
Abstract
The prevalence of self-prescribed complementary medicine (CM) use is an area of concern across the Middle East. We conducted a descriptive qualitative study to describe women’s use of CM during their childbearing years in Egypt, Jordan, Saudi Arabia and Iran. The study conducted using face to face audio-recorded interviews with 70 participants. Our findings showed that women used several herbal plants to ease pain and discomfort during menstruation and/or during pregnancy and in postpartum care. Acupuncture, meditation, and massage were less likely to be used by women. The impact of CM was often described in relation to perceived usefulness and safety of herbs. Cultural beliefs and roles of women contributed to the use of herbs among women. Given the high use of herbal medicine, there is a need for discussion about the potential of adverse effects of some plants or their metabolites following self-medication during the childbearing years.
Introduction
The use of complementary medicine (CM), including herbs for the management and treatment of various health conditions is widespread globally (Steel et al., 2020). According to Ozgoli and Saei Ghare Naz (2018), CM is defined as a diverse group of health-related therapies and natural remedies, including aromatherapy, acupuncture, herbs, homeopathy and reflexology. Internationally, the prevalence of herbal medicine use is varied across countries. In Australia (Skouteris et al., 2008), Norway (Nordeng and Haven, 2004) and the United States (Furlow et al., 2008), a prevalence rate of 37% was reported among women during pregnancy, while in Malaysia (Rahman et al., 2009) and Tanzania (Godlove, 2011) researchers have typically reported prevalence rates of nearly 50%. In contrast, the prevalence of herbal medicine use during pregnancy in the Middle East is estimated to be 82% (John and Shantakumari, 2015).
Broadly speaking, three types of CM are commonly used in the Middle East: herbal remedies, cauterisation, and wet cupping or hijama (Ali-Shtayeh et al., 2015; John & Shantakumari, 2015). These practices reflect traditional Muslim CM that date back to the beginning of the Islamic civilisation in the seventh century. In the Middle East, both registered and unregistered healing centres practice traditional Muslim CM (locally known as the Prophetic Medicine) (Qureshi et al., 2020). Traditional Muslim CM includes a system of traditional and complementary healing practices comprised of herbal medicine, dietary practices, mind-body practices, spiritual healing and applied therapy (Al-Rawi and Fetters, 2012).
Women in the Middle East have been using CM and herbs as sedative and antiemetic agents during the childbearing years (Al-Yahia et al., 2017). Many women are motivated to self-manage their health during pregnancy (Peprah et al., 2019), and interest in women’s experiences of self-care strategies has grown among healthcare professionals. A woman in her childbearing years is defined as any woman aged between 13 to 50 years old and who is pregnant or can become pregnant (Del Gobbo et al., 2010). Cultural beliefs and access to CM are factors attributed to the relatively high use of CM by women in earlier studies (Arabiat, Whitehead, Al Jabery, Darawad et al., 2019; Peprah et al., 2019). Other motivations for the use of CM by women have been linked to perceived safety and effectiveness of herbal medicine (Arabiat, Whitehead, Al Jabery, Darawad et al., 2019; Arabiat, Whitehead, AL Jabery, Hamdan-Mansour et al., 2019; Barnes et al., 2019). The higher use of CM in earlier studies was often associated with both middle-age and higher education in both developed (Bishop and Lewith, 2010) and developing countries (Ali-Shtayeh et al., 2015; Kaadaaga et al., 2014).
It is important that nurses and healthcare professionals are aware of the adverse risks that may be associated with the use of herbal plants. For example, Kacip Fatimah and Salindah are associated with preterm labour, while Tongkat Ali herbal coffee is significantly associated with hypertensive disorders in pregnancy and foetal distress (Yusof et al., 2016). Other herbal plants, such as sage, camomile and fenugreek can pose risks and are linked to miscarriage when taken in large doses (Abdul et al., 2018; Halicioglu et al., 2011; Ouzir et al., 2016). Despite growing attention around the safety and efficacy of CM used for dysmenorrhoea or painful periods (Armour et al., 2019), pregnancy (Adams et al., 2009) and postpartum (Dehury et al., 2018; Diamond-Smith et al., 2016), there is little information available on CM used by women in the Middle East. It is important to better understand women’s experiences of using CM to guide efforts to improve women’s knowledge of the safety and efficacy of CM. The present study was carried out to describe women’s use of CM in their childbearing years in Egypt, Jordan, Saudi Arabia and Iran. This study aimed to enhance knowledge on the types of CM used most frequently by women residing Egypt, Jordan, Saudi Arabia and Iran during the childbearing years and women’s perceptions of their CM usage.
Method
A descriptive qualitative approach as described by Sandelowski (2000) was adopted to describe perspectives and experiences from the worldview of women. As the experiences of using CM during childbearing years are influenced by women’s beliefs and their interaction with their broader community and the healthcare system, a qualitative descriptive approach was selected as a mean of gaining insight into women’s perspectives, using their own words. Semi-structured interviews using open-ended questions were conducted over a period of 5 years from 2015-2020 in Egypt, Jordan, Saudi Arabia and Iran.
Participants
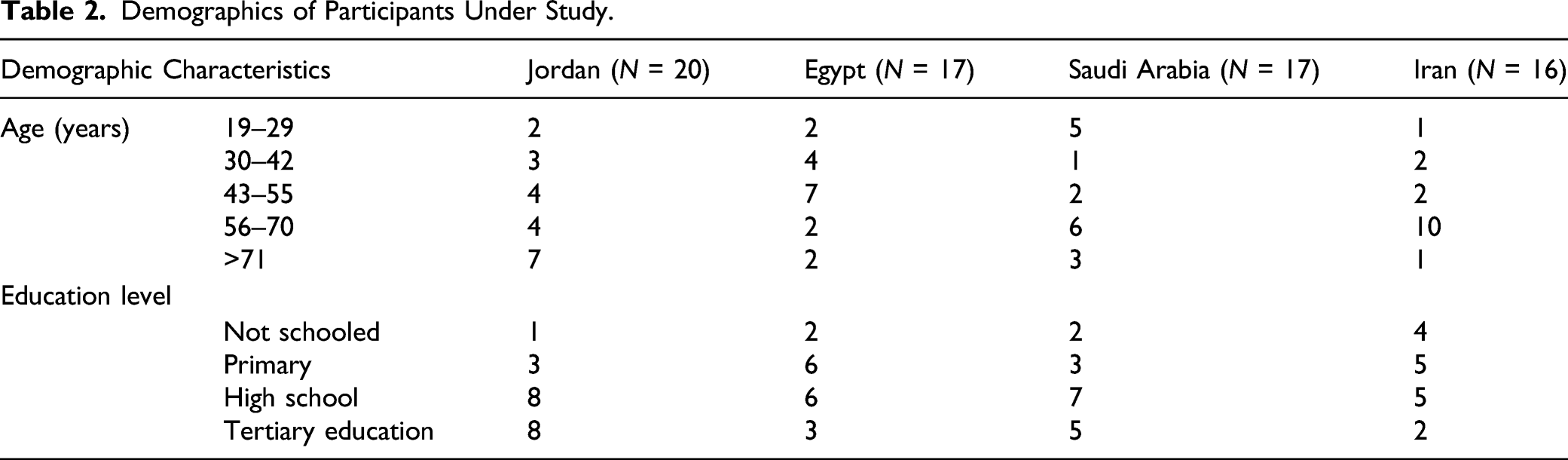
Participants were recruited from a larger qualitative study on folk models and traditional practices in the Middle East (Arabiat et al., 2021; Shaheen et al., 2020). Our study focused on women from four Middle Eastern countries: Egypt, Jordan, Saudi Arabia and Iran. These countries were chosen due to their location and research collaborations in place. Although the four countries are ethnically diverse, they share common beliefs and traditional heritage (AL Jabery and Arabiat, 2019; Mansfield, 2019). The shared history and heritage of faith underpin a wide variety of traditional practices. Hence, those countries were considered ideal locations for the study. With this variation in mind, a sample size of 20 participants in each country was sought (Boddy, 2016). Recruitment was limited to women aged ≥18 years with parity, able to speak and understand Arabic for women residing Egypt, Jordan and Saudi Arabia or Persian for women residing in Iran.
Recruitment and data collection
The first author e-mailed a contact research person from each country to introduce the study and seek support to recruit participants from Egypt, Jordan, Saudi Arabi and Iran. Ethics approval was then obtained from Princess Nourah Bint Abdlrahman University (IRB dated 18 May, 2015), The University of Jordan (IRB dated 26 May, 2016), Suez Canal University (IRB dated 19 July, 2017) and Arak Medical University (IRB dated 27 January, 2019). Data were then collected by means of a face to face semi-structured interview conducted in each country and lasted 30–60 minutes.
Both convenience and snowball sampling techniques were used to recruit participants. We used flyers, which were posted both in public places and social community settings to introduce the study, in addition to using a snow-balling technique to further identify potential participants who in turn may recommend others. Researchers clearly explained to participants the purpose of the study and participants were assured that any information they disclosed would remain confidential and would only be used for study purposes. Participants were provided with information about the general purpose of the study, approximate time to complete the interview, anonymity and the voluntary nature of participation.
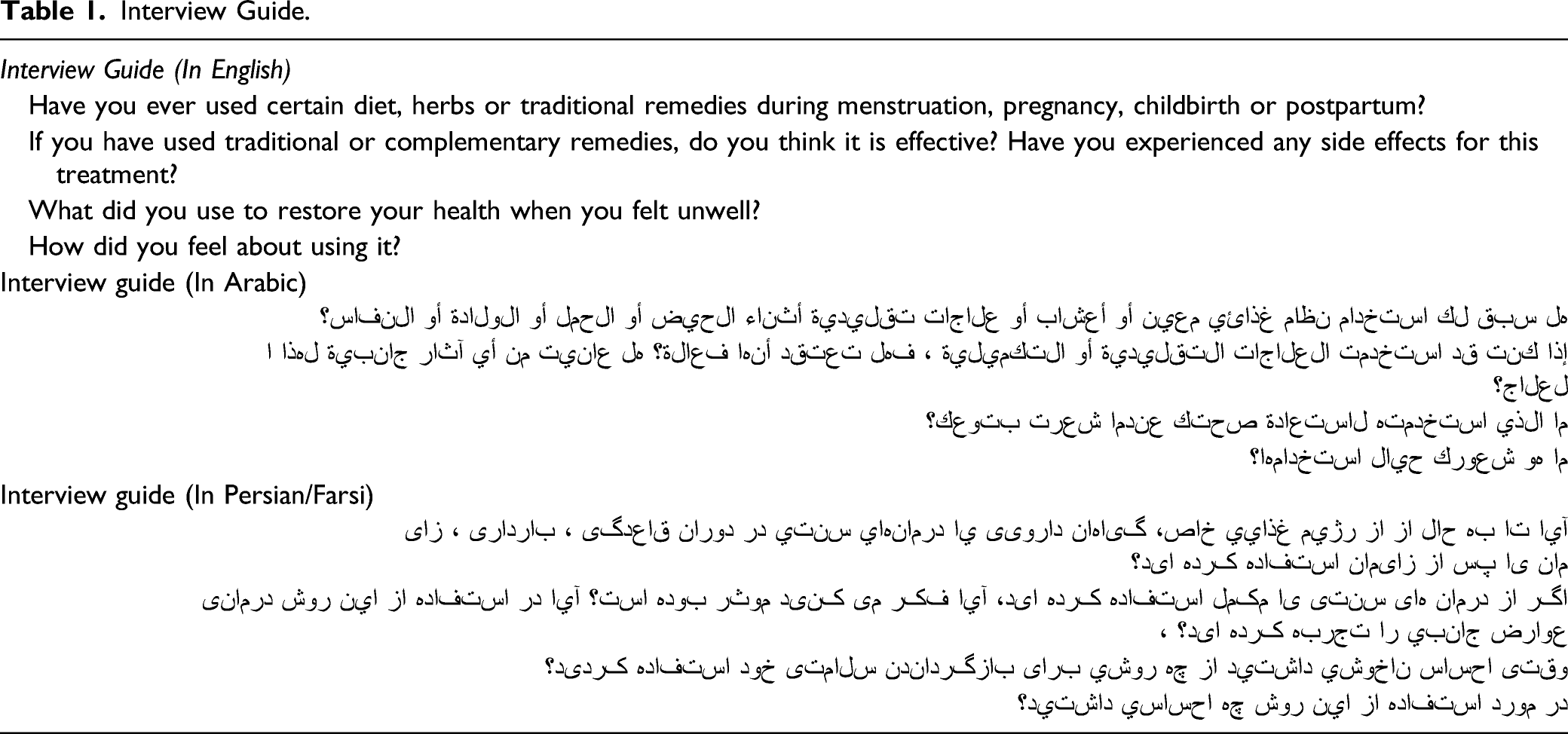
Interviews
Interview Guide.
Data Analysis
Qualitative data analysis described by Boyartzis (1998) was used to identify the major recurring themes in the interviews. For the purpose of this study, we extracted data related to women’s use of CM during their childbearing years.
A theme in this study was described as ‘a pattern found in the information that at a minimum describes and organises the possible observations and at maximum interprets the phenomenon’ (Boyatzis, 2007, p. 3). Analysis involved reducing the data to significant statements or quotes, and then identifying themes to draw together significant statements and coherent patterns (Braun and Clarke, 2006). Analysis then moved on to compare themes across transcripts and explore relationships.
Data analysis was conducted by three members of the research team (DA, SG and NN) and then discussed and approved by the rest of the team. Issues related to credibility, transferability, dependability and confirmability were addressed to ensure trustworthiness (Nowell et al., 2017; Shenton, 2004). Credibility was addressed through regular debriefing meetings to discuss data collection procedures and the analysis procedure, in addition to keeping an audit trail of decision making and coding schemes (Shenton, 2004). Prolonged engagement and searching for rival explanations were strategies used to enhance dependability, while using an audit trail and a research team with diverse perspectives and experiences enhanced confirmability (Shenton, 2004). Representative quotes were selected to support the findings. Pseudonyms are used to preserve anonymity, although quotes are identified by participant’s country of origin. Strategies to enhance transferability included using purposeful criterion sampling and collecting data from a diverse population with different demographic characteristics and comparing findings to published literature.
Results
Demographics of Participants Under Study.
Structure of Themes, Subthemes and Categories as Described by Women Describing their use of CM.

Women’s Experiences of Using CM
For most women, the use of CM was described as intrinsic to their traditional health beliefs and an integral part of their self-care practices. Their CM use was embedded in current practices related to: (a) Easing pain and discomfort; (b) Tackling concerns about infertility and (c) Pregnancy, labour and postpartum care.
Easing Pain and Discomfort
A common thread throughout the interviews was women’s experiences of using certain herbs to ease pain and discomfort associated with menstruation (e.g. pain, bloating, nausea and vomiting or back pain), as well as in self-managing infection (e.g. candida and vaginal discharge). A few women described experiencing dysmenorrhoea and used several herbs to ease pain and discomfort (e.g. marjoram, fennel, chamomile tea and cinnamon). This was exemplified by a participant who explained ‘I’ve used several things such as germander and yarrows….it is very helpful for pain, as well as for reliving bloating and nausea feeling’. (Amal, Jordan).
Women spoke of other strategies they used to ease other symptoms associated with menstruation, such as bloating or nausea and vomiting. This included using ginger, mint and marjoram. The use of herbal medicine was also perceived as an effective measure to control symptoms of discomfort such as itchiness related to vaginal infections, and other abnormal discharge that a woman may experience related to intrauterine infection or inflammation: ‘I used it while being pregnant (refers to CM). I used to have vaginal secretions and recurrent infections down there, so I used an onion and applied it externally on a cotton pad and it relieved all my discomfort’. (Manal, Egypt) Another woman stated: I added turmeric to milk to help with my menstrual cramps, as well as using heat pads. For nausea during menstruation, I had ginger honey tea. Sitting on hot bricks is also very effective for reducing pain in the perineal area, tummy and back. (Fatema, Iran).
In order to manage nausea and vomiting during pregnancy women used herbal tea, consisting of certain plants with special medicinal properties. In addition to herbs, women described using certain food and diets to control symptoms such as heartburn during pregnancy using traditional lentil soup and eating fresh cucumber. The most common CMs used by women in all countries were ginger and mint. For example, Mia (Egypt) stated: ‘When I was pregnant with Fatema, I often had colic pain and discomfort, so I was boiling mint with water and drank it and then felt much better’. Anoad (Saudi Arbia) recounted using mint and ginger for nausea, and Warda (Iran) reported using mint to manage bloating during pregnancy.
Tackling Concerns About Infertility
Women talked about using CM to balance hormones and/or to overcome infertility issues drawing on their own experiences and what they heard from older women. For example, Muna (Jordan) stated: ‘You know the soybean and cyperus [but grass] is helpful too … it increases women’s fertility and I used it often’. Whereas, Amal (Jordan) shared this information: ‘Other women told me that sage boosts women’s fertility and that majora moriganum regulates women’s hormones’. On the other hand, some women were advised not to use some CM to prevent miscarriages. For example, Mayam (Iran) stated: ‘I had a miscarriage once, so in the next pregnancy I was told not to drink echium amoenum and achillea millefolium and saffron tea because these plants cause miscarriage’.
Women also described the use of other CM approaches that did not include herbal medicine, and instead included the use of cauterisation. Rana (Jordan) stated; ‘Before falling pregnant, I used cauterization to assist with the infections and my infertility, but it was not useful’. Another woman described using spiritual practices, such as Quran recitation as a CM.
I have used it once (refers to CM). I was told that I have a jinn buddy (a spirit) that is causing my miscarriage, so they did certain spiritual rituals with Quran recitations and massage to the abdomen with olive oil and incense. I am not sure it made a difference, but I am sure it is harmless. (Nada, Egypt).
Another participant described what we may call as folk tales or old wives’ tales:
‘I had multi miscarriages before, so I was told to bring an egg, boil it and eat it with the skin on…. then I was told to collect the leftover of the bread’s wheat that I often bake and to bake it separately. I did that and since then I had no more miscarriages. (Asma, Egypt)
Pregnancy, labour and postpartum care
The majority of women reported the use of CM during pregnancy and after childbirth. The use of CM was a commonly reported response to a wide range of ailments during pregnancy, including gestational diabetes, hypertension and infection. For example, a woman reported the use of olive leaves and other herbal teas as a part of the self-management of hyperglycaemia. She used both homemade and commercially prepared mixtures, which were mostly herbal in nature. At work, when testing my blood sugar during my last pregnancy, it was high…I started drinking olive oil leaves and it helped my blood sugar to remain normal… it is effective and till now I do my best to drink it every morning. (Khawla, Jordan)
Others reported the benefits of using herbs during pregnancy: ‘While pregnant, I drink mint tea or dry powder of mint leaves in yogurt or salad and it works well against infections. ...During my pregnancy, my blood pressure was high, I used Roselle [Hibiscus sabdariffa] and got results’. (Slam, Iran)
Women spoke also of using CM to facilitate their labour. Several women described eating dates or fenugreek during the last month of pregnancy to induce labour. This was a common practice for all women interviewed, and for some the use of dates was sanctioned because it was included in the Quran (Muslim’s holy book). Only a few women described using Castor oil or certain foods to induce labour.
To help restore their health during the postpartum period, mothers also used a hot herbal tea made of cinnamon and coconut, which was taken for pain relief, washing out postpartum blood and improving weight loss. During the postpartum period, we usually soak fenugreek with cumin, penea, myrrah and fresh turmeric and it is taken every morning. This infusion is taken once a day during the postpartum period… The Alkanet is placed directly on the episiotomy to facilitate healing and prevent infection…This is a very effective practice that we’ve inherited and still practicing. (Sama, Saudi Arabia)
Women described using dates and municipal ghee, and a variety of herbal products such as caraway and fenugreek to help restore energy after birth, strengthen the body, prevent anaemia and to improve lactation. For example, Mia (Egypt) drank Fenugreek with honey, Maryam (Iran) ate a ‘healthy mixture of fried wheat flour, saffron, rosewater, cardamom and sugar with animal butter (cow or sheep)’, and Areej (Jordan) advocated for the use of sweets made of Fenugreek and other made of Caraway.
Perceived Impact of CM
Women’s perceptions of the impact of CM were grouped into two subthemes: (a) perceived usefulness of CM and (b) perceived safety of CM.
Perceived Usefulness of CM
Women valued the use of CM differently. For pain and discomfort related to dysmenorrhoea, most women in Egypt, Jordan, Saudi Arabia and Iran were positive and generally described feeling in control and satisfied with its results, adamant that the herbs or other CM (e.g. heat pads) they used ‘worked well’ for the symptoms they were treating.
On the other hand, some women questioned the efficacy of CM and preferred to seek appropriate medical advice. One woman recalled: ‘My family has always prepared herbs tea to help me feel better during menstrual pain and during pregnancy, but for me, I only felt reassured seeing a proper doctor’. (Suzy, Egypt)
Some women neither agreed nor disagreed with the use of CM and described going through a process of ‘trial and error’ when using CM to self-manage their symptoms and to determine whether CM or certain herbal treatments were effective or not. During the first four months of my pregnancy, I had severe nausea and vomiting. So sometimes I was hospitalized. The doctor did not prescribe anti-nausea medication because he said it was harmful to my baby. On the advice of my family, I used some herbal remedies such as ginger or cooked lamb tripe, but it didn’t work. (Alia, Iran)
While some women appreciated the use of cupping and certain herbs in treating fertility problems, others reported that the use of CM is not effective for most infertility cases and expressed uncertainty around its value. One woman stated: ‘I used traditional methods before pregnancy, but because of the many problems I had during my pregnancy, I was very worried and decided to just listen to my doctor and do what she said’. (Laila, Iran) Similarly, another woman stated: ‘It [CM] is not always effective. I used Fenugreek and myrrah for a miscarriage I had, but you can’t rely on it and sometimes there are side effects’. (Noor, Saudi Arabia)
Perceived Safety of Herbal Medicine
The most common reason for using traditional medicine in pregnancy was the perceived safety and natural properties. Women believed CM use during pregnancy was safe because they were ‘harmless’ and, unlike prescribed medications, did not have side effects. Herbal remedies have no side effects. If someone is doing traditional healing work, if he is experienced, I will accept his recommendations and follow his instructions…… Because I was worried and didn’t want to use the medicines and ointments that doctors give because it might be harmful for my baby. (Asma, Iran)
Other women spoke about their reluctance to use certain herbs during pregnancy, such as cinnamon, cumin or sage for fear of toxicity and adverse reactions, including causing miscarriages and early contractions. Some women understood there were contraindications regarding the use of herbs during pregnancy. One woman stated: ‘I learned that I should consult my doctor before taking these herbal medications [referred to echium amoenum and achillea millefolium and saffron tea] because many herbs are contraindicated during pregnancy’. (Anna, Iran).
Cultural Beliefs and Roles of Women
Cultural beliefs were reflected in women’s decision to use CM. Identified cultural beliefs and roles of women included: normalisation of pain or discomfort and the perceived holism of certain dietary and health practices.
Normalisation of Pain or Discomfort
Some woman stated that seeking professional help for menstrual pain and early pregnancy were not worthwhile, as they perceived pain or discomfort as ‘normal’ I would have used anything that time to manage my pain since my mom thought it would not be appropriate to go to a doctor for a normal thing (refers to menstrual pain) …. people will assume that I may have a problem and she feared I may face problems getting married (participant laughing). (Dana, Jordan).
Moreover, it was common for women to search for CM throughout both menstruation and pregnancy before seeing medical personnel. This practice stems in part from the idea that women do not seek medical advice unless the woman was ill or something was wrong. For example, Rasha (Egypt) stated: ‘My husband used to travel frequently and therefore my mother in law was helping me with a few traditional remedies to manage the health issues I had…at least till he returns and takes me to a doctor’.
Holism of treatment
The perceived holism of certain dietary practices, mainly those described as ‘prophetic food’ or part of ‘prophetic medicine’ such as hijama/cupping facilitated women’s decision to use certain CM treatments to promote their health during and after childbirth. The symbolic value of certain traditional diets (e.g. dates, honey and olive oil) as a ‘blessed’ diet was described by some participants who felt that certain CM treatments harmonise with their faith and cultural beliefs. One woman stated: ‘Olive oil came out of a blessed tree and honey is a blessed food so if they do no good, then it causes no harm’ (Feryal, Jordan). Similarly, another woman stated: ‘No doubt dates, honey and black seeds work well because they were used by Mary when she gave birth to Jesus…it is sunnah (refers to eating dates as part of faith rituals)’. (Anood, Saudi Arabia)
Discussion
This study did not attempt to quantify women’s practices of CM; rather, it intended to describe women’s perceptions regarding their use of CM among women during the childbearing years from Egypt, Jordan, Saudi Arabia and Iran. Our study found that women described experiences of using CM to ease pain and discomfort; to tackle concerns about fertility; and to promote health during pregnancy, labour and postpartum. Generally, women in Egypt, Jordan, Saudi Arabi and Iran used herbal teas made of ginger or mint for managing symptoms of nausea during pregnancy and menstruation, as well as using certain diets (e.g. lentil and cucumber for heartburn during pregnancy, and dates or fenugreek during the last month of pregnancy or during the postpartum period). Overall, herbs were more likely to be used than cupping and acupuncture. This is consistent with other studies from Palestine (Al-Ramhi et al., 2013), Egypt (Orief et al., 2014) and Iran (Khadivzadeh and Ghabel, 2012) which demonstrated acupuncture, meditation and massage are less likely to be used by women in the Middle East.
A second major theme in our findings related to the perceived impact of CM on women’s health. These findings suggested that some women have a high level of trust and satisfaction in the use of herbs as a safe alternative to antibiotics and other prescription drugs. Ingestion of camomile, mint, chaste tree or dill seeds described by women for menstrual pain have also been described in earlier research (Hardy, 2000; Ghaderi et al., 2016). The use of marjoram during menstruation has been used by women for its anti-inflammatory and antimicrobial properties (Tajallaie-Asl et al., 2017).
This study found that ginger was used widely to control morning sickness during pregnancy and reflects findings from China (Withers et al., 2018), Canada (Hollyer et al., 2002) and Egypt (Orief et al., 2014). While earlier studies described the safe use of ginger during pregnancy, there is a need to highlight the importance of counselling before it is used, as ginger may increase the likelihood of bleeding and can cause cardiac arrythmias or central nervous system depression, if used excessively (Mehrpouri et al., 2020).
In line with earlier studies from Palestine (Al-Ramahi et al., 2013), Iran (Khadivzadeh and Ghabel, 2012), Egypt (Orief et al., 2014) and Thailand (Kruekaew and Kritcharoen, 2018), the current findings indicate that increased and frequent consumption of dates was a common behaviour among women during the last month of pregnancy. An earlier clinical study suggested that dates are associated with a reduced need for induction and augmentation of labour (Al-Kuran et al., 2011). A less common CM reported by women from Egypt and Iran was the consumption of eggs to induce labour. The belief that eggs may induce labour or increase the risk of abortion or miscarriage is consistent with findings from Thailand (Kruekaew and Kritcharoen (2018).
Another common herbal medicine used by women in the postpartum period was cinnamon tea. Similar to other study findings, cinnamon was used to reduce perineal pain and improve healing following episiotomy (Mohammadi et al., 2014), as well as to control postpartum haemorrhage, menorrhagia and flooding during miscarriage (Ali-Shtayeh and Jamous, 2008). Postpartum women from Egypt, Jordan, Saudi Arabi and Iran used special tonics made of ghee. The use of diets high in protein, such as ghee was reported by women in India, and the use of herbal plants such as artemisia by Malaysian women (Dennis et al., 2007). Artemisia (tree wormwood, or sheeba in Arabic) was used in steam baths and vaginal washing by some women in this study. Use of artemisia extracts to support the flushing of natural toxins from the body, and in treating vaginal infection and vaginal candida was also described in a recent study (Saber-Mohammad et al., 2018).
Overall, our findings showed awareness of potential side effects and toxicities related to some herbal medicines. This indicates that women may have in-depth knowledge of herbal medicine, which is congruent with an earlier study from Ghana (Peprah et al., 2019), in which the authors suggested that traditional knowledge of herbs is the result of experiences accumulated through generations as well as knowledge through increased media on the safety of herbal medicine.
Given the link between beliefs and practice, it is not surprising that cultural norms and roles of women were identified as a major theme in this study. Our findings considered the possibility that certain cultural expectations created prescribed cultural roles within which women should normalise their feelings of pain or discomfort. Consistent with earlier studies (Ali-Shtayeh et al., 2015; Armour et al., 2019; Wood et al., 2007), cultural expectations around women’s health and the normalisation of pain contributed to women’s health-seeking behaviours, including the decision around when it was acceptable to access formal healthcare services.
Prophetic medicines according to Sheikh et al. (2017) are defined as the intake of dietary materials or plants or herbals such as Nigella Sativa (black seeds), Cymbogon citratus (lemon grass), ginger, honey and truffles that were used as remedy recipes and consumed as food elements by the Prophet Mohammed (PBUH). Our findings are in line with Peprah et al.’s (2019) argument that women strive for holistic health and ‘holism’ motivates them to seek traditional medicines over conventional medicine.
Strengths and Limitations
This is the first qualitative study to examine women’s use of CM across four different countries in the Middle East. Although our study lacked sufficient demographic data to examine how women’s socio-economic status is associated with CM use, it provided insight into women’s experiences of using herbal medicine across four countries during childbearing years. In terms of the research methodology, following Nowell et al. ’s (2017) model for enhancing the trustworthiness of thematic analysis, our analysis was conducted with rigour and transparency. Themes that emerged in this study were all verified by the authors (DA, SG, and NN) and all authors reached consensus on the final interpretation.
While our study provides insight into the use of CM by women in Egypt, Jordan, Saudi Arabia and Iran, our findings need to be considered within the context of the following methodological limitations. First, women were only sampled from one or two cities within each country, thus limiting the generalisability of the findings beyond those communities (Shenton, 2004). Second, whilst our study is the first to collect data across countries, our findings may not be applicable and transferable to other Middle Eastern countries. Third, we were unable to reach saturation as there are likely many variations in women’s experiences with CM use in each country. Data from a wider more representative sample are needed. Fourth, we did not examine variation in availability of certain CM or its association with women’s health beliefs or their decision to self-medicate, underscoring an area for future research. Finally, although the women who participated in this study were all encouraged to openly share their use of CM, there is always the potential for recall bias in interviews based on past experience.
Implications
The use of CM among women is not uncommon
Conclusion
Women described using several plants to promote their health and/or to self-manage health aliments during menstruation, pregnancy and after childbirth. Women’s perceptions of the effectiveness of CM was varied, with most women reporting high trust in the safety of herbs and their efficacy in easing pain and discomfort, but not when used during pregnancy or for fertility concerns. Cultural beliefs in the forms of cultural roles of women and using ‘Prophetic medicine’ generally contributed to the high use of herbs among women. To provide the best evidenced-based care for women during their childbearing years, nurse and midwives are recommended to remain aware of and updated on these practices and the safety of CM to support women’s health and wellbeing.
Supplemental Material
sj-pdf-1-gqn-10.1177_23333936211042616 – The Use of Complementary Medicine During Childbearing Years: A Multi-Country Study of Women From the Middle East The Use of Complementary Medicine During Childbearing Years: A Multi-Country Study of Women From the Middle East استفاده از طب مکمل در دوران باروری: یک مطالعه چند کشوری درزنان خاور میا نهاستخدام الطب التكميلي خلال سنوات الإنجاب: دراسة متعددة البلدان لنساء من الشرق الأوسط
Supplemental Material, sj-pdf-1-gqn-10.1177_23333936211042616 for The Use of Complementary Medicine During Childbearing Years: A Multi-Country Study of Women From the Middle East اس
Footnotes
Authors’ Contribution
DA and LW conceived the study. DA, SG, NN performed the analysis. SG, NN, EAS, NS, IS and RK collected and extracted relevant data. All authors contributed to manuscript preparation and revision for intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded through the University of Jordan in Amman and by Arak University of Medical Sciences in Iran.
Ethical Approval
All identifying information regarding the study participants has been omitted and this study was approved by the Scientific Research Committee at the Faculty of Nursing at the University of Jordan, Suez canal university in Egypt, Princess Nourah University in Saudi Arabia and Arak University of Medical Sciences in Iran.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.