
Abstract
Studies document that osteoarthritis-related joint pain is more severe in African American older adults, but research on the personal experience of osteoarthritis pain self-management in this population is limited. Using a qualitative descriptive design, our objective was to extend our understanding of the experience of life with osteoarthritis pain. Eighteen African Americans (50 years and older) were recruited from Louisiana to participate in a single semi-structured, in-depth interview. A conventional content analysis revealed that “Bearing the pain” characterized how older African Americans dealt with osteoarthritis. Bearing the pain comprised three actions: adjusting to pain, sharing pain with others, and trusting God as healer. We discovered that a metapersonal experience subsumes the complex biopsychosocial-cultural patterns and the intricate interaction of self, others, and God in living with and managing osteoarthritis pain. Study findings have implications for application of more inclusive self-management frameworks and interventions.
Osteoarthritis (OA) is one of the most common and pervasive causes of debilitating chronic pain and disability that affects more than 30 million adults (Cisternas et al., 2016) and represents the fourth most common reason for hospitalization (Lockett et al., 2019; Murphy & Helmick, 2012). Although racial minorities only account for three million of OA cases (Deshpande et al., 2016), OA in older African Americans is characterized by the severest forms of joint pain, functional and activity limitations, and decreases in mobility (Barbour et al., 2016; Vina et al., 2018). The incidence and progression of disease for both hip and knee OA is worse in African Americans compared with Caucasian Americans as indicated by greater severity of radiographic (i.e., more joint osteophytes and bone degeneration) and symptomatic OA (i.e., greater pain, aching, stiffness; Braga et al., 2009; Kopec et al., 2013; Murphy et al., 2016; Nelson et al., 2013). This may explain why severe OA pain affects a higher proportion of African Americans (38.7%) than any other racial population (i.e., 36.4% Hispanic Americans, 28.7% American Indians, 23.1% Caucasian Americans, 18.5% Asian Americans; Bolen et al., 2010). As a corollary, African Americans report significantly higher perceived arthritis-related stress than Caucasian Americans (McIlvane et al., 2008), which may limit the ability to effectively and consistently manage OA pain. Despite such negative outcomes and the psychosocial burden of living with OA (Harris et al., 2015), there is limited understanding on the experience of managing OA in later adulthood, especially in minority older adults including African Americans (Borkhoff et al., 2011).
OA pain and subsequent functional limitations are controlled through self-management, which is the daily process and tasks that an individual takes to monitor and manage symptoms, adhere to prescribed treatments, and adjust lifestyle to a changing health condition (Grey et al., 2015). Self-management may also include managing one’s everyday thoughts; communicating with family, friends, and providers; and dealing with others’ perceptions and stigmas. However, older African Americans continue to be underrepresented in pain research, and in return, our ability to support effective self-management through research generation and utilization is restricted. Research to date has focused, in isolation however, on elucidating and understanding ethnic differences in coping and beliefs (Golightly et al., 2015; Meints et al., 2016; Orhan et al., 2018), self-care strategies (Albert et al., 2008; Park et al., 2014; Silverman et al., 2008), communication patterns (Puia & McDonald, 2014), and disparities in total joint replacement (Bass et al., 2016; MacFarlane et al., 2018). African Americans are more likely to use spirituality/prayer, thermal modalities, creams, and nonsteroidal anti-inflammatory drug (NSAID) medication compared with other ethnic groups and to involve family and friends in their self-management decisions (Booker, Herr, & Tripp-Reimer, 2019; Park et al., 2014). However, many studies conclude that marked racial differences in treatment and OA outcomes are not entirely explained by sociodemographics, disease severity, social support, or trust in health care system. Unexplained differences can be attributed in part to (a) investigations of older African Americans’ self-management practices with little context, knowledge, or understanding of African American/Black culture and (b) a propensity to study interracial differences between Caucasian Americans and African Americans, further reducing the opportunity to fully understand the degree of intraracial patterns of engagement in OA pain self-management. As a result, we have important but partial evidence, rather than a complete picture, of older African Americans’ experience of managing OA. Thus, viewing older African Americans’ experience out of context limits a deep grasp of the subtle or explicit nuances that affect how the symptom experience is navigated in their daily lives.
Purpose
The goal of this study was to extend the understanding of the personal experience of life managing OA pain in older African Americans.
Methods
Design
The current study used a qualitative description approach (Bradshaw et al., 2017; Sandelowski, 2010) and was part of a larger multiple-method study (Booker, Herr, & Tripp-Reimer, 2019; Morse & Niehaus, 2009). Pain is a subjective phenomenon that is best identified, described, and understood based on individuals’ descriptions. But more importantly, pain is a common universal issue for nurses who strive to limit the suffering of patients; hence, qualitative description is well suited to answer the following research questions and to develop new patient-centered knowledge that prompt pragmatic ways of helping people outside the acute care setting mange pain: How do older African Americans manage OA and chronic pain? What is their experience of living with OA, and what patterns, processes, and responses emerge thereof?
Indeed, qualitative description is “epistemologically credible” and a suitable methodological base to present participants’ raw descriptions of OA pain. Qualitative description is particularly relevant to this study as it allows researchers to stay “close” to the data, without delving deep into interpretation of the abstract or engaging in significant re-presentation of the data (Bradshaw et al., 2017; Sandelowski, 2000). Therefore, data are not overanalyzed or interpreted with a deep structure, but rather are interpreted from the participant’s point of view (known as manifest content), maintaining a high level of cultural congruency, interpretative accuracy, and emic concreteness. Qualitative description is especially useful when there is limited evidence of a phenomenon (Bradshaw et al., 2017), such is the case with the experience of OA pain in older African Americans, and allows for a more descriptive investigation of the “contextual cultural factors that shape participants’ experiences” (Willis et al., 2016, p. 1198).
Our study placed emphasis on older African Americans’ worldview to elucidate contextual data on the thoughts/perceptions that influence how older adults communicate and engage in personal, interpersonal, cultural, and community-based self-management within the African American/Black culture, paying close attention to cultural distinctions/nuances, historical references, and familial descriptions. The University of Iowa Institutional Review Board (IRB) for Behavioral and Social Sciences approved the study protocol and study materials (IRB protocol #201601784). All participants provided consent to be interviewed and audio-recorded and were compensated for participation with a US$15.00 gift card to a local retail/grocery store and educational resources on managing OA.
Participants and Sampling
African Americans 50 years or older were purposively sampled from three major communities/cities in northwest and northeast regions of the state of Louisiana (United States) using maximum variation sampling varying on age group (50–64, 65–74, and 75 and older), gender, and education attainment and stratified by the level of pain to ensure sufficiently rich and relevant data (Booker, Herr, & Tripp-Reimer, 2019). Northwest and northeast Louisiana has the highest rates of arthritis, severe joint pain, and arthritis-attributable activity limitations compared with other geographic regions in Louisiana (Barbour et al., 2018). As a result, we had an appropriate pool of participants. Primary recruitment strategies centered on community outreach efforts to develop a genuine presence in the community, including participation in multiple organizational and church-based health fairs and health seminars (n = 8) over a 6-month period, and providing presentations on OA and pain management to senior groups and social clubs. Exclusion from the study was based on self-report of Hispanic ethnicity, other pain-related and neurological conditions (e.g., rheumatoid arthritis, lupus, sickle cell disease, Parkinson’s disease, and cerebrovascular accident), cognitive impairment (defined by a score <15 on the Animal Naming Test), and residence in a long-term care facility. Our methods are elaborated elsewhere (Booker, Cousin, & Buck, 2019; Booker, Herr, & Tripp-Reimer 2019).
Data Collection Procedures
All audio-recorded interviews were conducted in English during a time of day convenient for the participant. Interviews began with a general statement explaining the study purpose and strategies to maintain data safety. A one-time individual interview was conducted face to face by the principal investigator (PI; i.e., S.Q.B.) primarily in participants’ homes or their self-owned business between April 2016 and February 2017. These natural settings offered older African Americans the space, comfort, and time to share their thoughts. A PI-developed semi-structured interview guide, with probing questions (Table 1), elicited older African Americans’ experiences of living with OA, illness representations, daily management of OA, and social support structures to improve self-management capability. The interviewer also kept field notes on key participant statements, behavioral observations, and the researcher’s thoughts to clarify participants’ comments but field notes were not included in the current analysis. The interviewer’s hand-written field notes including reflexive statements were typed into more detailed field notes in Microsoft Word within a 24-hour period. The interviewer attempted to identify, monitor, and bracket out potential biases, stereotypes, or presuppositions (Bradshaw et al., 2017).
Semi-Structured Interview Guide
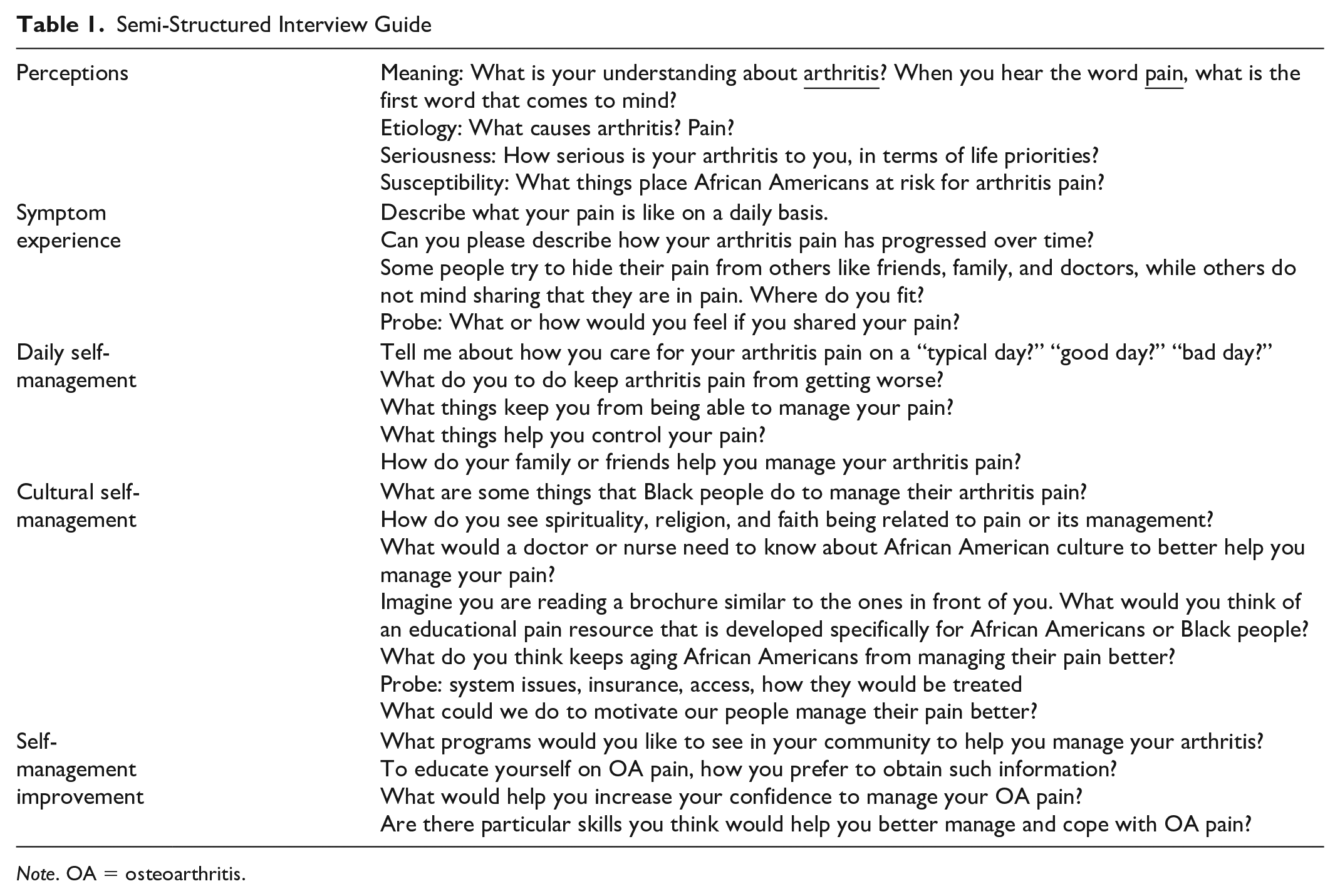
Note. OA = osteoarthritis.
Data Analysis
The interviews lasted between 37 and 106 minutes (
A systematic qualitative coding process was conducted in three stages. Stage 1 involved data familiarization and immersion by multiple readings of five transcripts and creating a narrative summary of first impressions by two coders (i.e., S.Q.B. and T.T.-R.—an experienced nurse anthropologist). Stage 2, over the course of the multiple readings, labels for inductive codes emerge that were reflective of salient key points. This served as the foundation for the initial coding template. Focusing on patterns in the data, each transcript was discussed, and the templates were combined to generate a more robust coding scheme. This coding scheme, consisting of 204 codes, was applied to the remaining 13 transcripts using HyperRESEARCH™ (ResearchWare, Inc., Version 3.7.3). After all transcripts were coded, Stage 3 proceeded with both researchers convening to organize content into meaningful clusters (N = 44) and then finally reduced into minor themes (N = 10), major themes (N = 3), and an overarching theme (N = 1). This means that minor themes were grouped into major themes, and together, these major and minor themes were assigned an overarching theme that summed up the self-management experience of older African Americans with OA pain. We were careful to preserve the essence of the participants’ voice, using their narratives to develop thematic titles; hence, our results include rich individual quotes (with assigned pseudonyms) as well as combinations of quotes from multiple participants to form a cohesive narrative. Following data analysis, a trifold pamphlet expressing gratitude for participation and reporting the study’s major results in plain language was mailed to each participant.
Rigor
To ensure trustworthiness and confirmability of the data, two coders with experience in pain/health disparities and anthropology independently coded transcripts and analyst triangulation ensured robust and well-developed themes. Intercoder reliability and credibility of themes were achieved by (a) discussing issues with coding in weekly team meetings over a 3-month period, (b) reconciling issues through careful rereading, conversation, and consensus, and (c) collectively aggregating codes into meaningful categories until an accurate interpretation of data was reached. If consensus was not reached, two codes were developed, prompting the interviewer to reread relevant transcripts and review the literature to identify support for either code or retain both codes, with clear definitions for each. Transferability to similar populations of African Americans was addressed by (a) giving a clear description of culture and context, (b) using two purposeful sampling techniques, stratified purposive sampling and maximum variation so that findings could be later applied or adapted to other similar populations, (c) collecting and reporting demographic characteristics, and (d) comparing our findings with literature.
Results
Participant characteristics: Eighteen African American adult men (N = 9) and women (N = 9) provided rich accounts of a multifaceted and varied life experience with OA pain. Participants ranged in age from 50 to 85 years, with a mean age of 67.94 (SD = 10.93) and were from rural and urban communities. 89% had moderate (N = 8) and severe pain (N = 8), while the remaining 11% (N= 2) reported mild pain. Those with severe pain were more likely to experience constant pain in contrast to individuals with moderate pain who experienced more intermittent pain. By sampling design, there was a mix of education levels: <high school (N = 4), = high school (N = 8), and college (N = 5).
Thematic results: “Dealin’ with it,” emerged as a robust and overarching theme from the qualitative data analysis. Within this overarching theme, three major themes were identified: (a) bearing OA pain, (b) understanding OA pain, and (c) controlling the pain. The first theme relates to the daily and personal experience of living with chronic pain. The second theme described older African Americans’ explanatory illness models of OA and joint pain, and the third theme encompasses more specifically the nature of experiencing pain and the ways in which they use coping, self-management tools, and provider involvement. Due to the richness and depth of the three major themes, this article focuses on one major theme, “Bearing the pain,” to allow for adequate representation of participants’ experiences. The remaining two themes will be presented in future publications.
Bearing the Pain
“Bearing the pain” is an inclusive expression and experience of living with chronic OA pain and comprises three central actions (i.e., minor themes): adjusting to pain, sharing pain with others, and trusting God as healer (Table 2). From multiple participants’ perspective, OA was just one of them things you have to deal and live with it. This left many older African Americans to “ . . . just
Thematic Structure of Results


Note. OA = osteoarthritis.
Adjusting to pain: An intrapersonal process
Adjusting to pain encompassed two divergent elements: (a) accepting OA and (b) not claiming OA.
Accepting OA
Adjusting to pain involved learning to accept it and try to deal with it the best way they can. Because most participants had lived with pain for at least 5 or more years, they expected pain on daily basis and had adapted their lives to this reality. As one man expressed, Cuz when the good Lord say, ‘Well, I’m gonna give him a little peace today,’ and then that peace’ll scare you because you don’t feel that pain. You think something else wrong now because like you said earlier, I done dealt with it so long that I’ve adjusted myself to the pain. (Jerry)
We noted that acceptance of pain can be positive or negative, depending on how this acceptance was mentally and emotionally processed. Positive acceptance of pain led to adjustments in their lifestyle to control OA in the best way possible. In contrast, passively accepting pain resulted in misconceptions that OA cannot be prevented or controlled; thus, they expected to develop arthritis because of its heritability. This form of negative acceptance was anticipatory and resulted in powerlessness over the pain and lack of self-management action. For example, one older woman beautifully characterized this passive acceptance as disbelief. She says, Disbelief in that everybody in the family had it, now it’s my turn . . . There’s nothing I can do about it. That’s the worst kinda thought . . . This is something we have to learn to care for, you know. Then, we just get comfortable with it, and don’t know that the comfortableness of it can kill us, too, and make us cripple. I think that there are times when we just accept bad things, even if it’s about our health. We just accept it. (Flora)
Not claiming OA
The contrast to acceptance was not to claim OA. Having an incurable, chronic condition proved difficult, and some early in their prognosis were not ready to face this reality. For some, acceptance was a process, and “it’s natural that you don’t wanna face that somethin’’s going on. They kept tellin’ me it could get worse. I didn’t wanna believe that” (Ada). Participants reported how some in the Black community are reluctant to accept and admit to having arthritis and problems, and resort to denying arthritis altogether. Ms. Claudine explains, A lot of times, a lot of people, I just—they amazes me. People actually, especially us Africans. Now White folks, they gonna own up to theirs and keep on goin’ and do what they gotta do to—I think a lot of us Black, African Americans, I think a lot of ours is pride. A lot of ours is pride. We don’t want no one to know . . . ‘I ain’t got no arthritis’.
The above statement gives credence to the African American cultural-specific colloquial phrase of “not claiming” a disease or condition (Spruill et al., 2015). Several discussed the cognitive process of not “claiming OA”: I began to wonder, “Has the arthritis started to seep back in?” I’m not even gonna claim that, you know what I mean? I’m not even gonna claim that. I know it’s gonna be work, for the rest of my life. The point is, is just not to give up. Don’t stop. Don’t give up. (Vera) When I was ignorant of some things and I confess what they [doctors] told me, that’s what happened to me. When I started to confessin’ the word of God, when I go in and talk to doctors, I don’t tell them I have this. They think I’m crazy. I’m diagnosed with it, but I don’t have it. They look at me and they say, “What do you mean?” I say, “I’m a child of God. I believe in healin.” (Ada)
Not claiming and denying a disease have slightly different connotations in the African American culture—the former taking on a spiritual meaning and serving as a protective mechanism and the latter an intentional disregard of the disease process. In either circumstance, this sentiment of accepting/not accepting arthritis is a major part of how older African Americans deal with pain. Regardless of accepting or denying pain, in essence, participants proactively or reactively adjusted to pain in their own way, of which included not allowing themselves to dwell on it.
Older adults did not allow themselves to dwell on the pain because there was an implied relationship that thinking or talking about pain intensifies its severity and overall power/control in their life. Some adjusted to pain in physical ways while verbally and mentally refusing to focus OA.
Usually, once I get up and get busy, I mean it just—the next thing you know, the pain is gone. I don’t dwell on it. Of course, keeping up, not falling behind in that walking, that particular kind of activity, and doing something, keeping my mind alert and active. I think all of that works well. I belong to about three or four groups, doing something three times a month with them. And so I think, if you’re active, you don’t focus—I don’t focus on the arthritis. I’m well. I keep saying that (Flora).
In addition to keeping the body and mind occupied, involvement in spiritual matters was another strategy that helped take older African Americans’ mind off the pain. “When people get off into the word [the Bible] their pain leaves too. When they be doing some spiritual things, it takes their mind off the pain” (Jerry).
Sharing pain with others: An interpersonal exchange
The second minor theme was “Sharing the Pain” and it also encompassed a dichotomy: (a) hiding and holding back pain and (b) revealing pain. Numerous factors influenced the circumstances under which African American elders revealed and shared pain with others or hid pain from others. The most prominent factor was their perception of others’ failure to believe that OA pain was severe or real, given that pain is not a visible symptom.
cuz people was tellin’ me, “You can’t walk because you don’t wanna get up.” . . . Just like other people in my life because they couldn’t see the symptoms. Cuz I still looked the same at the time. (Ada)
The reaction of others’ to the (in)visibility of pain led to a phenomenon called puttin’ on, or a state of perceived faking or exaggeration (Booker, Cousin, & Buck, 2019). Hence, it was not necessarily the pain or its intensity that influenced older African Americans’ decision not to open up about their pain but sometimes the meaning and stipulations that others would attach to the pain. Internalizing others’ perceptions of their condition manifested as a barrier to fully accepting their own condition and living transparently with OA pain. Anticipating others’ reaction and beliefs more often led to hiding pain rather than revealing pain. Those two tensions, (a) hiding pain and holding back and (b) revealing pain, are discussed herein.
Hiding and holding back pain
Most participants hid pain from others which consisted of not telling others they were in pain, continuing their normal duties to appear “well,” and being cognizant that their physical behaviors or mood were not indicative of pain or discomfort. Perceived lack of emotional benefit, perception of complaining, masculinity compromise, and learned stoicism were a few factors which fueled hiding pain. African American participants surmised that there was no emotional benefit for either party in talking about pain. They believed that discussing pain with others, even family, would not make them hurt any less. Others, especially men, perceived that sharing pain with others was a form of complaining or would be viewed as complaining or a sign of weakness; therefore, they hid their pain: Normally I don’t talk about it to people much. You understand? I got to the point now when people say, “How you feelin’? How you doing?” I’m in pain all the time, but I don’t let them know. What can they do to help me? Nothing. “I’ll pray for you,” and that’s it. The pain’s still here, so I don’t complain about the pain no more. I just keep it to myself. (Samuel)
There were notable gender differences, and most men were uncomfortable discussing pain with others. For these men, talking about pain was a threat to their masculine identities. “Mens wanna be macho and they don’t wanna confess when something get wrong with ‘em” (Charles). Instead, men would use jokes and metaphors to reveal pain, “The ‘ol gray mare ain’t what it used to be,” which was interpreted by others as a metaphor for aging and not pain related. Furthermore, many husbands did not even discuss their pain with their wives who also suffered with OA: That’s just normal. A man has a way of not goin’ to—it’s a man thing. He don’t want people to know he in pain, or he’s sufferin’ in any kind of way, so he just But they won’t talk about it around their women that they’re weak, but when they get around other men, they show weakness to a certain degree. You feel withdrawal with that relationship- talking about that manhood. Everybody’s in a competition for the power and we’re all hurting at the end of the day. [Laughter] I bet you. (Stanley)
Interestingly, when female participants spoke to their husbands about pain, it was viewed negatively as complaining, but when their male partners mentioned their pain to their wives, they did not view their self-expression as complaining. Thus, this gendered pattern was exposed as the following: Women complain (and are emotional) and men simply express their feelings. One example from a woman describing her late husband, [He] used to say that sometimes to me, that, “Complaining about it is not gonna help it, you just—everyday.” I said, “Well, you too. You complaining and don’t realize it.” When I’m talking about it to him, it was complaining, but when he was talking about his pain, I guess he didn’t consider that complaining. (Cassandra)
Participants also recalled how deceased relatives modeled silent suffering, never talking about pain or visiting a provider about arthritis. “She didn’t mention it. My grandma, oooh—because she saw it as weakness. She was dragging everything, dragging that cotton sack with two childrens on it” (Stanley). In particular, one woman discussed the historical origin behind hiding pain as a survival and coping mechanism: We don’t want no one to know. We can’t blame that on self, though. It was instilled in us, cuz if you think about it, back in the slavery, they had to do what they had to do. They had to hold it in in order to survive. We can be in 99—we can be in pain, but we know we got to do the job so we can take care of our family. We gonna suffer through this pain. We ain’t gonna let nobody know it. Back then, your grandparents and parents, they didn’t tell you if they was in pain or was hurtin’ neither. (Claudine) African Americans are probably more capable or better able to accept and deal with pain than others . . . because African Americans have had to deal with so many adverse situations all through life on down through the years. (Cassandra)
Revealing pain
While there was an underlying belief and unspoken norm among both men and women that pain was not an appropriate or important conversational topic, this did not always preclude them revealing or sharing their pain with others, especially when the pain was very severe. For example, two men found it acceptable and helpful to share their pain as an emotional outlet while simultaneously noting that their male friends did not share this same belief. One of the two men stated that “Just group talking. More of that can make it more I was talkin’ to this brother that is right over here. I was tellin’ him, “Man, I was in so much pain the other night, I didn’t know what to do. I didn’t have anything to take.” He said, “What did you take?” I said, “Tylenol PM.” He said, “Sit right where you are.” He went and got me a whole bottle. I told him, “Man, I don’t know how to tell you how much I appreciate.” I says, “Cause I ain’t got no money” [Laughter]. (Walter)
On the other hand, women generally did not mind if others, such as close family or friends, knew they were in pain; however, they did not find talking about and dwelling on pain to be emotionally helpful. This distinct cognitive differentiation between knowing that someone is in pain and not talking about the pain was illustrated in a typical response that was devoid of mentioning pain. For example, participants might say, “I don’t feel good today” or “I’m doing alright.” Most African American women felt it was important to let their friends know when they were not feeling well to prevent their restricted behavior from misinterpretation as not wanting to be bothered or being perceived as acting different or funny.
Trusting God as healer: An extrapersonal necessity
The third minor theme “Trusting God as Healer” exemplified how spirituality played “a big part of me managin’ a lot of time, cuz like I say, some days you don’t stop hurtin’. You just have to make the best of it. I guess faith is what gets you through the day” (Lenora). Because older African Americans understood that OA was a challenging chronic condition, the majority of participants found it necessary to naturally, fall back on their faith and trust God as healer.
Prayer was an essential task for faith and healing, and they considered it be number one! Participants knew that it would be all right once they called on that name [Jesus] and took it to God in prayer (multiple participants). At other times, older African Americans would ask others to pray for them or with them. There were dualities regarding prayer, and these were not necessarily opposing or incommensurable. This duality was to (a) pray for healing and to (b) pray for strength to bear the pain.
Prayer to heal the pain
“Black folk wanna go pray, ‘God, get this pain off of me!’” (Stanley). Hence, prayer for healing centered on God to remove the pain.
Yep. I pray on a daily basis, ask him to relieve any pain, take these pains away. I still feel it. If I forget about the pain, I know that’s his doing ‘cause I don’t feel the pain anymore. Then I realize that the pain’s gone away and the first thing that comes to my mind, “Thank you, Jesus.” Thank you, Jesus, that’s the prayer that you done answered for me. He’s still a prayer-answering God. (Samuel)
Healing was considered a miracle, and it is commonly said in the African American church that God is a “‘miracle-working God.” The prerequisite to healing was exercising faith and belief and trusting God. As one man stated, I do understand that God is in the healin’ business, and if I’m suffering, then I feel He can heal me, whatever goin’ on. That’s the reason why I say all the time that you just got to trust God. (John) If you truly know God and Jesus Christ and what they did for you, it’s gonna help you, havin’ faith that you know God’s gonna heal you, and He gonna give you the strength that you need. That’s the way I look at it. That’s who I depend on as my healer. Well, He is my healer. (Claudine)
Healing the physical body was most often discussed, but eternal healing on the other side was no less important. Candidly, one gentleman stated the following: I don’t think the Bible has helped me a lot with pain management, but it’s helped my attitude toward pain because we believe that—Revelation 21:3 and 4 says, “There’ll be no more pain” . . . In fact, when he sent Jesus here, that’s why he had him curing sick, resurrecting people, just to give them kind of a fore glimpse of what the future could be like. (Everett)
Prayer to bear the pain
While participants looked forward to a time when there would be no suffering, in the present time, they were assured that “ . . . He [God] wouldn’t put more on us than we could
You have faith, and you pray about it, ask to help you make it through it. But then, you go back to the verse in the Bible where Paul had a problem, and he asked the Lord to remove it, and said my grace is sufficient. I said, well, long as he [God] still able to—allowin’ you to get around. (Arthur) When I pray—I’m a firm believer in prayer—I just feel like when I ask God to give me strength and ease my pain—I just say, “Lord, take the pain.” I rub with my stuff, and I go on to sleep [laughs]. You gotta have faith, even when you take your medicine.” (Ernestine) Instead of sayin “Oh, God. Take the pain away.” I usually offer it up for my sins and sins of the whole world. Jesus didn’t die in vain, but I want him to know that I realize how much he suffered for my sins. (Lenora)
Refrain from asking pain to be removed seems to negate their trust in God to heal. However, when contextualized, thankfulness, humility, and cognizance of Jesus’ suffering mediated the gap between praying for strength and trusting God. “When I think about he went to the cross and had many, many pains for us, just because he loved us that much, then I can handle these little old pains I have down here. I think about that, too. God suffered. Why not me” (Iris).
It was evident from our data that older African Americans believed that dealin’ with pain is a personal matter, and their experiences shed light on the competing complexities of relationships with self, others, and God and the processes that accompany living with and managing a chronic condition. This was an important revelation because individuals often engage in self-management in the context of and conjunction with their environment, families, and communities (Grey et al., 2015). Living with OA was a culturally laden experience that involved adjusting to and managing pain on their own, then learning how to reveal pain to others, including family and providers, while allowing God to help and heal them within the context of familial and socialized priming for how the Black people deal or should deal with pain. Reeves and colleagues (2014) determined that “Support for self-management is therefore more meaningfully construed as a collective and networked phenomena, rather than as a set of individualized actions and behavior” (p. 11). This was true for our sample, and we discovered that this intrapersonal, interpersonal, and extrapersonal experience culminated into a metapersonal experience OA. This vivid depiction provides direction for clinical implications but also highlights the need for further research exploration as to the effects of their experience on pain-related health outcomes in African Americans.
Discussion
We have highlighted the multilayered experiences of how older African Americans bear the pain as a self-management axiom. Researchers have contextualized self-management as an individual experience rather than a cultured and social experience steeped in historical tradition, reflection and generativity, and simultaneous vulnerability (inequities/disparities) and resilience. We uncovered a number of culturally driven and socially influenced findings that give greater insight into unique differences that potentially mediate the disparate pain outcomes between African Americans and other populations both within and outside the United States.
A key finding was the cultural expectations and emotional and behavioral norms of pain adjustment and communication. Our participants viewed bearing OA pain as a deeply personal experience that involved accepting and adjusting to pain, a concept consistent with other studies (Harris et al., 2015). Recent work by Robinson-Lane (2019) maintains that chronic pain is a stimulus that requires an individual’s response system to adapt to remain functional and have quality of life. However, older African Americans’ acceptance of OA pain was often shrouded in a cycle of hiding and denying pain, perhaps a form of reluctant acceptance (Harris et al., 2015). While most participants did not discuss pain openly, they found safe ways to share their pain with others. This often meant using indirect statements, such as “I don’t feel good,” or unconsciously responding to others’ inquiry with “I’m fine.” These responses are in fact forms of hiding pain. Acclaimed African American life coach, Iyanla Vanzant, quoted in an episode of Iyanla: Fix My Life (Vanzant & Harrison, 2019), “when someone asks you ‘How are you?’ Don’t say ‘I’m fine,’ because it’s a habit. Say, ‘I hurt.’” Although the prior statement referred to emotional pain, the same advice could be applied to physical pain. It is important to point out that hiding and ignoring pain has been shaped by historic events and trauma, such as slavery, which provided a very strong incentive to hide pain and endure. As noted by our participants, such behavior has resulted in the transgenerational transmittal of social and health behaviors of slaves whose survival mechanisms included overlooking their pain and maintaining a stoic attitude to care for their family. In particular, Robinson-Lane’s (2019) study identified that older African Americans’ adaption to the chronic pain is multifaceted and involves maintaining a positive attitude, relying on faith and prayer, staying active, being engaged in the community, and having good support systems. While similar adjustment and coping strategies were noted in our study (e.g., staying active and praying), others have also found that women with OA particularly find it necessary to be stoic, strong, and faith driven to cope and survive life stressors (Harris et al., 2016).
The need to balance their identity with the social stigma of living with a crippling chronic disease and debilitating pain was indeed critical. Along the lines of identity preservation, the phenomenon of “not claiming” a health condition surfaced and is prominent in African American communities (McKenzie & Skelly, 2014 ; Spruill et al., 2015) and is often a declaration of faith. For example, this cultural behavior was first revealed in a seminal arthritis study when an older African American stated, “I do not claim arthritis. God has not told me I have it. You have to claim it to have it” (Fiargo et al., 2004, p. 325). Spruill et al. (2015) suggest using this deeply embedded cultural belief of not claiming a disease to improve self-management rather than to stigmatize populations. One way to do this is to integrate their cultural systems of spiritual care with professional health care (Booker, 2015) and to reframe that acknowledging OA is an important aspect of Christian teachings on specifying/naming the issue in prayer. This leads to our next important finding on faith-based self-management.
Our findings provide a new and important departure from most chronic illness self-management representations which typically focus on the self and interpersonal domains (family, friends, doctor/health care provider; e.g., Grey et al., 2015; Ryan & Sawin, 2009; Stewart et al., 2014), but not explicitly on the spiritual (God, Jesus, or Holy Spirit) aspect as a distinct and embedded domain. Schulman-Green et al. (2012) identified spiritual resources as an important process of chronic illness self-management. While older African Americans have acknowledged a need for greater social support, understanding, and compassion without judgment or pity from family and friends (Booker, Cousin, & Buck, 2019), God played an equally integral role in African American older adults’ self-management experience. A study with Dominican adults, who were primarily older, also demonstrated a strong reliance and faith in God and the role of endurance in coping with OA pain (Yu et al., 2016). Specifically, older African Americans rely heavily on the spiritual guidance of a higher/supreme power through prayer and faith to manage all types of chronic pain (Booker, Herr, & Tripp-Reimer, 2019; Robinson-Lane & Vallerand, 2018). However, lower levels of perceived control over pain may result from their strong spiritual beliefs that permit them to relinquish external control to God, also known as God-mediated control (Booker, 2015; Fiargo et al., 2004; Ibrahim et al., 2004). Jones and colleagues (2008) concluded that “hoping and praying may not increase a patient’s ability to manage arthritis related pain . . . ” (p. 345). While this may have some merit, self-management frameworks may have greater applicability for older African Americans if facets of faith in God, accepting OA, and communicating pain to key people such as family/friends and providers are incorporated.
Clinical Implications
Culturally congruent pain management seeks to provide culturally relevant and personalized pain care within evidence-based standards of care (Rosa, 2018). There are a number of clinical implications that support trends in culturally responsive pain care (Robinson-Lane & Booker, 2017). The importance of open communication about pain between older African Americans and people and/or providers they trust cannot be overstated. Cohorts of older African Americans may be unlikely to initiate conversations with providers about pain (Robinson-Lane & Vallerand, 2018). Not discussing pain, especially with providers, may cause others to discount their pain and limit opportunities for pain control. Thus, nurses must apply a more direct approach to assessing pain rather than general questions like “How are you doing today?” (Booker & Herr, 2016). This is not to disregard personal preferences for different communication styles but rather to limit the silent and invisible suffering of a vulnerable group of older adults. In fact, providers should be informed about older African Americans’ pain communication style and work within their cultural approaches to convey pain to best understand their experience (Puia & McDonald, 2014).
It cannot be stressed enough the importance of providers asking, listening, and believing their African American patients’ report of pain, then providing evidence-based education and treatment recommendations. Yet, denying arthritis altogether may cause individuals to be less proactive/active in self-management and therefore may not seek appropriate health care. The unfair treatment of African Americans with pain has long been documented (Green et al., 2003), and this certainly calls for nurses and physicians to develop greater awareness of the healing power of therapeutic presence and empathy. African American older adults desire for providers to be more sensitive and thorough in their health assessments and pain treatment plans (Robinson-Lane & Vallerand, 2018).
Understanding the entire self-management process is important for fluidity in patient-centered care coordination and developing treatment plans that integrate biopsychosocial aspects that attend to how older African Americans interact with and maneuver their social and religious systems to deal with pain. Our participants’ experience aligns with the “Whole Health Perspective” which centers the patient at the core of their health care and is enveloped by self-care, professional care, and community to address health and well-being areas that matter most to patients (U.S. Department of Veterans Affairs, n.d.). The analysis reported here and in other publications (Booker, Cousin, & Buck, 2019; Booker, Herr, & Tripp-Reimer, 2019) showcases the importance of self-management, professional management, and the involvement of community/social systems in managing the pain of OA in African Americans. Rosa (2018) calls for nurses to optimize transcultural pain management and return to caring for the whole individual to achieve “human-centered pain alleviation” (p. 25). Nurses can work within the holistic framework to enhance care coordination and case management of patients with complex chronic pain.
Finally, providers and nurses should work more closely with older African Americans after diagnosis of OA to facilitate early acceptance and adjustment to the disease and empowerment to take control over pain. Acceptance and commitment therapy (ACT; Clarke et al., 2017) may prove beneficial to older African Americans when cultural values and meaning are integrated. ACT has been used across many health conditions, and its objective is to promote value-based action and behavioral changes that will lead to improvements in pain, functioning, and quality of life (Hughes et al., 2017). ACT can also counteract the personal pride that prevents some patients from accepting their diagnosis and instead motivate them toward action. Furthermore, the identification of key cultural factors and patterns, beyond spirituality, may yield important knowledge that informs more targeted interventions for this painful chronic condition. Our research can be used to provide a common support structure in developing evidence-based self-management care models and culturally innovative interventions (Tripp-Reimer, Choi, Kelley, & Enslein, 2001).
Strengths and Limitations
Despite a small convenience sample size, one strength of this study is its rigorous and full description of the experience of OA from a socioeconomically diverse sample of older African American men and women. Although women are often overrepresented in OA studies, we purposefully included both women and men in this study and attended to gender-related influences reflected in the stories of living with OA. Although new understanding on this common health condition was gained, this study was conducted among African Americans residing in Louisiana who have a distinct culture steeped in the integration of multiple cultures (e.g., African, Cajun/Creole, Native American) and religions (e.g., Protestant and Catholic); thus, our results may not be entirely generalizable or transferable to other African American/Black populations in the United States. In particular, it may be overly representative of a geographically defined culture and way of life.
While the interviews yielded rich data, a potential limitation of this study is the specificity of questions yielding response bias from participants. Furthermore, this study was a one-time analysis and only provides a small snapshot of their daily life experience. Member checking is one method to enhance trustworthiness of the data, albeit with some limitations of its own (Birt et al., 2016; Sandelowski, 1993), and we did not perform member validation; however, at the end of each interview, the interviewer summarized the participant’s key points and asked for clarification or elaboration before concluding the interview. Other analytic approaches such as phenomenological descriptive, ethnography, or grounded theory may have been appropriate, given the richness of our data. Overall, our study is one of the first studies in this decade to present new data to the scientific body on the African American experience of OA.
Conclusion
Bearing the pain is one complex process that African American older adults use to live with, cope, and manage pain as effectively as possible. This process includes adjusting to pain, sharing pain with others, and trusting God as healer. In this manner, older African Americans’ experience transcended into a metapersonal experience. In conclusion, our study is one of the first descriptive studies to focus on the experience of an underrepresented population living with chronic pain, therefore advancing our knowledge of their intimate personal and cultural ways of self-management. Their narratives ignite a level of introspection and cultural awareness that we as nurses and providers must possess when caring for populations who have unique understandings and experiences.
Footnotes
Acknowledgements
Appreciation is given to Dr. Maichou Lor and Dr. Sandy Daack-Hirsch for reviewing this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (T32NR011147, T32AG049673).