mentally disconnected as like ‘driving in another lane’ following the CHD event. This description nuanced our pre-understanding that the feeling of loneliness is not necessarily related to the patients’ quantity or perceived quality of support provided by social network members. The interpretation of these descriptions suggests that the CHD event could act as a trigger event initiating the feeling of loneliness. In this interpretation, the feeling of loneliness in patients treated for CHD may only to a minor extent be related to either the quantity or perceived quality of the existing social network. The feeling of loneliness may instead mainly be related to a circumstantial feeling of being mentally disconnected from everyday life in conjunction with a lack of corresponding initiatives from the social network members. In this interpretation, the initiated or intensified feeling of loneliness may differ from that of a population that is not affected by critical illness.
Similarly, some participants said that the unmet need for support to handle the physical and psychological aftermath was founded in uncertainty towards network members’ capability of fully relating to the thoughts and emotions related to the CHD event, rather than lack of quantity of social network members. Other participants had experienced that the network members did not sufficiently accommodate the changed need for support as they simply did not make any additional contact in relation to the event.
In relation to accommodating relevant health behaviours, the participants similarly expressed an increased need for social support. One way of understanding patients’ health behaviour is through the scope of the theory on self-care (Vassilev et al., 2011). Self-care is defined by nursing theorist Dorothea Orem as ‘the practice of activities that individuals initiate and perform on their own behalf in maintaining life, health and well-being’ (Orem, 1985). According to self-care theory, actions for self-care need to be motivated, and among several factors promoting motivation, social networks play an essential role (Orem, 1985; Vassilev et al., 2014). This study reveals that the opposite mechanism is also applicable, as the feeling of being socially disconnected negatively affected some participants’ valuation of themselves as human beings, and therefore diminished their motivation to perform adequate self-care. This may contribute to an understanding on why medical and health science finds that in patients feeling lonely, the ability to perform physical and mental self-care is negatively affected (Albus, 2010; Authors/Task Force et al., 2016; Karatas & Bostanoglu, 2017; Magrin et al., 2015; Vassilev et al., 2014) as well as their likelihood of participation in cardiac rehabilitation (Graversen et al., 2017; Pedersen et al., 2018). This finding expanded and added new understanding to our pre-understanding as it suggested that a devaluation of one’s own value might be one of the key factors in the association between lack of social support and inadequate health behaviour following CHD treatment.
Despite the expressed need for social support in the early rehabilitation period following CHD treatment, participants in this study described mutual and complementary societal, dyadic and psychological mechanisms that impacted how and from whom they could receive adequate social support.
Several of the participants expressed the view that social norms framed who and how they could ask for social support. They explained that these norms dictated that social support should be provided by a network member that was in a close relationship with them in advance of the CHD event and that support should be offered unrequested. This statement is supported by sociological research claiming that in Western cultures, people, in general, are taught to be independent and therefore may experience a drop in self-esteem when asking for help and as a result, a person might decide not to utilise available support. These social barriers may further hamper to ask for help for the increasing number of people who live alone (Cacioppo & Cacioppo, 2018) and therefore do not necessarily have a primary caregiver in their everyday life. Furthermore, the norms can be mediated by the basic changes in the way people socially interact when the welfare state handles most of the care tasks that the citizen needs when affected by illness, which potentially crowds out informal caregiving (Oorschot, 2005).
In addition to social norms, participants also described how dyadic relational mechanisms could either promote or limit who they could ask for social support following discharge from hospital. Participants experienced a need for reciprocity in both practical and emotional support in the relationship. This aspect is also evident in the literature, as an essential part of making sense of social relationships is that both individuals have value and worth to each other (Cacioppo and Patrick, 2008). In the rehabilitation period following CHD treatment this reciprocity was challenged as the participants had an increased need for social support and at the same time lacked physical and mental energy to socialise and provide support for others. This ambivalence toward socialization added nuances to our pre-understanding of social support as being basically desirable in the early rehabilitation period.
The perceived social norms and patterns, alongside the need for reciprocity, may limit patients’ ability to ask for social support from network members after discharge from hospital. This is an important finding as these mechanisms might be different from people feeling lonely in a general and healthy population.
Implications for Clinical Practise
This study highlights the importance for clinical practice to consider loneliness as an influencing factor on patients’ wellbeing and ability to perform health behaviour changes in the rehabilitation period following CHD treatment. Recognizing the importance of loneliness in patients with CHD should enable implementation of support interventions based on patient needs.
Insight into the patient’s perspective of the societal, dyadic and psychological mechanisms that aggravate loneliness may provide valuable information on the structure and content in supporting initiatives.
Limitations
Participants in this study were screened for their experience of loneliness during hospital admission and the interviews were done 8–12 weeks following discharge. As patients’ perceptions of loneliness might be different in these phases of the disease course, the feeling of loneliness may have changed in the period from the patient were screened to the interview were conducted.
Approximately half of the eligible patients accepted the final invitation to participate in an interview session. As the patients invited to participate were characterised by feeling lonely and loneliness engenders with other negative emotions, for example, depression, non-participants may, to a greater extent than participants, have barriers toward the social interaction which is embedded in an interview session. Therefore, a limitation in the present study may be that the participants did not represent patients affected most severely by loneliness. On the other hand, the opposite may be the case: that the patients most severely affected by loneliness had an increased desire to participate. In both cases, the high number of non-participants may have influenced the study findings.
As this study involved a philosophically hermeneutical approach, language is perceived as an integral part of understanding. However, we are aware that loneliness as a phenomenon has an existential nature and is woven into the participants’ way of being in the world, and therefore, the feeling of loneliness is only to some extent possible to put into words, and thus be a subject of comprehension. Therefore, in the interview sessions, it was challenging for participants to capture the essence of loneliness without describing the content and quality of former, current or imagined social relationships.
The interpretation of social support and the subjective feeling of loneliness can differ between males and females (Maes et al., 2019) why future research should explore the influence of gender-related factors on experiences of loneliness among patients treated for CHD.
Conclusions
Patients having sparse social networks in their everyday day life are in a particularly vulnerable situation in the early rehabilitation period following CHD treatment, as this period is characterised by an increased need for practical, informational and emotional support. Consequently, a feeling of loneliness can be initiated or intensified. Loneliness negatively affected patients’ prerequisites to handle the physical and mental aftermath of the CHD event and the motivation to perform health behaviour changes in the early rehabilitation period. Participants in this study assessed that societal, dyadic and psychological mechanisms had an impact on their access to support from social network members.
Footnotes
Acknowledgments
We wish to sincerely thank the participants who volunteered and generously shared their thougths in focus groups or individual interviews. Also, we wish to thank Malene Lindegaard Juul Larsen for helping with the questionnaire survey and Signe Westh Christensen for helping with the transcription of the interviews.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Rigshospitalet research grant (E-22281-07).
Data Availability
The datasets generated and/or analysed during the current study are available in an anonymised form from the corresponding author on reasonable request.